Identification and Validation of Circulating Micrornas as Prognostic Biomarkers in Pancreatic Ductal Adenocarcinoma Patients Undergoing Surgical Resection

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population Characteristic
2.1.1. RNA Isolation from Blood Plasma Specimens
2.1.2. Small RNA Libraries Preparation and Next Generation Sequencing
2.1.3. Quantitative Real-Time PCR (qRT-PCR)
2.1.4. Data Normalization and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Poredska, K.; Kunovsky, L.; Prochazka, V.; Dolina, J.; Chovancova, M.; Vlazny, J.; Andrasina, T.; Eid, M.; Jabandziev, P.; Kysela, P. Triple malignancy (NET, GIST and pheochromocytoma) as a first manifestation of neurofibromatosis type-1 in an adult patient. Diag. Pathol. 2019, 14, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A.; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A Randomized Trial of Chemoradiotherapy and Chemotherapy after Resection of Pancreatic Cancer. N. Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neoptolemos, J.P.; Stocken, D.D.; Smith, C.T.; Bassi, C.; Ghaneh, P.; Owen, E.; Moore, M.; Padbury, R.; Doi, R.; Smith, D.; et al. Adjuvant 5-fluorouracil and folinic acid vs observation for pancreatic cancer: Composite data from the ESPAC-1 and -3(v1) trials. Br. J. Cancer 2009, 100, 246–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; E Psarelli, E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; A O’Reilly, D.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Jang, J.-Y.; Kang, M.; Heo, J.S.; Choi, S.H.; Choi, D.W.; Park, S.-J.; Han, S.-S.; Yoon, D.S.; Yu, H.C.; Kang, K.J.; et al. A Prospective Randomized Controlled Study Comparing Outcomes of Standard Resection and Extended Resection, Including Dissection of the Nerve Plexus and Various Lymph Nodes, in Patients with Pancreatic Head Cancer. Ann. Surg. 2014, 259, 656–664. [Google Scholar] [CrossRef] [Green Version]
- Farnell, M.B.; Pearson, R.K.; Sarr, M.G.; DiMagno, E.P.; Burgart, L.J.; Dahl, T.R.; Foster, N.; Sargent, D.; the Pancreas Cancer Working Group. A prospective randomized trial comparing standard pancreatoduodenectomy with pancreatoduodenectomy with extended lymphadenectomy in resectable pancreatic head adenocarcinoma. Surgery 2005, 138, 618–630. [Google Scholar] [CrossRef]
- Zheng, L.; Wolfgang, C.L. Which patients with resectable pancreatic cancer truly benefit from oncological resection: Is it destiny or biology? Cancer Boil. 2015, 16, 360–362. [Google Scholar] [CrossRef] [Green Version]
