Systemic Inflammation during and after Bronchiectasis Exacerbations: Impact of Pseudomonas aeruginosa

 , , and
, , and
Abstract
:1. Introduction
2. Study Protocol
2.1. Design and Participants
2.2. Data Collection
2.3. Microbiological Diagnosis
2.4. Cytokine and Biomarker Determination
2.5. Exacerbation Definition and Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of Patients Treated as Outpatients and Inpatients for Exacerbations
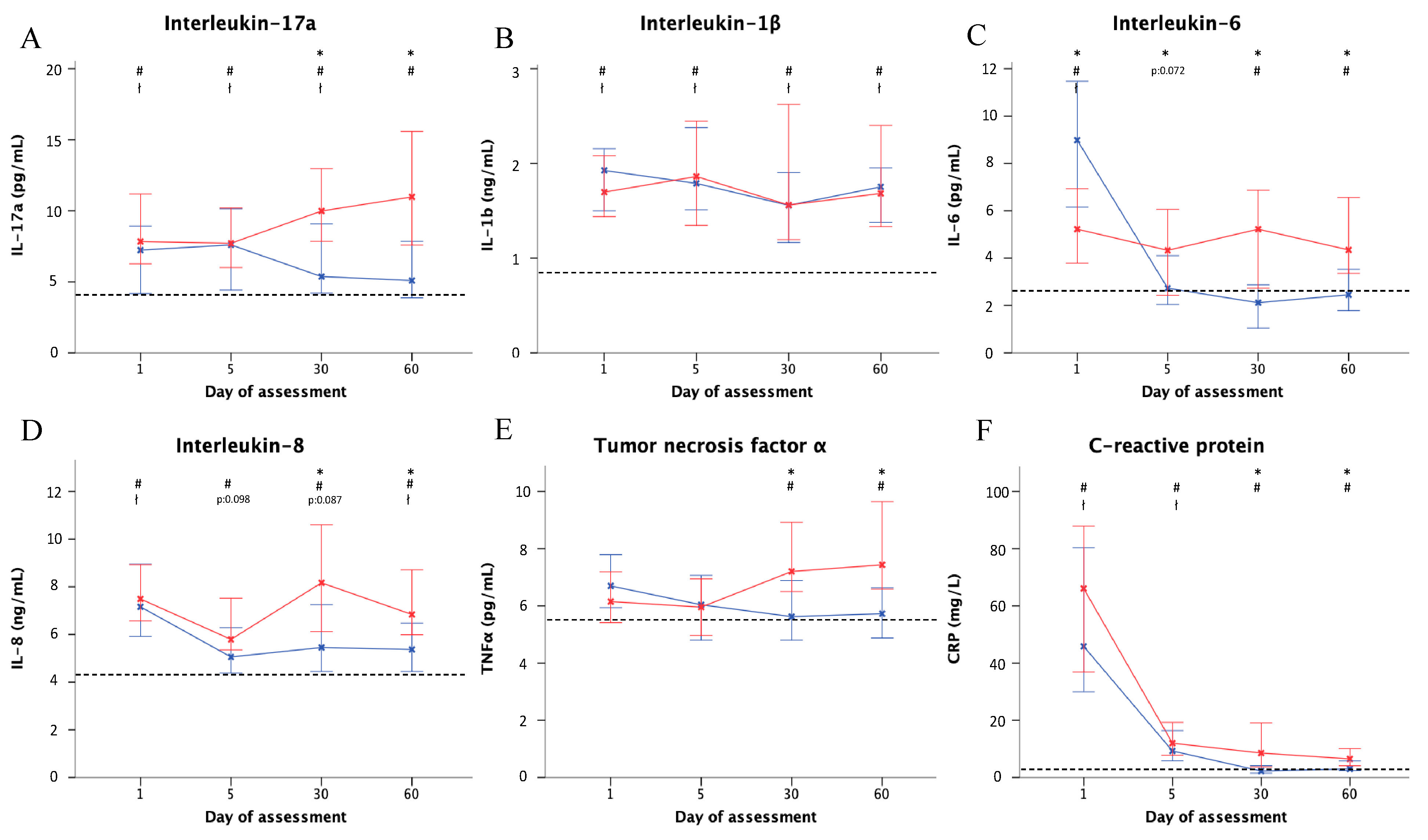
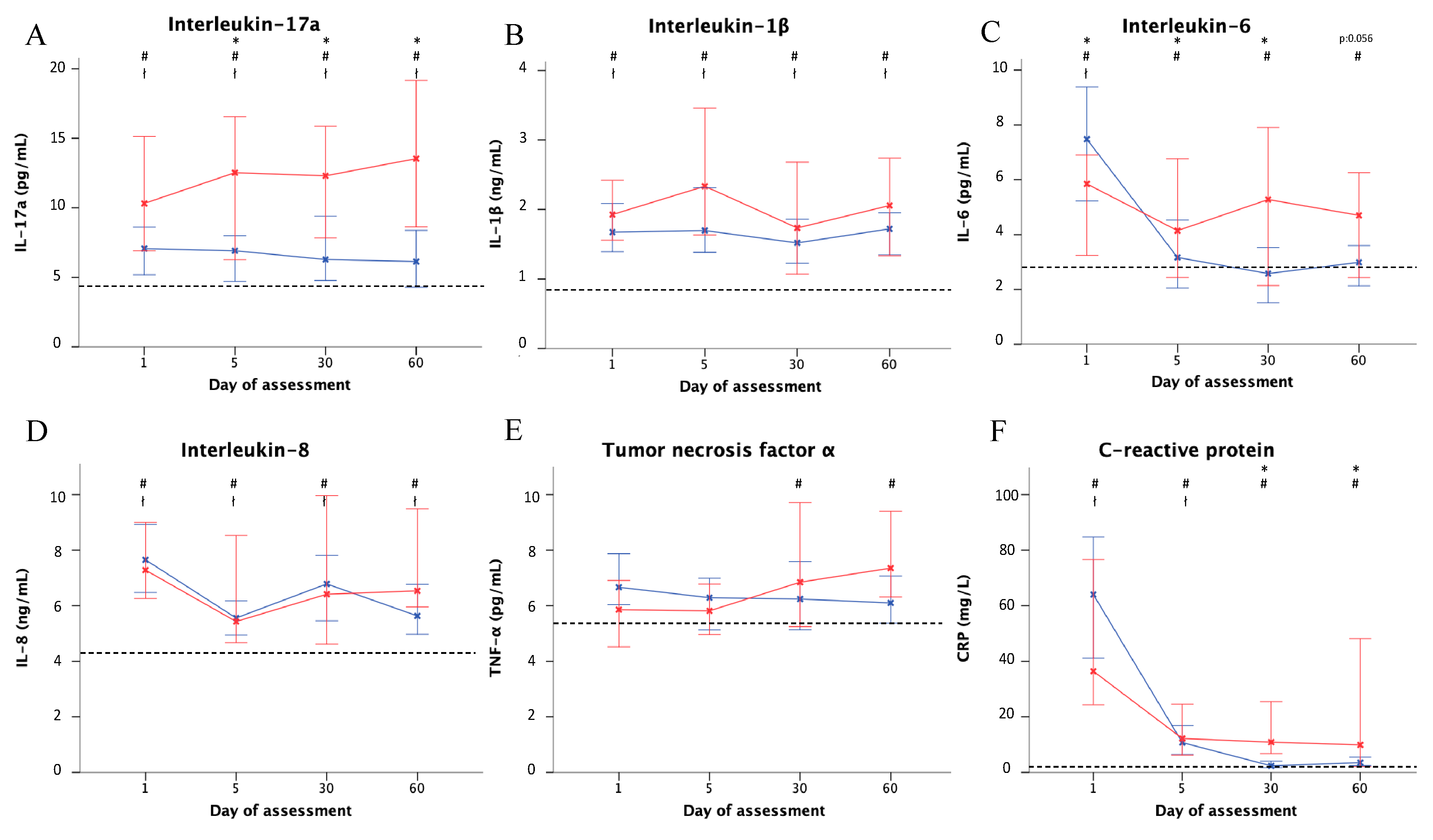
3.3. Systemic Inflammation in Exacerbations
3.3.1. Severe and Non-Severe Exacerbation
3.3.2. P. aeruginosa vs. Other Microorganisms or Unknown Etiology
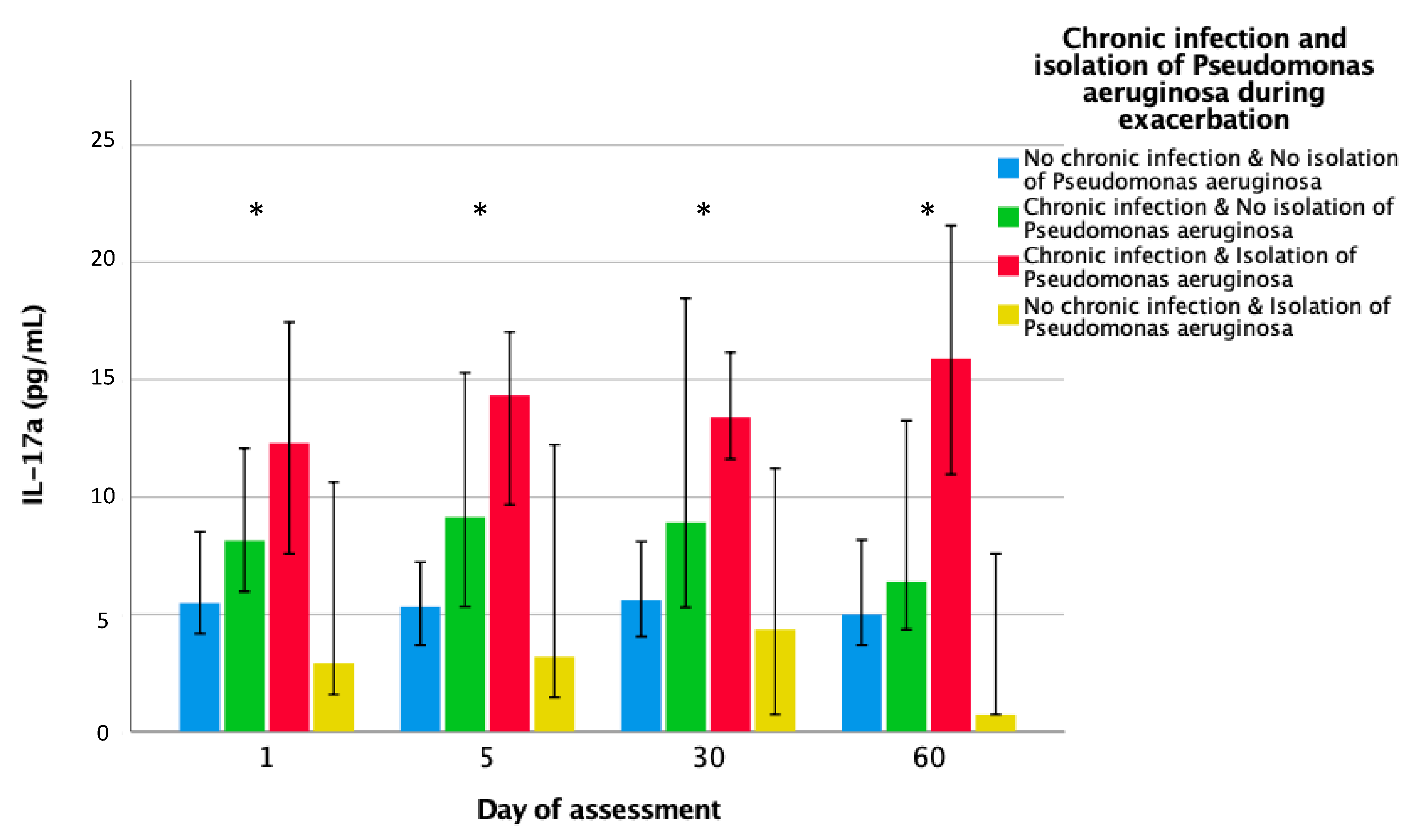
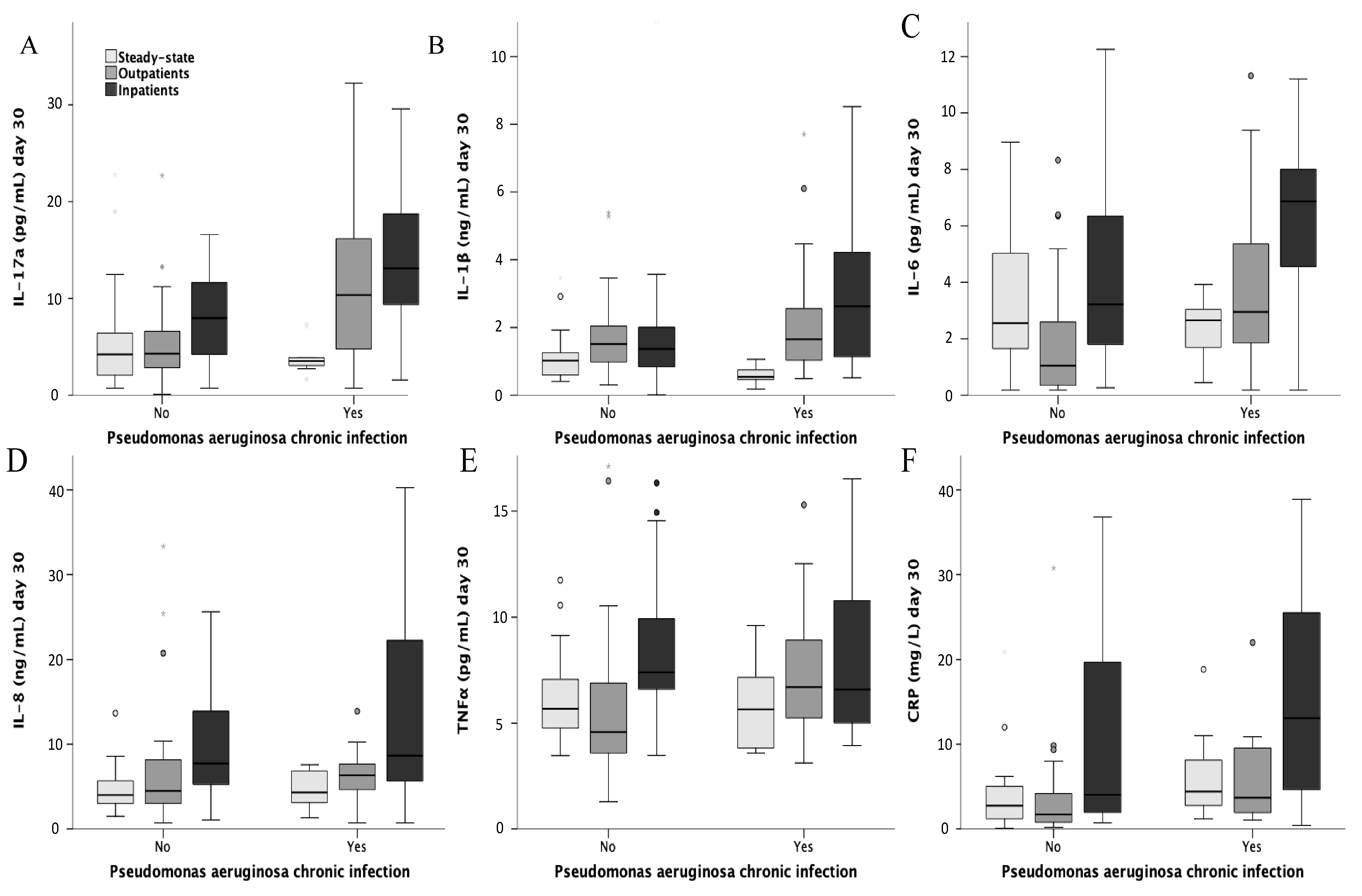
3.3.3. Prior Chronic P. aeruginosa Infection
3.4. Multivariable Analysis for Raised Inflammation at Day 30
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- McShane, P.J.; Naureckas, E.T.; Tino, G.; Strek, M.E. Non-cystic fibrosis bronchiectasis. Am. J. Respir. Crit. Care Med. 2013, 188, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Aliberti, S.; Blasi, F. Management of bronchiectasis in adults. Eur. Respir. J. 2015, 45, 1446–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, J.D.; Goeminne, P.; Aliberti, S.; McDonnell, M.J.; Lonni, S.; Davidson, J.; Poppelwell, L.; Salih, W.; Pesci, A.; Dupont, L.J.; et al. The bronchiectasis severity index an international derivation and validation study. Am. J. Respir. Crit. Care Med. 2014, 189, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.Á.; de Gracia, J.; Vendrell Relat, M.; Giron, R.-M.; Maiz Carro, L.; de la Rosa Carrillo, D.; Oliveira, C. Multidimensional approach to non-cystic fibrosis bronchiectasis: The FACED score. Eur. Respir. J. 2014, 43, 1357–1367. [Google Scholar] [CrossRef]
