PCSK9 Levels Are Raised in Chronic HCV Patients with Hepatocellular Carcinoma


 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. PCSK9 Measurement
2.3. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Ryerson, A.B.; Eheman, C.R.; Altekruse, S.F.; Ward, J.W.; Jemal, A.; Sherman, R.L.; Henley, S.J.; Holtzman, D.; Lake, A.; Noone, A.M.; et al. Annual Report to the Nation on the Status of Cancer, 1975-2012, featuring the increasing incidence of liver cancer. Cancer 2016, 122, 1312–1337. [Google Scholar] [CrossRef] [PubMed]
- Fasani, P.; Sangiovanni, A.; De Fazio, C.; Borzio, M.; Bruno, S.; Ronchi, G.; Del Ninno, E.; Colombo, M. High prevalence of multinodular hepatocellular carcinoma in patients with cirrhosis attributable to multiple risk factors. Hepatology 1999, 29, 1704–1707. [Google Scholar] [CrossRef]
- Yoshizawa, H. Hepatocellular carcinoma associated with hepatitis C virus infection in Japan: Projection to other countries in the foreseeable future. Oncology 2002, 62 (Suppl. 1), 8–17. [Google Scholar] [CrossRef] [PubMed]
- Popescu, C.I.; Riva, L.; Vlaicu, O.; Farhat, R.; Rouille, Y.; Dubuisson, J. Hepatitis C virus life cycle and lipid metabolism. Biology 2014, 3, 892–921. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Otgonsuren, M.; Henry, L.; Venkatesan, C.; Mishra, A.; Erario, M.; Hunt, S. Association of nonalcoholic fatty liver disease (NAFLD) with hepatocellular carcinoma (HCC) in the United States from 2004 to 2009. Hepatology 2015, 62, 1723–1730. [Google Scholar] [CrossRef]
- Maxwell, K.N.; Fisher, E.A.; Breslow, J.L. Overexpression of PCSK9 accelerates the degradation of the LDLR in a post-endoplasmic reticulum compartment. Proc. Natl. Acad. Sci. USA 2005, 102, 2069–2074. [Google Scholar] [CrossRef] [Green Version]
