EUS-Guided Versus Percutaneous Celiac Neurolysis for the Management of Intractable Pain Due to Unresectable Pancreatic Cancer: A Randomized Clinical Trial

 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
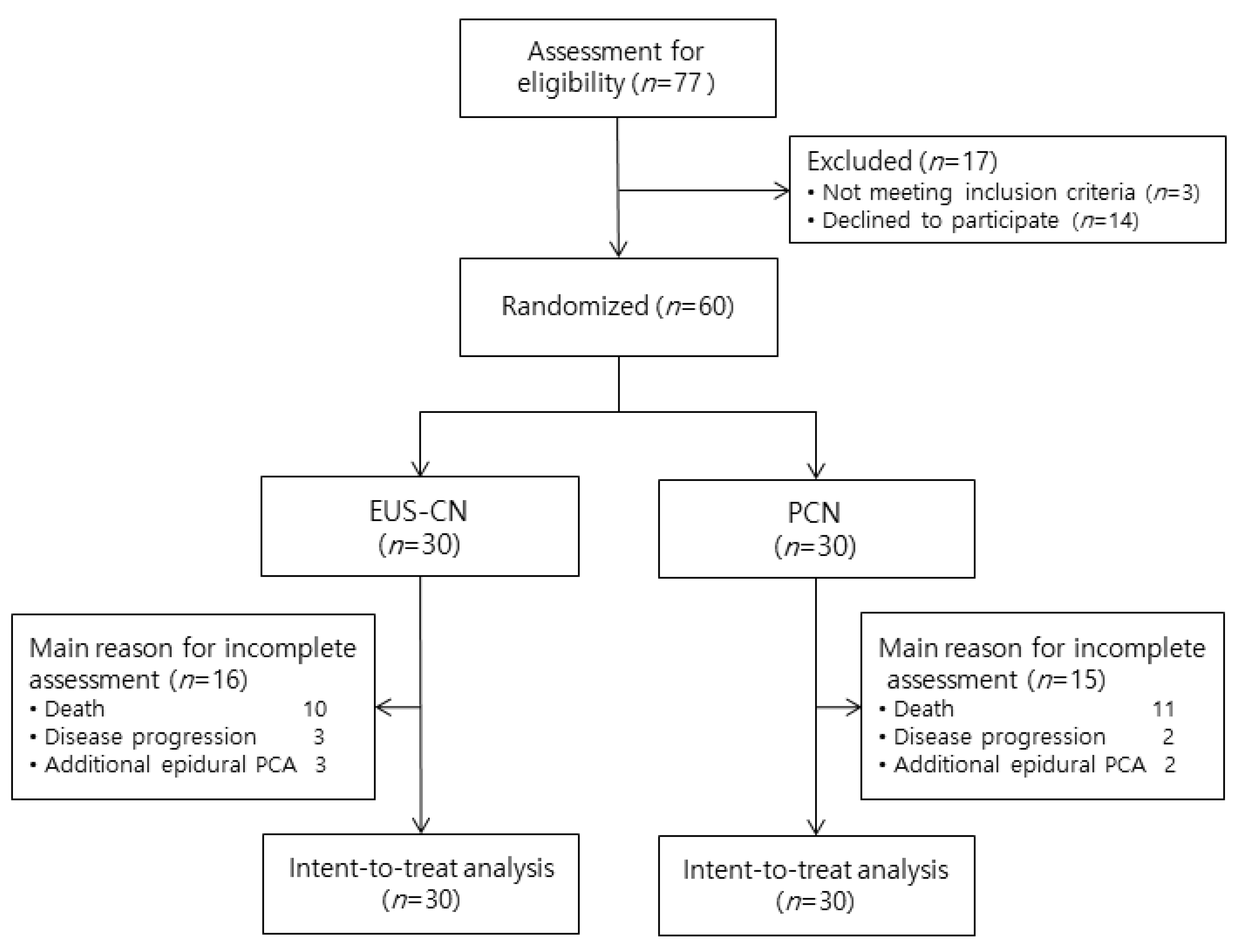
2.1. Study Design and Participants
2.2. Randomization and Masking
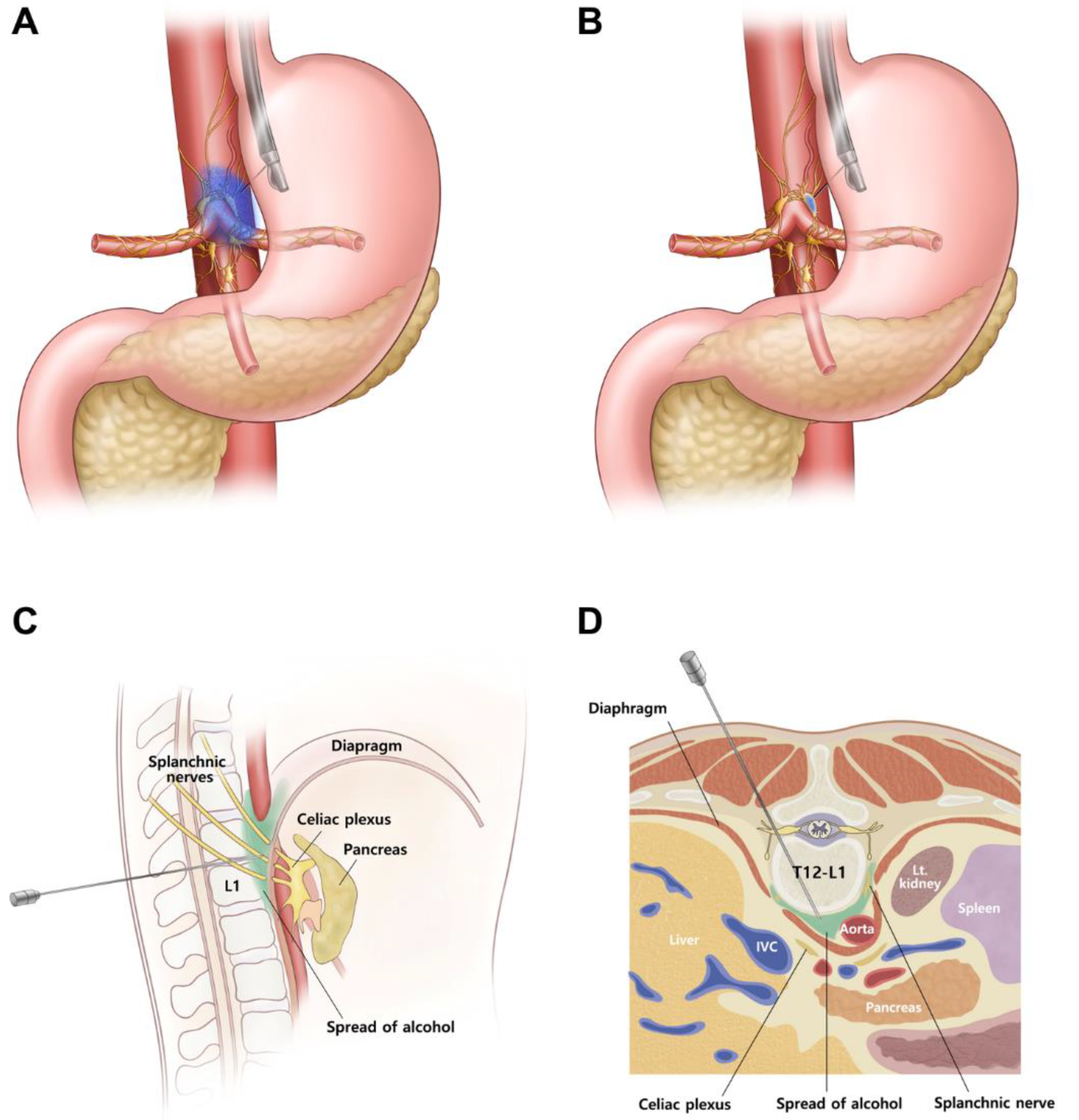
2.3. EUS-CN
2.4. Percutaneous CN (PCN)
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
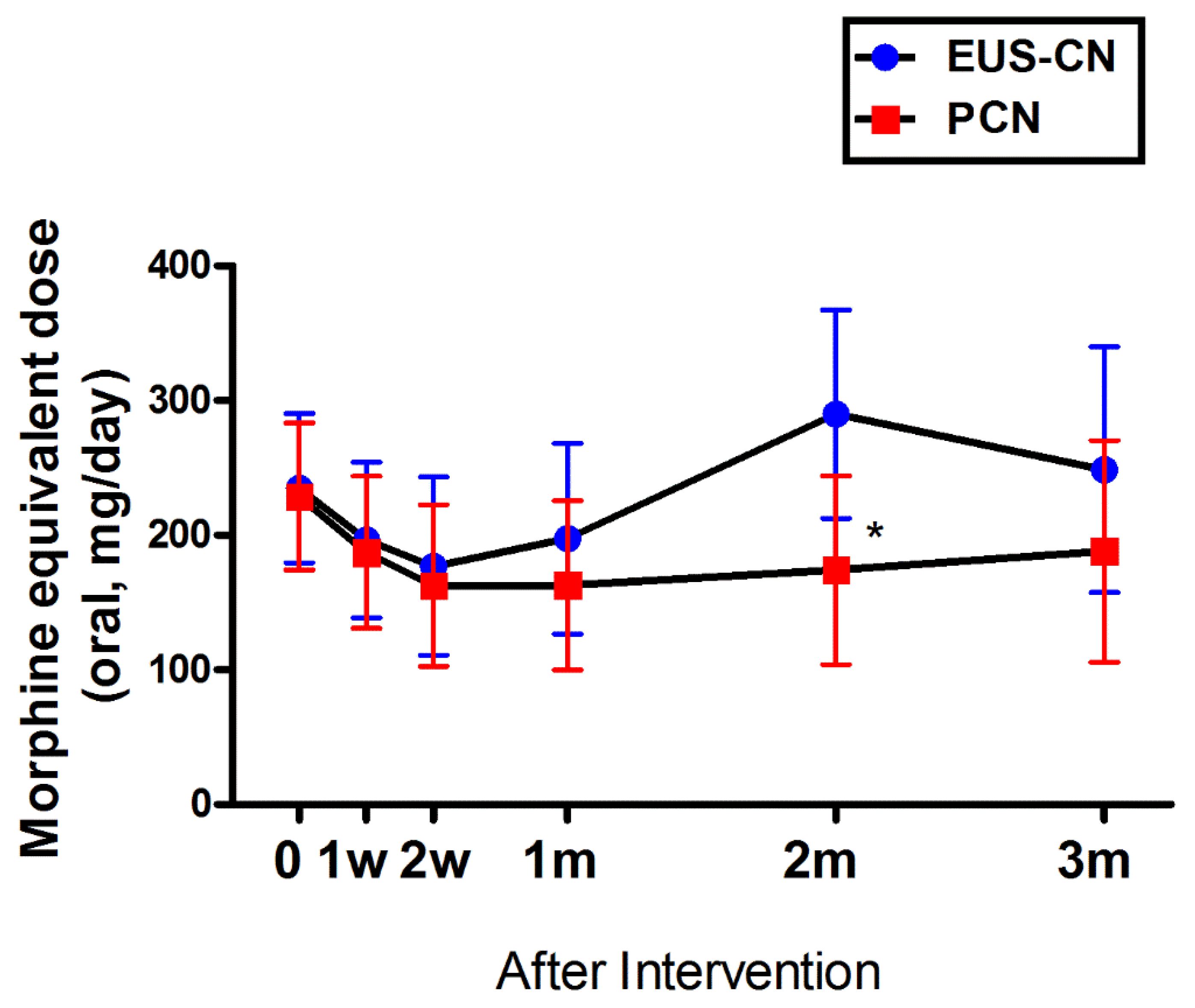
3.2. Primary Outcomes
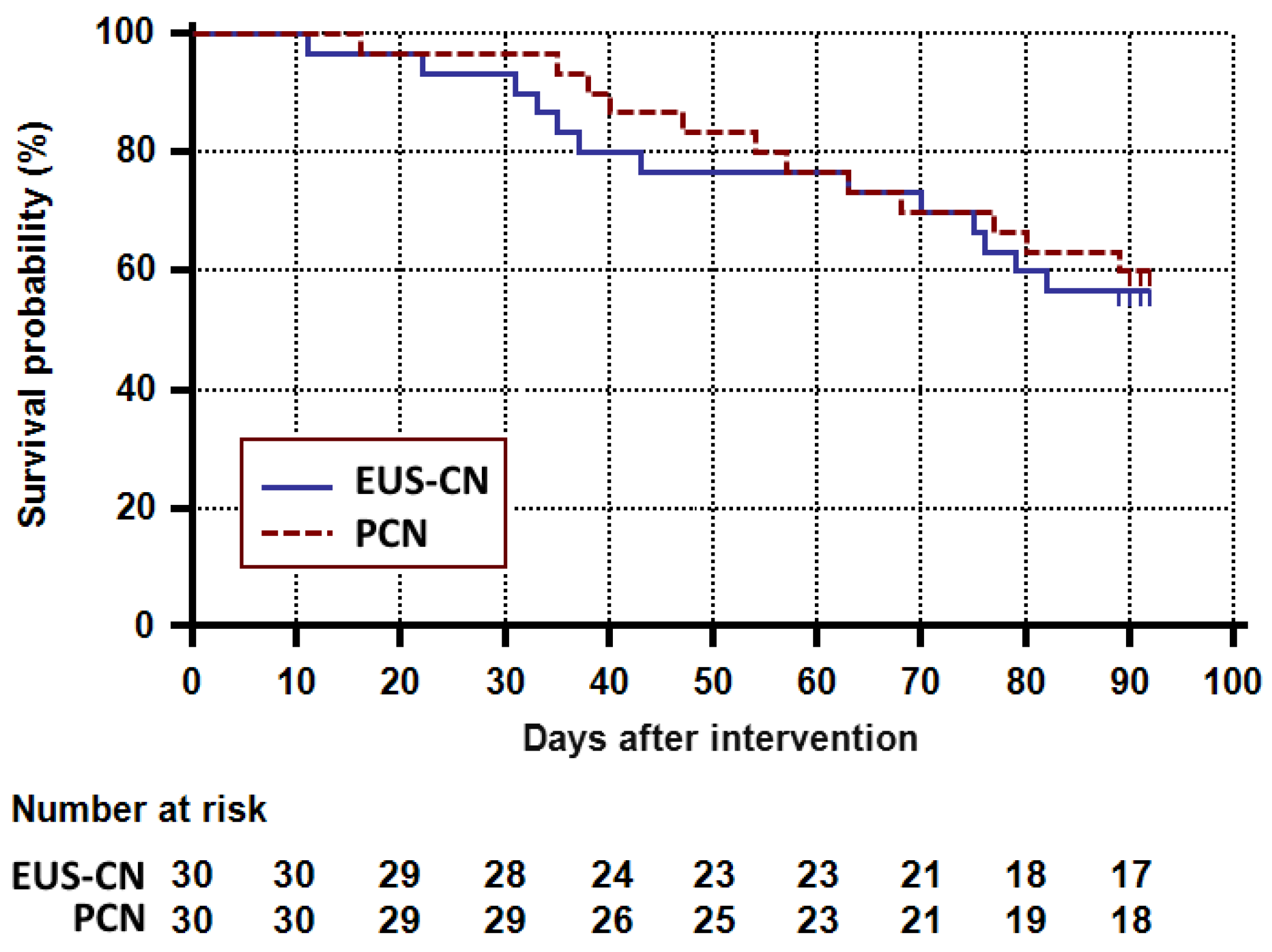
3.3. Secondary Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ilic, M.; Ilic, I. Epidemiology of pancreatic cancer. World J. Gastroenterol. 2016, 22, 9694–9705. [Google Scholar] [CrossRef] [PubMed]
- Kindler, H.L. A glimmer of hope for pancreatic cancer. N. Engl. J. Med. 2018, 379, 2463–2464. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Jansen, L.; Balavarca, Y.; Molina-Montes, E.; Babaei, M.; van der Geest, L.; Lemmens, V.; Van Eycken, L.; De Schutter, H.; Johannesen, T.B.; et al. Resection of pancreatic cancer in Europe and USA: An international large-scale study highlighting large variations. Gut 2019, 68, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Lakatos, G.; Balazs, A.; Kui, B.; Godi, S.; Szucs, A.; Szentesi, A.; Szentkereszty, Z.; Szmola, R.; Kelemen, D.; Papp, R.; et al. Pancreatic cancer: Multicenter prospective data collection and analysis by the Hungarian Pancreatic Study Group. J. Gastrointest. Liver Dis. 2016, 25, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Arcidiacono, P.G.; Calori, G.; Carrara, S.; McNicol, E.D.; Testoni, P.A. Celiac plexus block for pancreatic cancer pain in adults. