Real-World Clinical Outcomes Associated with Canagliflozin in Patients with Type 2 Diabetes Mellitus in Spain: The Real-Wecan Study

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Patient Population
2.2. Outcomes and Study Measures
2.3. Statistical Methods
3. Results
3.1. Demographic and Baseline Characteristics
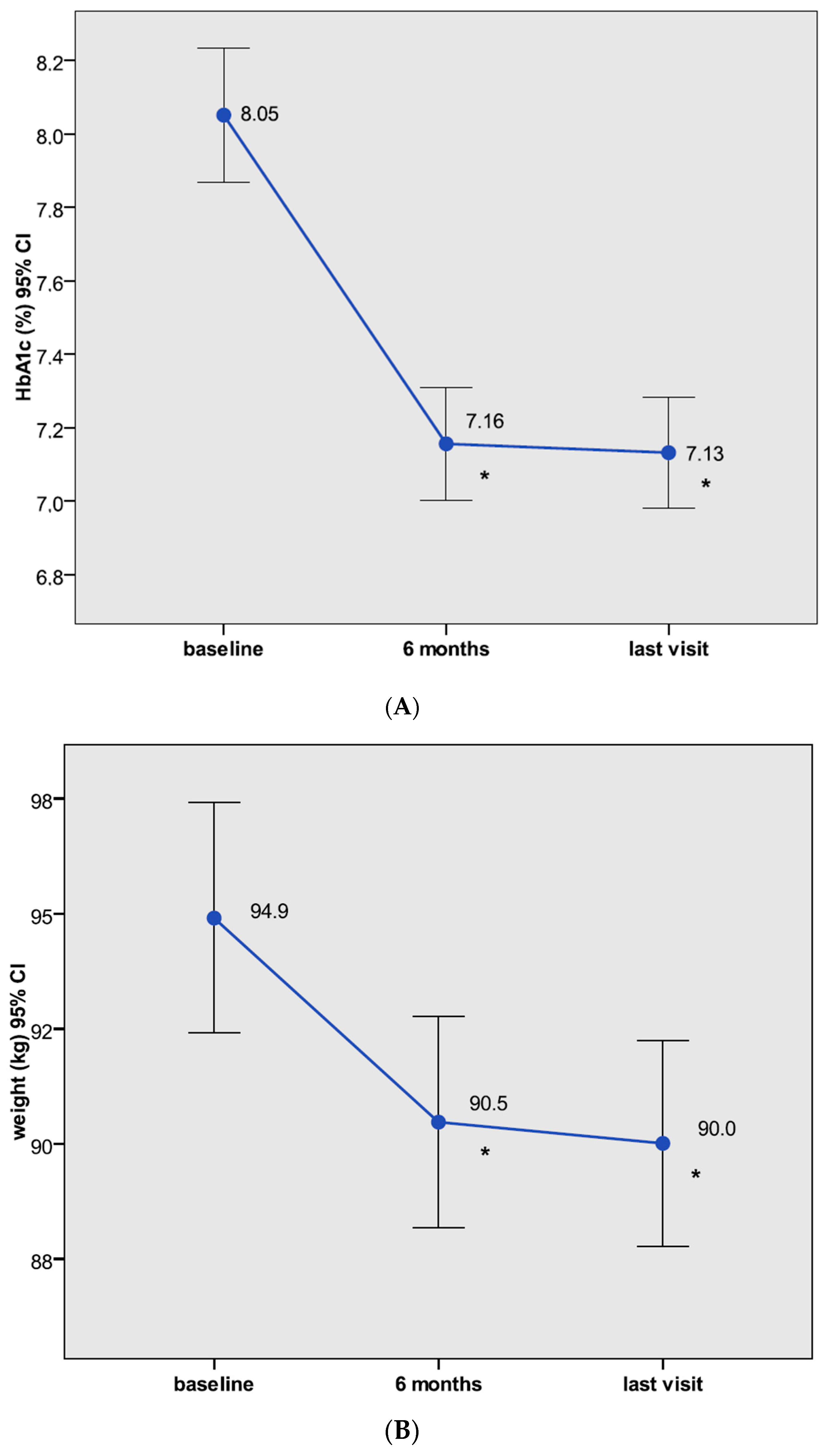
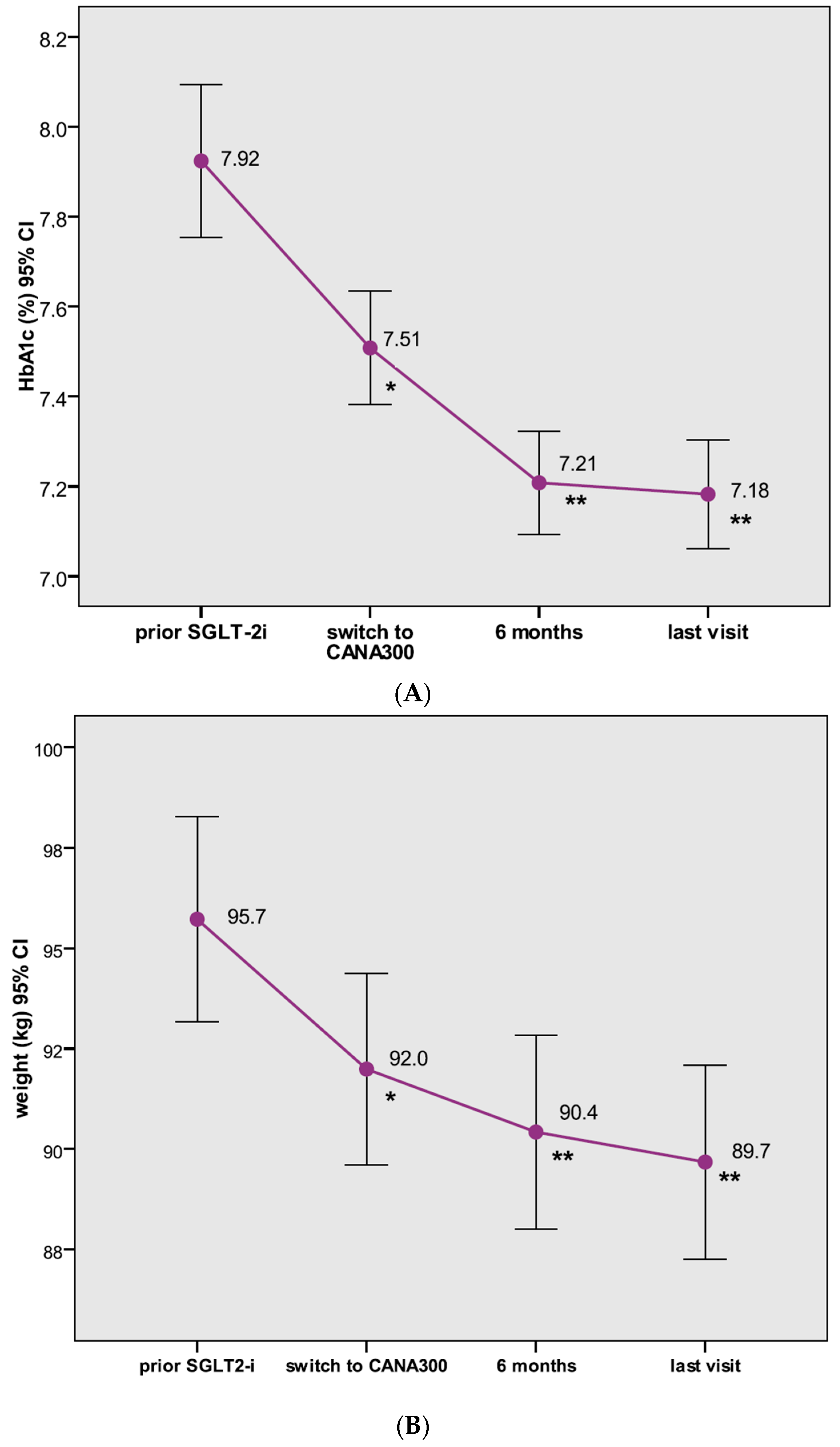
3.2. Analyses of Effectiveness
3.3. Analyses of Safety
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Prior Publication
Abbreviations
| ACEis | angiotensin-converting enzyme inhibitors |
| AEs | adverse effects |
| ALT | alanine transaminase |
| ARBs | angiotensin II receptor blockers |
| AST | aspartate aminotransferase |
| BP | blood pressure |
| CANA100 | canagliflozin 100 mg |
| CANA300 | canagliflozin 300 mg |
| CKD | chronic kidney disease |
| CV | cardiovascular |
| DBP | diastolic blood pressure |
| DKA | diabetic ketoacidosis |
| DPP-4is | dipeptidyl peptidase 4 inhibitors |
| eGFR | estimated glomerular filtrate rate |
| FPG | fasting plasma glucose |
| GGT | gamma-glutamyl transferase |
| GLDs | glucose-lowering drugs |
| GLP-1 | glucagon-like peptide-1 |
| GLP-1ras | GLP-1 receptor agonists |
| GLUT-9 | human glucose transporter 9 |
| GMIs | genital mycotic infections |
| HbA1c | glycated hemoglobin |
| HDL-C | high-density lipoprotein cholesterol |
| HR | heart rate |
| IQR | interquartile range |
| LDL-C | low-density lipoprotein cholesterol |
| NAFLD | non-alcoholic fatty liver disease |
| PYY | peptide tyrosine tyrosine |
| RCTs | randomized clinical trials |
| Real-WECAN | Real World Evidence with Canagliflozin |
| RWS | real-world studies |
| SBP | systolic blood pressure |
| SD | standard deviation |
| SGLT-1 | sodium–glucose co-transporter type 1 |
| SGLT-2is | sodium–glucose co-transporter type 2 inhibitors |
| T2DM | type 2 diabetes |
| UGE | urinary glucose excretion |
| UTIs | urinary tract infections |
| V1 | visit 1 |
| V2 | visit 2 |
| V3 | visit 3 |
| WDs | withdrawals |
| WL | weight loss. |
References
- Thomas, M.C.C.; Cherney, D.Z. The actions of SGLT2 inhibitors on metabolism, renal function and blood pressure. Diabetologia 2018, 61, 2098–2107. [Google Scholar] [CrossRef] [Green Version]
- Chilton, R.J. Effects of sodium-glucose cotransporter-2 inhibitors on the cardiovascular and renal complications of type 2 diabetes. Diabetes Obes. Metab. 2020, 22, 16–29. [Google Scholar] [CrossRef]
- Devineni, D.D.; Curtin, C.R.; Polidori, D.; Gutierrez, M.J.; Murphy, J.; Rusch, S.; Rothenberg, P.L. Pharmacokinetics and pharmacodynamics of canagliflozin, a sodium glucose co-transporter 2 inhibitor, in subjects with type 2 diabetes mellitus. J. Clin. Pharmacol. 2013, 53, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Sha, S.; Polidori, D.; Farrell, K.; Ghosh, A.; Natarajan, J.; Vaccaro, N.; Plum-Mörschel, L. Pharmacodynamic differences between canagliflozin and dapagliflozin: Results of a randomized, double-blind, crossover study. Diabetes Obes. Metab. 