Correlation Between Tumor-Associated Macrophage and Immune Checkpoint Molecule Expression and Its Prognostic Significance in Cutaneous Melanoma

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Histopathological Analysis and Immunohistochemistry
2.3. Statistical Analyses
2.4. Variables of Interest
3. Results
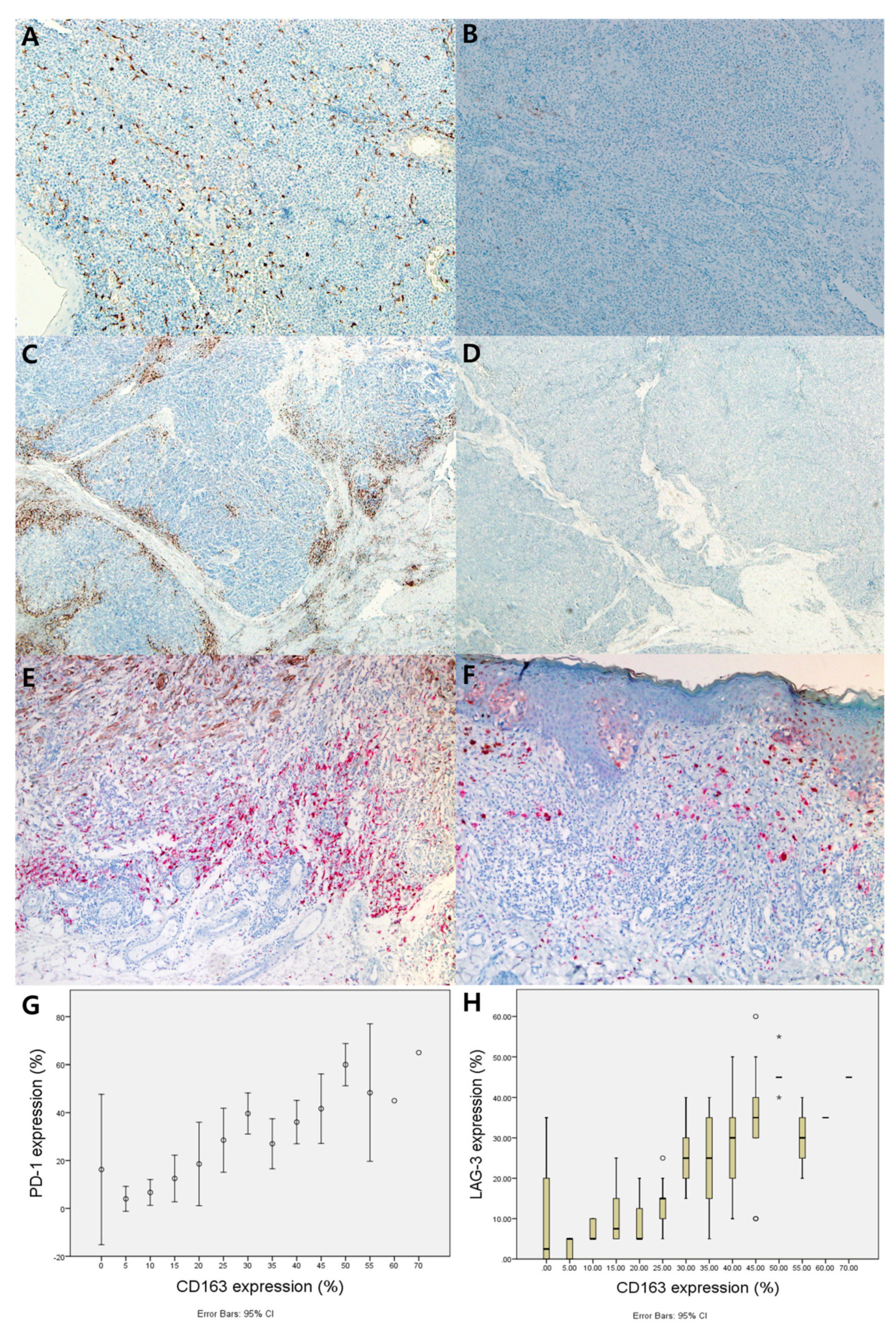
3.1. Correlation between CD163, PD-1, and LAG-3 Expression in Melanoma Tissue
3.2. Expression of CD163, PD-1, LAG-3, and Their Association With Clinicopathological Features
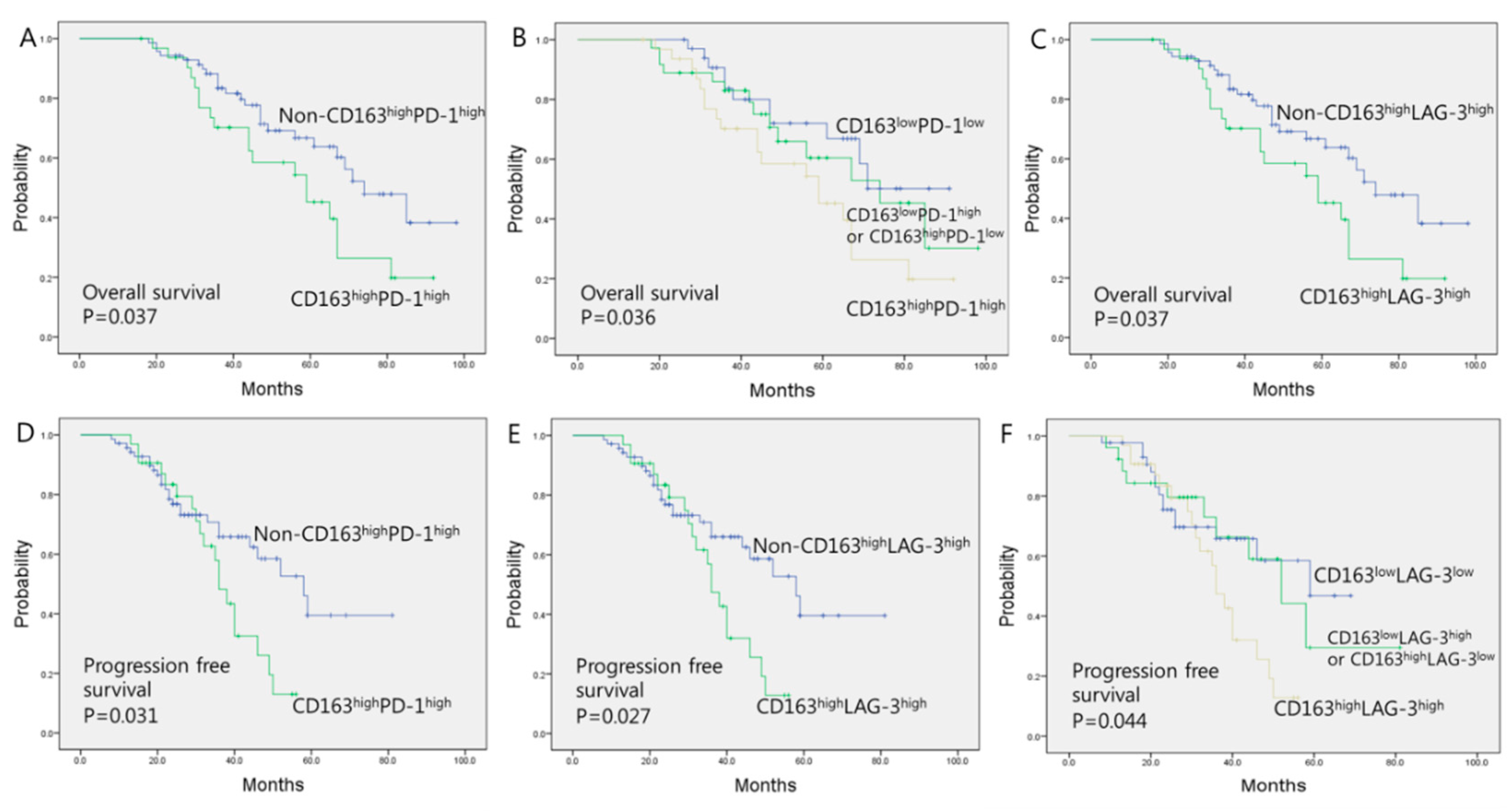
3.3. Prognostic Significance of CD163, PD-1, and LAG-3 Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dong, Y.; Sun, Q.; Zhang, X. PD-1 and its ligands are important immune checkpoints in cancer. Oncotarget 2017, 8, 2171–2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poh, A.R.; Ernst, M. Targeting Macrophages in Cancer: From Bench to Bedside. Front. Oncol. 2018, 8, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Fei, X.; Mao, Y.; Wang, X.; Garfield, D.H.; Huang, O.; Wang, J.; Yuan, F.; Sun, L.; Yu, Q.; et al. PD-1+ immune cell infiltration inversely correlates with survival of operable breast cancer patients. Cancer Immunol. Immunother. 2014, 63, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and anti-CTLA-4 therapies in cancer: mechanisms of action, efficacy, and limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef]
- Grosso, J.F.; Goldberg, M.V.; Getnet, D.; Bruno, T.C.; Yen, H.R.; Pyle, K.J.; Hipkiss, E.; Vignali, D.A.; Pardoll, D.M.; Drake, C.G. Functionally distinct LAG-3 and PD-1 subsets on activated and chronically stimulated CD8 T cells. J. Immunol. 2009, 182, 6659–6669. [Google Scholar] [CrossRef] [Green Version]
- Basu, A.; Yearley, J.H.; Annamalai, L.; Pryzbycin, C.; Rini, B. Association of PD-L1, PD-L2, and immune response markers in matched renal clear cell carcinoma primary and metastatic tissue specimens. Am. J. Clin. Pathol. 2019, 151, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Yuan, A.; Hsiao, Y.J.; Chen, H.Y.; Chen, H.W.; Ho, C.C.; Chen, Y.Y.; Liu, Y.C.; Hong, T.H.; Yu, S.L.; Chen, J.J.; et al. Opposite effects of M1 and M2 macrophage subtypes on lung cancer progression. Sci. Rep. 2015, 5, 14273. [Google Scholar] [CrossRef] [Green Version]