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Koulouris, A.I.; Banim, P.; Hart, A.R. Pain in patients with pancreatic cancer: Prevalence, mechanisms, management and future developments. Dig. Dis. Sci. 2017, 62, 861–870. [Google Scholar] [CrossRef]
- Barbera, L.; Taylor, C.; Dudgeon, D. Why do patients with cancer visit the emergency department near the end of life? CMAJ 2010, 182, 563–568. [Google Scholar] [CrossRef] [Green Version]
- Drewes, A.M.; Campbell, C.M.; Ceyhan, G.O.; Delhaye, M.; Garg, P.K.; van Goor, H.; Laquente, B.; Morlion, B.; Olesen, S.S.; Singh, V.K.; et al. Pain in pancreatic ductal adenocarcinoma: A multidisciplinary, International guideline for optimized management. Pancreatol. 2018, 18, 446–457. [Google Scholar] [CrossRef]
- WHO’s Cancer Pain Ladder for Adults. Available online: https://www.who.int/cancer/palliative/painladder/en/. (accessed on 14 May 2019).
- Minaga, K.; Takenaka, M.; Kamata, K.; Yoshikawa, T.; Nakai, A.; Omoto, S.; Miyata, T.; Yamao, K.; Imai, H.; Sakamoto, H.; et al. Alleviating pancreatic cancer-associated pain using endoscopic ultrasound-guided neurolysis. Cancers (Basel) 2018, 10, 50. [Google Scholar] [CrossRef] [Green Version]
- Fugere, F.; Lewis, G. Coeliac plexus block for chronic pain syndromes. Can. J. Anaesth. 1993, 40, 954–963. [Google Scholar] [CrossRef]