2015, 17, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Rieg, T.; Vallon, V. Development of SGLT1 and SGLT2 inhibitors. Diabetologia 2018, 61, 2079–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polidori, D.; Sha, S.; Mudaliar, S.; Ciaraldi, T.P.; Ghosh, A.; Vaccaro, N.; Henry, R.R. Canagliflozin lowers postprandial glucose and insulin by delaying intestinal glucose absorption in addition to increasing urinary glucose excretion: Results of a randomized, placebo-controlled study. Diabetes Care 2013, 36, 2154–2161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Prato, S.; Nauck, M.; Duran-Garcia, S.; Maffei, L.; Rohwedder, K.; Theuerkauf, A.; Parikh, S. Long-term glycaemic response and tolerability of dapagliflozin versus a sulphonylurea as add-on therapy to metformin in patients with type 2 diabetes: 4-year data. Diabetes Obes. Metab. 2015, 17, 581–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridderstråle, M.; Andersen, K.R.; Zeller, C.; Kim, G.; Woerle, H.J.; Broedl, U.C. EMPA-REG H2H-SU trial investigators. Comparison of empagliflozin and glimepiride as add-on to metformin in patients with type 2 diabetes: A 104-week randomised, active-controlled, double-blind, phase 3 trial. Lancet Diabetes Endocrinol. 2014, 2, 691–700. [Google Scholar]
- Leiter, L.A.; Yoon, K.H.; Arias, P.; Langslet, G.; Xie, J.; Balis, D.A.; Millington, D.; Vercruysse, F.; Canovatchel, W.; Meininger, G. Canagliflozin provides durable glycemic improvements and body weight reduction over 104 weeks versus glimepiride in patients with type 2 diabetes on metformin: A randomized, double-blind, phase 3 study. Diabetes Care 2015, 38, 355–364. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, J.; Mathieu, C.; Chen, H.; Garcia-Sanchez, R.; Saraiva, G.L. Dapagliflozin versus saxagliptin as add-on therapy in patients with type 2 diabetes inadequately controlled with metformin. Arch. Endocrinol. Metab. 2018, 62, 424–443. [Google Scholar] [CrossRef] [Green Version]
- Roden, M.; Weng, J.; Eilbracht, J.; Delafont, B.; Kim, G.; Woerle, H.J.; Broedl, U.C. EMPA-REG MONO trial investigators. Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2013, 1, 208–219. [Google Scholar] [CrossRef]
- Lavalle-González, F.J.; Januszewicz, A.; Davidson, J.; Tong, C.; Qiu, R.; Canovatchel, W.; Meininger, G. Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: A randomised trial. Diabetologia 2013, 56, 2582–2592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, R.R.; Murray, A.V.; Marmolejo, M.H.; Hennicken, D.; Ptaszynska, A.; List, J.F. Dapagliflozin, metformin XR, or both: Initial pharmacotherapy for type 2 diabetes, a randomised controlled trial. Int. J. Clin. Pract. 