- Etzerodt, A.; Tsalkitzi, K.; Maniecki, M.; Damsky, W.; Delfini, M.; Baudoin, E.; Moulin, M.; Bosenberg, M.; Graversen, J.H.; Auphan-Anezin, N.; et al. Specific targeting of CD163+ TAMs mobilizes inflammatory monocytes and promotes T cell-mediated tumor regression. J. Exp. Med. 2019, 216, 2394–2411. [Google Scholar] [CrossRef]
- Neagu, M. The immune system--a hidden treasure for biomarker discovery in cutaneous melanoma. Adv. Clin. Chem. 2012, 58, 89–140. [Google Scholar]
- Gordon, S.R.; Maute, R.L.; Dulken, B.W.; Hutter, G.; George, B.M.; McCracken, M.N.; Gupta, R.; Tsai, J.M.; Sinha, R.; Corey, D.; et al. PD-1 expression by tumour-associated macrophages inhibits phagocytosis and tumour immunity. Nature 2017, 545, 495–499. [Google Scholar] [CrossRef]
- Chen, L.; Cao, M.F.; Xiao, J.F.; Ma, Q.H.; Zhang, H.; Cai, R.L.; Miao, J.Y.; Wang, W.Y.; Zhang, H.; Luo, M.; et al. Stromal PD-1+ tumor-associated macrophages predict poor prognosis in lung adenocarcinoma. Hum. Pathol. 2020, 97, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Lee, Y.J.; Choi, M.E.; Yun, K.A.; Won, C.H.; Lee, M.W.; Choi, J.H.; Chang, S.E. Expression of lymphocyte-activating gene 3 and T-cell immunoreceptor with immunoglobulin and ITIM domains in cutaneous melanoma and their correlation with programmed cell death 1 expression in tumor-infiltrating lymphocytes. J. Am. Acad. Dermatol. 2019, 81, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, S.D.; Shin, H.; Haining, W.N.; Zou, T.; Workman, C.J.; Polley, A.; Betts, M.R.; Freeman, G.J.; Vignali, D.A.A.; Wherry, E.J. Coregulation of CD8+ T cell exhaustion by multiple inhibitory receptors during chronic viral infection. Nat. Immunol. 2009, 10, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quaranta, V.; Schmid, M.C. Macrophage-mediated subversion of anti-tumour immunity. Cells 2019, 8, 747. [Google Scholar] [CrossRef] [Green Version]
- Gershenwald, J.E.; Scolyer, R.A. Melanoma staging: American Joint Committee on Cancer (AJCC) 8th edition and beyond. Ann. Surg. Oncol. 2018, 25, 2105–2110. [Google Scholar] [CrossRef]