- Ruscica, M.; Ferri, N.; Macchi, C.; Meroni, M.; Lanti, C.; Ricci, C.; Maggioni, M.; Fracanzani, A.L.; Badiali, S.; Fargion, S.; et al. Liver fat accumulation is associated with circulating PCSK9. Ann. Med. 2016, 48, 384–391. [Google Scholar] [CrossRef]
- Ferri, N.; Corsini, A.; Macchi, C.; Magni, P.; Ruscica, M. Proprotein convertase subtilisin kexin type 9 and high-density lipoprotein metabolism: Experimental animal models and clinical evidence. Transl. Res. J. Lab. Clin. Med. 2016, 173, 19–29. [Google Scholar] [CrossRef]
- Ferri, N.; Ruscica, M. Proprotein convertase subtilisin/kexin type 9 (PCSK9) and metabolic syndrome: Insights on insulin resistance, inflammation, and atherogenic dyslipidemia. Endocrine 2016, 54, 588–601. [Google Scholar] [CrossRef] [PubMed]
- Labonte, P.; Begley, S.; Guevin, C.; Asselin, M.C.; Nassoury, N.; Mayer, G.; Prat, A.; Seidah, N.G. PCSK9 impedes hepatitis C virus infection in vitro and modulates liver CD81 expression. Hepatology 2009, 50, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, A.; Gusarova, V.; Stahl, N.; Gurnett-Bander, A.; Kyratsous, C.A. Alirocumab, a Therapeutic Human Antibody to PCSK9, Does Not Affect CD81 Levels or Hepatitis C Virus Entry and Replication into Hepatocytes. PLoS ONE 2016, 11, e0154498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adorni, M.P.; Cipollari, E.; Favari, E.; Zanotti, I.; Zimetti, F.; Corsini, A.; Ricci, C.; Bernini, F.; Ferri, N. Inhibitory effect of PCSK9 on Abca1 protein expression and cholesterol efflux in macrophages. Atherosclerosis 2017, 256, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, Q. Hepatitis C virus regulates proprotein convertase subtilisin/kexin type 9 promoter activity. Biochem. Biophys. Res. Commun. 2018, 496, 1229–1235. [Google Scholar] [CrossRef]