2012, 66, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Hollander, P.; Liu, J.; Hill, J.; Johnson, J.; Jiang, Z.W.; Golm, G.; Huyck, S.; Terra, S.G.; Mancuso, J.P.; Engel, S.S.; et al. Ertugliflozin Compared with Glimepiride in Patients with Type 2 Diabetes Mellitus Inadequately Controlled on Metformin: The VERTIS SU Randomized Study. Diabetes 2018, 9, 193–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. EMPA-REG OUTCOME Investigators. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. CANVAS Program Collaborative Group. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. CREDENCE Trial Investigators. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. DAPA-HF Trial Committees and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, J.; Aggarwal, N.; Polidori, D.; Zhao, Y.; Arbit, D.; Usiskin, K.; Capuano, G.; Canovatchel, W. Canagliflozin, DIA 2001 Study Group. Dose-ranging effects of canagliflozin, a sodium-glucose cotransporter 2 inhibitor, as add-on to metformin in subjects with type 2 diabetes. Diabetes Care 2012, 35, 1232–1238. [Google Scholar] [CrossRef] [Green Version]
- Zaccardi, F.; Webb, D.R.; Htike, Z.Z.; Youssef, D.; Khunti, K.; Davies, M.J. Efficacy and safety of sodium-glucose co-transporter-2 inhibitors in type 2 diabetes mellitus: Systematic review and network meta-analysis. Diabetes Obes. Metab. 2016, 18, 783–794. [Google Scholar] [CrossRef]
- Baptist, G. The Cardiovascular Benefits Associated with the Use of Sodium-Glucose Cotransporter 2 Inhibitors—Real-World Data. Eur. Endocrinol. 2018, 14, 17–23. [Google Scholar]
- Kosiborod, M.; Cavender, M.A.; Fu, A.Z.; Wilding, J.P.; Khunti, K.; Holl, R.W.; Norhammar, A.; Birkeland, K.I.; Jørgensen, M.E.; Thuresson, M.; et al. CVD-REAL Investigators and Study Group*. Lower Risk of Heart Failure and Death in Patients Initiated on Sodium-Glucose Cotransporter-2 Inhibitors Versus Other Glucose-Lowering Drugs: The C.V.D-REAL Study (Comparative Effectiveness of Cardiovascular Outcomes in New Users of Sodium-Glucose Cotransporter-2 Inhibitors). Circulation 2017, 136, 249–259. [Google Scholar] [PubMed]
- Kosiborod, M.; Lam, C.S.P.; Kohsaka, S.; Kim, D.J.; Karasik, A.; Shaw, J.; Tangri, N.; Goh, S.Y.; Thuresson, M.; Chen, H.; et al. CVD-REAL Investigators and Study Group. Cardiovascular Events Associated With, S.G.LT-2 Inhibitors Versus Other Glucose-Lowering Drugs: The, C.V.D-REAL 2 Study. J. Am. Coll. Cardiol. 2018, 71, 2628–2639. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Karasik, A.; Thuresson, M.; Melzer-Cohen, C.; Chodick, G.; Khunti, K.; Wilding, J.P.H.; Garcia Rodriguez, L.A.; Cea-Soriano, L.; Kohsaka, S.; et al. Kidney outcomes associated with use of, S.G.LT2 inhibitors in real-world clinical practice (CVD-REAL 3): A multinational observational cohort study. Lancet Diabetes Endocrinol. 2020, 8, 27–35. [Google Scholar] [CrossRef]