- Rhim, A.D.; Mirek, E.T.; Aiello, N.M.; Maitra, A.; Bailey, J.M.; McAllister, F.; Reichert, M.; Beatty, G.L.; Rustgi, A.K.; Vonderheide, R.H.; et al. EMT and Dissemination Precede Pancreatic Tumor Formation. Cell 2012, 148, 349–361. [Google Scholar] [CrossRef] [Green Version]
- Strobel, O.; Neoptolemos, J.P.; Jäger, D.; Büchler, M.W. Optimizing the outcomes of pancreatic cancer surgery. Nat. Rev. Clin. Oncol. 2018, 16, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.B.; Lee, S.S.; Kim, J.H.; Kim, H.J.; Byun, J.H.; Hong, S.-M.; Song, K.-B.; Kim, S. Pancreatic Cancer CT: Prediction of Resectability according to NCCN Criteria. Radiology 2018, 289, 710–718. [Google Scholar] [CrossRef] [Green Version]
- Pandiaraja, J.; Viswanathan, S.; Antomy, T.B.; Thirumuruganand, S.; Kumaresan, D.S. The Role of CA19-9 in Predicting Tumour Resectability in Carcinoma Head of Pancreas. J. Clin. Diagn. Res. 2016, 10, PC06–PC09. [Google Scholar] [CrossRef]
- Schanen, B.C.; Li, X. Transcriptional regulation of mammalian miRNA genes. Genomics 2011, 97, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jabandziev, P.; Bohosova, J.; Pinkasova, T.; Kunovsky, L.; Slaby, O.; Goel, A. The Emerging Role of Noncoding RNAs in Pediatric Inflammatory Bowel Disease. Inflamm. Bowel. Dis. 2020, 26, 985–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galatenko, V.V.; Galatenko, A.V.; Samatov, T.R.; Turchinovich, A.A.; Shkurnikov, M.Y.; Makarova, J.A.; Tonevitsky, A.G. Comprehensive network of miRNA-induced intergenic interactions and a biological role of its core in cancer. Sci. Rep. 2018, 8, 2418. [Google Scholar] [CrossRef] [Green Version]
- Vorvis, C.; Koutsioumpa, M.; Iliopoulos, D. Developments in miRNA gene signaling pathways in pancreatic cancer. Futur. Oncol. 2016, 12, 1135–1150. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Ba, Y.; Ma, L.; Cai, X.; Yin, Y.; Wang, K.; Guo, J.; Zhang, Y.; Chen, J.; Guo, X.; et al. Characterization of microRNAs in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [Green Version]
- Weber, J.A.; Baxter, D.H.; Zhang, S.; Huang, D.Y.; Huang, K.H.; Lee, M.-J.; Galas, D.J.; Wang, K. The MicroRNA Spectrum in 12 Body Fluids. Clin. Chem. 2010, 56, 1733–1741. [Google Scholar] [CrossRef]
- McAlexander, M.A.; Phillips, M.J.; Witwer, K.W. Comparison of Methods for miRNA Extraction from Plasma and Quantitative Recovery of RNA from Cerebrospinal Fluid. Front. Genet. 2013, 4, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marabita, F.; De Candia, P.; Torri, A.; Tegnér, J.; Abrignani, S.; Rossi, R.L. Normalization of circulating microRNA expression data obtained by quantitative real-time RT-PCR. Brief. Bioinform. 