- Nagels, W.; Pease, N.; Bekkering, G.; Cools, F.; Dobbels, P. Celiac plexus neurolysis for abdominal cancer pain: A systematic review. Pain Med. 2013, 14, 1140–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.Y.; Schroeder, D.R.; Carns, P.E.; Wilson, J.L.; Martin, D.P.; Kinney, M.O.; Mantilla, C.B.; Warner, D.O. Effect of neurolytic celiac plexus block on pain relief, quality of life, and survival in patients with unresectable pancreatic cancer: A randomized controlled trial. JAMA 2004, 291, 1092–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiersema, M.J.; Wiersema, L.M. Endosonography-guided celiac plexus neurolysis. Gastrointest. Endosc. 1996, 44, 656–662. [Google Scholar] [CrossRef]
- Levy, M.J.; Topazian, M.D.; Wiersema, M.J.; Clain, J.E.; Rajan, E.; Wang, K.K.; de la Mora, J.G.; Gleeson, F.C.; Pearson, R.K.; Pelaez, M.C.; et al. Initial evaluation of the efficacy and safety of endoscopic ultrasound-guided direct ganglia neurolysis and block. Am. J. Gastroenterol. 2008, 103, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.; Yasuda, I.; Kawakami, H.; Hayashi, T.; Hisai, H.; Irisawa, A.; Mukai, T.; Katanuma, A.; Kubota, K.; Ohnishi, T.; et al. Endoscopic ultrasound-guided celiac ganglia neurolysis vs. celiac plexus neurolysis: A randomized multicenter trial. Endoscopy 2013, 45, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.J.; Gleeson, F.C.; Topazian, M.D.; Fujii-Lau, L.L.; Enders, F.T.; Larson, J.J.; Mara, K.; Abu Dayyeh, B.K.; Alberts, S.R.; Hallemeier, C.L.; et al. Combined celiac ganglia and plexus neurolysis shortens survival, without benefit, vs plexus neurolysis alone. Clin. Gastroenterol. Hepatol. 2019, 17, 728–738.e9. [Google Scholar] [CrossRef] [Green Version]
