Methylphenidate in Autism Spectrum Disorder: A Long-Term Follow Up Naturalistic Study

 ,
,
Abstract
:1. Introduction
1.1. ASD and ADHD
1.2. Psychotropic Drugs in ASD
1.3. MPH in ADHD with Comorbid ASD
2. Materials and Methods
2.1. Participants and Procedures
2.2. Statistical Analysis
3. Results
3.1. MPH Treatment
3.2. Primary Outcomes
3.2.1. CGI Measures
3.2.2. C-GAS Measures
3.2.3. Other Psychotropic Medications at the Last Follow-Up
3.2.4. Safety
3.2.5. Discontinuation Rate
3.3. Secondary Outcomes
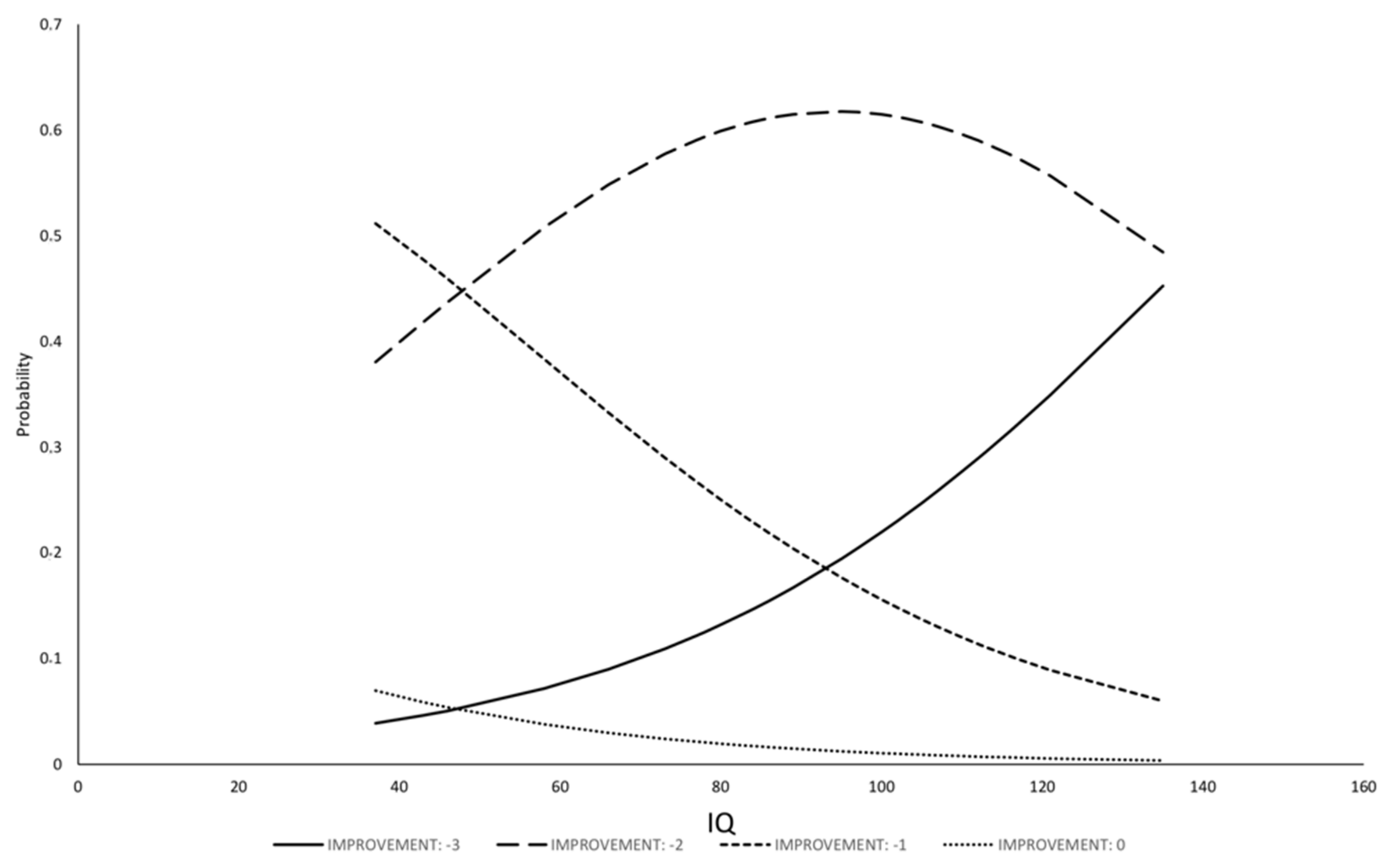
3.3.1. Evaluation of Factors to Predict Amelioration in Severity of the Illness
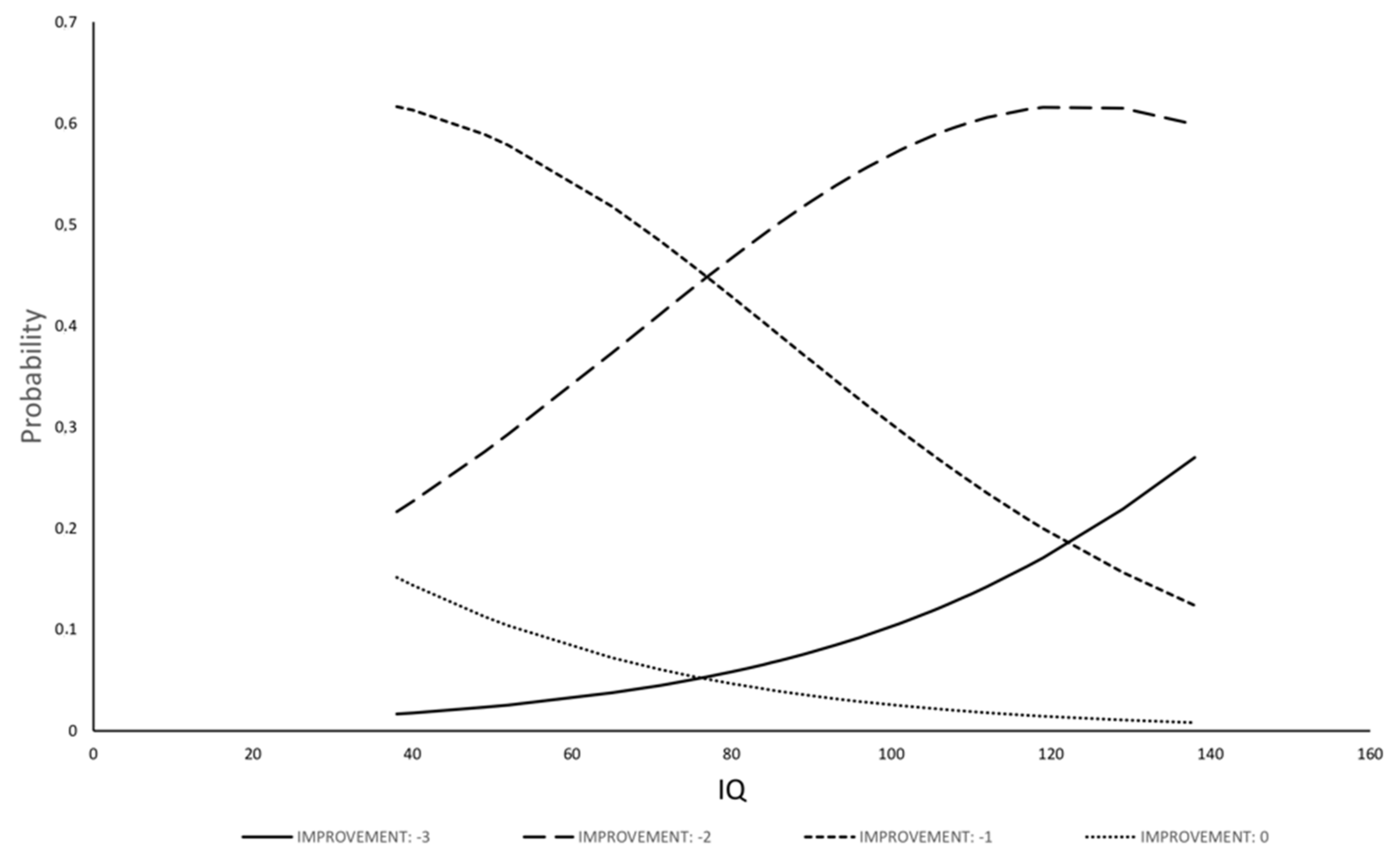
3.3.2. Evaluation of Factors to Predict Clinical Improvement
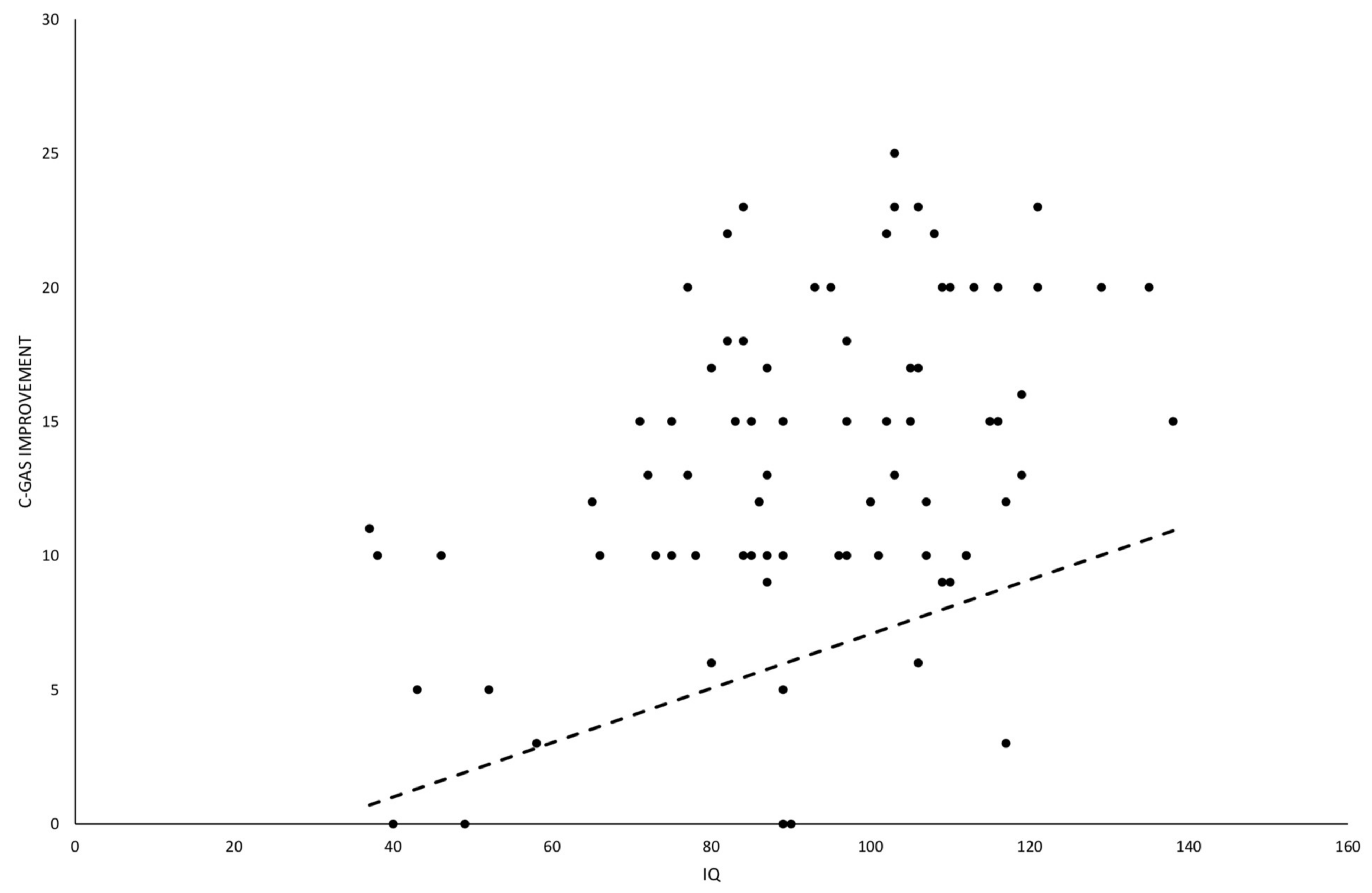
3.3.3. Evaluation of Factors to Predict Amelioration in Global Functioning
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5; American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- Baio, J.; Wiggins, L.; Christensen, D.L.; Maenner, M.J.; Daniels, J.; Warren, Z.; Kurzius-Spencer, M.; Zahorodny, W.; Robinson Rosenberg, C.; White, T.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2018, 67, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.R.; Gonda, X.; Tarazi, F.I. Autism Spectrum Disorder: Classification, diagnosis and therapy. Pharmacol. Ther. 2018, 190, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Christensen, D.L.; Maenner, M.J.; Bilder, D.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M.; Pettygrove, S.D.; Robinson, C.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 4 Years—Early Autism and Developmental Disabilities Monitoring Network, Seven Sites, United States, 2010, 2012, and 2014. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2019, 68, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, D. ADHD in children and young people: Prevalence, care pathways, and service provision. Lancet. Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (In Text Rev.), DSM-IV-TR, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Reiersen, A.M.; Todd, R.D. Co-occurrence of ADHD and autism spectrum disorders: Phenomenology and treatment. Expert Rev. Neurother. 2008, 8, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Gargaro, B.A.; Rinehart, N.J.; Bradshaw, J.L.; Tonge, B.J.; Sheppard, D.M. Autism and ADHD: How far have we come in the comorbidity debate? Neurosci. Biobehav. Rev. 2011, 35, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Rieske, R.D.; Williams, L.W. The relationship between autism spectrum disorders and attention-deficit/hyperactivity disorder: An overview. Res. Dev. Disabil. 2013, 34, 2475–2484. [Google Scholar] [CrossRef]
- Howes, O.D.; Rogdaki, M.; Findon, J.L.; Wichers, R.H.; Charman, T.; King, B.H.; Loth, E.; McAlonan, G.M.; McCracken, J.T.; Parr, J.R.; et al. Autism spectrum disorder: Consensus guidelines on assessment, treatment and research from the British Association for Psychopharmacology. J. Psychopharmacol. 2018, 32, 3–29. [Google Scholar] [CrossRef]
- Antshel, K.M.; Russo, N. Autism Spectrum Disorders and ADHD: Overlapping Phenomenology, Diagnostic Issues, and Treatment Considerations. Curr. Psychiatry Rep. 2019, 21, 34. [Google Scholar] [CrossRef]