2015, 17, 204–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karasek, P.; Gablo, N.; Hlavsa, J.; Kiss, I.; Vychytilova-Faltejskova, P.; Hermanová, M.; Kala, Z.; Slaby, O.; Prochazka, V. Pre-operative Plasma miR-21-5p Is a Sensitive Biomarker and Independent Prognostic Factor in Patients with Pancreatic Ductal Adenocarcinoma Undergoing Surgical Resection. Cancer Genom. Proteom. 2018, 15, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Yuan, T.; Tschannen, M.; Sun, Z.; Jacob, H.J.; Du, M.; Liang, M.; Dittmar, R.L.; Liu, Y.; Liang, M.; et al. Characterization of human plasma-derived exosomal RNAs by deep sequencing. BMC Genom. 2013, 14, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Stroese, A.J.; Ullerich, H.; Koehler, G.; Raetzel, V.; Senninger, N.; Dhayat, S.A. Circulating microRNA-99 family as liquid biopsy marker in pancreatic adenocarcinoma. J. Cancer Res. Clin. Oncol. 2018, 144, 2377–2390. [Google Scholar] [CrossRef]
- Dhayat, S.A.; Mardin, W.A.; Seggewiß, J.; Ströse, A.J.; Matuszcak, C.; Hummel, R.; Senninger, N.; Mees, S.T.; Haier, J. MicroRNA Profiling Implies New Markers of Gemcitabine Chemoresistance in Mutant p53 Pancreatic Ductal Adenocarcinoma. PLoS ONE 2015, 10, e0143755. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Dou, H.; Wang, P.; Zhao, S.; Wang, T.; Gong, W.; Zhao, J.; Li, E.; Tan, R.; Hou, Y.; et al. A novel small-molecule compound diaporine A inhibits non-small cell lung cancer growth by regulating miR-99a/mTOR signaling. Cancer Biol. Ther. 2014, 15, 1423–1430. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Chang, L.; Li, Z.; Gao, Q.; Cai, D.; Tian, Y.; Zeng, L.; Li, M. MiR-99a and -99b inhibit cervical cancer cell proliferation and invasion by targeting mTOR signaling pathway. Med. Oncol. 2014, 31, 934. [Google Scholar] [CrossRef]
- Hu, Y.; Zhu, Q.; Tang, L. MiR-99a Antitumor Activity in Human Breast Cancer Cells through Targeting of mTOR Expression. PLoS ONE 2014, 9, e92099. [Google Scholar] [CrossRef]
- Cheng, H.; Xue, J.; Yang, S.; Chen, Y.; Wang, Y.; Zhu, Y.; Wang, X.; Kuang, D.; Ruan, Q.; Duan, Y.; et al. Co-targeting of IGF1R/mTOR pathway by miR-497 and miR-99a impairs hepatocellular carcinoma development. Oncotarget 2017, 8, 47984–47997. [Google Scholar] [CrossRef]