- Wyse, J.M.; Carone, M.; Paquin, S.C.; Usatii, M.; Sahai, A.V. Randomized, double-blind, controlled trial of early endoscopic ultrasound-guided celiac plexus neurolysis to prevent pain progression in patients with newly diagnosed, painful, inoperable pancreatic cancer. J. Clin. Oncol. 2011, 29, 3541–3546. [Google Scholar] [CrossRef]
- Gunaratnam, N.T.; Sarma, A.V.; Norton, I.D.; Wiersema, M.J. A prospective study of EUS-guided celiac plexus neurolysis for pancreatic cancer pain. Gastrointest. Endosc. 2001, 54, 316–324. [Google Scholar] [CrossRef]
- Teoh, A.Y.B.; Dhir, V.; Kida, M.; Yasuda, I.; Jin, Z.D.; Seo, D.W.; Almadi, M.; Ang, T.L.; Hara, K.; Hilmi, I.; et al. Consensus guidelines on the optimal management in interventional EUS procedures: Results from the Asian EUS group RAND/UCLA expert panel. Gut 2018, 67, 1209–1228. [Google Scholar] [CrossRef] [Green Version]
- Gress, F.; Schmitt, C.; Sherman, S.; Ikenberry, S.; Lehman, G. A prospective randomized comparison of endoscopic ultrasound- and computed tomography-guided celiac plexus block for managing chronic pancreatitis pain. Am. J. Gastroenterol. 1999, 94, 900–905. [Google Scholar] [CrossRef]
- Samanta, J.; Kendall, J.; Samanta, A. 10-minute consultation: Chronic low back pain. BMJ 2003, 326, 535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerke, H.; Silva, R.G., Jr.; Shamoun, D.; Johnson, C.J.; Jensen, C.S. EUS characteristics of celiac ganglia with cytologic and histologic confirmation. Gastrointest. Endosc. 