- Grzadzinski, R.; Di Martino, A.; Brady, E.; Mairena, M.A.; O’Neale, M.; Petkova, E.; Lord, C.; Castellanos, F.X. Examining Autistic Traits in Children with ADHD: Does the Autism Spectrum Extend to ADHD? J. Autism Dev. Disord. 2011, 41, 1178–1191. [Google Scholar] [CrossRef] [Green Version]
- Craig, F.; Lamanna, A.L.; Margari, F.; Matera, E.; Simone, M.; Margari, L. Overlap Between Autism Spectrum Disorders and Attention Deficit Hyperactivity Disorder: Searching for Distinctive/Common Clinical Features. Autism Res. 2015, 8, 328–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antshel, K.M.; Zhang-James, Y.; Wagner, K.E.; Ledesma, A.; Faraone, S.V. An update on the comorbidity of ADHD and ASD: A focus on clinical management. Expert Rev. Neurother. 2016, 16, 279–293. [Google Scholar] [CrossRef] [PubMed]
- Colombi, C.; Ghaziuddin, M. Neuropsychological Characteristics of Children with Mixed Autism and ADHD. Autism Res. Treat. 2017, 2017, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronald, A.; Simonoff, E.; Kuntsi, J.; Asherson, P.; Plomin, R. Evidence for overlapping genetic influences on autistic and ADHD behaviours in a community twin sample. J. Child Psychol. Psychiatry 2008, 49, 535–542. [Google Scholar] [CrossRef]
- Lichtenstein, P.; Carlström, E.; Råstam, M.; Gillberg, C.; Anckarsäter, H. The genetics of autism spectrum disorders and related neuropsychiatric disorders in childhood. Am. J. Psychiatry 2010, 167, 1357–1363. [Google Scholar] [CrossRef] [Green Version]
- Rommelse, N.N.; Franke, B.; Geurts, H.M.; Hartman, C.A.; Buitelaar, J.K. Shared heritability of attention-deficit/hyperactivity disorder and autism spectrum disorder. Eur. Child Adolesc. Psychiatry 2010, 19, 281–295. [Google Scholar] [CrossRef] [Green Version]
- Serretti, A.; Fabbri, C. Shared genetics among major psychiatric disorders. Lancet 2013, 381, 1339–1341. [Google Scholar] [CrossRef]
- Taylor, M.J.; Martin, J.; Lu, Y.; Brikell, I.; Lundström, S.; Larsson, H.; Lichtenstein, P. Association of Genetic Risk Factors for Psychiatric Disorders and Traits of These Disorders in a Swedish Population Twin Sample. JAMA Psychiatry 2019, 76, 280–289. [Google Scholar] [CrossRef]
- Craig, F.; Margari, F.; Legrottaglie, A.; Palumbi, R.; De Giambattista, C. A review of executive function deficits in autism spectrum disorder and attention-deficit/hyperactivity disorder. Neuropsychiatr. Dis. Treat. 2016, 12, 1191. [Google Scholar]
- Lukito, S.; Jones, C.; Pickles, A.; Baird, G.; Happé, F.; Charman, T.; Simonoff, E. Specificity of executive function and theory of mind performance in relation to attention-deficit/hyperactivity symptoms in autism spectrum disorders. Mol. Autism 2017, 8, 60. [Google Scholar] [CrossRef] [Green Version]