- Finch, S.; McDonnell, M.J.; Abo-Leyah, H.; Aliberti, S.; Chalmers, J.D. A comprehensive analysis of the impact of pseudomonas aeruginosa colonisation on prognosis in adult bronchiectasis. Ann. Am. Thorac. Soc. 2015, 12, 1602–1611. [Google Scholar]
- Menéndez, R.; Méndez, R.; Polverino, E.; Rosales-Mayor, E.; Amara-Elori, I.; Reyes, S.; Sahuquillo-Arce, J.M.; Fernandez-Barat, L.; Alcaraz, V.; Torres, A. Risk factors for multidrug-resistant pathogens in bronchiectasis exacerbations. BMC Infect. Dis. 2017, 17, 659. [Google Scholar] [CrossRef]
- Martínez-García, M.A.; Soler-Cataluña, J.-J.; Perpiñá-Tordera, M.; Román-Sánchez, P.; Soriano, J. Factors associated with lung function decline in adult patients with stable non-cystic fibrosis bronchiectasis. Chest 2007, 132, 1565–1572. [Google Scholar] [CrossRef]
- Quint, J.K.; Millett, E.R.C.C.; Joshi, M.; Navaratnam, V.; Thomas, S.L.; Hurst, J.R.; Smeeth, L.; Brown, J.S. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: A population-based cohort study. Eur. Respir. J. 2016, 47, 186–193. [Google Scholar] [CrossRef]
- Seitz, A.E.; Olivier, K.N.; Steiner, C.A.; Montes de Oca, R.; Holland, S.M.; Prevots, D.R. Trends and burden of bronchiectasis-associated hospitalizations in the United States, 1993–2006. Chest 2010, 138, 944–949. [Google Scholar] [CrossRef] [Green Version]
- Saleh, A.D.; Chalmers, J.D.; De Soyza, A.; Fardon, T.C.; Koustas, S.O.; Scott, J.; Simpson, A.J.; Brown, J.S.; Hurst, J.R. The heterogeneity of systemic inflammation in bronchiectasis. Respir. Med. 2017, 127, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Flume, P.A.; Chalmers, J.D.; Olivier, K.N. Advances in bronchiectasis: Endotyping, genetics, microbiome, and disease heterogeneity. Lancet 2018, 392, 880–890. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, J.D.; Smith, M.P.; McHugh, B.J.; Doherty, C.; Govan, J.R.; Hill, A.T. Short- and long-term antibiotic treatment reduces airway and systemic inflammation in non-cystic fibrosis bronchiectasis. Am. J. Respir. Crit. Care Med. 2012, 186, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Gao, Y.-H.; Xu, G.; Lin, Z.-Y.; Tang, Y.; Li, H.-M.; Lin, Z.-M.; Jiang, M.; Zheng, J.-P.; Chen, R.-C.; et al. Inflammatory responses, spirometry, and quality of life in subjects with bronchiectasis exacerbations. Respir. Care 2015, 60, 1180–1189. [Google Scholar] [CrossRef] [Green Version]
- Boyton, R.J.; Altmann, D.M. Bronchiectasis: Current concepts in pathogenesis, immunology, and microbiology. Annu. Rev. Pathol. 2016, 11, 523–554. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.C.H.; Martin, M.L.; Lourie, R.; Rogers, G.B.; Burr, L.D.; Hasnaim, S.Z.; Bowler, S.D.; McGuckin, M.A.; Serisier, D. Adult non-cystic fibrosis bronchiectasis is characterised by airway luminal Th17 pathway activation. PLoS ONE 2015, 10, e0119325. [Google Scholar] [CrossRef]
- Vendrell, M.; de Gracia, J.; Olveira, C.; Martinez-Garcia, M.A.; Giron, R.; Maiz, L.; Canton, R.; Coll, R.; Escribano, A.; Sole, A. Diagnosis and treatment of bronchiectasis. Spanish society of pneumology and thoracic surgery. Arch. Bronconeumol. 2008, 44, 629–640. [Google Scholar] [CrossRef]
- Polverino, E.; Cilloniz, C.; Menendez, R.; Gabarrus, A.; Rosales-Mayor, E.; Alcaraz, V.; Terraneo, S.; de la Bella Casa, J.P.; Mensa, J.; Ferrer, M.; et al. Microbiology and outcomes of community acquired pneumonia in non cystic-fibrosis bronchiectasis patients. J. Infect. 2015, 71, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Garcia, M.A.; Maiz, L.; Olveira, C.; Giron, R.M.; de la Rosa, D.; Blanco, M.; Canton, R.; Vendell, M.; Polverino, E.; de Garcia, J.; et al. Spanish guidelines on the evaluation and diagnosis of bronchiectasis in adults. Arch. Bronconeumol. 2018, 54, 79–87. [Google Scholar] [CrossRef]