- Li, Z.; Liu, Q. Proprotein convertase subtilisin/kexin type 9 inhibits hepatitis C virus replication through interacting with NS5A. J. Gen. Virol. 2018, 99, 44–61. [Google Scholar] [CrossRef]
- Ruscica, M.; Ferri, N.; Fogacci, F.; Rosticci, M.; Botta, M.; Marchiano, S.; Magni, P.; D’Addato, S.; Giovannini, M.; Borghi, C.; et al. Circulating Levels of Proprotein Convertase Subtilisin/Kexin Type 9 and Arterial Stiffness in a Large Population Sample: Data From the Brisighella Heart Study. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [Green Version]
- Syed, G.H.; Tang, H.; Khan, M.; Hassanein, T.; Liu, J.; Siddiqui, A. Hepatitis C virus stimulates low-density lipoprotein receptor expression to facilitate viral propagation. J. Virol. 2014, 88, 2519–2529. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.H.; Chen, W.C.; Tsan, Y.T.; Chen, M.J.; Shih, W.T.; Tsai, Y.H.; Chen, P.C. Statin use and the risk of cirrhosis development in patients with hepatitis C virus infection. J. Hepatol. 2015, 63, 1111–1117. [Google Scholar] [CrossRef]
- Tsan, Y.T.; Lee, C.H.; Ho, W.C.; Lin, M.H.; Wang, J.D.; Chen, P.C. Statins and the risk of hepatocellular carcinoma in patients with hepatitis C virus infection. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 1514–1521. [Google Scholar] [CrossRef]
- Ye, J.; Wang, C.; Sumpter, R., Jr.; Brown, M.S.; Goldstein, J.L.; Gale, M., Jr. Disruption of hepatitis C virus RNA replication through inhibition of host protein geranylgeranylation. Proc. Natl. Acad. Sci. USA 2003, 100, 15865–15870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchet, M.; Le, Q.T.; Seidah, N.G.; Labonte, P. Statins can exert dual, concentration