- Lee, W.J.; Lee, M.H.; Kim, H.T.; Won, C.H.; Lee, M.W.; Choi, J.H.; Chang, S.E. Prognostic significance of CD163 expression and its correlation with cyclooxygenase-2 and vascular endothelial growth factor expression in cutaneous melanoma. Melanoma Res. 2019, 29, 501–509. [Google Scholar] [CrossRef]
- Zhao, X.; Qu, J.; Sun, Y.; Wang, J.; Liu, X.; Wang, F.; Zhang, H.; Wang, W.; Ma, X.; Gao, X.; et al. Prognostic significance of tumor-associated macrophages in breast cancer: a meta-analysis of the literature. Oncotarget 2017, 8, 30576–30586. [Google Scholar] [CrossRef] [Green Version]
- Yin, S.; Huang, J.; Li, Z.; Zhang, J.; Luo, J.; Lu, C.; Xu, H.; Xu, H. The prognostic and clinicopathological significance of tumor-associated macrophages in patients with gastric cancer: a meta-analysis. PLoS ONE 2017, 12, e0170042. [Google Scholar] [CrossRef]
- Yuan, X.; Zhang, J.; Li, D.; Mao, Y.; Mo, F.; Du, W.; Ma, X. Prognostic significance of tumor-associated macrophages in ovarian cancer: a meta-analysis. Gynecol. Oncol. 2017, 147, 181–187. [Google Scholar] [CrossRef]
- Yu, M.; Guan, R.; Hong, W.; Zhou, Y.; Lin, Y.; Jin, H.; Hou, B.; Jian, Z. Prognostic value of tumor-associated macrophages in pancreatic cancer: a meta-analysis. Cancer Manag. Res. 2019, 11, 4041–4058. [Google Scholar] [CrossRef] [Green Version]
- Troiano, G.; Caponio, V.C.A.; Adipietro, I.; Tepedino, M.; Santoro, R.; Laino, L.; Lo Russo, L.; Cirillo, N.; Lo Muzio, L. Prognostic significance of CD68+ and CD163+ tumor associated macrophages in head and neck squamous cell carcinoma: a systematic review and meta-analysis. Oral Oncol. 2019, 93, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, T.; Sato, Y.; Tanita, K.; Kambayashi, Y.; Otsuka, A.; Fujisawa, Y.; Yoshino, K.; Matsushita, S.; Funakoshi, T.; Hata, H.; et al. Serum level of soluble CD163 may be a predictive marker of the effectiveness of nivolumab in patients with advanced cutaneous melanoma. Front. Oncol. 2018, 8, 530. [Google Scholar] [CrossRef] [PubMed]