- Hill, A.T.; Haworth, C.S.; Aliberti, S.; Barker, A.; Blasi, F.; Boersma, W.; Chalmers, J.D.; De Soyza, A.; Dimakou, K.; Elborn, J.S.; et al. Pulmonary exacerbation in adults with bronchiectasis: A consensus definition for clinical research. Eur. Respir. J. 2017, 49, 1700051. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; John Wiley: New York, NY, USA, 1989. [Google Scholar]
- Navaratnam, V.; Millett, E.R.C.; Hurst, J.R.; Thomas, S.L.; Smeeth, L.; Hubbard, R.B.; Brown, J.; Quint, J.K. Bronchiectasis and the risk of cardiovascular disease: A population-based study. Thorax 2017, 72, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Saleh, A.D.; Kwok, B.; Brown, J.S.; Hurst, J.R. Correlates and assessment of excess cardiovascular risk in bronchiectasis. Eur. Respir. J. 2017, 50, 1701121. [Google Scholar] [CrossRef] [PubMed]
- Courtney, J.M.; Kelly, M.G.; Watt, A.; Garske, L.; Bradley, J.; Ennis, M.; Elborn, J.S. Quality of life and inflammation in exacerbations of bronchiectasis. Chronic Respir. Dis. 2008, 5, 161–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurczynski, S.J.; Moore, B.B. IL-17 in the lung: The good, the bad, and the ugly. Am. J. Phys. Lung Cell. Mol. Physiol. 2017, 314, L6–L16. [Google Scholar] [CrossRef] [PubMed]
- Amatya, N.; Garg, A.V.; Gaffen, S.L. IL-17 Signaling: The yin and the yang. Trends Immunol. 2017, 38, 310–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritchie, N.D.; Ritchie, R.; Bayes, H.K.; Mitchell, T.J.; Evans, T.J. IL-17 can be protective or deleterious in murine pneumococcal pneumonia. PLoS Pathog. 2018, 14, e1007099. [Google Scholar] [CrossRef] [Green Version]
- Lorè, N.I.; Cigana, C.; Riva, C.; De Fino, I.; Nonis, A.; Spagnuolo, L.; Sipione, B.; Cariani, L.; Girelli, D.; Rossi, G.; et al. IL-17A impairs host tolerance during airway chronic infection by Pseudomonas aeruginosa. Sci. Rep. 2016, 6, 1–11. [Google Scholar]
