Social Stress-Induced Oxidative DNA Damage Is Related to Prospective Cardiovascular Risk

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
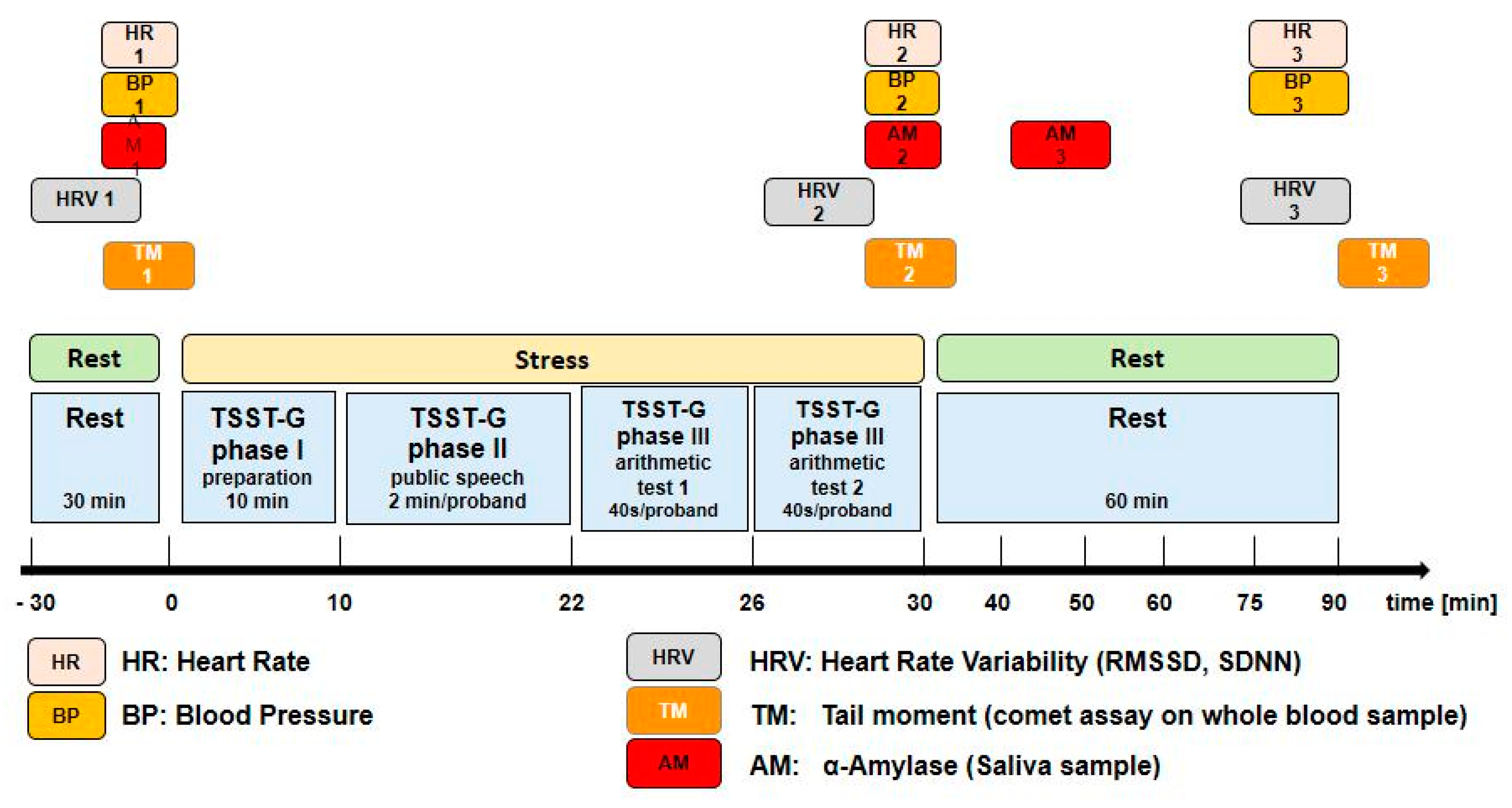
2. Methods
Statistical Analysis
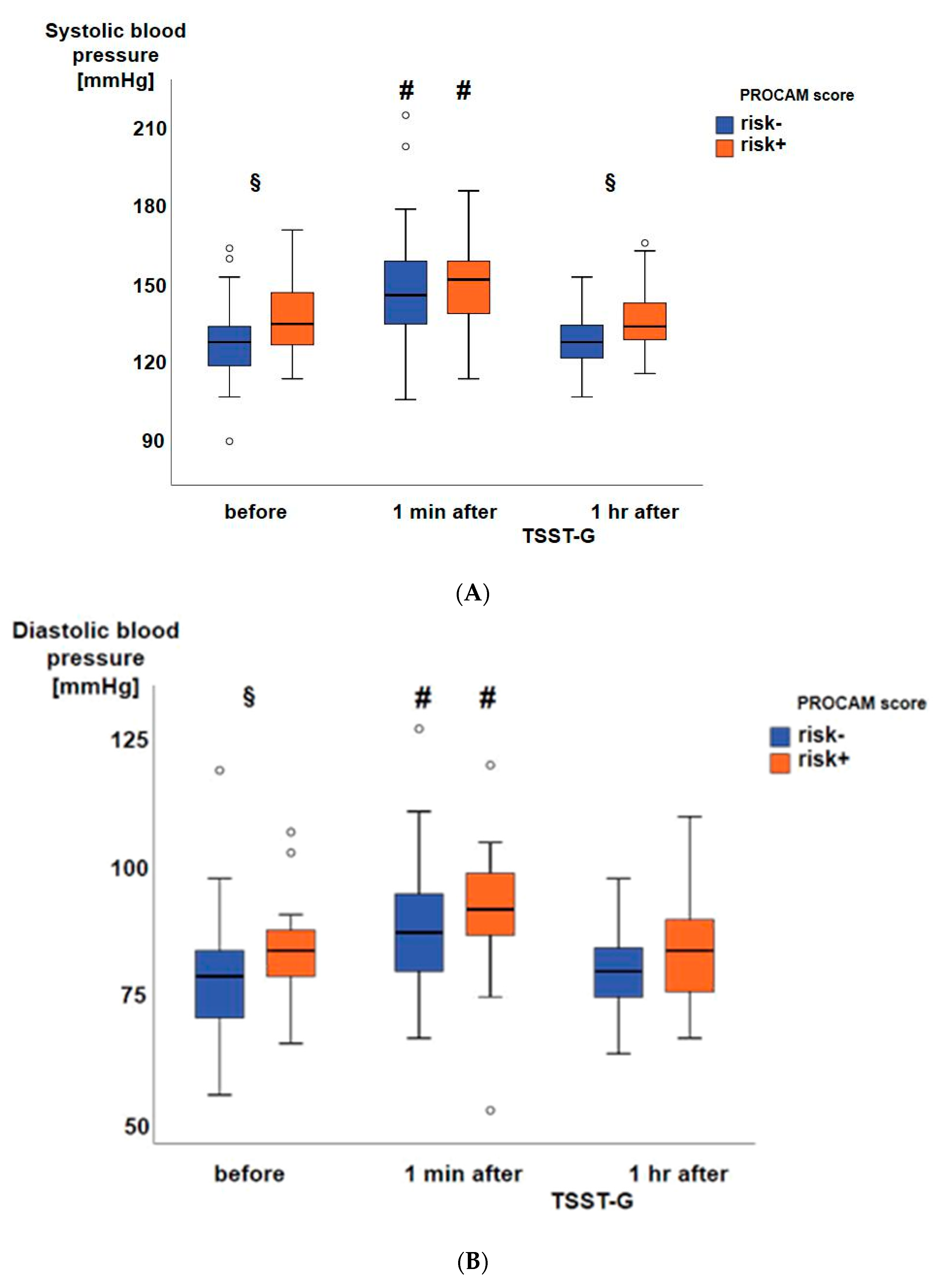
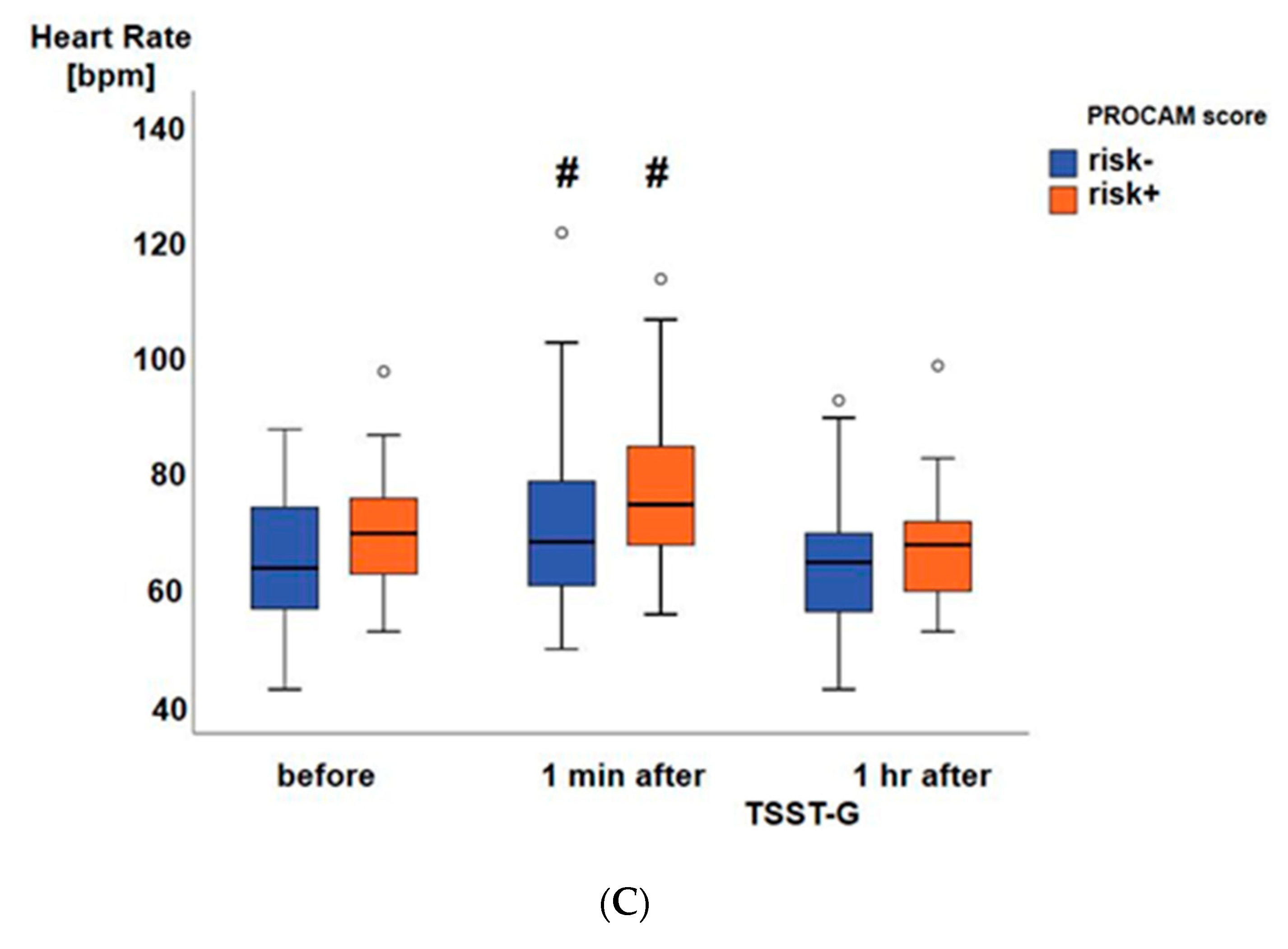
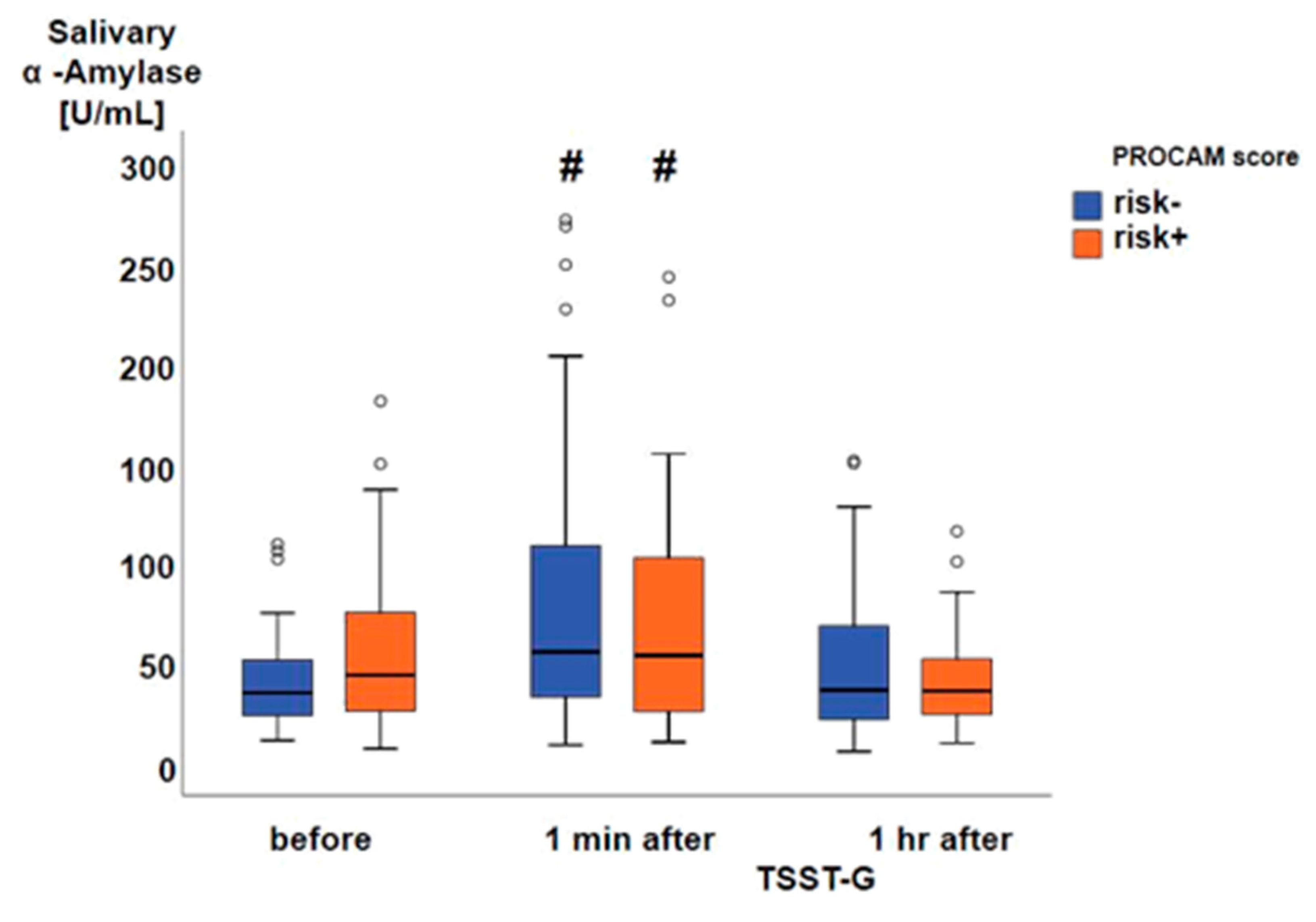
3. Results
4. Discussion
4.1. Limitations of The Study
4.2. Clinical Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pereira, V.H.; Cerqueira, J.J.; Palha, J.A.; Sousa, N. Stressed brain, diseased heart: A review on the pathophysiologic mechanisms of neurocardiology. Int. J. Cardiol. 2013, 166, 30–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waller, C.; Bauersachs, J.; Hoppmann, U.; Höch, J.; Krause, S.; Szabo, F.; Engler, H.; Rottler, E.; Herrmann-Lingen, C.; Gündel, H. Blunted Cortisol Stress Response and Depression-Induced Hypocortisolism Is Related to Inflammation in Patients With CAD. J. Am. Coll. Cardiol. 2016, 67, 1124–1126. