Clusterin as a New Marker of Kidney Injury in Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation—A Pilot Study †

 , , and
, , and
Abstract
:1. Introduction
2. Aim of Study
3. Material and Methods
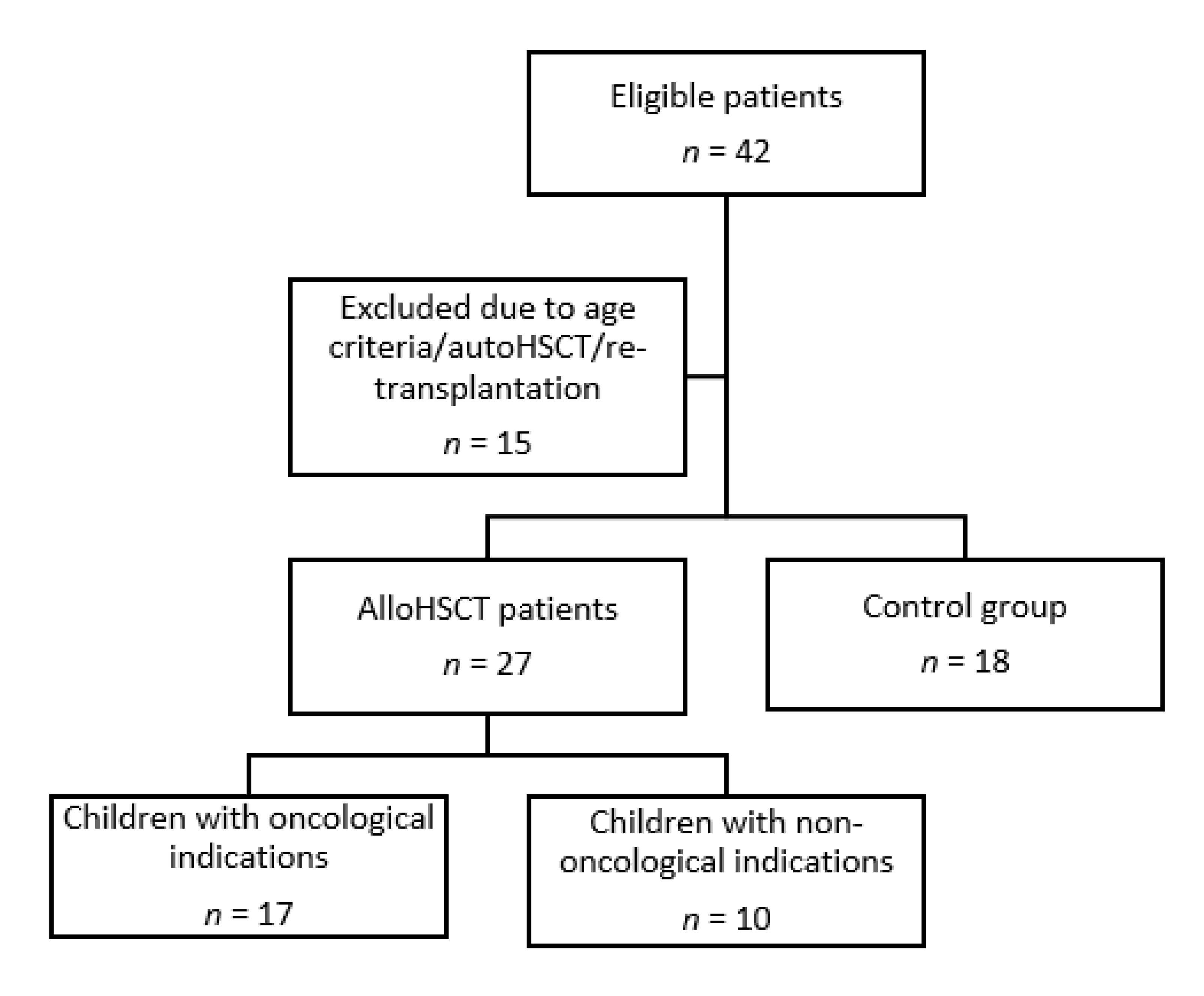
3.1. Study Design and Settings
3.2. Methods
3.3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Standards
References
- Mamoulakis, C.; Tsarouhas, K.; Fragkiadoulaki, I.; Heretis, I.; Wilks, M.; Spandidos, D.; Tsitsimpikou, C.; Tsatsakis, A. Contrast-induced nephropathy: Basic concepts, pathophysiological implications and prevention strategies. Pharmacol. Ther. 2017, 180, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Mamoulakis, C.; Fragkiadoulaki, I.; Karkala, P.; Georgiadis, G.; Zisis, I.E.; Stivaktakis, P.; Kalogeraki, A.; Tsiaoussis, T.; Burykina, T.; Lazopoulos, G.; et al. Contrast-indiced nephropathy in an animal model: Evaluation of novel biomarkers in blood and tissue samples. Toxicol. Rep. 2019, 6, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Tsarouhas, K.; Tsitsimpikou, C.; Papantoni, X.; Lazaridou, D.; Koutouzis, M.; Mazzaris, S.; Rezaee, R.; Mamoulakis, C.; Georgoulias, P.; Nepka, C.; et al. Oxidative stress and kidney injury in trans-radial catheterization. Biomed. Rep. 2018, 8, 417–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chevalier, R.L. The proximal tubule is the primary target of injury and progression of kidney disease: Role of the glomerulotubular junction. Am. J. Physiol. Renal Physiol. 2016, 311, F145–F161. [Google Scholar] [CrossRef]
- Koh, K.N.; Sunkara, A.; Kang, G. Acute Kidney Injury in Pediatric Patients Receiving Allogeneic Hematopoietic Cell Transplantation: Incidence, Risk Factors, and Outcomes. Biol. Blood Marrow Transplant. 2018, 24, 758–764. [Google Scholar] [CrossRef] [Green Version]
- Raina, R.; Herrera, N.; Krishnappa, V.; Sethi, S.K.; Deep, A.; Kao, W.; Bunchman, T.; Abu-Arja, R. Hematopoietic stem cell transplantation and acute kidney injury in children: A comprehensive review. Pediatr. Transplant. 2017, 21, e12935. [Google Scholar] [CrossRef]
- Didsbury, M.S.; Mackie, F.E.; Kennedy, S.E. A systematic review of acute kidney injury in pediatric allogeneic hematopoietic stem cell recipients. Pediatr. Transplant. 2015, 19, 460–470. [Google Scholar] [CrossRef]
- Kizilbash, S.J.; Kashtan, C.E.; Chavers, B.M.; Cao, Q.; Smith, A.R. Acute kidney injury and the risk of mortality in children undergoing hematopoietic stem cell transplantation. Biol. Blood Marrow Transplant. 2016, 22, 1264–1270. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, S.M.; Byrnes, J.J.; Kothari, M.; Longhurst, C.A.; Dutta, S.; Garcia, P.; Goldstein, S.L. AKI in hospitalized children: Comparing the pRIFLE, AKIN, and KDIGO definitions. Clin. J. Am. Soc. Nephrol. 2015, 10, 554–561. [Google Scholar] [CrossRef] [Green Version]