- Fouka, E.; Lamprianidou, E.; Arvanitidis, K.; Filidou, E.; Kolios, G.; Miltiades, P.; Paraskakis, E.; Antiniadis, A.; Kotsianidis, I.; Bouros, D. Low-dose clarithromycin therapy modulates Th17 response in non-cystic fibrosis bronchiectasis patients. Lung 2014, 192, 849–855. [Google Scholar] [CrossRef]
- Brill, S.E.; Patel, A.R.C.; Singh, R.; Mackay, A.J.; Brown, J.S.; Hurst, J.R. Lung function, symptoms and inflammation during exacerbations of non-cystic fibrosis bronchiectasis: A prospective observational cohort study. Respir. Res. 2015, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Sibila, O.; Laserna, E.; Shoemark, A.; Keir, H.R.; Finch, S.; Rodrigo-Tryano, A.; Perea, L.; Lonergan, M.; Goeminne, P.C.; Chalmers, J.D. Airway bacterial load and inhaled antibiotic response in bronchiectasis. Am. J. Respir. Crit. Care Med. 2019, 200, 33–41. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.A.; Aksamit, T.R.; Agusti, A. Clinical fingerprinting: A way to address the complexity and heterogeneity of bronchiectasis in practice. Am. J. Respir. Crit. Care Med. 2019, 201, 14–19. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | N = 165 |
|---|---|
| Demographics | |
| Age | 71 (62–78) |
| Female | 103 (62.4) |
| Smoking | |
| Current | 4 (2.4) |
| Former | 68 (41.2) |
| Never | 93 (56.4) |
| Comorbidities | |
| COPD | 41 (24.8) |
| Asthma | 17 (10.3) |
| Heart disease | 29 (17.6) |
| Etiology | |
| Post-infective | 51 (30.9) |
| Idiopathic | 49 (29.7) |
| COPD | 30 (18.2) |
| Other | 35 (21.2) |
| Usual treatments | |
| Inhaled steroids | 139 (84.2) |
| Long term macrolides | 26 (15.8) |
| Inhaled antibiotics | 35 (21.2) |
| Severity | |
| FACED | 3 (1–4) |
| Mild | 73 (44.2) |
| Moderate | 59 (35.8) |
| Severe | 33 (20) |
| BSI | 10 (7–13) |
| Mild | 18 (10.9) |
| Moderate | 38 (23) |
| Severe | 109 (66.1) |