- Demetriou, E.A.; Lampit, A.; Quintana, D.S.; Naismith, S.L.; Song, Y.; Pye, J.E.; Hickie, I.; Guastella, A.J. Autism spectrum disorders: A meta-analysis of executive function. Mol. Psychiatry 2018, 23, 1198–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guttmann-Steinmetz, S.; Gadow, K.D.; DeVincent, C.J.; Crowell, J. Anxiety symptoms in boys with autism spectrum disorder, attention-deficit hyperactivity disorder, or chronic multiple tic disorder and community controls. J. Autism Dev. Disord. 2010, 40, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.A.; Landa, R.J. Association between severity of behavioral phenotype and comorbid attention deficit hyperactivity disorder symptoms in children with autism spectrum disorders. Autism 2014, 18, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.J.; Manangan, C.N.; Dauterman, H.A.; Davis, H.N. ADHD symptoms moderate the relation between ASD status and internalizing symptoms in 3-6-year-old children. J. Autism Dev. Disord. 2014, 44, 1347–1356. [Google Scholar] [CrossRef]
- Mansour, R.; Dovi, A.T.; Lane, D.M.; Loveland, K.A.; Pearson, D.A. ADHD severity as it relates to comorbid psychiatric symptomatology in children with Autism Spectrum Disorders (ASD). Res. Dev. Disabil. 2017, 60, 52–64. [Google Scholar] [CrossRef] [Green Version]
- Thomas, S.; Sciberras, E.; Lycett, K.; Papadopoulos, N.; Rinehart, N. Physical Functioning, Emotional, and Behavioral Problems in Children With ADHD and Comorbid ASD: A Cross-Sectional Study. J. Atten. Disord. 2018, 22, 1002–1007. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, L.; Bilenberg, N.; Thomsen Ernst, M.; Abitz Boysen, S.; Pottegård, A. Use of Psychotropic Drugs among Children and Adolescents with Autism Spectrum Disorders in Denmark: A Nationwide Drug Utilization Study. J. Clin. Med. 2018, 7, 339. [Google Scholar] [CrossRef] [Green Version]
- Coury, D.L.; Anagnostou, E.; Manning-Courtney, P.; Reynolds, A.; Cole, L.; McCoy, R.; Whitaker, a.; Perrin, J.M. Use of Psychotropic Medication in Children and Adolescents With Autism Spectrum Disorders. Pediatrics 2012, 130 (Suppl. 2), S69–S76. [Google Scholar] [CrossRef] [Green Version]
- Mohiuddin, S.; Ghaziuddin, M. Psychopharmacology of autism spectrum disorders: A selective review. Autism Int. J. Res. Pract. 2013, 17, 645–654. [Google Scholar] [CrossRef]
- Murray, M.L.; Hsia, Y.; Glaser, K.; Simonoff, E.; Murphy, D.G.M.; Asherson, P.J.; Eklund, H.; Wong, I.C.K. Pharmacological Treatments Prescribed to People With Autism Spectrum Disorder (ASD) in Primary Health Care. Psychopharmacology 2014, 231, 1011–1021. [Google Scholar] [CrossRef] [Green Version]
- Hong, M.P.; Erickson, C.A. Investigational drugs in early-stage clinical trials for autism spectrum disorder. Expert Opin. Investig. Drugs 2019, 28, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Anagnostou, E. Clinical trials in autism spectrum disorder: Evidence, challenges and future directions. Curr. Opin. Neurol. 2018, 31, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E.; Phillips, A.; Chaplin, W.; Zagursky, K.; Novotny, S.; Wasserman, S.; Iyengar, R. A placebo controlled crossover trial of liquid fluoxetine on repetitive behaviors in childhood and adolescent autism. Neuropsychopharmacology 2005, 30, 582–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, S.; Waschbusch, D.A.; Pelham, W.E.; Frankland, B.W.; Andrade, B.F.; Jacques, S.; Corkum, P.V. Social information processing in elementary-school aged children with ADHD: Medication effects and comparisons with typical children. J. Abnorm. Child Psychol. 2009, 37, 579–589. [Google Scholar] [CrossRef]