- Cantero-Cid, R.; Casas-Martin, J.; Hernandez-Jimenez, E.; Cubillos-Zapata, C.; Varela-Serrano, A.; Avendano-Ortiz, J.; Casarrubios, M.; Montalban-Hernandez, K.; Villacanas-Gil, I.; Guerra-Pastrian, L.; et al. PD-L1/PD-1 crosstalk in colorectal cancer: are we targeting the right cells? BMC Cancer 2018, 18, 945. [Google Scholar] [CrossRef] [PubMed]
- Man, K.; Gabriel, S.S.; Liao, Y.; Gloury, R.; Preston, S.; Henstridge, D.C.; Pellegrini, M.; Zehn, D.; Berberich-Siebelt, F.; Febbraio, M.A.; et al. Transcription factor IRF4 promotes CD8+ T cell exhaustion and limits the development of memory-like T cells during chronic infection. Immunity 2017, 47, 1129–1141.e5. [Google Scholar] [CrossRef] [Green Version]
- Noy, R.; Pollard, J.W. Tumor-Associated Macrophages: From Mechanisms to Therapy. Immunity 2014, 41, 49–61. [Google Scholar] [CrossRef] [Green Version]
- Deng, W.W.; Mao, L.; Yu, G.T.; Bu, L.L.; Ma, S.R.; Liu, B.; Gutkind, J.S.; Kulkarni, A.B.; Zhang, W.F.; Sun, Z.J. LAG-3 confers poor prognosis and its blockade reshapes antitumor response in head and neck squamous cell carcinoma. Oncoimmunology 2016, 5, e1239005. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.J.; Lee, Y.J.; Shin, H.J.; Won, C.H.; Chang, S.E.; Choi, J.H.; Lee, M.W. Clinicopathological significance of tumor-infiltrating lymphocytes and programmed death-1 expression in cutaneous melanoma: a comparative study on clinical subtypes. Melanoma Res. 2018, 28, 423–434. [Google Scholar] [CrossRef]
- Fourcade, J.; Sun, Z.; Benallaoua, M.; Guillaume, P.; Luescher, I.F.; Sander, C.; Kirkwood, J.M.; Kuchroo, V.; Zarour, H.M. Upregulation of Tim-3 and PD-1 expression is associated with tumor antigen-specific CD8+ T cell dysfunction in melanoma patients. J. Exp. Med. 2010, 207, 2175–2186. [Google Scholar] [CrossRef]
- Tsukamoto, H.; Fujieda, K.; Miyashita, A.; Fukushima, S.; Ikeda, T.; Kubo, Y.; Senju, S.; Ihn, H.; Nishimura, Y.; Oshiumi, H. Combined blockade of IL6 and PD-1/PD-L1 signaling abrogates mutual regulation of their immunosuppressive effects in the tumor microenvironment. Cancer Res. 2018, 78, 5011–5022. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.J.; Ni, L.; Zhang, Y.; Zhang, C.L.; Wu, X.Y.; Atia, A.N.; Thayer, P.; Moorman, J.P.; Yao, Z.Q. PD-1 negatively regulates interleukin-12 expression by limiting STAT-1 phosphorylation in monocytes/macrophages during chronic hepatitis C virus infection. Immunology 2011, 132, 421–431. [Google Scholar] [CrossRef]