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Rump, A.F.E.; Klaus, W. Evidence for norepinephrine cardiotoxicity mediated by superoxide anion radicals in isolated rabbit hearts. Naunyn. Schmiedebergs. Arch. Pharmacol. 1994, 349, 295–300. [Google Scholar] [CrossRef]
- Neri, M.; Cerretani, D.; Fiaschi, A.I.; Laghi, P.F.; Lazzerini, P.E.; Maffione, A.B.; Micheli, L.; Bruni, G.; Nencini, C.; Giorgi, G.; et al. Correlation between cardiac oxidative stress and myocardial pathology due to acute and chronic norepinephrine administration in rats. J. Cell. Mol. Med. 2007, 11, 156–170. [Google Scholar] [CrossRef]
- Møller, P.; Stopper, H.; Collins, A.R. Measurement of DNA damage with the comet assay in high-prevalence diseases: Current status and future directions. Mutagenesis 2020, 35, 5–18. [Google Scholar] [CrossRef]
- Kliemann, M.; Prá, D.; Müller, L.L.; Hermes, L.; Horta, J.A.; Reckziegel, M.B.; Burgos, M.S.; Maluf, S.W.; Franke, S.I.R.; da Silva, J. DNA damage in children and adolescents with cardiovascular disease risk factors. An. Acad. Bras. Cienc. 2012, 84, 833–840. [Google Scholar] [CrossRef] [Green Version]