- Findling, R.L.; Mankoski, R.; Timko, K.; Lears, K.; McCartney, T.; McQuade, R.D.; Eudicone, J.M.; Amatniek, J.; Marcus, R.N.; Sheehan, J.J. A Randomized Controlled Trial Investigating the Safety and Efficacy of Aripiprazole in the Long-Term Maintenance Treatment of Pediatric Patients With Irritability Associated With Autistic Disorder. J. Clin. Psychiatry 2014, 75, 22–30. [Google Scholar] [CrossRef]
- Young, S.; Sedgwick, O.; Fridman, M.; Gudjonsson, G.; Hodgkins, P.; Lantigua, M.; González, R.A. Co-morbid psychiatric disorders among incarcerated ADHD populations: A meta-analysis. Psychol. Med. 2015, 45, 2499–2510. [Google Scholar] [CrossRef] [Green Version]
- Levine, S.; Kodesh, A.; Goldberg, Y.; Reichenberg, A.; Furukawa, T.; Kolevzon, A.; Leucht, S. Initial severity and efficacy of risperidone in autism: Results from the RUPP trial. Eur. Psychiatry 2016, 32, 16–20. [Google Scholar] [CrossRef]
- Sturman, N.; Deckx, L.; van Driel, M.L. Methylphenidate for children and adolescents with autism spectrum disorder. Cochrane Database Syst. Rev. 2017, 11, CD011144. [Google Scholar] [CrossRef]
- Goel, R.; Hong, J.S.; Findling, R.L.; Ji, N.Y. An update on pharmacotherapy of autism spectrum disorder in children and adolescents. Int. Rev. Psychiatry 2018, 30, 78–95. [Google Scholar] [CrossRef]
- Smith, T.; Aman, M.G.; Arnold, L.E.; Silverman, L.B.; Lecavalier, L.; Hollway, J.; Tumuluru, R.; Hyman, S.L.; Buchan-Page, K.A.; Hellings, J.; et al. Atomoxetine and Parent Training for Children With Autism and Attention-Deficit/Hyperactivity Disorder: A 24-Week Extension Study. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Arnold, L.E.; Ober, N.; Aman, M.G.; Handen, B.; Smith, T.; Pan, H.; Hyman, S.L.; Hollway, J.; Lecavalier, L.; Page, K.; et al. A 1.5-Year Follow-Up of Parent Training and Atomoxetine for Attention-Deficit/Hyperactivity Disorder Symptoms and Noncompliant/Disruptive Behavior in Autism. J. Child. Adolesc. Psychopharmacol. 2018, 28, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Banas, K.; Sawchuk, B. Clonidine as a Treatment of Behavioural Disturbances in Autism Spectrum Disorder: A Systematic Literature Review. J. Can. Acad. Child Adolesc. Psychiatry 2020, 29, 110–120. [Google Scholar] [PubMed]
- Scahill, L.; McCracken, J.T.; King, B.H.; Rockhill, C.; Shah, B.; Politte, L.; Sanders, R.; Minjarez, M.; Cowen, J.; Mullett, J.; et al. Extended-Release Guanfacine for Hyperactivity in Children With Autism Spectrum Disorder. Am. J. Psychiatry 2015, 172, 1197–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, M. Pharmacotherapy in early infantile autism. Biol. Psychiatry 1981, 10, 399–423. [Google Scholar]
- Sporn, A.; Pinsker, H. Use of stimulant medication in treating pervasive developmental disorder. Am. J. Psychiatry 1981, 138, 997. [Google Scholar]
- Schmidt, K. The effect of stimulant medication in childhood-onset pervasive developmental disorder—A case report. J. Dev. Behav. Pediatrics 1982, 3, 244–246. [Google Scholar] [CrossRef]