- Dhupkar, P.; Gordon, N.; Stewart, J.; Kleinerman, E.S. Anti-PD-1 therapy redirects macrophages from an M2 to an M1 phenotype inducing regression of OS lung metastases. Cancer Med. 2018, 7, 2654–2664. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Ruffell, B.; Chang-Strachan, D.; Chan, V.; Rosenbusch, A.; Ho, C.M.; Pryer, N.; Daniel, D.; Hwang, E.S.; Rugo, H.S.; Coussens, L.M. Macrophage IL-10 blocks CD8+ T cell-dependent responses to chemotherapy by suppressing IL-12 expression in intratumoral dendritic cells. Cancer Cell 2014, 26, 623–637. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Rivard, C.J.; Rozeboom, L.; Yu, H.; Ellison, K.; Kowalewski, A.; Zhou, C.; Hirsch, F.R. Lymphocyte-activation gene-3, an important immune checkpoint in cancer. Cancer Sci. 2016, 107, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Georgoudaki, A.M.; Prokopec, K.E.; Boura, V.F.; Hellqvist, E.; Sohn, S.; Ostling, J.; Dahan, R.; Harris, R.A.; Rantalainen, M.; Klevebring, D.; et al. Reprogramming tumor-associated macrophages by antibody targeting inhibits cancer progression and metastasis. Cell Rep. 2016, 15, 2000–2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Total | CD163High | CD163High PD-1High | CD163High LAG-3High | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 102 | No (n = 55) | Yes (n = 47) | p-value | No (n = 70) | Yes (n = 32) | p-value | No (n = 70) | Yes (n = 32) | p-value | |
| Age (years) | 0.455 | 0.662 | 0.624 | |||||||
| Range | 25–89 | 25–80 | 31–89 | 25–89 | 31–86 | 25–89 | 31–82 | |||
| Mean | 61.8 | 60.8 | 62.1 | 61.4 | 62.0 | 61.3 | 62.4 | |||
| Sex | 0.769 | 0.705 | 0.419 | |||||||
| Male | 57 | 30 (54.5) | 27 (57.4) | 40 (57.1) | 17 (53.1) | 41 (58.6) | 16 (50.0) | |||
| Female | 45 | 25 (45.5) | 20 (42.6) | 30 (42.9) | 15 (46.9) | 29 (41.4) | 16 (50.0) | |||
