Maternal and Perinatal Outcomes in Patients with Suspected COVID-19 and Their Relationship with a Negative RT-PCR Result

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Patients and Methods
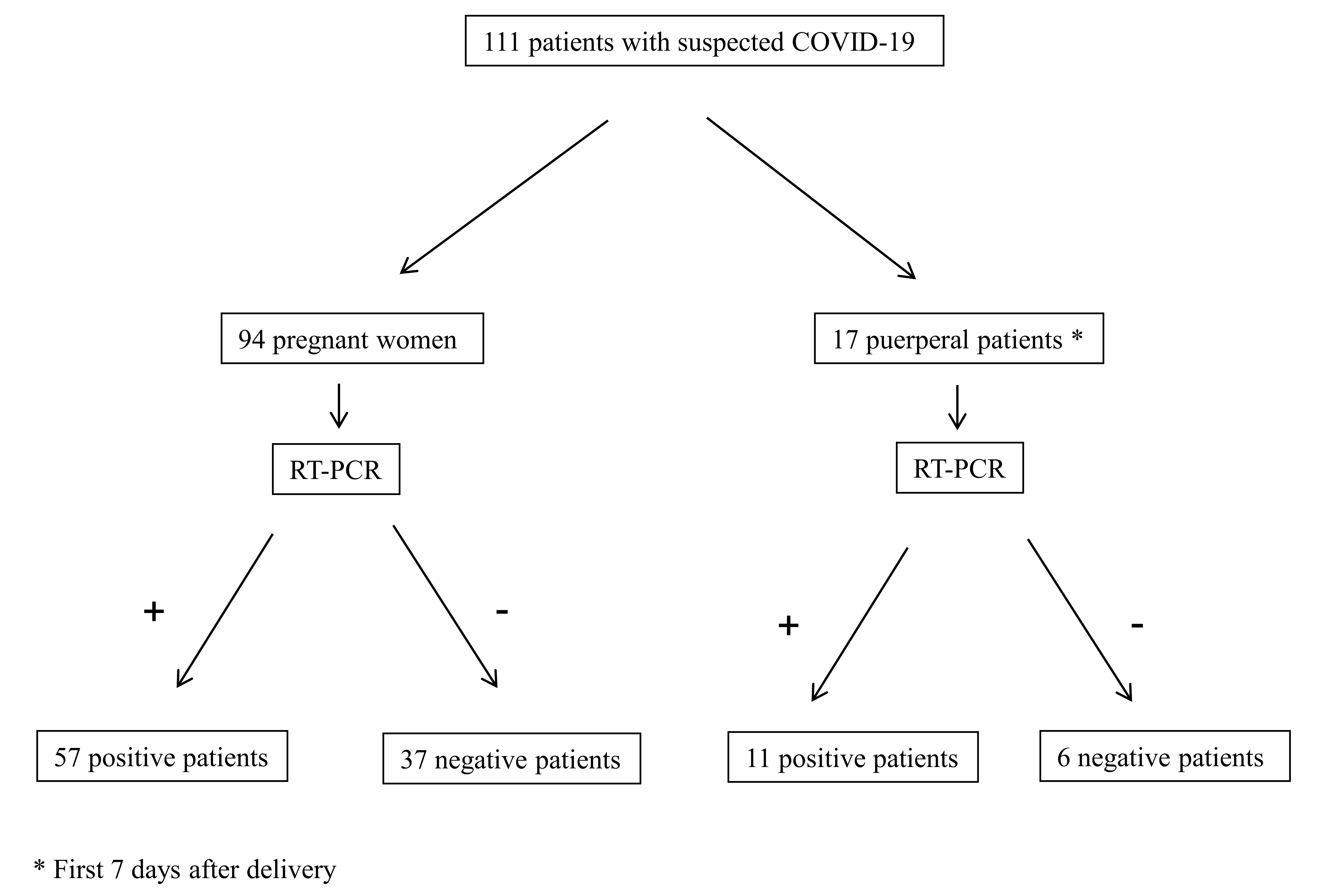
2.1. Patient Cohort and Study Design
- Mild cases—the clinical symptoms were mild and there was no sign of pneumonia when imaged.