- Ryan, P.B.; Buse, J.B.; Schuemie, M.J.; DeFalco, F.; Yuan, Z.; Stang, P.E.; Berlin, J.A.; Rosenthal, N. Comparative effectiveness of canagliflozin, SGLT2 inhibitors and non-SGLT2 inhibitors on the risk of hospitalization for heart failure and amputation in patients with type 2 diabetes mellitus: A real-world meta-analysis of 4 observational databases (OBSERVE-4D). Diabetes Obes. Metab. 2018, 20, 2585–2597. [Google Scholar]
- Yuan, Z.; DeFalco, F.J.; Ryan, P.B.; Schuemie, M.J.; Stang, P.E.; Berlin, J.A.; Desai, M.; Rosenthal, N. Risk of lower extremity amputations in people with type 2 diabetes mellitus treated with sodium-glucose co-transporter-2 inhibitors in the USA: A retrospective cohort study. Diabetes Obes. Metab. 2018, 20, 582–589. [Google Scholar] [CrossRef] [Green Version]
- Udell, J.A.; Yuan, Z.; Rush, T.; Sicignano, N.M.; Galitz, M.; Rosenthal, N. Cardiovascular Outcomes and Risks After Initiation of a Sodium Glucose Cotransporter 2 Inhibitor: Results From the, EASEL Population-Based Cohort Study (Evidence for Cardiovascular Outcomes with Sodium Glucose Cotransporter 2 Inhibitors in the Real World). Circulation 2018, 137, 1450–1459. [Google Scholar] [CrossRef]
- Tanton, D.; Duh, M.S.; Lafeuille, M.H.; Lefebvre, P.; Pilon, D.; Zhdanava, M.; Emond, B.; Inman, D.; Bailey, R.A. Real-world evaluation of Hba1c, blood pressure, and weight loss among patients with type 2 diabetes mellitus treated with canagliflozin: An analysis of electronic medical records from a network of hospitals in Florida. Curr. Med. Res. Opin. 2018, 34, 1099–1115. [Google Scholar] [CrossRef]
- Buysman, E.K.; Anderson, A.; Bacchus, S.; Ingham, M. Retrospective Study on the Impact of Adherence in Achieving Glycemic Goals in Type 2 Diabetes Mellitus Patients Receiving Canagliflozin. Adv. Ther. 2017, 34, 937–953. [Google Scholar] [CrossRef]
- Johnson, J.F.; Parsa, R.; Bailey, R. Real world clinical outcomes and patient characteristics for canagliflozin treated patients in a specialty diabetes clinic. Curr. Med. Res. Opin. 2017, 33, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Woo, V.; Bell, A.; Clement, M.; Noronha, L.; Tsoukas, M.A.; Camacho, F.; Traina, S.; Georgijev, N.; Culham, M.D.; Rose, J.B.; et al. CANadian CAnagliflozin REgistry: Effectiveness and safety of canagliflozin in the treatment of type 2 diabetes mellitus in Canadian clinical practice. Diabetes Obes. Metab. 2019, 21, 691–699. [Google Scholar] [CrossRef]
- Rosenthal, N.; Meininger, G.; Ways, K.; Polidori, D.; Desai, M.; Qiu, R.; Alba, M.; Vercruysse, F.; Balis, D.; Shaw, W.; et al. Canagliflozin: A sodium glucose co-transporter 2 inhibitor for the treatment of type 2 diabetes mellitus. Ann. N. Y. Acad. Sci. 2015, 1358, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, P.; Pilon, D.; Robitaille, M.N.; Lafeuille, M.H.; Chow, W.; Pfeifer, M.; Duh, M.S. Real-world glycemic, blood pressure, and weight control in patients with type 2 diabetes mellitus treated with canagliflozin-an electronic health-record-based study. Curr. Med. Res. Opin 2016, 32, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Buysman, E.K.; Chow, W.; Henk, H.J.; Rupnow, M.F. Characteristics and outcomes of patients with type 2 diabetes mellitus treated with canagliflozin: A real-world analysis. BMC Endocr. Disord. 2015, 15, 67. [Google Scholar] [CrossRef] [Green Version]