| Exacerbation frequency/year | 2 (1–2) |
| Previous microbiology | |
| Pseudomonas aeruginosa chronic infection | 72 (43.6) |
| Microbiology during exacerbation | |
| Pseudomonas aeruginosa | 44 (26.7) |
| Haemophilus influenzae | 13 (7.9) |
| Streptococcus pneumoniae | 13 (7.9) |
| Other | 30 (18.2) |
| Outcomes | |
| Exacerbation one month after | 21 (12.7) |
| Exacerbation one year after | 90 (54.5) |
| 1-year mortality | 14 (8.5) |
| Outpatients | Inpatients | p | Stable Patients | |
|---|---|---|---|---|
| N | 72 | 93 | 34 | |
| Demographics | ||||
| Age | 65.5 (57–72) | 75 (70–80) | <0.001 | 65.5 (54–76) |
| Female | 55 (76.4) | 48 (51.6) | 0.001 | 24 (70.6) |
| Smoking | ||||
| Current | 3 (4.2) | 1 (1.1) | 2 (5.9) | |
| Former | 28 (38.9) | 40 (43) | 0.412 | 12 (35.3) |
| Never | 41 (56.9) | 52 (55.9) | 20 (58.8) | |
| Comorbidities | ||||
| COPD | 10 (13.9) | 31 (33.3) | 0.004 | 3 (8.8) |
| Asthma | 8 (11.1) | 9 (9.7) | 0.764 | 3 (8.8) |
| Heart disease | 5 (6.9) | 24 (25.8) | 0.002 | 6 (17.6) |
| Etiology | ||||
| Post-infective | 19 (30.2) | 32 (34.8) | 12 (35.3) | |
| Idiopathic | 25 (39.7) | 24 (26.1) | 0.081 | 18 (52.9) |
| COPD | 7 (11.1) | 23 (25) | 2 (5.9) | |
| Other | 12 (19) | 13 (14.1) | 2 (5.9) | |
| Usual treatment | ||||
| Inhaled steroids | 60 (83.3) | 79 (84.9) | 0.778 | 13 (38.2) |
| Long-term macrolides | 12 (16.7) | 14 (15.1) | 0.778 | 3 (8.8) |
| Inhaled antibiotic | 17 (23.6) | 18 (19.4) | 0.507 | 4 (11.8) |
| Severity | ||||
| FACED | 1.5 (1–3) | 3 (2–5) | <0.001 | 2 (1–3) |
| Mild | 48 (66.7) | 25 (26.9) | 22 (64.7) | |
| Moderate | 17 (23.6) | 42 (45.2) | <0.001 | 9 (26.5) |
| Severe | 7 (9.7) | 26 (28) | 3 (8.8) | |
| BSI | 8.5 (5–11) | 12 (9–14) | <0.001 | 5 (2–7) |
| Mild | 14 (19.4) | 4 (4.3) | 14 (41.2) | |
| Moderate | 22 (30.6) | 16 (17.2) | <0.001 | 14 (41.2) |
| Severe | 36 (50) | 73 (78.5) | 6 (17.6) | |