- Volkmar, F.R.; Hoder, E.L.; Cohen, D.J. Inappropriate uses of stimulant medications. Clin. Paediatr. 1985, 24, 127–130. [Google Scholar] [CrossRef]
- Realmuto, G.M.; August, G.J.; Garfinkel, B.D. Clinical effect of buspirone in autistic children. J. Clin. Psychopharmacol. 1989, 9, 122–125. [Google Scholar] [CrossRef]
- Quintana, H.; Birmaher, B.; Stedge, D.; Lennon, S.; Freed, J.; Bridge, J.; Greenhill, L. Use of methylphenidate in the treatment of children with autistic disorder. J. Autism Dev. Disord. 1995, 25, 283–294. [Google Scholar] [CrossRef]
- Handen, B.L.; Johnson, C.R.; Lubetsky, M. Efficacy of methylphenidate among children with autism and symptoms of attention-deficit hyperactivity disorder. J. Autism Dev. Disord. 2000, 30, 245–255. [Google Scholar] [CrossRef]
- Di Martino, A.; Melis, G.; Cianchetti, C.; Zuddas, A. Methylphenidate for Pervasive Developmental Disorders: Safety and Efficacy of Acute Single Dose Test and Ongoing Therapy: An Open-Pilot Study. J. Child Adolesc. Psychopharmacol. 2004, 14, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Santosh, P.J.; Baird, G.; Pityaratstian, N.; Tavare, E.; Gringras, P. Impact of comorbid autism spectrum disorders on stimulant response in children with attention deficit hyperactivity disorder: A retrospective and prospective effectiveness study. Child Care Health Dev. 2006, 32, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Posey, D.J.; Aman, M.G.; McCracken, J.T.; Scahill, L.; Tierney, E.; Arnold, L.E.; Vitiello, B.; Chuang, S.Z.; Davies, M.; Ramadan, Y.; et al. Positive effects of methylphenidate on inattention and hyperactivity in pervasive developmental disorders: An analysis of secondary measures. Biol. Psychiatry 2007, 61, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Ghuman, J.K.; Aman, M.G.; Lecavalier, L.; Riddle, M.A.; Gelenberg, A.; Wright, R.; Ghuman, H.S.; Fort, C. Randomized, placebo-controlled, crossover study of methylphenidate for attention-deficit/hyperactivity disorder symptoms in preschoolers with developmental disorders. J. Child Adolesc. Psychopharmacol. 2009, 19, 329–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahromi, L.B.; Kasari, C.L.; McCracken, J.T.; Lee, L.S.; Aman, M.G.; McDougle, C.J.; Scahill, L.; Tierney, E.; Arnold, L.E.; Vitiello., B.; et al. Positive Effects of Methylphenidate on Social Communication and Self-Regulation in Children with Pervasive Developmental Disorders and Hyperactivity. J. Autism Dev. Disord. 2009, 39, 395–404. [Google Scholar] [CrossRef]
- Pearson, D.A.; Santos, C.W.; Aman, M.G.; Arnold, L.E.; Casat, C.D.; Mansour, R.; Lane, D.M.; Loveland, K.A.; Bukstei, G.; Jerger, S.W.; et al. Effects of Extended Release Methylphenidate Treatment on Ratings of Attention-Deficit/Hyperactivity Disorder (ADHD) and Associated Behavior in Children with Autism Spectrum Disorders and ADHD Symptoms. J. Child Adolesc. Psychopharmacol. 2013, 23, 337–351. [Google Scholar] [CrossRef]