2006, 64, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Yamamuro, M.; Kusaka, K.; Kato, M.; Takahashi, M. Celiac plexus block in cancer pain management. Tohoku J. Exp. Med. 2000, 192, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, Y.G.; Shin, J.W.; Leem, J.G.; Suh, J.H. Computed tomography (CT) simulated fluoroscopy-guided transdiscal approach in transcrural celiac plexus block. Korean J. Pain 2013, 26, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.; Degenhardt, L.; Hoban, B.; Gisev, N. A synthesis of oral morphine equivalents (OME) for opioid utilisation studies. Pharmacoepidemiol. Drug Saf. 2016, 25, 733–737. [Google Scholar] [CrossRef]
- Butt, Z.; Parikh, N.D.; Beaumont, J.L.; Rosenbloom, S.K.; Syrjala, K.L.; Abernethy, A.P.; Benson, A.B., 3rd; Cella, D. Development and validation of a symptom index for advanced hepatobiliary and pancreatic cancers: The National Comprehensive Cancer Network Functional Assessment of Cancer Therapy (NCCN-FACT) Hepatobiliary-Pancreatic Symptom Index (NFHSI). Cancer 2012, 118, 5997–6004. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef]
- Amr, Y.M.; Makharita, M.Y. Comparative study between 2 protocols for management of severe pain in patients with unresectable pancreatic cancer: One-year follow-up. Clin. J. Pain 2013, 29, 807–813. [Google Scholar] [CrossRef]
- Kappelle, W.F.W.; Bleys, R.; van Wijck, A.J.M.; Siersema, P.D.; Vleggaar, F.P. EUS-guided celiac ganglia neurolysis: A clinical and human cadaver study (with video). Gastrointest. Endosc. 2017, 86, 655–663. [Google Scholar] [CrossRef]