- von Dawans, B.; Kirschbaum, C.; Heinrichs, M. The Trier Social Stress Test for Groups (TSST-G): A new research tool for controlled simultaneous social stress exposure in a group format. Psychoneuroendocrinology 2011, 36, 514–522. [Google Scholar] [CrossRef]
- Assmann, G.; Cullen, P.; Schulte, H. Simple Scoring Scheme for Calculating the Risk of Acute Coronary Events Based on the 10-Year Follow-up of the Prospective Cardiovascular Münster (PROCAM) Study. Circulation 2002, 105, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart Rate Variability Standards of Measurement, Physiological Interpretation, and Clinical Use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Umetani, K.; Singer, D.H.; McCraty, R.; Atkinson, M. Twenty-four hour time domain heart rate variability and heart rate: Relations to age and gender over nine decades. J. Am. Coll. Cardiol. 1998, 31, 593–601. [Google Scholar] [CrossRef]
- Gröger, M.; Öter, S.; Simkova, V.; Bolten, M.; Koch, A.; Warninghoff, V.; Georgieff, M.; Muth, C.M.; Speit, G.; Radermacher, P. DNA damage after long-term repetitive hyperbaric oxygen exposure. J. Appl. Physiol. 2009, 106, 311–315. [Google Scholar] [CrossRef] [Green Version]
- Witte, J.; Kähler, W.; Wunderlich, T.; Radermacher, P.; Wohlrab, C.; Koch, A. Dose-time dependency of hyperbaric hyperoxia-induced DNA-strand breaks in human immune cells visualized with the Comet Assay. Undersea Hyperb. Med. 2014, 41, 171–181. [Google Scholar] [PubMed]
- Rohleder, N.; Wolf, J.M.; Maldonado, E.F.; Kirschbaum, C. The psychosocial stress-induced increase in salivary alpha-amylase is independent of saliva flow rate. Psychophysiology 2006, 43, 645–652. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.E.; Rijnbeek, P.R.; Niemeijer, M.N.; Hofman, A.; van Herpen, G.; Bots, M.L.; Hillege, H.; Swenne, C.A.; Eijgelsheim, M.; Stricker, B.H.; et al. Normal Values of Corrected Heart-Rate Variability in 10-Second Electrocardiograms for All Ages. Front. Physiol. 2018, 9, 424. [Google Scholar] [CrossRef]