- Kuo, Y.-Z.; Tai, Y.-H.; Lo, H.-I.; Chen, Y.-L.; Cheng, H.-C.; Fang, W.-Y.; Lin, S.-H.; Yang, C.-L.; Tsai, S.-T.; Wu, L.-W. MiR-99a exerts anti-metastasis through inhibiting myotubularin-related protein 3 expression in oral cancer. Oral Dis. 2013, 20, e65–e75. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Shen, J.; Jiang, C.-P.; Liu, B. How to Explain the Contradiction of microRNA 200c Expression and Survival in Solid Tumors?: A Meta-analysis. Asian Pac. J. Cancer Prev. 2014, 15, 3687–3690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, L.; Xiao, X.; Georgikou, C.; Yin, Y.; Liu, L.; Karakhanova, S.; Luo, Y.; Gladkich, J.; Fellenberg, J.; Sticht, C.; et al. MicroRNA-365a-3p inhibits c-Rel-mediated NF-kappaB signaling and the progression of pancreatic cancer. Cancer Lett. 2019, 452, 203–212. [Google Scholar] [CrossRef]
- Cao, Z.; Liu, C.; Xu, J.; You, L.; Wang, C.; Lou, W.; Sun, B.; Miao, Y.; Liu, X.; Wang, X.; et al. Plasma microRNA panels to diagnose pancreatic cancer: Results from a multicenter study. Oncotarget 2016, 7, 41575–41583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, X.; Wei, J.; Huang, Z.; Zhou, X.; Lu, Z.; Zhu, W.; Miao, Y. Identification of a six-miRNA panel in serum benefiting pancreatic cancer diagnosis. Cancer Med. 2019, 8, 2810–2822. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Discovery Cohort | Validation Cohort | |
|---|---|---|
| n (Patients) | 48 | 64 |
| Age | ||
| 65 years | 15 | 24 |
| >65 years | 33 | 40 |
| Sex | ||
| Male | 24 | 24 |
| Female | 24 | 40 |
| Tumor location | ||
| pancreatic head | 38 | 50 |
| pancreatic body/tail | 10 | 14 |
| pT stage | ||
| T2 | 0 | 9 |
| T3 | 48 | 55 |
| pN stage | ||
| N0 | 5 | 20 |
| N1-2 | 43 | 44 |
| pM stage | ||
| M0 | 48 | 64 |
| CA19-9 | ||
| High | 22 | 30 |
| Low | 18 | 20 |
| NA | 8 | 14 |
| Adjuvant chemotherapy | ||
| Yes | 42 | 44 |
| No | 6 | 20 |
| Poor survival group (median 9, range 4–14 months) | 24 | 14 |
| Good survival group (median 27, range 20–47 months) | 24 | 16 |
| microRNA | BaseMean | log2FC | p-Value |
|---|---|---|---|
| miR-99a-5p | 200.59 | −1.19 | 0.001 |
| miR−9-5p | 12.70 | 1.48 | 0.002 |
| miR-365a-3p | 16.54 | −1.75 | 0.002 |
| miR-362-5p | 3.39 | 1.07 | 0.005 |
| miR-627-5p | 4.33 | −1.26 | 0.006 |
| miR-22-3p | 566.82 | −0.61 | 0.006 |
| miR-885-5p | 27.65 | −1.50 | 0.008 |
| miR-1273h-5p | 7.55 | 0.90 | 0.009 |
| miR-940 | 0.89 | 1.49 | 0.011 |
| miR-499a-5p | 2.38 | −1.50 | 0.011 |
| miR-34c-3p | 2.09 | 2.11 | 0.012 |
| miR-200c-3p | 79.59 | 0.49 | 0.012 |
| miR-101-5p | 1.28 | −2.17 | 0.012 |
| miR-18b-3p | 0.66 | −2.01 | 0.014 |
| let-7e-5p | 843.66 | 0.54 | 0.014 |
| miR-30e-5p | 3565.64 | −0.35 | 0.015 |
| miR-100-5p | 99.16 | −0.97 | 0.015 |
| miR-122-5p | 196,465.98 | −1.14 | 0.016 |
| miR-99b-5p | 298.30 | 0.45 | 0.019 |
| let-7b-3p | 9.59 | −1.02 | 0.020 |
| let-7f-5p | 24,401.75 | 0.33 | 0.024 |