- Haase, M.; Kellum, J.A.; Ronco, C. Subclinical AKI—An emerging syndrome with important consequences. Nat. Rev. Nephrol. 2012, 8, 735–739. [Google Scholar] [CrossRef]
- Ronco, C.; Kellum, J.A.; Haase, M. Subclinical AKI is still AKI. Crit. Care 2012, 16, 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, R.K.; Wong, H.R.; Krawczeski, C.D.; Wheeler, D.S.; Manning, P.B.; Chawla, L.S.; Devarajan, P.; Goldstein, S.L. Combining functional and tubular damage biomarkers improves diagnostic precision for acute kidney injury after cardiac surgery. J. Am. Coll. Cardiol. 2014, 64, 2753–2762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benoit, S.W.; Dixon, B.P.; Goldstein, S.L.; Bennett, M.R.; Lane, A.; Lounder, D.T.; Rotz, S.J.; Gloude, N.J.; Lake, K.E.; Litts, B.; et al. A novel strategy for identifying early acute kidney injury in pediatric hematopoietic stem cell transplantation. Bone Marrow Transplant. 2019, 54, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Kanduri, S.R.; Cheungpasitporn, W.; Thongprayoon, C.; Bathini, T.; Kovvuru, K.; Garla, V.; Medaura, J.; Vaitla, P.; Kashani, K.B. Incidence and mortality of acute kidney injury in patients undergoing hematopoietic stem cell transplantation: A systematic review and meta-analysis. QJM 2020. [Google Scholar] [CrossRef] [PubMed]
- Caliskan, Y.; Besisik, S.K.; Sargin, D.; Ecder, T. Early renal injury after myeloablative allogeneic and autologous hematopoietic cell transplantation. Bone Marrow Transplant. 2006, 38, 141–147. [Google Scholar] [CrossRef] [Green Version]
- Basu, R.K. Targeting acute kidney injury: Can an innovative approach to existing and novel biomarkers shift the paradigm? Nephron 2019, 143, 207–210. [Google Scholar] [CrossRef]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.H.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Cachat, F.; Combescure, C.; Cauderay, M.; Girardin, E.; Chehade, H. A systematic review of glomerular hyperfiltration assessment and definition in the medical literature. Clin. J. Am. Soc. Nephrol. 2015, 10, 382–389. [Google Scholar] [CrossRef]
- Iduoriyekemwen, N.J.; Ibadin, M.O.; Aikhionbare, H.A.; Idogun, S.E.; Abiodun, M.T. Glomerular hyperfiltration in excess weight adolescents. Niger. J. Clin. Pract. 2019, 22, 842–848. [Google Scholar] [CrossRef]
- Zhou, W.; Guan, Q.; Kwan, C.C.H.; Chen, H.; Gleave, M.E.; Nguan, C.Y.C.; Du, C. Loss of clusterin expression worsens renal ischemia-reperfusion injury. Am. J. Physiol. Renal Physiol. 2010, 298, F568–F578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, J.; Guan, Q.; Liu, X.; Wang, H.; Gleave, M.E.; Nguan, C.Y.C.; Du, C. Relationship of clusterin with renal inflammation and fibrosis after the recovery phase of ischemia-reperfusion injury. BMC Nephrol. 