- Bailey, T.S.; Takács, R.; Tinahones, F.J.; Rao, P.V.; Tsoukas, G.M.; Thomsen, A.B.; Kaltoft, M.S.; Maislos, M. Efficacy and safety of switching from sitagliptin to liraglutide in subjects with type 2 diabetes (LIRA-SWITCH): A randomized, double-blind, double-dummy, active-controlled 26-week trial. Diabetes Obes. Metab. 2016, 18, 1191–1198. [Google Scholar] [CrossRef]
- Buse, J.B.; Sesti, G.; Schmidt, W.E.; Montanya, E.; Chang, C.T.; Xu, Y.; Blonde, L.; Rosenstock, J. Liraglutide Effect Action in Diabetes-6 Study Group. Switching to once-daily liraglutide from twice-daily exenatide further improves glycemic control in patients with type 2 diabetes using oral agents. Diabetes Care 2010, 33, 1300–1303. [Google Scholar] [CrossRef] [Green Version]
- Buse, J.B.; Drucker, D.J.; Taylor, K.L.; Kim, T.; Walsh, B.; Hu, H.; Wilhelm, K.; Trautmann, M.; Shen, L.Z.; Porter, L.E. DURATION-1 Study Group. DURATION-1: Exenatide once weekly produces sustained glycemic control and weight loss over 52 weeks. Diabetes Care 2010, 33, 1255–1261. [Google Scholar] [CrossRef] [Green Version]
- Leiter, L.A.; Forst, T.; Polidori, D.; Balis, D.A.; Xie, J.; Sha, S. Effect of canagliflozin on liver function tests in patients with type 2 diabetes. Diabetes Metab. 2016, 42, 25–32. [Google Scholar] [CrossRef]
- Inoue, M.; Hayashi, A.; Taguchi, T.; Arai, R.; Sasaki, S.; Takano, K.; Inoue, Y.; Shichiri, M. Effects of canagliflozin on body composition and hepatic fat content in type 2 diabetes patients with non-alcoholic fatty liver disease. J. Diabetes Investig. 2019, 10, 1004–1011. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inzucchi, S.E.; Zinman, B.; Fitchett, D.; Wanner, C.; Ferrannini, E.; Schumacher, M.; Schmoor, C.; Ohneberg, K.; Johansen, O.E.; George, J.T.; et al. How Does Empagliflozin Reduce Cardiovascular Mortality? Insights from a Mediation Analysis of the, E.M.PA-REG OUTCOME Trial. Diabetes Care 2018, 41, 356–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Woodward, M.; Perkovic, V.; Figtree, G.A.; Heerspink, H.J.L.; Mahaffey, K.W.; de Zeeuw, D.; Vercruysse, F.; Shaw, W.; Matthews, D.R.; et al. Mediators of the Effects of Canagliflozin on Heart Failure in Patients with Type 2 Diabetes. JACC Heart Fail. 2020, 8, 57–66. [Google Scholar] [CrossRef]
- Bailey, C.J. Uric acid and the cardio-renal effects of, S.G.LT2 inhibitors. Diabetes Obes. Metab. 2019, 21, 1291–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnott, C.; Huang, Y.; Neuen, B.; Di Tanna, G.L.; Cannon, C.P.; Oh, R.; Edwards, R.; Kavalam, M.; Rosenthal, N.; Perkovic, V.; et al. The effect of canagliflozin on amputation risk in the, CANVAS Program and the CREDENCE trial. Diabetes Obes. Metab. 2020. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | CANA 100 MG | Switch to Cana 300 |