| miR-6770-3p | 0.64 | 1.65 | 0.025 |
| miR-181c-5p | 6.71 | 0.81 | 0.026 |
| miR-5010-5p | 9.20 | 0.74 | 0.028 |
| miR-30a-5p | 954.09 | −0.66 | 0.030 |
| miR-4676-3p | 2.38 | 1.11 | 0.030 |
| miR-885-3p | 109.35 | −1.16 | 0.030 |
| miR-193b-3p | 1.43 | −1.69 | 0.034 |
| miR-12135 | 3.27 | 0.95 | 0.035 |
| miR-1275 | 5.86 | −0.69 | 0.037 |
| miR-202-3p | 2.46 | −1.30 | 0.037 |
| miR-552-5p | 2.50 | −1.03 | 0.037 |
| miR-99b-3p | 29.24 | 0.74 | 0.038 |
| miR-210-3p | 14.32 | −0.69 | 0.041 |
| miR-3146 | 2.11 | 1.31 | 0.043 |
| miR-148a-3p | 12,136.24 | −0.66 | 0.043 |
| miR-1249-3p | 0.83 | 2.18 | 0.043 |
| miR-6875-5p | 1.63 | 1.25 | 0.044 |
| miR-6796-5p | 0.68 | 1.51 | 0.045 |
| miR-548bc | 2.49 | 1.47 | 0.046 |
| miR-191-5p | 8975.04 | 0.45 | 0.047 |
| miR-378a-3p | 677.18 | −0.63 | 0.047 |
| miR-224-5p | 485.23 | −0.66 | 0.049 |
| miR-96-5p | 63.60 | −0.78 | 0.050 |
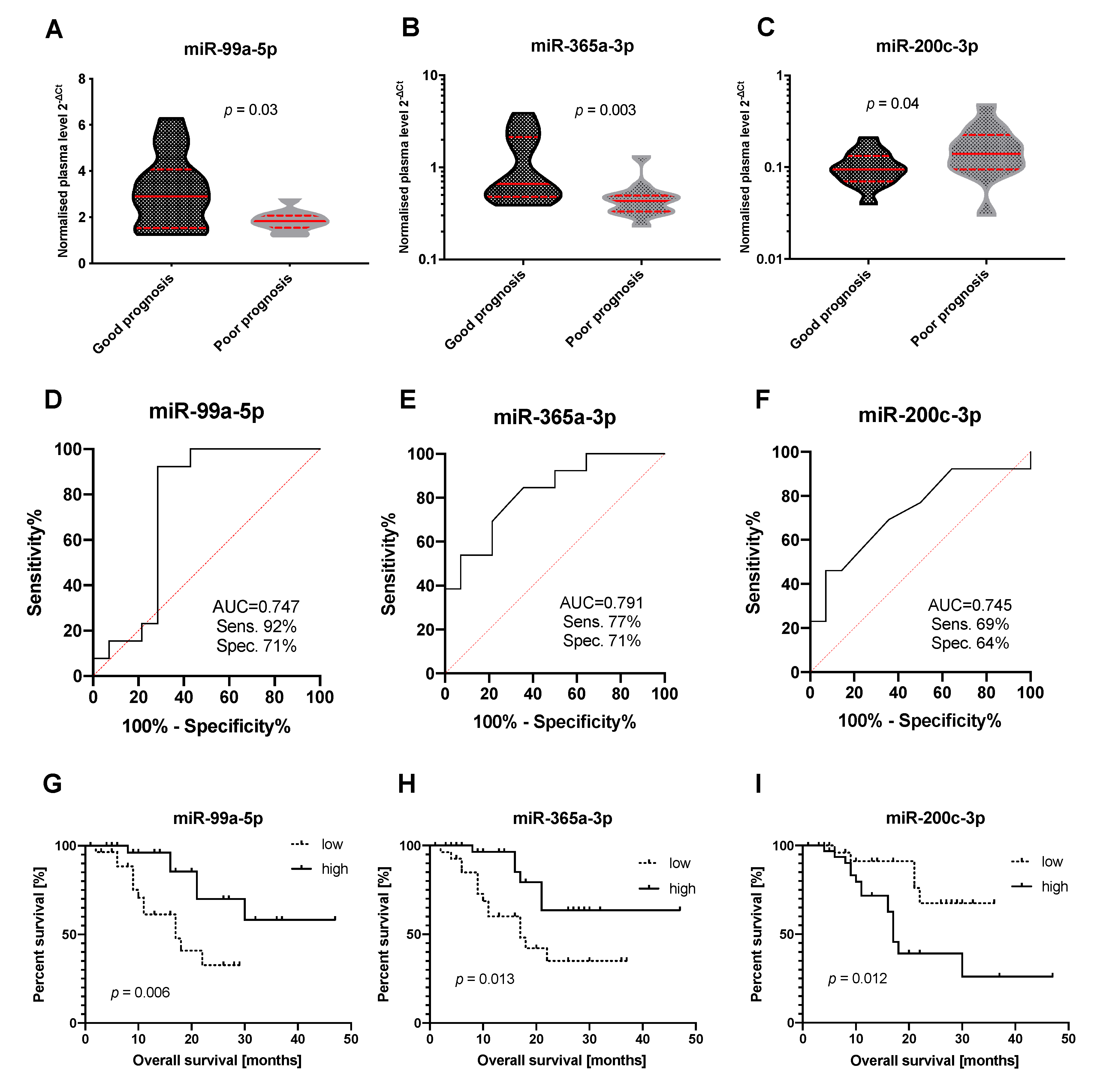
| microRNA | NGS Discovery Cohort | qPCR Group Comparison Validation Cohort | qPCR Survival Analysis Validation Cohort | ||
|---|---|---|---|---|---|
| Log2FC | p-Value | Log2FC | p-Value | p-Value | |
| miR-99a-5p | −1.188 | 0.001 | −1.324 | 0.03 | 0.006 |
| miR-365a-3p | −1.752 | 0.002 | −1.39 | 0.003 | 0.013 |
| miR-200c-3p | 0.493 | 0.012 | 0.766 | 0.04 | 0.012 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gablo, N.; Trachtova, K.; Prochazka, V.; Hlavsa, J.; Grolich, T.; Kiss, I.; Srovnal, J.; Rehulkova, A.; Lovecek, M.; Skalicky, P.; et al. Identification and Validation of Circulating Micrornas as Prognostic Biomarkers in Pancreatic Ductal Adenocarcinoma Patients Undergoing Surgical Resection. J. Clin. Med. 2020, 9, 2440. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082440
Gablo N, Trachtova K, Prochazka V, Hlavsa J, Grolich T, Kiss I, Srovnal J, Rehulkova A, Lovecek M, Skalicky P, et al. Identification and Validation of Circulating Micrornas as Prognostic Biomarkers in Pancreatic Ductal Adenocarcinoma Patients Undergoing Surgical Resection. Journal of Clinical Medicine. 2020; 9(8):2440. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082440
Chicago/Turabian StyleGablo, Natalia, Karolina Trachtova, Vladimir Prochazka, Jan Hlavsa, Tomas Grolich, Igor Kiss, Josef Srovnal, Alona Rehulkova, Martin Lovecek, Pavel Skalicky, and et al. 2020. "Identification and Validation of Circulating Micrornas as Prognostic Biomarkers in Pancreatic Ductal Adenocarcinoma Patients Undergoing Surgical Resection" Journal of Clinical Medicine 9, no. 8: 2440. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082440