- Moderate cases—fever and respiratory symptoms with radiological findings of pneumonia.
- Severe cases—any of the following conditions:
- a.
- Respiratory distress (respiratory rate of ≥30 per min).
- b.
- Oxygen saturation on room air at rest of ≤93%.
- c.
- Partial pressure of oxygen in arterial blood/fraction of inspired oxygen ≤ 300 mmHg.
- Critical cases—any of the following conditions:
- a.
- Respiratory failure and requiring mechanical ventilation.
- b.
- Shock.
- c.
- Patients with another organ failure that requires ICU care.
2.2. Data Analysis
2.3. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| COVID-19 | coronavirus disease 2019 |
| RT-PCR | real-time reverse transcription polymerase chain reaction |
| ICU | intensive care unit |
| MPOs | maternal–perinatal outcomes |
| BMI | body mass index |
| LDH | lactate dehydrogenase |
| GA | gestational age |
| NICU | neonatal intensive care unit |
| CI | confidence interval |
References
- World Health Organization. Coronavirus Disease (COVID-19). Weekly Epidemiological Update. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200921-weekly-epi-update-pdf?sfvrsn=d9cf9496_ (accessed on 25 September 2020).
- World Health Organization. Diagnostic Testing for SARS-CoV-2. 11 September 2020. Available online: https://www.who.int/publications/i/item/diagnostic-testing-for-sars-cov-2 (accessed on 25 October 2020).
- Li, Z.; Yi, Y.; Luo, X.; Xiong, N.; Liu, Y.; Li, S.; Sun, R.; Wang, Y.; Hu, B.; Chen, W.; et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J. Med Virol. 2020, 92, 1518–1524. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: Retrospective cohort study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, V.S.; Gurgel, R.Q.; Cuevas, L.E.; Martins-Filho, P.R. Prolonged Fecal Shedding of SARS-CoV-2 in Pediatric Patients: A Quantitative Evidence Synthesis. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 150–152. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients of Novel Coronavirus Disease 2019. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Centro de coordinación de Alertas y Emergencias Sanitarias. Actualización nª Enfermedad por el coronavirus (COVID-19); Ministerio de Sanidad, 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_215_COVID-pdf (accessed on 25 September 2020).
- Comunidad de Madrid. Reoganización de la atención obstétrica/ginecológica y neonatológica urgente de la Comunidad de Madrid. 23 March 2020. Available online: https://www.comunidad.madrid/noticias/2020/03/23/comunidad-reorganiza-atencion-obstetrica-ginecologica-neonatologica-urgente (accessed on 25 May 2020).
- Pacheco, L.D.; Saad, A.F.; Saade, G. Early Acute Respiratory Support for Pregnant Patients with Coronavirus Disease 2019 (COVID-19) Infection. Obstet. Gynecol. 2020, 136, 42–45. [Google Scholar] [CrossRef]
- Peng, F.; Tu, L.; Yang, Y.; Hu, P.; Wang, R.; Hu, Q.; Cao, F.; Jiang, T.; Sun, J.; Xu, G.; et al. Management and Treatment of COVID-19: The Chinese Experience. Can. J. Cardiol. 2020, 36, 915–930. [Google Scholar] [CrossRef]
