Risk and Severity of COVID-19 and ABO Blood Group in Transcatheter Aortic Valve Patients

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
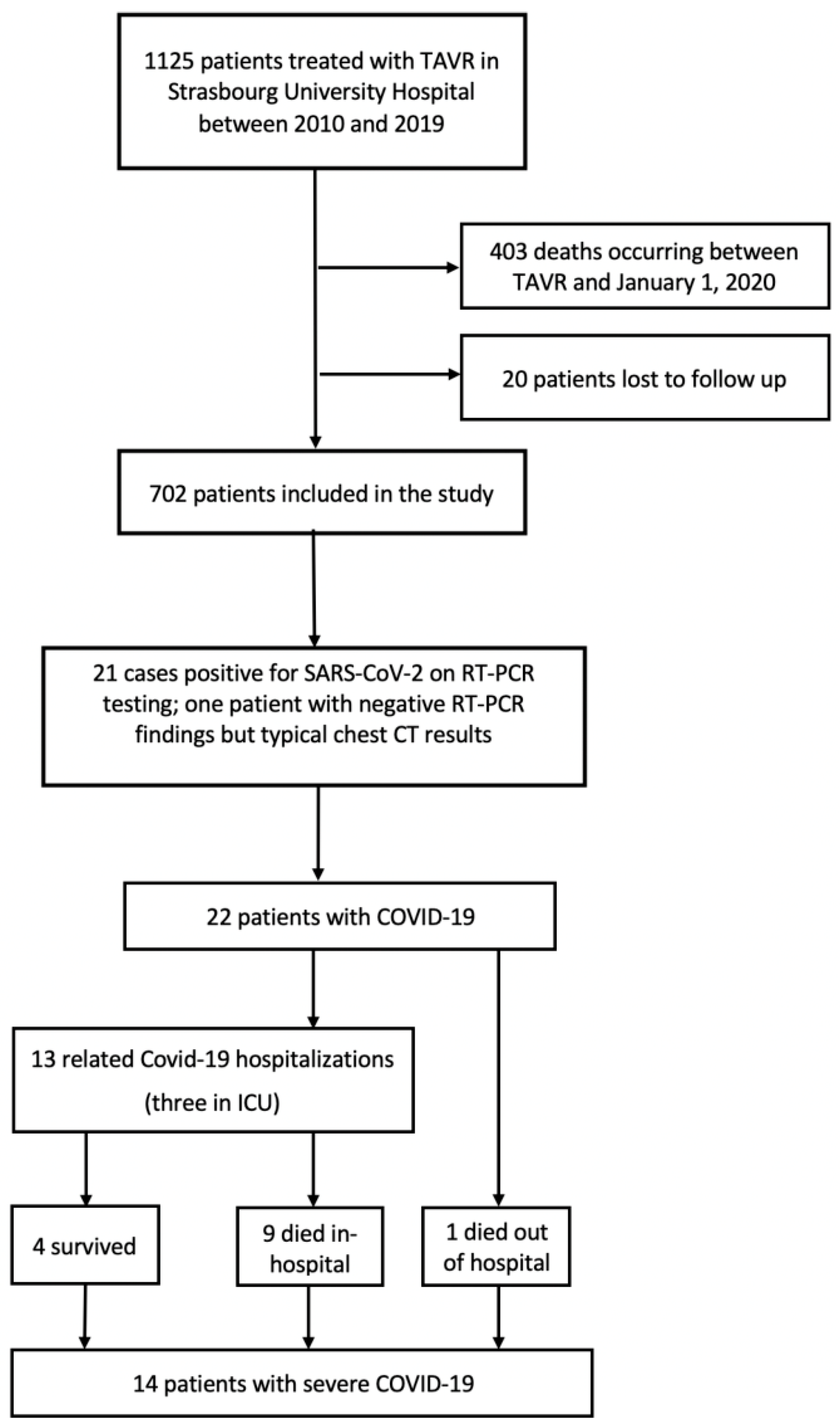
2.1. Study Setting and Patient Enrollment
2.2. Definitions
2.3. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Occurrence and Presentation of COVID-19
3.3. COVID-19, Hospitalizations and Mortality
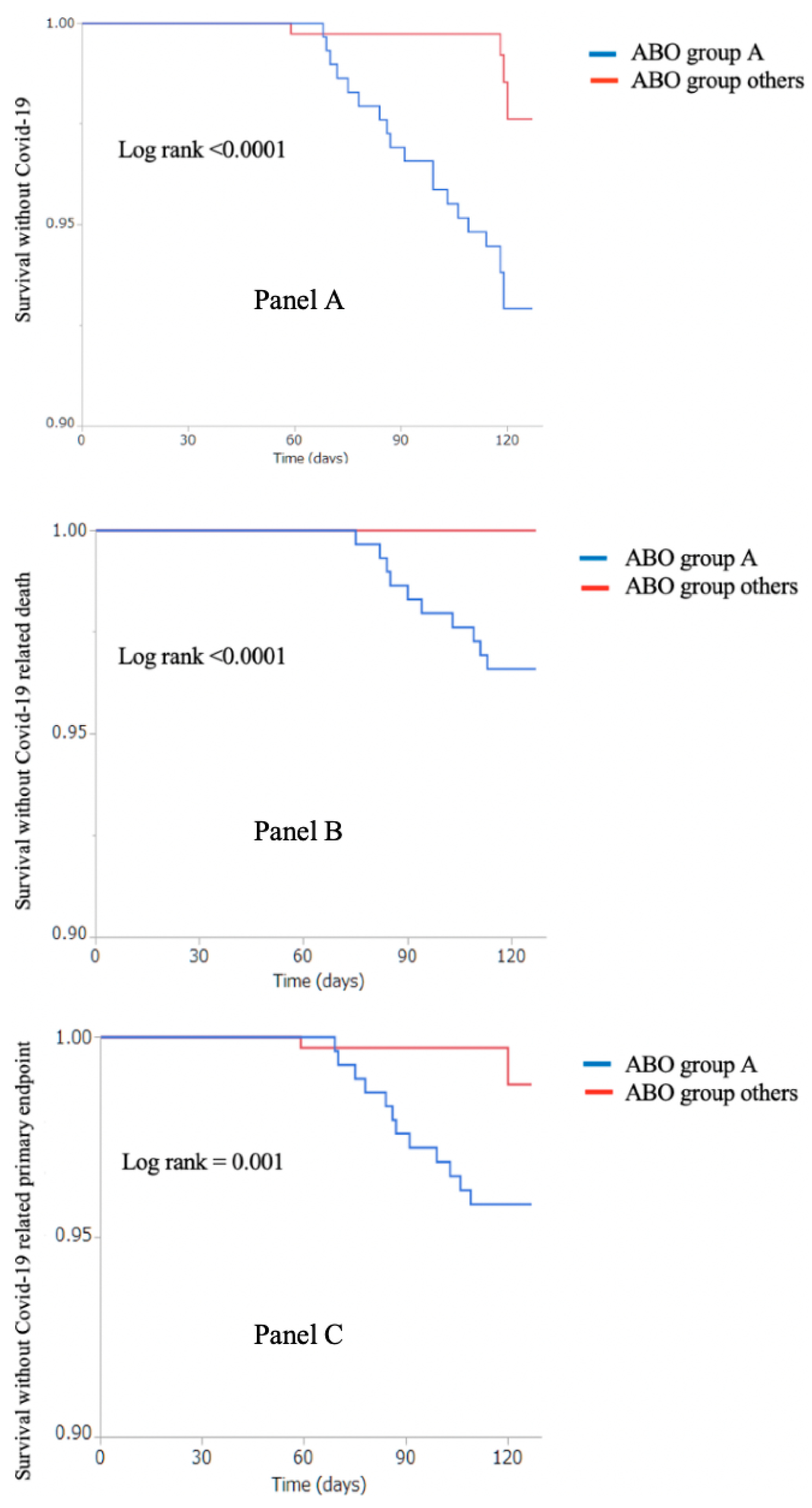
3.4. COVID-19 and ABO blood group
3.5. Predictors of COVID-19
3.6. Predictors of Severe COVID-19
4. Discussion
4.1. Prevalence of COVID-19
4.2. ABO Blood Group and COVID-19
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Situation Report, World Health Organization. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200514-covid-19-sitrep-115.pdf?sfvrsn=3fce8d3c_6 (accessed on 20 May 2020).