| Exacerbation frequency/year | 1 (0.5–2) | 2 (1–3) | 0.746 | |
| Previous microbiology | ||||
| Pseudomonas aeruginosa chronic infection | 33 (45.8) | 39 (41.9) | 0.617 | 12 (35.3) |
| Microbiology during exacerbation | ||||
| Pseudomonas aeruginosa | 14 (19.4) | 30 (32.3) | 0.065 | - |
| Haemophilus influenzae | 7 (9.7) | 6 (6.5) | 0.439 | - |
| Streptococcus pneumoniae | 4 (5.6) | 9 (9.7) | 0.330 | - |
| Other | 14 (19.4) | 16 (17.2) | 0.711 | - |
| Outcomes | ||||
| Exacerbation one month after | 4 (5.7) | 17 (18.5) | 0.017 | 1 (2.9) |
| Exacerbation one year after | 32 (46.4) | 58 (63) | 0.035 | 6 (17.6) |
| 1-year mortality | 1 (1.4) | 13 (14) | 0.004 | 0 (0) |
| IL-17a | IL-1β | IL-6 | IL-8 | TNF-α | CRP | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median at Day 30 | 8.29 pg/mL | 1.56 ng/mL | 2.84 pg/mL | 6.69 ng/mL | 6.64 pg/mL | 3.67 mg/L | ||||||
| p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | |
| Age (>65 years) | 0.303 | 1.78 (0.59–5.34) | 0.412 | 1.49 (0.58–3.86) | 0.453 | 0.67 (0.24–1.9) | 0.568 | 0.75 (0.28–2.02) | 0.157 | 1.98 (0.77–5.07) | 0.163 | 0.42 (0.12–1.43) |
| Sex (men) | 0.322 | 0.54 (0.16–1.83) | 0.374 | 0.62 (0.22–1.77) | 0.742 | 0.83 (0.28–2.51) | 0.110 | 2.49 (0.81–7.63) | 0.833 | 1.12 (0.4–3.16) | 0.701 | 0.75 (0.17–3.26) |
| BSI (severe) | 0.186 | 0.42 (0.11–1.53) | 0.977 | 1.02 (0.34–3.01) | 0.793 | 0.86 (0.27–2.73) | 0.681 | 1.27 (0.41–3.88) | 0.574 | 1.36 (0.47–3.99) | 0.394 | 0.53 (0.12–2.28) |
| Hospital Admission Last Year | 0.945 | 1.04 (0.33–3.33) | 0.543 | 0.73 (0.26–2.03) | 0.971 | 1.02 (0.35–3.01) | 0.261 | 0.54 (0.18–1.59) | 0.838 | 1.11 (0.4–3.09) | 0.886 | 0.91 (0.24–3.4) |
| Inhaled Steroids | 0.085 | 0.28 (0.07–1.19) | 0.320 | 1.99 (0.51–7.69) | 0.585 | 1.45 (0.38–5.52) | 0.033 | 5.38 (1.15–25.2) | 0.938 | 1.05 (0.28–3.98) | 0.401 | 0.51 (0.11–2.47) |