- Rickham, P.P. Human Experimentation. Code of Ethics of the World Medical Association. Declaration of Helsinki. Br. Med. J. 1964, 2, 177. [Google Scholar] [PubMed] [Green Version]
- Sutton, D.; Fuchs, K.; D’Alton, M.; Goffman, D. Universal Screening for SARS-CoV-2 in Women Admitted for Delivery. N. Engl. J. Med. 2020, 382, 2163–2164. [Google Scholar] [CrossRef]
- Li, Y.Y.; Wang, W.N.; Lei, Y.; Zhang, B.; Yang, J.; Hu, J.W.; Ren, Y.L.; Lu, Q.F. Comparison of the clinical characteristics between RNA positive and negative patients clinically diagnosed with 2019 novel coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, E023. [Google Scholar]
- Atanasova, V.B.; Arevalo-Serrano, J.; Alvarado, E.A.; Larroca, S.G.-T. Maternal mortality in Spain and its association with country of origin: Cross-sectional study during the period 1999–2015. BMC Public Health 2018, 18, 1171. [Google Scholar]
- Larroca, S.G.-T.; Arevalo-Serrano, J.; Vila, A.D.; Recarte, M.P.P.; Hernandez, I.C.; Pierna, A.S.; Bonelli, S.L.; De Leon-Luis, J. Human Development Index (HDI) of the maternal country of origin as a predictor of perinatal outcomes—A longitudinal study conducted in Spain. BMC Pregnancy Childbirth 2017, 17, 314. [Google Scholar]
- Larroca, S.G.-T.; Valera, F.A.; Herrera, E.A.; Hernandez, I.C.; Lopez, Y.C.; De Leon-Luis, J. Human Development Index of the maternal country of origin and its relationship with maternal near miss: A systematic review of the literature. BMC Pregnancy Childbirth 2020, 20, 1–24. [Google Scholar]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Finer, N.; Garnett, S.P.; Bruun, J.M. COVID-19 and obesity. Clin. Obes. 2020, 10, e12365. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, M.; Zhu, Z.; Liu, Y. Coronavirus disease 2019 (COVID-19) and pregnancy: A systematic review. J. Matern. Neonatal Med. 2020, 1–4. [Google Scholar]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Merad, M.; Martin, J.C. Pathological inflammation in patients with COVID-19: A key role for monocytes and macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pan, Y.; Hu, X. Abnormalities of peripheral blood system in patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta 2020, 507, 174–180. [Google Scholar] [CrossRef]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yan, L.-M.; Wan, L.; Xiang, T.-X.; Le, A.; Liu, J.-M.; Peiris, M.; Poon, L.L.M.; Zhang, W. Viral dynamics in mild and severe cases of COVID. Lancet Infect. Dis. 2020, 20, 656–657. [Google Scholar] [CrossRef] [Green Version]
- Hantoushzadeh, S.; Shamshirsaz, A.A.; Aleyasin, A.; Seferovic, M.D.; Aski, S.K.; Arian, S.E.; Pooransari, P.; Ghotbizadeh, F.; Aalipour, S.; Soleimani, Z.; et al. Maternal death due to COVID-19 disease. Am. J. Obstet. Gynecol. 2020, 223, e1–e16. [Google Scholar] [CrossRef]
- Di Mascio, D.; The WAPM (The World Association of Perinatal Medicine) Working Group on COVID-19; Saccone, G.; Sen, C.; Galindo, A.; Grünebaum, A.; Yoshimatsu, J.; Stanojevic, M.; Kurjak, A.; Chervenak, F.; et al. Maternal and Perinatal Outcomes of Pregnant Women with SARS-COV-2 infection. Ultrasound Obstet. Gynecol. 2020. [Google Scholar] [CrossRef]