dependent effects on HCV entry in vitro. Antivir. Res. 2016, 128, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Careskey, H.E.; Davis, R.A.; Alborn, W.E.; Troutt, J.S.; Cao, G.; Konrad, R.J. Atorvastatin increases human serum levels of proprotein convertase subtilisin/kexin type 9. J Lipid Res 2008, 49, 394–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, N.; Marchiano, S.; Lupo, M.G.; Trenti, A.; Biondo, G.; Castaldello, P.; Corsini, A. Geranylgeraniol prevents the simvastatin-induced PCSK9 expression: Role of the small G protein Rac1. Pharmacol. Res. 2017, 122, 96–104. [Google Scholar] [CrossRef]
- Bhat, M.; Skill, N.; Marcus, V.; Deschenes, M.; Tan, X.; Bouteaud, J.; Negi, S.; Awan, Z.; Aikin, R.; Kwan, J.; et al. Decreased PCSK9 expression in human hepatocellular carcinoma. BMC Gastroenterol. 2015, 15, 176. [Google Scholar] [CrossRef] [Green Version]
- Hyrina, A.; Olmstead, A.D.; Steven, P.; Krajden, M.; Tam, E.; Jean, F. Treatment-Induced Viral Cure of Hepatitis C Virus-Infected Patients Involves a Dynamic Interplay among three Important Molecular Players in Lipid Homeostasis: Circulating microRNA (miR)-24, miR-223, and Proprotein Convertase Subtilisin/Kexin Type 9. EBioMedicine 2017, 23, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Jeong, H.J.; Lee, H.S.; Kim, K.S.; Kim, Y.K.; Yoon, D.; Park, S.W. Sterol-dependent regulation of proprotein convertase subtilisin/kexin type 9 expression by sterol-regulatory element binding protein-2. J. Lipid. Res. 2008, 49, 399–409. [Google Scholar] [CrossRef] [Green Version]
- Ruscica, M.; Ricci, C.; Macchi, C.; Magni, P.; Cristofani, R.; Liu, J.; Corsini, A.; Ferri, N. Suppressor of Cytokine Signaling-3 (SOCS-3) Induces Proprotein Convertase Subtilisin Kexin Type 9 (PCSK9) Expression in Hepatic HepG2 Cell Line. J. Biol. Chem. 2016, 291, 3508–3519. [Google Scholar] [CrossRef] [Green Version]