|---|---|---|
| Number of patients (n, %) | ||
| Patients with data at V1 | 279 (100%) | 304 (100%) |
| Patients with data at V2 | 265 (95.0%) | 288 (94.7%) |
| Patients with data at V3 | 269 (96.4%) | 294 (96.7%) |
| Follow-up time (months) * | 9.1 (5.3–21.2) | 15.4 (7.3–27.1) |
| Gender (male/female) | 54.8/45.2 | 55.9/44.1 |
| Age (years) | 59.7 (12.4) | 61.1 (10.3) |
| Duration of T2DM (years) * | 10.4 (4.8–15.3) | 12.5 (7.2–17.4) |
| HbA1c (%) | 8.05 (1.53) | 7.51 (1.12) |
| Patients with HbA1c > 7% | 74.8% | 71.1% |
| Fasting plasma glucose (mg/dL) | 163.3 (57.5) | 143.7 (35.9) |
| Weight (kg) | 94.9 (21.1) | 92.0 (21.1) |
| Height (cm) | 165.3 (10.1) | 163.6 (10.3) |
| BMI (kg/m2) | 34.8 (7.2) | 34.5 (7.5) |
| SBP (mmHg) | 138.5 (20.2) | 135.8 (14.5) |
| DBP (mmHg) | 79.2 (10.1) | 77.2 (11.0) |
| Heart rate (bpm) | 84.6 (14.7) | 84.9 (13.0) |
| LDL-C (mg/dL) | 90.5 (39.5) | 79.4 (24.8) |
| HDL-C (mg/dL) | 42.0 (11.1) | 45.0 (13.8) |
| Triglycerides (mg/dL) * | 153.0 (114.0–227.5) | 141.0 (108.0–195.8) |
| Uric acid (mg/dL) | 5.5 (1.5) | 5.1 (1.4) |
| Hematocrit (%) | 44.3 (5.8) | 45.5 (4.1) |
| AST (U/L) * | 21 (16–27) | 20.0 (15.5–25.5) |
| ALT (U/L) * | 25 (18–36) | 23.0 (17.0–30.0) |
| GGT (U/L) * | 35 (22–58) | 28.0 (19.0–44.0) |
| Serum creatinine (mg/dL) | 0.84 (0.21) | 0.85 (0.23) |
| eGFR (mL/min/1.73 m2) | 86.5 (16.4) | 84.9 (17.0) |
| Microalbuminuria (mg/g Cr) * | 7.4 (4.1–31.1) | 8.1 (0.0–26.3) |
| Diabetic renal disease (%) | ||
| Stage G0/G1 | 51.7 | 47.6 |
| Stage G2 | 37.3 | 43.2 |
| Stage G3a | 10.4 | 8.5 |
| Stage G3b | 1.9 | 0.3 |
| Stage G4 | 0 | 0.3 |
| Stage G5 | 0 | 0 |
| Stage A1 | 74.4 | 79.3 |
| Stage A2 | 19.9 | 18.0 |
| Stage A3 | 5.8 | 2.7 |
| Hypertension | 73.5 | 83.6 |
| Hypercholesterolemia | 79.9 | 90.8 |
| Hypertriglyceridemia | 39.6 | 51.8 |
| Combined hyperlipidemia | 35.6 | 48.8 |
| Current smoker | 11.9 | 15.6 |
| Ex-smoker | 31.4 | 35.0 |
| No smoker | 56.7 | 49.3 |
| Sleep apnea | 17.3 | 24.3 |
| Diabetic retinopathy | 13.3 | 18.4 |
| Diabetic renal disease | 20.8 | 27.6 |
| Diabetic neuropathy | 7.9 | 11.5 |
| Coronary artery disease | 8.6 | 10.5 |
| Stroke | 3.9 | 3.6 |
| Peripheral artery disease | 3.2 | 9.2 |
| Arrhythmias | 4.7 | 4.6 |
| Heart failure | 1.8 | 3.0 |
| Left ventricular hypertrophy (echo) | 2.5 | 3.3 |
| Glucose-lowering drugs | ||
| Metformin | 82.8 | 88.8 |
| Sulphonylureas or glinides | 18.6 | 9.9 |
| Pioglitazone | 1.4 | 3.0 |
| DPP-4 inhibitors | 41.6 | 24.3 |
| GLP-1 receptor agonists | 32.3 | 61.2 |
| SGLT-2i | 0 | 100 |
| Dapagliflozin 10 mg | 0 | 51.0 |
| Empagliflozin 10 mg | 0 | 7.3 |
| Empagliflozin 25 mg | 0 | 11.1 |
| Canagliflozin 100 mg | 0 | 30.6 |
| Time with prior SGLT-2i (months) * | 0 | 17.1 |