- Yu, X.; Sun, S.; Shi, Y.; Wang, H.; Zhao, R.; Sheng, J. SARS-CoV-2 viral load in sputum correlates with risk of COVID-19 progression. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.C.; Chan, F.K.L.; Chan, P.K.S. Screening FMT donors during the COVID-19 pandemic: A protocol for stool SARS-CoV-2 viral quantification. Lancet Gastroenterol. Hepatol. 2020, 5, 642–643. [Google Scholar] [CrossRef]
- Carosso, A.; Cosma, S.; Borella, F.; Marozio, L.; Coscia, A.; Ghisetti, V.; Di Perri, G.; Benedetto, C. Pre-Labor Anorectal Swab for SARS-CoV-2 in COVID-19 Patients: Is it Time to Think About It? SSRN Electron. J. 2020, 249, 98–99. [Google Scholar]
- Carosso, A.R.; Cosma, S.; Benedetto, C. Vaginal delivery in COVID-19 pregnant women: Anorectum as a potential alternative route of SARS-CoV-2 transmission. Am. J. Obstet. Gynecol. 2020, 223, 612. [Google Scholar] [CrossRef]


{kind=link}
| Overall | RT-PCR Positive | RT-PCR Negative | p-Value | |
|---|---|---|---|---|
| N (%) | 111 | 68 (61.3%) | 43 (38.7%) | |
| Maternal Features | ||||
| Maternal race, n (%) | 0.557 | |||
| Caucasian | 63 (56.8%) | 38 (55.9%) | 25 (58.1%) | |
| Hispanic | 45 (40.5%) | 29 (42.7%) | 16 (37.2%) | |
| Asiatic | 3 (2.7%) | 1 (1.5%) | 2 (4.7%) | |
| Maternal age, mean (CI 95%) | 33.0 (31.8–34.3) | 33.5 (32.0–35.0) | 32.3 (30.3–34.3) | 0.347 |
| Tobacco, n (%) | 12 (11.1%) | 6 (9.1%) | 6 (14.3%) | 0.408 |
| Maternal morbidities, n (%) | 45 (40.9%) | 25 (36.8%) | 20 (47.6%) | 0.262 |
| BMI, mean (CI 95%) | 26.4 (25.3–27.5) | 27.1 (25.6–28.7) | 25.3 (23.8–26.9) | 0.118 |
| Obstetric Features | ||||
| Obstetric morbidities, n (%) | 26 (23.9%) | 14 (21.2%) | 12 (27.9%) | 0.425 |
| Multiparous, n (%) | 67 (60.9%) | 40 (58.8%) | 27 (64.3%) | 0.568 |
| Onset of symptoms in pregnancy, n (%) | 93 (84.6%) | 57 (83.8%) | 36 (85.7%) | 0.789 |
| Gestational age at triage, mean (CI 95%) | 27.7 (25.5–29.9) | 28.6 (25.8–31.4) | 26.2 (22.5–29.9) | 0.302 |
| Maternal Signs and Symptoms | ||||
| Fever, n (%) | 61 (55.0%) | 36 (52.9%) | 25 (58.1%) | 0.591 |
| Cough, n (%) | 59 (53.2%) | 37 (54.4%) | 22 (51.2%) | 0.738 |
| Shortness of breath, n (%) | 33 (29.7%) | 20 (29.4%) | 13 (30.2%) | 0.927 |
| Diarrhoea, n (%) | 7 (6.3%) | 4 (5.9%) | 3 (7.7%) | 0.818 |
| Temperature, mean (CI 95%) | 36.7 (36.5–37.0) | 36.7 (36.5–37.1) | 36.7 (36.5–37.1) | 0.884 |
| Oxygen saturation, mean (CI 95%) | 96.6 (95.8–97.4) | 96.4 (95.7–97.1) | 96.9 (95.2–98.5) | 0.571 |
| Breathing frequency, mean (CI 95%) | 22.1 (19.9–24.2) | 23.3 (20.1–26.5) | 20.0 (17.9–22.1) | 0.139 |
| Complementary Maternal Studies | ||||
| Pneumonia, n (%) | 40 (36.4%) | 31 (45.6%) | 9 (21.4%) | 0.009 |
| Leukocytes, mean (CI 95%) | 11,465.7 (7963.6–14,967.8) | 9762.2 (7255.7–12,268.6) | 14,021 (5948.0–22,094.0) | 0.239 |
| Lymphocytes, mean (CI 95%) | 1351 (1234.6–1467.4) | 1301.7 (1160.9–1442.5) | 1425 (1218.9–1631.1) | 0.306 |