- Ministry of Health France. Tableau de Bord des Données Régionales. Published online May 2020. Available online: https://www.grand-est.ars.sante.fr/system/files/2020-05/2020-05-15_Données%20du%20jour.pdf (accessed on 20 May 2020).
- COVID-19: Point épidémiologique hebdomadaire du14 mai 2020. Ministry of Health France. Published online May 2020. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-14-mai-2020 (accessed on 20 May 2020).
- Inciardi, R.M.; Adamo, M.; Lupi, L.; Cani, D.S.; Di Pasquale, M.; Tomasoni, D.; Italia, L.; Zaccone, G.; Tedino, C.; Fabbricatore, D.; et al. Characteristics and outcomes of patients hospitalized for COVID-19 and cardiac disease in Northern Italy. Eur. Heart J. 2020, 41, 1821–1829. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Cheng, G.; Chui, C.H.; Lau, F.Y.; Chan, P.K.S.; Ng, M.H.L.; Sung, J.J.Y.; Wong, R.S.M. ABO Blood Group and Susceptibility to Severe Acute Respiratory Syndrome. JAMA 2005, 293, 1447–1451. [Google Scholar] [CrossRef]
- Wang, D.-S.; Chen, D.-L.; Ren, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. ABO blood group, hepatitis B viral infection and risk of pancreatic cancer. Int. J. Cancer 2012, 131, 461–468. [Google Scholar] [CrossRef]
- Lindesmith, L.; Moe, C.; Marionneau, S.; Ruvoen, N.; Jiang, X.; Lindblad, L.; Stewart, P.; LePendu, J.; Baric, R. Human susceptibility and resistance to Norwalk virus infection. Nat. Med. 2003, 9, 548–553. [Google Scholar] [CrossRef]
- Boren, T.; Falk, P.; Roth, K.; Larson, G.; Normark, S. Attachment of Helicobacter pylori to human gastric epithelium mediated by blood group antigens. Science 1993, 262, 1892–1895. [Google Scholar] [CrossRef]
- Dai, X. ABO blood group predisposes to COVID-19 severity and cardiovascular diseases. Eur. J. Prev. Cardiol. 2020, 27. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Chen, J.; Cai, Y.; Deng, A.; Yang, M. Association between ABO blood groups and risk of SARS-CoV-2 pneumonia. Br. J. Haematol. 2020, 190, bjh.16797. [Google Scholar] [CrossRef]
- O’Sullivan, J.M.; Ward, S.; Fogarty, H.; O’Donnell, J.S. More on “Association between ABO blood groups and risk of SARS-CoV-2 Pneumonia”. Br. J. Haematol. 2020, 190, bjh.16845. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Global Surveillance for COVID-19 Caused by Human Infection with COVID-19 Virus: Interim Guidance. 2020. Available online: https://apps.who.int/iris/handle/10665/331506 (accessed on 20 May 2020).
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, 200642. [Google Scholar] [CrossRef] [Green Version]
- Info Coronavirus Covid 19—Carte et Donnees Covid 19 en France. Gouvernement.fr. Available online: https://www.gouvernement.fr/info-coronavirus/carte-et-donnees (accessed on 20 May 2020).