2016, 17, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.S.; Song, S.H.; Kim, J.H.; Jeon, Y.K.; Kim, B.H.; Kang, M.-C.; Chun, S.W.; Hong, S.H.; Chung, M.; Kim, Y.K.; et al. Urine clusterin/apolipoprotein J is linked to tubular damage and renal outcomes in patients with type 2 diabetes mellitus. Clin. Endocrinol. 2017, 87, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Yang, J.; Sarwal, R.D.; Sigdel, T.K.; Liberto, J.; Damm, I.; Louie, V.; Sigdel, S.; Livingstone, D.; Soh, K.; et al. A novel multi-biomarker assay for non-invasive quantitative monitoring of kidney injury. J. Clin. Med. 2019, 8, 499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da, Y.; Akalya, K.; Murali, T.; Vathsala, A.; Tan, C.-S.; Low, S.; Lim, H.-N.; Teo, B.-W.; Lau, T.; Ong, L.; et al. Serial quantification of urinary protein biomarkers to predict drug-induced acute kidney injury. Curr. Drug Metab. 2019, 20, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Sarveazad, A.; Ali, K.M.; Yousefifard, M.; Hosseini, M. Accuracy of urine kidney injury molecule-1 in predicting acute kidney injury in children; a systematic review and meta-analysis. Arch. Acad. Emerg. Med. 2020, 8, e44. [Google Scholar] [PubMed]
- Humphreys, B.D.; Xu, F.; Sabbisetti, V.; Grgic, I.; Naini, S.M.; Wang, N.; Chen, G.; Xiao, S.; Patel, D.; Henderson, J.M.; et al. Chronic epithelial kidney injury molecule-1 expression causes murine kidney fibrosis. J. Clin. Investig. 2013, 123, 4023–4035. [Google Scholar] [CrossRef] [Green Version]
- Kwatra, N.S.; Meany, H.J.; Ghelani, S.J.; Zahavi, D.; Pandya, N.; Majd, M. Glomerular hyperfiltration in children with cancer: Prevalence and a hypothesis. Pediatr. Radiol. 2017, 47, 221–226. [Google Scholar] [CrossRef]
- Filler, G.; Lee, M. Educational review: Measurement of GFR in special populations. Pediatr. Nephrol. 2018, 33, 2037–2046. [Google Scholar] [CrossRef]
- Young, J.; Dahale, D.; Demmel, K.; O’Brien, M.; Geller, J.I.; Courter, J.; Haslam, D.B.; Danziger-Isakov, L.; Goldstein, S.L. Reducing acute kidney injury in pediatric oncology patients: An improvement project targeting nephrotoxic medications. Pediatr. Blood Cancer 2020, 67, e28396. [Google Scholar] [CrossRef]
- Georgiadis, G.; Zisis, I.-E.; Docea, A.O.; Tsarouhas, K.; Fragkiadoulaki, I.; Mavridis, C.; Karavitakis, M.; Stratakis, S.; Stylianou, K.; Tsitsimpikou, C.; et al. Current concepts on the reno-protective effects of phosphodiesterase 5 inhibitors in acute kidney injury: Systematic search and review. J. Clin. Med. 2020, 9, 1284. [Google Scholar] [CrossRef] [PubMed]
- Iordache, A.M.; Buga, A.M.; Albulescu, D.; Vasile, R.C.; Mitrut, R.; Georgiadis, G.; Zisis, I.-E.; Mamoulakis, C.; Tsatsakis, A.; Docea, A.O.; et al. Phosphodiesterase-5 inhibitors ameliorate structural kidney damage in a rat model of contrast-induced nephropathy. Food Chem. Toxicol. 2020, 143, 111535. [Google Scholar] [CrossRef] [PubMed]