| Breslow thickness, mm | 0.001 * | 0.001 * | 0.011 * | |||||||
| ≤1 (T1) | 15/55 (27.2) | 6/47 (12.8) | T1 or T2 | T1 or T2 | T1 or T2 | T1 or T2 | ||||
| >1 to ≤2 (T2) | 24/55 (43.6) | 12/47 (25.5) | 47/70 (67.1) | 10/32 (31.3) | 45/70 (64.3) | 12/32 (37.5) | ||||
| >2 to ≤4 (T3) | 10/55 (18.2) | 16/47 (34.0) | T3 or T4 | T3 or T4 | T3 or T4 | T3 or T4 | ||||
| >4 (T4) | 6/55 (10.9) | 13/47 (27.7) | 23/70 (32.9) | 22/32 (68.8) | 25/70 (35.7) | 20/32 (62.5) | ||||
| Ulceration | 0.591 | 0.659 | 0.173 | |||||||
| No | 70 | 39/55 (70.9) | 31/47 (66.0) | 49/70 (70.0) | 21/32 (65.6) | 51/70 (72.9) | 19/32 (59.4) | |||
| Yes | 32 | 16/55 (29.1) | 16/47 (34.0) | 21/70 (30.0) | 11/32 (34.4) | 19/70 (27.1) | 13/32 (40.6) | |||
| Vertical growth phase | 0.001 * | <0.001 * | <0.001 * | |||||||
| No | 61 | 41/55 (74.5) | 20/47 (42.6) | 51/70 (72.9) | 10/32 (31.3) | 50/70 (71.4) | 11/32 (34.4) | |||
| Yes | 41 | 14/55 (25.5) | 27/47 (57.4) | 19/70 (27.1) | 22/32 (68.8) | 20/70 (28.6) | 21/32 (65.6) | |||
| Lymph node involvement | 0.005 * | 0.033 * | 0.008 * | |||||||
| No | 80 | 49/55 (89.1) | 31/47 (66.0) | 59/70 (84.3) | 21/32 (65.6) | 60/70 (85.7) | 20/32 (62.5) | |||
| Yes | 22 | 6/55 (10.9) | 16/47 (34.0) | 11/70 (15.7) | 11/32 (34.4) | 10/70 (14.3) | 12/32 (37.5) | |||
| Visceral involvement | 0.087 | 0.048 * | 0.237 | |||||||
| No | 94 | 53/55 (96.4) | 41/47 (87.2) | 67/70 (95.7) | 27/32 (84.4) | 66/70 (94.3) | 28/32 (87.5) | |||
| Yes | 8 | 2/55 (3.6) | 6/47 (12.8) | 3/70 (4.3) | 5/32 (15.6) | 4/70 (5.7) | 4/32 (12.5) | |||
| AJCC stage | 0.012 * | 0.028 * | 0.007 * | |||||||
| I/II | 75 | 46/55 (83.6) | 29/47 (61.7) | 56/70 (80.0) | 19/32 (59.4) | 57/70 (81.4) | 18/32 (56.3) | |||
| III/IV | 27 | 9/55 (16.4) | 18/47 (38.3) | 14/70 (20.0) | 13/32 (40.6) | 13/70 (18.6) | 14/32 (43.8) | |||
| PD-1 Expression, n (%) | LAG-3 Expression, n (%) | |||||
|---|---|---|---|---|---|---|
| Low Expression (n = 49) | High Expression (n = 53) | p-Value | Low Expression (n = 58) | High Expression (n = 44) | p-Value | |
| CD163 expression | 0.003 * | <0.001 * | ||||
| Low expression (n = 55) | 34/49 (69.4) | 21/53 (39.6) | 43/58 (74.1) | 12/44 (27.3) | ||