| Monocytes, mean (CI 95%) | 690.7 (508.4–872.9) | 518.8 (441.0–596.6) | 946.2 (508.5–1383.8) | 0.022 |
| Platelets, mean (CI 95%) | 215,511.8 (195,538.3–235,485.4) | 200,453 (178,323.5–222,582.6) | 238,100 (200,601.0–275,599.0) | 0.067 |
| LDH, mean (CI 95%) | 201.6 (182.5–220.6) | 224.5 (198.1–250.8) | 168 (144.9–191.1) | 0.003 |
| Maternal Treatments | ||||
| Antivirals, n (%) | 29 (26.4) | 24 (35.3%) | 5 (11.9%) | 0.005 |
| Antibiotics, n (%) | 36 (32.7%) | 29 (42.7%) | 7 (16.7%) | 0.004 |
| Antirheumatics, n (%) | 28 (25.5%) | 23 (33.8%) | 5 (11.9%) | 0.008 |
| Anticoagulants, n (%) | 38 (34.6%) | 34 (50.0%) | 4 (9.5%) | <0.001 |
| Maternal–Perinatal Outcomes | ||||
| Oxygen therapy, n (%) | 20 (18.5%) | 19 (28.8%) | 1 (2.4%) | <0.001 |
| Admission to ICU, n (%) | 4 (3.7%) | 4 (6.0%) | 0 (0.0%) | 0.046 |
| C-section | 23 (44.2%) | 19 (48.7%) | 4 (30.8%) | 0.253 |
| Prematurity | 15 (28.9%) | 13 (33.3%) | 2 (15.4%%) | 0.196 |
| Neonatal birthweight, mean (CI 95%) | 2806.1 (2588.2–3025.3) | 2755.3 (2487.2–3023.5) | 2953.1 (2550.6–3355.5) | 0.431 |
| Apgar score at five minutes, mean (CI 95%) | 9.5 (9.3-9.8) | 9.5 (9.2–9.9) | 9.6 (9.2–10.0) | 0.865 |
| Admission to NICU, mean (CI 95%) | 17 (32.7%) | 134 (35.9%) | 3 (23.1%) | 0.383 |
| Neonatal mortality, n (%) | 2 (4.2%) | 2 (5.7%) | 0 (0.0%) | 0.255 |
| COVID-19 Severity | Overall | RT-PCR Positive | RT-PCR Negative | p-Value |
|---|---|---|---|---|
| N, (%) | 111 | 68 | 43 | 0.022 |
| Mild, n (%) | 71 (64.0%) | 37 (52.4%) | 34 (79.1%) | |
| Moderate, n (%) | 26 (23.4%) | 19 (27.9%) | 7 (16.3%) | |
| Severe, n (%) | 10 (9.0%) | 8 (11.8%) | 2 (4.7%) | |
| Critical, n (%) | 4 (3.6%) | 4 (5.9%) | 0 (0.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuñarro-López, Y.; Cano-Valderrama, Ó.; Pintado-Recarte, P.; Cueto-Hernández, I.; González-Garzón, B.; García-Tizón, S.; Bujan, J.; Asúnsolo, Á.; Ortega, M.A.; De León-Luis, J.A. Maternal and Perinatal Outcomes in Patients with Suspected COVID-19 and Their Relationship with a Negative RT-PCR Result. J. Clin. Med. 2020, 9, 3552. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113552
Cuñarro-López Y, Cano-Valderrama Ó, Pintado-Recarte P, Cueto-Hernández I, González-Garzón B, García-Tizón S, Bujan J, Asúnsolo Á, Ortega MA, De León-Luis JA. Maternal and Perinatal Outcomes in Patients with Suspected COVID-19 and Their Relationship with a Negative RT-PCR Result. Journal of Clinical Medicine. 2020; 9(11):3552. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113552
Chicago/Turabian StyleCuñarro-López, Yolanda, Óscar Cano-Valderrama, Pilar Pintado-Recarte, Ignacio Cueto-Hernández, Blanca González-Garzón, Santiago García-Tizón, Julia Bujan, Ángel Asúnsolo, Miguel A. Ortega, and Juan Antonio De León-Luis. 2020. "Maternal and Perinatal Outcomes in Patients with Suspected COVID-19 and Their Relationship with a Negative RT-PCR Result" Journal of Clinical Medicine 9, no. 11: 3552. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113552