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Gheblawi, M.; Oudit, G.Y. Angiotensin Converting Enzyme 2: A Double-Edged Sword. Circulation 2020, 142. [Google Scholar] [CrossRef] [PubMed]
- Sriram, K.; Insel, P.A. Dangers of ACE Inhibitor and ARB Usage in COVID-19: Evaluating the Evidence. Pharmacol. Ther. 2020. [Google Scholar] [CrossRef]
- Kuster, G.M.; Pfister, O.; Burkard, T.; Zhou, Q.; Twerenbold, R.; Haaf, P.; Widmer, A.F.; Osswald, S. SARS-CoV2: Should inhibitors of the renin–angiotensin system be withdrawn in patients with COVID-19? Eur. Heart J. 2020, 41. [Google Scholar] [CrossRef] [Green Version]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383. [Google Scholar] [CrossRef]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef]
- Zhao, J.; Yang, Y.; Huang, H.; Li, D.; Gu, D.; Lu, X.; Zhang, Z.; Liu, L.; Liu, T.; Liu, Y.; et al. Relationship between the ABO Blood Group and the COVID-19 Susceptibility. Epidemiology 2020. Preprint. [Google Scholar] [CrossRef] [Green Version]
- Zietz, M.; Tatonetti, N.P. Testing the Association between Blood Type and COVID-19 Infection, Intubation, and Death. Infect. Dis. (Except HIV/AIDS) 2020. [Google Scholar] [CrossRef] [Green Version]
- Guillon, P.; Clément, M.; Sébille, V.; Rivain, J.-G.; Chou, C.-F.; Ruvoën-Clouet, N.; Le Pendu, J. Inhibition of the interaction between the SARS-CoV Spike protein and its cellular receptor by anti-histo-blood group antibodies. Glycobiology 2008, 18, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Wu, O.; Bayoumi, N.; Vickers, M.A.; Clark, P. ABO(H) blood groups and vascular disease: A systematic review and meta-analysis: ABO groups and thrombosis. J. Thromb. Haemost. 2007, 6, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Paré, G.; Chasman, D.I.; Kellogg, M.; Zee, R.Y.L.; Rifai, N.; Badola, S.; Miletich, J.P.; Ridker, P.M. Novel Association of ABO Histo-Blood Group Antigen with Soluble ICAM-1: Results of a Genome-Wide Association Study of 6578 Women. Gibson, G., Ed. PLoS Genet. 2008, 4, e1000118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunne, E.; Qi, Q.M.; Shaqfeh, E.S.; O’Sullivan, J.M.; Schoen, I.; Ricco, A.J.; O’Donnell, J.S.; Kenny, D. Blood group alters platelet binding kinetics to von Willebrand factor and consequently platelet function. Blood 2019, 133, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Bowen, D.J. An influence of ABO blood group on the rate of proteolysis of von Willebrand factor by ADAMTS13. J. Thromb. Haemost. 2003, 1, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Ellinghaus, D.; Degenhardt, F.; Bujanda, L.; Buti, M.; Albillos, A.; Invernizzi, P.; Fernández, J.; Prati, D.; Baselli, G.; Asselta, R.; et al. Genomewide Association Study of Severe Covid-19 with Respiratory Failure. N. Engl. J. Med. 2020, 383. [Google Scholar] [CrossRef]
- Ahamed, J. Severe aortic stenosis patient risk during the COVID-19 pandemic. Open Heart. 2020, 7, e001355. [Google Scholar] [CrossRef] [PubMed]
- Ryffel, C.; Lanz, J.; Corpataux, N.; Reusser, N.; Stortecky, S.; Windecker, S.; Pilgrim, T. Mortality, Stroke, and Hospitalization Associated with Deferred vs Expedited Aortic Valve Replacement in Patients Referred for Symptomatic Severe Aortic Stenosis During the COVID-19 Pandemic. JAMA Netw Open. 2020, 3. [Google Scholar] [CrossRef]