- Nakhjavan-Shahraki, B.; Yousefifard, M.; Ataei, N.; Baikpour, M.; Ataei, F.; Bazargani, B.; Abbasi, A.; Ghelichkhani, P.; Javidilarijani, F.; Hosseini, M. Accuracy of cystatin C in prediction of acute kidney injury in children; serum or urine levels: Which one works better? A systematic review and meta-analysis. BMC Nephrol. 2017, 18, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| eGFR (mL/min/1.73 m2) Median Value (Interquartile Range) | Before alloHSCT | 24 h after alloHSCT | 1 Week after alloHSCT | 2 Weeks after alloHSCT | 3 Weeks after alloHSCT | 4 Weeks after alloHSCT |
|---|---|---|---|---|---|---|
| Oncological patients | 142 (112–149) a | 183 (153–216) a,b | 172 (155–205) a,b | 188 (166–195) a,b | 149 (140–174) a,b,c | 134 (123–149) a,c |
| Non-oncological patients | 107 (96–129) | 140 (126–176) b | 131 (118–149) b | 130 (114–136) b | 129 (100–145) b | 126 (92–134) |
| Serum Parameter Median Value (Interquartile Range) | s Clusterin (ng/mL) | s KIM1 (ng/mL) | s Cystatin C (ng/mL) |
|---|---|---|---|
| Control group | 1.3 (1.2–1.4) | 2.3 (2.2–2.4) | 148 (141.7–164.3) |
| Before alloHSCT | 3.1 (3.0–3.1) a | 4.2 (4.1–4.3) a | 408 (387.6–433) a |
| 24 hafter alloHSCT | 7.9 (7.2–8.4) a,b | 6.7 (6.3–6.8) a,b | 634.8 (604.6–689.1) a,b |
| 1 week after alloHSCT | 8.9 (8.8–9.1) a,c | 6.7 (6.0–6.8) a | 905.6 (879–961.6) a,c |
| 2 weeks after alloHSCT | 9.5 (9.3–10) a,d | 8 (7.8–8.2) a,d | 898 (878.7–926.3) a |
| 3 weeks after alloHSCT | 13.3 (12.8–13.6) a,e | 8.9 (8.8–8.9) a,e | 1106 (1053–1157) a,e |
| 4 weeks after alloHSCT | 13.3 (12.8–13.6) a | 9.2 (9.1–9.2) a,f | 1262 (1222–1288) a,f |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musiał, K.; Augustynowicz, M.; Miśkiewicz-Migoń, I.; Kałwak, K.; Ussowicz, M.; Zwolińska, D. Clusterin as a New Marker of Kidney Injury in Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation—A Pilot Study. J. Clin. Med. 2020, 9, 2599. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082599
Musiał K, Augustynowicz M, Miśkiewicz-Migoń I, Kałwak K, Ussowicz M, Zwolińska D. Clusterin as a New Marker of Kidney Injury in Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation—A Pilot Study. Journal of Clinical Medicine. 2020; 9(8):2599. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082599
Chicago/Turabian StyleMusiał, Kinga, Monika Augustynowicz, Izabella Miśkiewicz-Migoń, Krzysztof Kałwak, Marek Ussowicz, and Danuta Zwolińska. 2020. "Clusterin as a New Marker of Kidney Injury in Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation—A Pilot Study" Journal of Clinical Medicine 9, no. 8: 2599. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082599