| Insulin | 38.4 | 42.1 |
| Insulin therapy (years) * | 5.3 (1.9–9.3) | 6.4 (2.6–11.2) |
| Insulin dose(U/d) | 56.5 (34.6) | 46.2 (26.7) |
| Basal (%) | 56.3 | 82.7 |
| Basal-bolus (%) | 43.7 | 17.3 |
| Antihypertensive drugs | ||
| 0 (%) | 31.5 | 21.4 |
| 1 (%) | 22.9 | 28.9 |
| ≥2 (%) | 45.6 | 49.7 |
| ACEis (%) | 32.9 | 31.0 |
| ARBs (%) | 30 | 44.6 |
| Thiazides (%) | 31.7 | 31.3 |
| Loop diuretics (%) | 5.8 | 6.6 |
| Lipid-lowering drugs | ||
| 0 (%) | 25.4 | 12.5 |
| 1 (%) | 64.5 | 73.7 |
| ≥2 (%) | 10.1 | 13.8 |
| V1 | V2 | V3 | p (vs. V1) | |
|---|---|---|---|---|
| CANAGLIFLOZIN 100 MG (n 279) | ||||
| SBP (mmHg) | 138.4 (1.5) | 134.2 (1.0) | 133.8 (1.3) | <0.0001 |
| DBP (mmHg) | 79.2 (0.7) | 77.3 (0.7) | 76.5 (0.7) | <0.01 |
| HR (bpm) | 84.6 (1.2) | 83.3 (1.1) | 83.2 (1.1) | NS |
| FPG (mg/dL) | 163.2 (3.6) | 132.1 (2.6) | 132.7 (2.6) | <0.0001 |
| Hematocrit (%) | 44.3 (0.4) | 46.1 (0.5) | 46.1 (0.4) | <0.0001 |
| LDL-C (mg/dL) | 90.5 (2.5) | 87.2 (1.9) | 83.8 (1.8) | NS (V2) 0.013 (V3) |
| HDL-C (mg/dL) | 42.0 (0.7) | 43.1 (0.7) | 44.6 (0.8) | NS (V2) < 0.0001 (V3) |
| TG (mg/dL) | 189.1 (8.1) | 179.6 (11.0) | 177.1 (10.0) | <0.005 |
| Uric acid (mg/dL) | 5.5 (0.1) | 5.0 (0.1) | 5.0 (0.1) | <0.0001 |
| AST (U/L) | 25.8 (1.2) | 22.5 (0.8) | 23.0 (0.9) | <0.05 |
| ALT (U/L) | 30.6 (1.3) | 26.9 (1.2) | 26.3 (0.9) | <0.0001 |
| GGT (U/L) | 57.5 (5.3) | 41.3 (3.3) | 38.9 (3.0) | <0.0001 |
| eGFR (mL/min) | 86.3 (1.0) | 84.1 (1.2) | 84.4 (1.2) | <0.001 |
| albuminuria (mg/g) | 7.4 (4.1–31.1) | 7.7 (3.0–22.2) | 8.1 (2.0–20.6) | NS |
| SWITCH TO CANAGLIFLOZIN 300 MG (n 304) | ||||
| SBP (mmHg) | 136.4 (0.9) | 132.6 (1.0) | 132.9 (1.1) | <0.005 |
| DBP (mmHg) | 77.0 (0.7) | 75.4 (0.8) | 73.8 (0.6) | NS (V2) < 0.0001 (V3) |
| HR (bpm) | 84.9 (0.9) | 83.8 (0.9) | 83.9 (0.9) | NS |
| FPG (mg/dL) | 144.1 (2.1) | 134.8 (2.2) | 132.7 (2.3) | <0.0001 |
| Hematocrit (%) | 45.5 (0.3) | 45.5 (0.3) | 45.9 (0.3) | NS |
| LDL-C (mg/dL) | 79.4 (1.4) | 78.1 (1.4) | 75.7 (1.3) | NS (V2) 0.031 (V3) |
| HDL-C (mg/dL) | 45.0 (0.8) | 45.7 (0.9) | 46.6 (0.8) | NS (V2) 0.047 (V3) |
| TG (mg/dL) | 172.9 (8.7) | 170.6 (7.1) | 161.4 (6.6) | NS (V2) 0.033 (V3) |
| Uric acid (mg/dL) | 5.1 (0.1) | 5.1 (0.1) | 5.1 (0.1) | NS |
| AST (U/L) | 23.2 (1.3) | 20.9 (1.0) | 21.6 (1.0) | <0.01 |
| ALT (U/L) | 25.9 (0.8) | 24.4 (0.8) | 23.1 (0.7) | <0.005 |
| GGT (U/L) | 41.9 (2.9) | 37.3 (3.1) | 35.8 (2.4) | <0.05 |
| eGFR (mL/min) | 85.4 (1.0) | 85.2 (1.0) | 83.8 (1.0) | NS (V2) 0.006 (V3) |
| albuminuria (mg/g) | 8.1 (0.0–26.3) | 6.4 (0.0–18.1) | 5.8 (0.0–15.4) | <0.001 |
| Drug Class | V1 | V2 | V3 |
|---|---|---|---|
| CANAGLIFLOZIN 100 MG (n 279) | |||
| Metformin (%) | 82.8 | 88.7 | 87.7 |
| Sulphonylureas or glinides (%) | 18.6 | 8.3 | 7.4 |
| Pioglitazone (%) | 1.4 | 1.9 | 1.5 |
| DPP4is (%) | 41.6 | 24.2 | 24.9 |
| GLP-1ras (%) | 32.3 | 47.5 | 49.4 |
| Insulin (%) | 38.4 | 37 | 36.3 |