- Bang, J.Y.; Sutton, B.; Hawes, R.H.; Varadarajulu, S. EUS-guided celiac ganglion radiofrequency ablation versus celiac plexus neurolysis for palliation of pain in pancreatic cancer: A randomized controlled trial (with videos). Gastrointest. Endosc. 2019, 89, 58–66.e53. [Google Scholar] [CrossRef]
- Rykowski, J.J.; Hilgier, M. Efficacy of neurolytic celiac plexus block in varying locations of pancreatic cancer: Influence on pain relief. Anesthesiology 2000, 92, 347–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | EUS-CN (n = 30) | PCN (n = 30) |
|---|---|---|
| Age, mean (SD), years | 58.4 (9.6) | 61.2 (7.4) |
| Male, No. (%) | 15 (50.0) | 20 (66.7) |
| Height, mean (SD), cm | 162.4 (10.3) | 162.8 (9.1) |
| Weight, mean (SD), kg | 53.7 (8.6) | 55.8 (9.2) |
| Comorbidity, No. (%) | ||
| Diabetes | 10 (33.3) | 15 (50.0) |
| Hypertension | 11 (36.7) | 14 (46.7) |
| Pain duration, median (IQR), months | 6.0 (2.0 to 10.0) | 6.0 (4.0 to 11.0) |
| Pain intensity, median (IQR), NRS a | ||
| Abdominal pain | 6.0 (4.0 to 8.0) | 6.0 (4.0 to 8.0) |
| Back pain | 6.0 (4.0 to 8.0) | 6.0 (4.0 to 8.0) |
| Pain area, No. (%) | ||
| Abdomen and back | 7 (11.7) | 14 (23.3) |
| Abdomen only | 20 (33.3) | 11 (36.7) |
| Back only | 3 (10.0) | 5 (16.7) |
| Pancreas cancer location No. (%) | ||
| Head | 15 (50.0) | 17 (56.7) |
| Body and tail | 19 (63.3) | 13 (43.3) |
| Overall stage at intervention | ||
| III | 4 (13.3) | 6 (20.0) |
| IV | 26 (86.7) | 24 (80.0) |