- Dimitroglou, E.; Zafiropoulou, M.; Messini-Nikolaki, N.; Doudounakis, S.; Tsilimigaki, S.; Piperakis, S.M. DNA damage in a human population affected by chronic psychogenic stress. Int. J. Hyg. Environ. Health 2003, 206, 39–44. [Google Scholar] [CrossRef]
- Boeck, C.; Gumpp, A.M.; Koenig, A.M.; Radermacher, P.; Karabatsiakis, A.; Kolassa, I.T. The association of childhood maltreatment with lipid peroxidation and DNA damage in postpartum women. Front. Psychiatry 2019, 10, 23. [Google Scholar] [CrossRef] [Green Version]
- Sivonová, M.; Zitnanová, I.; Hlincíková, L.; Skodácek, I.; Trebatická, J.; Duracková, Z. Oxidative stress in university students during examinations. Stress 2004, 7, 183–188. [Google Scholar] [CrossRef]
- Tryfidou, D.V.; McClean, C.; Nikolaidis, M.G.; Davison, G.W. DNA Damage Following Acute Aerobic Exercise: A Systematic Review and Meta-analysis. Sports Med. 2020, 50, 103–127. [Google Scholar] [CrossRef] [Green Version]
- Plappert-Helbig, U.; Guérard, M. Inter-laboratory comparison of the in vivo comet assay including three image analysis systems. Environ. Mol. Mutagen. 2015, 56, 788–793. [Google Scholar] [CrossRef]
- Collins, A.R.; El Yamani, N.; Lorenzo, Y.; Shaposhnikov, S.; Brunborg, G.; Azqueta, A. Controlling variation in the comet assay. Front. Genet. 2014, 5, 359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muth, C.M.; Glenz, Y.; Klaus, M.; Radermacher, P.; Speit, G.; Leverve, X. Influence of an orally effective SOD on hyperbaric oxygen-related cell damage. Free Radic. Res. 2004, 38, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Speit, G.; Dennog, C.; Radermacher, P.; Rothfuss, A. Genotoxicity of hyperbaric oxygen. Mutat. Res. 2002, 512, 111–119. [Google Scholar] [CrossRef]
- Matheny, M.; McPheeters, M.L.; Glasser, A.; Mercaldo, N.; Weaver, R.B.; Jerome, R.N.; Walden, R.; McKoy, J.N.; Pritchett, J.; Tsai, C. Systematic Review of Cardiovascular Disease Risk Assessment Tools; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011.