- Shende, V.R.; Wu, M.; Singh, A.B.; Dong, B.; Kan, C.F.; Liu, J. Reduction of circulating PCSK9 and LDL-C levels by liver-specific knockdown of HNF1alpha in normolipidemic mice. J. Lipid. Res. 2015, 56, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M.; Stepanova, M.; Estep, M.; Negro, F.; Clark, P.J.; Hunt, S.; Song, Q.; Paulson, M.; Stamm, L.M.; Brainard, D.M.; et al. Dysregulation of distal cholesterol biosynthesis in association with relapse and advanced disease in CHC genotype 2 and 3 treated with sofosbuvir and ribavirin. J. Hepatol. 2016, 64, 29–36. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | HCC Patients (n = 86) | Not HCC Patients (n = 92) | |||||
|---|---|---|---|---|---|---|---|
| Cirrhotic | Chronic Hepatitis | ||||||
| Control | HCV+ | HCV- | HCV+ | HCV- | HCV+ | HCV- | |
| N (M/F) | 24 (9/15) | 53 (39/14) | 33 (28/5) | 19 (15/4) | 15 (11/4) | 54 (29/25) | 4 (2/2) |
| Age (years) Mean ± SEM | 51.4 ± 9.6 | 64.6 ± 11.3 b | 66.6 ± 8.4 b | 62.8 ± 11.4 | 64.6 ± 7.3 | 57.1 ± 21.2 m | 66.1 ± 9.6 |
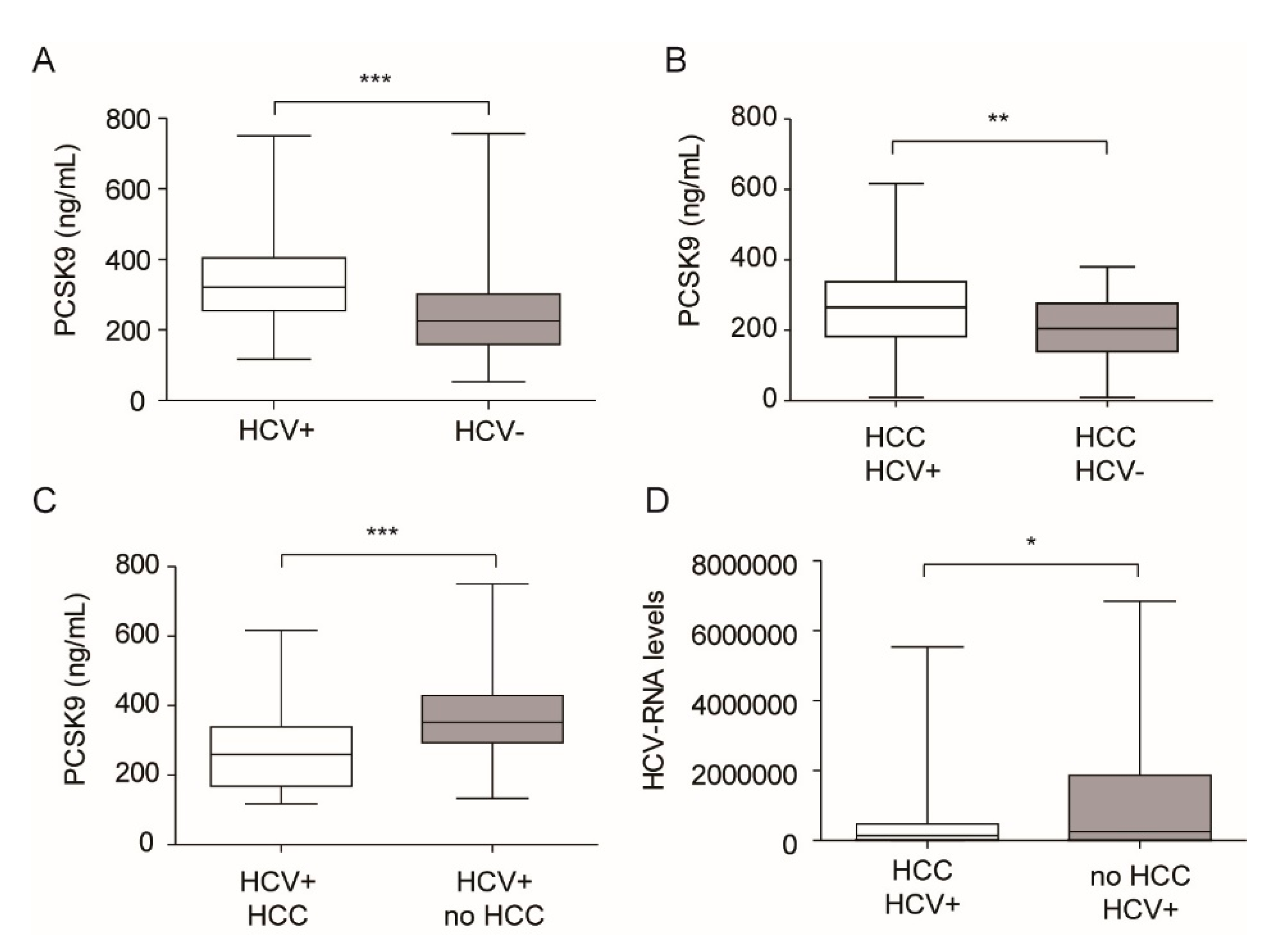
| PCSK9 (ng/mL) Mean ± SEM | 244.9 ± 74.2 | 271.76 ± 123 | 252.06 ± 130.06 | 307.9 ± 143.1 | 205.6 ± 105 | 357.9 ± 114.7 b,e,g,l | 330.6 ± 78 |
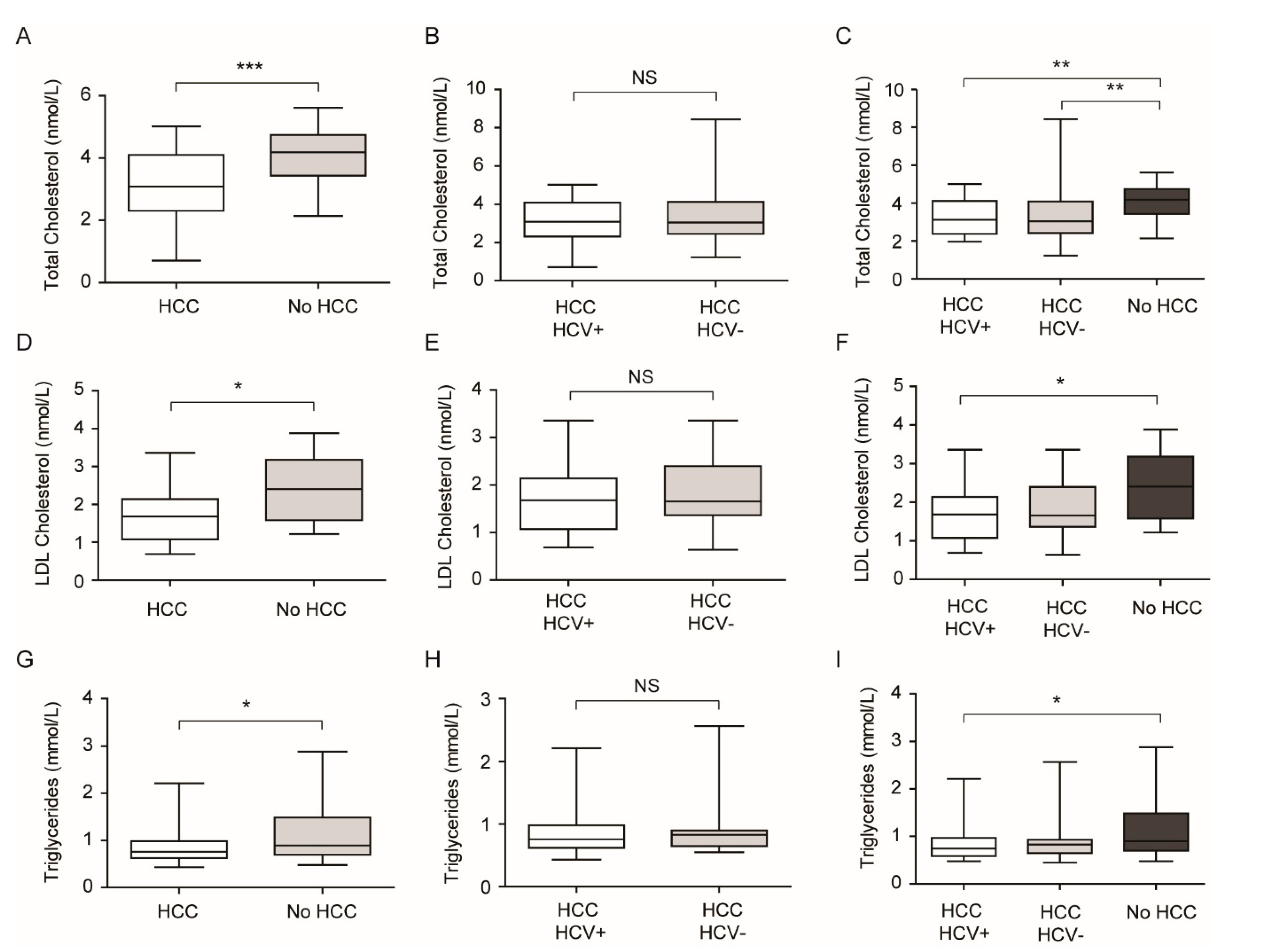
| TC (mmol/L) Mean ± SEM | 5.07 ± 0.9 | 3.21 ± 1.15 c | 3.39 ± 1.4 c | 2.8 ± 0.8 c | 2.95 ± 0.88 c | 4.1 ± 0.89 b,f,m,h,i | 3.58 ± 0.67 |
| LDL-C (mmol/L) Mean ± SEM | 2.7 ± 0.7 | 1.71 ± 0.82l c | 1.90 ± 0.7 b | 1.39 ± 0.8 c | 1.92 ± 0.77 a | 2.4 ± 0.85 f,h | 1.98 ± 0.88 |
| TG (mmol/L) Mean ± SEM | 1.47 ± 0.36 | 0.86 ± 0.36 c | 0.92 ± 0.40 c | 0.88 ± 0.20 c | 0.85 ± 0.31 c | 1.15 ± 0.64 d | 1.01 ± 0.32 |