| MED, mean (SD), mg/day | 221.7 (162.3) | 214.2 (146.1) |
| BDI, mean (SD) b | 21.4 (10.0) | 21.2 (10.1) |
| NFHSI, mean (SD) c | 35.3 (10.5) | 36.5 (7.1) |
| Interval from diagnosis to CN, median (IQR), weeks | 32.0 (21.0 to 54.0) | 34.0 (20.0 to 50.0) |
| Variables | Time | Adjusted Prediction (95% CI) a | Estimated Difference (95% CI) b | p-Value | |
|---|---|---|---|---|---|
| EUS-CN | PCN | ||||
| Abdominal pain | Baseline | 6.0 (5.1 to 7.0) | 5.5 (4.6 to 6.5) | −0.5 (−1.8 to 0.8) | 0.46 |
| (NRS) | 1 week | 4.8 (3.9 to 5.8) | 3.8 (2.9 to 4.8) | −1.0 (−2.3 to 0.3) | 0.15 |
| 2 weeks | 4.6 (3.6 to 5.5) | 3.9 (2.9 to 4.8) | −0.7 (−2.0 to 0.7) | 0.33 | |
| 1 month | 4.7 (3.7 to 5.7) | 3.7 (2.7 to 4.6) | −1.0 (−2.4 to 0.4) | 0.17 | |
| 2 months | 5.4 (4.3 to 6.5) | 3.9 (2.9 to 5.0) | −1.5 (−3.0 to 0.0) | 0.052 | |
| 3 months | 5.6 (4.4 to 6.9) | 4.2 (3.0 to 5.4) | −1.4 (−3.1 to 0.3) | 0.11 | |
| Back pain | Baseline | 5.5 (4.5 to 6.5) | 5.6 (4.7 to 6.6) | 0.1 (−1.2 to 1.5) | 0.85 |
| (NRS) | 1 week | 3.7 (2.7 to 4.7) | 3.1 (2.1 to 4.0) | −0.7 (−2.0 to 0.7) | 0.35 |
| 2 weeks | 4.0 (3.0 to 5.0) | 3.0 (2.0 to 4.0) | −1.0 (−2.4 to 0.4) | 0.17 | |
| 1 month | 3.6 (2.6 to 4.6) | 2.7 (1.7 to 3.7) | −0.9 (−2.4 to 0.5) | 0.21 | |
| 2 months | 4.3 (3.2 to 5.4) | 3.4 (2.3 to 4.4) | −0.9 (−2.5 to 0.6) | 0.24 | |
| 3 months | 4.3 (3.1 to 5.6) | 3.4 (2.2 to 4.6) | −0.9 (−2.7 to 0.9) | 0.31 | |
| Variable | Time | Estimated Proportion (95% CI) b | Difference of Proportion (95% CI) c | p-Value d | |
|---|---|---|---|---|---|
| EUS-CN | PCN | ||||