| Exacerbation with Admission | 0.015 | 4.58 (1.34–15.71) | 0.779 | 1.15 (0.43–3.13) | 0.006 | 4.89 (1.58–15.14) | 0.037 | 3.08 (1.07–8.86) | 0.201 | 1.89 (0.71–5.04) | 0.011 | 6.7 (1.54–29.23) |
| Chronic PA Infection | 0.002 | 7.47 (2.09–26.76) | 0.221 | 1.93 (0.67–5.51) | 0.034 | 3.44 (1.09–10.84) | 0.654 | 1.29 (0.42–3.94) | 0.727 | 0.83 (0.29–2.37) | 0.180 | 2.61 (0.64–10.6) |
| PA Isolation during Exacerbation | 0.444 | 1.66 (0.45–6.13) | 0.535 | 1.43 (0.46–4.47) | 0.991 | 0.99 (0.30–3.32) | 0.429 | 0.61 (0.18–2.06) | 0.689 | 1.26 (0.4–3.97) | 0.108 | 4.32 (0.73–25.66) |
| Treatment Duration >14 Days | 0.257 | 1.89 (0.63–5.7) | 0.726 | 1.19 (0.44–3.21) | 0.495 | 1.43 (0.51–4.05) | 0.436 | 0.66 (0.24–1.86) | 0.977 | 0.99 (0.37–2.65) | 0.209 | 2.07 (0.67–6.44) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menéndez, R.; Méndez, R.; Amara-Elori, I.; Reyes, S.; Montull, B.; Feced, L.; Alonso, R.; Amaro, R.; Alcaraz, V.; Fernandez-Barat, L.; et al. Systemic Inflammation during and after Bronchiectasis Exacerbations: Impact of Pseudomonas aeruginosa. J. Clin. Med. 2020, 9, 2631. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082631
Menéndez R, Méndez R, Amara-Elori I, Reyes S, Montull B, Feced L, Alonso R, Amaro R, Alcaraz V, Fernandez-Barat L, et al. Systemic Inflammation during and after Bronchiectasis Exacerbations: Impact of Pseudomonas aeruginosa. Journal of Clinical Medicine. 2020; 9(8):2631. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082631
Chicago/Turabian StyleMenéndez, Rosario, Raúl Méndez, Isabel Amara-Elori, Soledad Reyes, Beatriz Montull, Laura Feced, Ricardo Alonso, Rosanel Amaro, Victoria Alcaraz, Laia Fernandez-Barat, and et al. 2020. "Systemic Inflammation during and after Bronchiectasis Exacerbations: Impact of Pseudomonas aeruginosa" Journal of Clinical Medicine 9, no. 8: 2631. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9082631