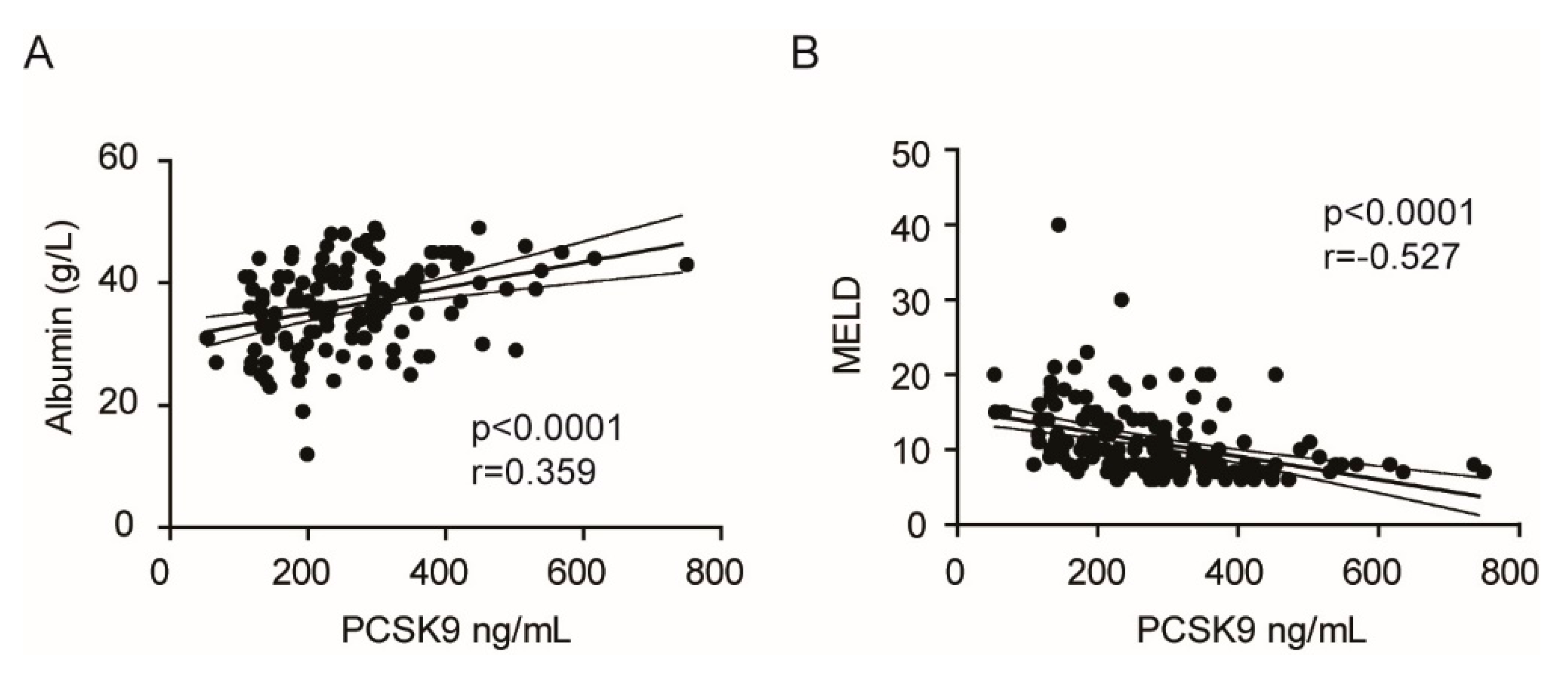
| Albumin (g/L) Mean ± SEM | ND | 34.7 ± 7.3 | 36.5 ± 6.8 | 37.9 ± 6.0 | 34.7 ± 5.8 | 41.9 ± 5.6 | 37.5 ± 9.2 |
| Coefficients a | |||||
|---|---|---|---|---|---|
| Model | UnstandardizedCoefficients | Standardized Coefficients | t | p-Value | |
| B | Std. Error | Beta | |||
| 1 (Constant) | 261.811 | 84.762 | 3.089 | 0.003 | |
| Age | −0.859 | 0.852 | −0.103 | −1.009 | 0.316 |
| Sex | −28.789 | 33.901 | −0.091 | −0.849 | 0.399 |
| Total cholesterol | 23.586 | 30.146 | 0.184 | 0.782 | 0.437 |
| LDL-C | 25.849 | 38.699 | 0.155 | 0.668 | 0.506 |
| HCV | 61.433 | 30.207 | 0.210 | 2.034 | 0.046 |
| HCC | −80.080 | 30.388 | −0.281 | −2.635 | 0.010 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fasolato, S.; Pigozzo, S.; Pontisso, P.; Angeli, P.; Ruscica, M.; Savarino, E.; De Martin, S.; Lupo, M.G.; Ferri, N. PCSK9 Levels Are Raised in Chronic HCV Patients with Hepatocellular Carcinoma. J. Clin. Med. 2020, 9, 3134. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103134
Fasolato S, Pigozzo S, Pontisso P, Angeli P, Ruscica M, Savarino E, De Martin S, Lupo MG, Ferri N. PCSK9 Levels Are Raised in Chronic HCV Patients with Hepatocellular Carcinoma. Journal of Clinical Medicine. 2020; 9(10):3134. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103134
Chicago/Turabian StyleFasolato, Silvano, Sabrina Pigozzo, Patrizia Pontisso, Paolo Angeli, Massimiliano Ruscica, Edoardo Savarino, Sara De Martin, Maria Giovanna Lupo, and Nicola Ferri. 2020. "PCSK9 Levels Are Raised in Chronic HCV Patients with Hepatocellular Carcinoma" Journal of Clinical Medicine 9, no. 10: 3134. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103134