| Successful | 1 week | 60.0 (42.5 to 77.5) | 56.7 (38.9 to 74.4) | −3.3 (−28.5 to 21.8) | 0.79 |
| Responder a | 2 weeks | 46.7 (28.8 to 64.5) | 53.3 (35.5 to 71.2) | 6.7 (−18.8 to 32.2) | 0.61 |
| 1 month | 56.7 (38.9 to 74.4) | 70.0 (53.6 to 86.4) | 13.3 (−11.3 to 37.9) | 0.29 | |
| 2 months | 30.0 (13.6 to 46.4) | 43.3 (25.6 to 61.1) | 13.3 (−11.3 to 37.9) | 0.29 | |
| 3 months | 23.3 (8.2 to 38.5) | 36.7 (19.4 to 53.9) | 14.6 (−9.1 to 38.3) | 0.26 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, W.J.; Oh, Y.; Yoo, C.; Jang, S.; Cho, S.-S.; Suh, J.-H.; Choi, S.-S.; Park, D.H. EUS-Guided Versus Percutaneous Celiac Neurolysis for the Management of Intractable Pain Due to Unresectable Pancreatic Cancer: A Randomized Clinical Trial. J. Clin. Med. 2020, 9, 1666. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061666
Yoon WJ, Oh Y, Yoo C, Jang S, Cho S-S, Suh J-H, Choi S-S, Park DH. EUS-Guided Versus Percutaneous Celiac Neurolysis for the Management of Intractable Pain Due to Unresectable Pancreatic Cancer: A Randomized Clinical Trial. Journal of Clinical Medicine. 2020; 9(6):1666. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061666
Chicago/Turabian StyleYoon, Won Jae, Yul Oh, Changhoon Yoo, Sunguk Jang, Seong-Sik Cho, Jeong-Hun Suh, Seong-Soo Choi, and Do Hyun Park. 2020. "EUS-Guided Versus Percutaneous Celiac Neurolysis for the Management of Intractable Pain Due to Unresectable Pancreatic Cancer: A Randomized Clinical Trial" Journal of Clinical Medicine 9, no. 6: 1666. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061666