- Tanguturi, V.K.; Lindman, B.R.; Pibarot, P.; Passeri, J.J.; Kapadia, S.; Mack, M.J.; Inglessis, I.; Langer, N.B.; Sundt, T.M.; Hung, J.; et al. Managing Severe Aortic Stenosis in the COVID-19 Era. Jacc. Cardiovasc. Interv. 2020, 13, 1937–1944. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Characteristics | Entire Cohort (n = 702) | COVID-19 (n = 22) | No COVID-19 (n = 680) | p Value |
|---|---|---|---|---|
| Age, years | 82 ± 6.9 | 82 ± 8.4 | 82 ± 6.9 | 0.961 |
| Male sex–n (%) | 313 (44) | 7 (31.8) | 306 (45) | 0.220 |
| STS score–% | 5.9 ± 4.9 | 5.5 ± 2.4 | 5.9 ± 5.0 | 0.757 |
| Cardiovascular risk factors–n (%) | ||||
| Current smoking | 26 (3.7) | 1 (4.5) | 25 (3.7) | 0.832 |
| Hypertension | 587 (83.6) | 18 (81.8) | 569 (83.7) | 0.817 |
| Obesity (Body mass index > 30 kg/m2) | 183 (26.1) | 6 (27.3) | 177 (26.1) | 0.899 |
| Dyslipidemia | 428 (61) | 12 (54.5) | 416 (61.2) | 0.530 |
| Diabetes | 213 (30.3) | 6 (27.3) | 207 (30.4) | 0.750 |
| Comorbidities–n (%) | ||||
| Coronary artery disease | 318 (45.3) | 12 (54.5) | 306 (45.0) | 0.376 |
| Congestive heart failure | 252 (35.9) | 6 (27.3) | 246 (36.5) | 0.392 |
| Stroke | 98 (14) | 3 (13.6) | 95 (14.0) | 0.964 |
| Atrial fibrillation | 283 (40.3) | 6 (27.3) | 277 (40.7) | 0.205 |
| Peripheral arterial disease | 191 (27.2) | 5 (22.7) | 186 (27.4) | 0.631 |
| COPD | 82 (11.7) | 3 (13.6) | 79 (11.6) | 0.740 |
| Prior cancer | 189 (26.9) | 10 (45.5) | 179 (26.3) | 0.053 |
| CKD (Creatinine levels > 130 μmol/L) | 115 (16.5) | 4 (18.2) | 111 (16.4) | 0.824 |
| LVEF after TAVR–% | 56 ± 11 | 56 ± 12 | 56 ± 11 | 0.902 |
| Treatment at time of follow up–n (%) | ||||
| Aspirin | 365 (53.3) | 13 (59.1) | 352 (53.1) | 0.579 |
| P2Y12 inhibitors | ||||
| VKA | 144 (21.0) | 4 (18.2) | 140 (21.1) | 0.740 |
| DOAC | 175 (25.5) | 6 (27.3) | 169 (25.5) | 0.850 |
| ACE-i/ARB | 335 (48.9) | 12 (54.5) | 323 (48.7) | 0.591 |
| Statins | 344 (50.2) | 9 (40.9) | 335 (50.5) | 0.375 |
| Amiodarone | 101 (14.7) | 2 (9.1) | 99 (14.9) | 0.447 |
| ABO blood type–n (%) | ||||
| A | 299 (42.6) | 18 (81.8) | 281 (41.3) | 0.002 |
| B | 63 (9) | 0 (0) | 63 (9.3) | |
| AB | 20 (2.9) | 0 (0) | 20 (2.9) | |
| O | 320 (45.6) | 4 (18.2) | 316 (46.5) | |
| Rhesus positive (Rh+)–n (%) | 352 (58.6) | 11 (68.8) | 341 (58.3) | 0.402 |
| Blood type–no. (%) | ||||
| A Rh- | 87 (12.4) | 3 (13.6) | 84 (12.4) | 0.027 |
| A Rh+ | 212 (30.2) | 15 (68.2) | 197 (29.0) | |
| AB Rh- | 8 (1.1) | 0 (0) | 8 (1.2) | |
| AB Rh+ | 17 (2.4) | 0 (0) | 17 (2.5) | |
| B Rh- | 14 (2.0) | 0 (0) | 14 (2.1) | |
| B Rh+ | 49 (7.0) | 0 (0) | 49 (7.2) | |
| O Rh- | 74 (10.5) | 1 (4.5) | 73 (10.7) | |
| O Rh+ | 154 (21.9) | 2 (9.1) | 152 (22.4) | |
| Missing | 87 (12.4) | 1 (4.5) | 86 (12.6) | |
| Entire Cohort (n = 702) | COVID-19 (n = 22) | No COVID-19 (n = 680) | p Value | |
|---|---|---|---|---|
| Hospitalization–n (%) | 25 (3.6) | 13 (59.1) | 12 (1.8) | <0.0001 |
| Conventional unit | 22 (3.2) | 10 (45.5) | 12 (1.8) | <0.0001 |
| Intensive care unit | 3 (0.44) | 3 (13.6) | 0 (0) | <0.0001 |
| Mortality from January 1, 2020–n (%) | ||||
| All-cause mortality | 48 (6.8) | 10 (45.5) | 38 (5.6) | <0.0001 |