| High expression (n = 47) | 15/49 (30.6) | 32/53 (60.4) | 15/58 (25.9) | 32/44 (72.7) | ||
| Mean OS (95% CI) (Months) | Mean PFS (95% CI) (Months) | |
|---|---|---|
| A) CD163lowPD-1low expression (n = 34) | 70.94 (61.78–80.10) | 51.48 (43.41–59.55) |
| B) Either CD163lowPD-1high or CD163highPD-1low expression (n = 36) | 68.17 (57.36–78.98) | 50.46 (39.54–61.39) |
| C) CD163highPD-1high expression (n = 32) | 57.57 (48.49–66.66) | 37.06 (32.24–41.87) |
| D) CD163lowLAG-3low expression (n = 44) | 68.53 (60.20–76.85) | 50.19 (42.83–57.57) |
| E) Either CD163lowLAG-3high or CD163highLAG-3low expression (n = 26) | 70.35 (57.80–82.89) | 50.93 (38.74–63.12) |
| F) CD163highLAG-3high expression (n = 32) | 57.57 (48.49–66.66) | 36.89 (32.06–41.72) |
| Overall (n = 102) | 66.86 (60.67–73.05) | 48.39 (42.26–54.53) |
| p-value | ||
| A, B, C separately | 0.036 *,§ | 0.026 *,§ |
| C versus. others | 0.037 *,§§ | 0.031 *,§§ |
| D, E, F separately | 0.064 ǂ | 0.044 *,ǂ |
| F versus. others | 0.037 *,ǂǂ | 0.027 *,ǂǂ |
| Univariate analysis | ||||||
|---|---|---|---|---|---|---|
| OS | PFS | |||||
| Covariate | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Age (years) | ||||||
| <60 vs. ≥60 | 0.92 | 0.68–2.93 | 0.328 | 1.10 | 0.68–1.78 | 0.624 |
| Sex | ||||||
| Female vs. Male | 1.84 | 0.67–3.28 | 0.412 | 1.28 | 0.79–4.57 | 0.492 |
| AJCC stage | ||||||
| Early vs. Advanced | 2.41 | 1.24–4.28 | 0.023 * | 2.19 | 1.14–5.37 | 0.045 * |
| Involvement of LN | ||||||
| Yes vs. No | 1.69 | 1.10–5.63 | 0.037 * | 1.13 | 1.16–5.74 | 0.041 * |
| Amelanosis | ||||||
| Yes vs. No | 0.69 | 0.23–4.69 | 0.333 | 0.71 | 0.29–5.19 | 0.572 |
| Breslow thickness | ||||||
| T1 | 0.75 | 0.35–0.82 | 0.027 * | 0.52 | 0.31–0.81 | 0.031 * |
| T2 | 0.82 | 0.05–1.18 | 0.141 | 0.86 | 0.23–1.11 | 0.062 |
| T3 | 1.88 | 1.16–5.23 | 0.029 * | 1.52 | 1.14–6.32 | 0.041 * |
| T4 | 2.41 | 1.11-4.82 | 0.018 * | 1.99 | 1.19–5.81 | 0.039 * |
| CD163 expression | ||||||
| Yes vs. No | 2.62 | 1.39–4.88 | 0.033* | 2.71 | 1.13–4.16 | 0.159 |
| LAG-3 expression | ||||||
| High vs. Low | 2.11 | 1.21–5.20 | 0.037* | 2.07 | 1.13–5.31 | 0.041 * |