| Insulin dose (U/d) | 56.5 (34.6) | 48.7 (30.0) * | 45.0 (30.4) * |
| Number of GLDs ** | 2.2 (0.9) | 2.0 (0.9) | 2.0 (0.9) |
| ACEis (%) | 32.9 | 31.6 | 30.9 |
| ARBs (%) | 30.0 | 33.1 | 32.7 |
| Thiazides (%) | 31.7 | 28.3 | 28.0 |
| Loop diuretics (%) | 5.8 | 4.5 | 4.9 |
| Number of antihypertensive drugs | 1.4 (1.2) | 1.4 (1.2) | 1.4 (1.2) |
| Lipid-lowering drugs (%) | 74.6 | 79.8 | 83.2 |
| Number of lipid-lowering drugs | 0.85 (0.6) | 1.0 (0.6) | 1.0 (0.6) |
| SWITCH TO CANAGLIFLOZIN 300 MG (n 304) | |||
| Metformin (%) | 88.8 | 89.7 | 88.8 |
| Sulphonylureas or glinides (%) | 9.9 | 7.9 | 8.8 |
| Pioglitazone (%) | 3 | 3.4 | 11.5 |
| DPP4is (%) | 24.3 | 19.9 | 20.7 |
| GLP-1ras (%) | 61.2 | 65.8 | 70.1 |
| Insulin (%) | 42.1 | 41.4 | 46.4 |
| Insulin dose (U/d) | 46.2 (26.7) | 42.9 (27.1) *** | 41.3 (29.0) *** |
| Number of GLDs | 2.8 (0.9) | 2.2 (0.9) | 2.4 (0.8) |
| ACEis (%) | 31.0 | 29.0 | 27.9 |
| ARBs (%) | 44.6 | 45.7 | 47.3 |
| Thiazides (%) | 31.3 | 28 | 29.2 |
| Loop diuretics (%) | 6.6 | 5.7 | 6.1 |
| Number of antihypertensive drugs | 1.6 (1.2) | 1.6 (1.3) | 1.6 (1.2) |
| Lipid-lowering drugs (%) | 87.5 | 89.7 | 92.5 |
| Number of lipid-lowering drugs | 1.0 (0.5) | 1.1 (0.5) | 1.1 (0.5) |
| CANA100 (n 279) | CANA300 (n 304) | p-Value | |
|---|---|---|---|
| Withdrawals (%) * | 10.8 | 9.2 | 0.534 |
| Deaths (%) | 0 | 0.3 | 1.0 |
| AEs of special interest | |||
| Genital mycotic infections (%) | 11.8 | 9.2 | 0.302 |
| Hypoglycemia (%) | 8.2 | 9.2 | 0.680 |
| Urinary tract infections (%) | 4.7 | 7.2 | 0.191 |
| Intravascular volume-related AEs (%) | 1.4 | 0.3 | 0.148 |
| Fractures (%) | 1.1 | 0 | 0.109 |
| Polyglobulia (%) | 0.4 | 1.0 | 0.916 |
| Ketoacidosis (%) | 0 | 0 | NA |
| Amputations (%) | 0 | 0 | NA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorgojo-Martínez, J.J.; Gargallo-Fernández, M.A.; Galdón Sanz-Pastor, A.; Antón-Bravo, T.; Brito-Sanfiel, M.; Wong-Cruz, J. Real-World Clinical Outcomes Associated with Canagliflozin in Patients with Type 2 Diabetes Mellitus in Spain: The Real-Wecan Study. J. Clin. Med. 2020, 9, 2275. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072275
Gorgojo-Martínez JJ, Gargallo-Fernández MA, Galdón Sanz-Pastor A, Antón-Bravo T, Brito-Sanfiel M, Wong-Cruz J. Real-World Clinical Outcomes Associated with Canagliflozin in Patients with Type 2 Diabetes Mellitus in Spain: The Real-Wecan Study. Journal of Clinical Medicine. 2020; 9(7):2275. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072275
Chicago/Turabian StyleGorgojo-Martínez, Juan J., Manuel A. Gargallo-Fernández, Alba Galdón Sanz-Pastor, Teresa Antón-Bravo, Miguel Brito-Sanfiel, and Jaime Wong-Cruz. 2020. "Real-World Clinical Outcomes Associated with Canagliflozin in Patients with Type 2 Diabetes Mellitus in Spain: The Real-Wecan Study" Journal of Clinical Medicine 9, no. 7: 2275. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072275