- Research Units on Pediatric Psychopharmacology Autism Network. Randomized, controlled, crossover trial of methylphenidate in pervasive developmental disorders with hyperactivity. Randomized Control. Trial Arch. Gen. Psychiatry 2005, 62, 1266–1274. [Google Scholar] [CrossRef]
- Reichow, B.; Volkmar, F.R.; Bloch, M.H. Systematic review and meta-analysis of pharmacological treatment of the symptoms of attention-deficit/hyperactivity disorder in children with pervasive developmental disorders. J. Autism Dev. Disord. 2013, 43, 2435–2441. [Google Scholar] [CrossRef] [Green Version]
- McDougle, C.J.; Scahill, L.; Aman, M.G.; McCracken, J.T.; Tierney, E.; Davies, M.; Arnold, L.E.; Posey, D.J.; Martin, A.; Ghuman, J.K.; et al. Risperidone for the core symptom domains of autism: Results from the study by the autism network of the research units on pediatric psychopharmacology. Am. J. Psychiatry 2005, 162, 1142–1148. [Google Scholar] [CrossRef]
- Kim, S.J.; Shonka, S.; French, W.P.; Strickland, J.; Miller, L.; Stein, M.A. Dose-Response Effects of Long-Acting Liquid Methylphenidate in Children with Attention Deficit/Hyperactivity Disorder (ADHD) and Autism Spectrum Disorder (ASD): A Pilot Study. J. Autism Dev. Disord. 2017, 47, 2307–2313. [Google Scholar] [CrossRef]
- Storebø, O.J.; Pedersen, N.; Ramstad, E.; Kielsholm, M.L.; Nielsen, S.S.; Krogh, H.B.; Moreira-Maia, C.R.; Magnusson, F.L.; Holmskov, M.; Gerner, T.; et al. Methylphenidate for attention deficit hyperactivity disorder (ADHD) in children and adolescents—Assessment of adverse events in non-randomised studies. Cochrane Database Syst. Rev. 2018, 9, CD012069. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Maia, C.R.; Cortese, S.; Caye, A.; Kuhn Deakin, T.; Polanczyk, G.V.; Polanczyk, C.A.; Paim Rohde, L.A. Long-Term Efficacy of Methylphenidate Immediate-Release for the Treatment of Childhood ADHD. J. Atten. Disord. 2017, 21, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Conners, C.K.; Sitarenios, G.; Parker, J.D.; Epstein, J.N. The Revised Conners’ Parent Rating Scale (CPRS-R): Factor Structure, Reliability, and Criterion Validity. J. Abnorm. Child. Psychol. 1998, 26, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S.L. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual (Part I): Modules 1–4; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Lord, C.; Luyster, R.J.; Gotham, K.; Guthrie, W. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual (Part II): Toddler Module; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism Diagnostic Interview-Revised Manual; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Gillberg, C.; Gillberg, C.; Råstam, M.; Wentz, E. The Asperger Syndrome (And High-Functioning Autism) Diagnostic Interview (ASDI): A Preliminary Study of a New Structured Clinical Interview. Autism 2001, 5, 57–66. [Google Scholar] [CrossRef]
- Wechsler, D. The Wechsler Preschool and Primary Scale of Intelligence, Third Edition (WPPSI-Ill); The Psychological Corporation: San Antonio, TX, USA, 2002. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children- Fourth Edition: Canadian (WISC-IV); Psychological Corporation Ed.: Toronto, ON, Canada, 2005. [Google Scholar]