| PD-1 expression | ||||||
| High vs. Low | 1.09 | 0.59–4.75 | 0.421 | 1.13 | 0.85–4.92 | 0.280 |
| CD163highPD-1high | 2.31 | 1.21–5.11 | 0.029* | 1.88 | 1.07–5.09 | 0.043 * |
| CD163highLAG-3high | 2.03 | 1.18–5.44 | 0.032 * | 2.08 | 1.14–5.25 | 0.038 * |
| Multivariate analysis | ||||||
| AJCC stage | ||||||
| Early vs. Advanced | 1.89 | 1.21–4.59 | 0.042 * | 1.87 | 1.11–4.21 | 0.051 |
| Involvement of LN | ||||||
| Yes vs. No | 1.12 | 0.82–4.19 | 0.156 | 1.17 | 0.65–3.84 | 0.147 |
| Breslow thickness | ||||||
| T1 | 0.88 | 0.43–0.91 | 0.043 * | 0.92 | 0.55–0.98 | 0.047 * |
| T2 | 0.89 | 0.27–1.47 | 0.117 | 0.84 | 0.33–1.61 | 0.215 |
| T3 | 1.16 | 1.08–5.14 | 0.088 | 1.21 | 1.03–4.22 | 0.174 |
| T4 | 1.89 | 0.041 * | 1.61 | 1.10-4.87 | 0.063 | |
| CD163 expression | ||||||
| High vs. Low | 2.38 | 1.16–4.74 | 0.040 * | 2.19 | 1.06–5.08 | 0.188 |
| LAG-3 expression | ||||||
| High vs. Low | 1.99 | 1.19–5.44 | 0.044 * | 1.87 | 1.10–5.01 | 0.061 |
| CD163highPD-1high | 2.08 | 1.14–5.57 | 0.042 * | 1.76 | 1.08–5.46 | 0.066 |
| CD163highLAG-3high | 1.88 | 1.16–5.87 | 0.044 * | 1.54 | 1.07–5.13 | 0.046 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.J.; Won, C.H.; Lee, M.W.; Choi, J.H.; Chang, S.E.; Lee, W.J. Correlation Between Tumor-Associated Macrophage and Immune Checkpoint Molecule Expression and Its Prognostic Significance in Cutaneous Melanoma. J. Clin. Med. 2020, 9, 2500. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082500
Kim YJ, Won CH, Lee MW, Choi JH, Chang SE, Lee WJ. Correlation Between Tumor-Associated Macrophage and Immune Checkpoint Molecule Expression and Its Prognostic Significance in Cutaneous Melanoma. Journal of Clinical Medicine. 2020; 9(8):2500. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082500
Chicago/Turabian StyleKim, Young Jae, Chong Hyun Won, Mi Woo Lee, Jee Ho Choi, Sung Eun Chang, and Woo Jin Lee. 2020. "Correlation Between Tumor-Associated Macrophage and Immune Checkpoint Molecule Expression and Its Prognostic Significance in Cutaneous Melanoma" Journal of Clinical Medicine 9, no. 8: 2500. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082500