| Cardiovascular mortality | 20 (2.8) | 0 (0) | 20 (2.8) | 0.414 |
| COVID-19 mortality | 10 (1.5) | 10 (45.5) | 0 (0) | <0.0001 |
| COVID-19 severity–n (%) | ||||
| COVID-19 related hospitalization or death | 14 (2.0) | 14 (63.6) | 0 (0) | <0.0001 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age | 0.99 | 0.94–1.06 | 0.610 | |||
| Male sex | 0.57 | 0.23–1.42 | 0.226 | |||
| Diabetes | 0.86 | 0.33–2.22 | 0.751 | |||
| Obesity | 0.89 | 0.41–2.76 | 0.899 | |||
| Hypertension | 0.89 | 0.29–2.64 | 0.817 | |||
| Dyslipidemia | 0.76 | 0.32–1.79 | 0.531 | |||
| Current smoking | 0.83 | 0.16–9.65 | 0.832 | |||
| Atrial fibrillation | 0.55 | 0.21–1.41 | 0.212 | |||
| Peripheral artery disease | 0.78 | 0.28–2.15 | 0.632 | |||
| CKD (Creatinine levels > 130 umol/L) | 1.13 | 0.38–3.41 | 0.703 | |||
| Prior cancer | 2.33 | 0.99–5.49 | 0.053 | 2.28 | 0.96–5.43 | 0.062 |
| ACE-i/ARBs | 1.26 | 0.54–2.96 | 0.591 | |||
| P2Y12 inhibitors | 0.70 | 0.09–5.37 | 0.736 | |||
| Aspirin | 1.28 | 0.54–3.03 | 0.580 | |||
| Statins | 0.68 | 0.29–1.61 | 0.377 | |||
| A blood group | 6.29 | 2.14–19.08 | 0.001 | 6.32 | 2.11–18.92 | 0.001 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age | 0.98 | 0.92–1.05 | 0.649 | |||
| Sex (male) | 0.68 | 0.23–2.07 | 0.502 | |||
| Diabetes | 1.74 | 0.59–5.09 | 0.309 | |||
| Obesity | 0.77 | 0.21–2.78 | 0.688 | |||
| Hypertension | 0.71 | 0.19–2.59 | 0.608 | |||
| Dyslipidemia | 0.85 | 0.29–2.48 | 0.767 | |||
| Atrial fibrillation | 0.57 | 0.18–1.69 | 0.371 | |||
| Peripheral artery disease | 1.07 | 0.33–3.47 | 0.908 | |||
| CKD (Cr > 130 umol/L) | 2.07 | 0.64–6.71 | 0.226 | |||
| Coronary artery disease | 1.63 | 0.56–4.74 | 0.373 | |||
| Heart failure | 0.71 | 0.22–2.29 | 0.566 | |||
| COPD | 1.26 | 0.28–5.75 | 0.761 | |||
| Stroke | 1.03 | 0.23–4.66 | 0.972 | |||
| Prior cancer | 5.08 | 1.68–15.34 | 0.004 | 4.99 | 1.64–15.27 | 0.005 |
| A blood group | 8.38 | 1.86–37.74 | 0.006 | 8.27 | 1.83–37.43 | 0.006 |
| O blood group | 0.19 | 0.04–0.87 | 0.033 | |||
| Aspirin | 0.87 | 0.30–2.52 | 0.804 | |||
| ACE-i/ARB | 1.05 | 0.36–3.01 | 0.934 | |||
| Statins | 0.74 | 0.25–2.15 | 0.579 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kibler, M.; Dietrich, L.; Kanso, M.; Carmona, A.; Marchandot, B.; Matsushita, K.; Trimaille, A.; How-Choong, C.; Odier, A.; Gennesseaux, G.; et al. Risk and Severity of COVID-19 and ABO Blood Group in Transcatheter Aortic Valve Patients. J. Clin. Med. 2020, 9, 3769. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113769
Kibler M, Dietrich L, Kanso M, Carmona A, Marchandot B, Matsushita K, Trimaille A, How-Choong C, Odier A, Gennesseaux G, et al. Risk and Severity of COVID-19 and ABO Blood Group in Transcatheter Aortic Valve Patients. Journal of Clinical Medicine. 2020; 9(11):3769. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113769
Chicago/Turabian StyleKibler, Marion, Laurent Dietrich, Mohamad Kanso, Adrien Carmona, Benjamin Marchandot, Kensuke Matsushita, Antonin Trimaille, Cécile How-Choong, Albane Odier, Gabrielle Gennesseaux, and et al. 2020. "Risk and Severity of COVID-19 and ABO Blood Group in Transcatheter Aortic Valve Patients" Journal of Clinical Medicine 9, no. 11: 3769. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113769