- Farmer, C. Leiter International Performance Scale-Revised (Leiter-R). In Encyclopedia of Autism Spectrum Disorders; Springer: New York, NY, USA, 2013. [Google Scholar]
- Achenbach, T.M.; Edelbrock, C. Manual for the Child Behavior Checklist and Revised Child Behavior Profile; University of Vermont Press: Burlington, VT, USA, 1983. [Google Scholar]
- Busner, J.; Targum, S.D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry (Edgmont) 2007, 4, 28–37. [Google Scholar]
- Shaffer, D.; Gould, M.S.; Brasic, J.; Ambrosini, P.; Fisher, P.; Bird, H.; Aluwahlia, S. A children’s global assessment scale (CGAS). Arch. Gen. Psychiatry 1983, 40, 1228–1231. [Google Scholar] [CrossRef]
- Grizenko, N.; Qi Zhang, D.D.; Polotskaia, A.; Joober, R. Efficacy of Methylphenidate in ADHD Children across the Normal and the Gifted Intellectual Spectrum. J. Can. Acad. Child Adolesc. Psychiatry 2012, 21, 282–288. [Google Scholar]
- Tarrant, N.; Roy, M.; Deb, S.; Odedra, S.; Retzer, A.; Roy, A. The effectiveness of methylphenidate in the management of Attention Deficit Hyperactivity Disorder (ADHD) in people with intellectual disabilities: A systematic review. Res. Dev. Disabil. 2018, 83, 217–232. [Google Scholar] [CrossRef]
- Marcus, S.C.; Durkin, M. Stimulant adherence and academic performance in urban youth with attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 480–489. [Google Scholar] [CrossRef]
- Stigler, K.A.; Desmond, L.A.; Posey, D.J.; Wiegand, R.E.; McDougle, C.J. A naturalistic retrospective analysis of psychostimulants in pervasive developmental disorders. J. Child Adolesc. Psychopharmacol. 2004, 14, 49–56. [Google Scholar] [CrossRef]
- Birmaher, B.; Quintana, H.; Greenhill, L.L. Case Study Methylphenidate treatment of hyperactive autistic children. J. Am. Acad. Child Adolesc. Psychiatry 1988, 27, 248–251. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ASD + ADHD Group (n = 40) | ADHD Group (n = 40) | p-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Sex | |||||
| M | 32 | 80 | 28 | 70 | |
| F | 8 | 20 | 12 | 30 | 0.3047 |
| Median | 95% CI | Median | 95% CI | ||
| Age (years) | 15.5 | 14–17 | 15 | 14–17 | 0.7502 |
| n | % | n | % | ||
| ASD level | |||||
| 1 | 34 | 85 | |||
| 2 | 4 | 10 | |||
| 3 | 2 | 5 | |||
| ADHD severity level | |||||
| Severe | 12 | 30 | 14 | 35 | 0.6352 |
| Moderate | 28 | 70 | 26 | 65 | |
| ADHD specifiers | |||||
| Inattentive | 8 | 20 | 6 | 15 | 0.5587 |
| Combined | 32 | 80 | 34 | 85 | |
| Median | 95% CI | Median | 95% CI | ||
| Intelligence Quotient (IQ) | 89.5 | 84.33–101.66 | 98.5 | 86.33–104.32 | 0.4558 |
| n | % | n | % | ||
| Comorbidities | |||||
| Learning disorder | 31 | 77.5 | 32 | 80 | |
| Motor coordination disorder | 11 | 27.5 | 2 | 5 | |
| Sleep–wake disorder | 10 | 25 | 11 | 27.5 | |
| Anxiety disorder | 9 | 22.5 | 6 | 15 | |
| Oppositional defiant disorder | 6 | 15 | 32 | 80 | |
| Disruptive mood dysregulation disorder | 5 | 12.5 | 8 | 20 | |
| Other psychotropic medications | |||||
| Antipsychotics (FGA and SGA) | 11 | 27.5 | 7 | 17.5 | |
| Mood stabilizer | 4 | 10 | 5 | 12.5 | |
| Antidepressants | 2 | 5 | 1 | 2.5 | |
| Anxiolytics | 1 | 2.5 | 0 | 0 | |
| Melatonin | 8 | 20 | 9 | 22.5 | |
| ADHD + ASD | ADHD | p-Value | |||
|---|---|---|---|---|---|
| Age of therapy onset (Years) | Median (IQR) | 95% CI | Median (IQR) | 95% CI | 0.2309 |
| 9 (7–13) | 7–10 | 10 (8.5–13) | 9–11.6 | ||
| MPH dose (mg/kg/day) | 0.6 (0.46–0.7) | 0.5–0.7 | 0.6 (0.46–0.825) | 0.52–0.7 | 0.6026 |
| Therapy duration (months) | 36 (24–78) | 24–78 | 48 (36–57.97) | 24–72 | 0.5679 |
| CGI-S | ASD + ADHD Group | ADHD Group | p-Value |
|---|---|---|---|
| T0 | n = 40 | n = 40 | |
| Median Range (95% CI) | 5 4–7 (5–6) | 5 4–7 (5–6) | 0.5609 |
| T1 | n = 40 | n = 40 | |
| Median Range (95% CI) | 5 3–7 (4.5–5) | 5 3–6 (4–5) | 0.1138 |
| T6 | n = 39 | n = 40 | |
| Median Range (95% CI) | 4 2–7 (4–5) | 4 2–6 (3–4) | 0.0501 |
| T24 | n = 37 | n = 39 | |
| Median Range (95% CI) | 4 2–5 (3.4–4) | 3 2–6 (3–4) | 0.1104 |
| p-value (T0–T24) | <0.0001 | <0.0001 | |
| CGI-I | ASD + ADHD group | ADHD group | p-value |
| T1 | n = 40 | n = 40 | |
| Median Range (95% CI) | 3 2–5 (3–3) | 3 2–4 (3–3) | 0.9715 |
| T6 | n = 39 | n = 40 | |
| Median Range (95% CI) | 3 2–6 (2–3) | 2 2–4 (2–3) | 0.594 |
| T24 | n = 37 | n = 39 | |
| Median Range (95% CI) | 2 1–4 (2–3) | 2 1–4 (2–3) | 0.8116 |
| p-value (T1–T24) | 0.00001 | <0.00001 | |
| CGI-E | ASD + ADHD group | ADHD group | p-value |
| Median Range (95% CI) | 2 0.25–3 (1.5–2) | 2 0.5–4 (1.5–2) | 0.7986 |
| ASD + ADHD Group | ADHD Group | p-Value | |
|---|---|---|---|
| T0 Median Range (95% CI) | 43 25–50 (40–45) | 45 30–55 (45–47.66) | 0.0632 |
| Last follow-up Median Range (95% CI) | 55 25–70 (50–58.32) | 60 40–70 (55–64.32) | 0.0907 |
| p-value (T0–T24) | <0.0001 | <0.0001 |
| ASD + ADHD Group n (%) | ADHD Group n (%) | p-Value | |
|---|---|---|---|
| Loss of appetite | 19 (47.5) | 23 (57.5) | 0.9865 |
| Abdominal discomfort | 18 (45) | 14 (35) | 0.9792 |
| Headache | 10 (25) | 6 (15) | 0.8147 |
| Irritability | 4 (10) | 3 (7.5) | 1 |
| Palpitation | 3 (7.5) | 1 (2.5) | 0.9974 |
| Restlessness | 3 (7.5) | 1 (2.5) | 0.9974 |
| Anxiety | 2 (5) | 0 | 0.97 |
| Insomnia | 1 (2.5) | 2 (5) | 1 |
| Dizziness | 1 (2.5) | 1 (2.5) | 1 |
| Drowsiness | 0 | 0 | 1 |
| Tic disorder | 0 | 0 | 1 |
| Hallucinations | 0 | 0 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ventura, P.; de Giambattista, C.; Spagnoletta, L.; Trerotoli, P.; Cavone, M.; Di Gioia, A.; Margari, L. Methylphenidate in Autism Spectrum Disorder: A Long-Term Follow Up Naturalistic Study. J. Clin. Med. 2020, 9, 2566. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082566
Ventura P, de Giambattista C, Spagnoletta L, Trerotoli P, Cavone M, Di Gioia A, Margari L. Methylphenidate in Autism Spectrum Disorder: A Long-Term Follow Up Naturalistic Study. Journal of Clinical Medicine. 2020; 9(8):2566. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082566
Chicago/Turabian StyleVentura, Patrizia, Concetta de Giambattista, Laura Spagnoletta, Paolo Trerotoli, Maddalena Cavone, Alessandra Di Gioia, and Lucia Margari. 2020. "Methylphenidate in Autism Spectrum Disorder: A Long-Term Follow Up Naturalistic Study" Journal of Clinical Medicine 9, no. 8: 2566. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082566