- Hense, H.W.; Schulte, H.; Löwel, H.; Assmann, G.; Keil, U. Framingham risk function overestimates risk of coronary heart disease in men and women from Germany-results from the MONICA Augsburg and the PROCAM cohorts. Eur. Heart. J. 2003, 24, 937–945. [Google Scholar] [CrossRef]
- Vrentzos, G.E.; Papadakis, J.A.; Ganotakis, E.S.; Paraskevas, K.I.; Gazi, I.F.; Tzanakis, N.; DNair, D.R.; Mikhailidis, D.P. Predicting coronary heart disease risk using the Framingham and PROCAM equations in dyslipidaemic patients without overt vascular disease. Int. J. Clin. Pract. 2007, 61, 1643–1653. [Google Scholar] [CrossRef] [PubMed]
- Dent, T.H.S. Predicting the risk of coronary heart disease I. The use of conventional risk markers. Atherosclerosis 2010, 213, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.M.; McKechnie, P.S.; Macfarlane, P.W. Can cardiac vagal tone be estimated from the 10-s ECG? Int. J. Cardiol. 2004, 95, 109–115. [Google Scholar] [CrossRef]
- Schuster, A.K.; Fischer, J.E.; Thayer, J.F.; Mauss, D.; Jarczok, M.N. Decreased heart rate variability correlates to increased cardiovascular risk. Int. J. Cardiol. 2016, 203, 728–730. [Google Scholar] [CrossRef]
- Thoma, M.V.; Kirschbaum, C.; Wolf, J.M.; Rohleder, N. Acute stress responses in salivary alpha-amylase predict increases of plasma norepinephrine. Biol. Psychol. 2012, 91, 342–348. [Google Scholar] [CrossRef]
- Maruyama, Y.; Kawano, A.; Okamoto, S.; Ando, T.; Ishitobi, Y.; Tanaka, Y.; Inoue, A.; Imanaga, J.; Kanehisa, M.; Higuma, H.; et al. Differences in salivary alpha-amylase and cortisol responsiveness following exposure to electrical stimulation versus the Trier Social Stress Tests. PLoS ONE 2012, 7, e39375. [Google Scholar] [CrossRef]
- Petrakova, L.; Doering, B.K.; Vits, S.; Engler, H.; Rief, W.; Schedlowski, M.; Grigoleit, J.S. Psychosocial Stress Increases Salivary Alpha-Amylase Activity Independently from Plasma Noradrenaline Levels. PLoS ONE 2015, 10, e0134561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarczok, M.N.; Koenig, J.; Schuster, A.K.; Thayer, J.F.; Fischer, J.E. Nighttime heart rate variability, overnight urinary norepinephrine, and glycemic status in apparently healthy human adults. Int. J. Cardiol. 2013, 168, 3025–3026. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Fukuma, N.; Kimura-Kato, Y.; Aisu, N.; Tuchida, T.; Mabuchi, K.; Takano, T. Improvement of sympathetic response to exercise by oral administration of ascorbic acid in patients after myocardial infarction. Int. J. Cardiol. 2006, 111, 240–246. [Google Scholar] [CrossRef]
- Versteylen, M.O.; Joosen, I.A.; Shaw, L.J.; Narula, J.; Hofstra, L. Comparison of Framingham, PROCAM, SCORE, and Diamond Forrester to predict coronary atherosclerosis and cardiovascular events. J. Nucl. Cardiol. 2011, 18, 904–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griendling, K.K.; Touyz, R.M.; Zweier, J.J.; Dikalov, S.; Chilian, W.; Chen, Y.R.; Harrison, D.G.; Bhatnagar, A. American Heart Association Council on Basic Cardiovascular Sciences: American Heart Association Council on Basic Cardiovascular Sciences, Measurement of Reactive Oxygen Species, Reactive Nitrogen Species, and Redox-Dependent Signaling in the Cardiovascular System: A Scientific Statement From the American Heart Association. Circ. Res. 2016, 119, e39–e75. [Google Scholar] [CrossRef]
- Koenig, W.; Karakas, M.; Zierer, A.; Herder, C.; Baumert, J.; Meisinger, C.; Thorand, B. Oxidized LDL and the risk of coronary heart disease: Results from the MONICA/KORA Augsburg Study. Clin. Chem. 2011, 57, 1196–1200. [Google Scholar] [CrossRef] [Green Version]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waller, C.; Rhee, D.-S.; Gröger, M.; Rappel, M.; Maier, T.; Müller, M.; Rottler, E.; Nerz, K.; Nerz, C.; Brill, S.; et al. Social Stress-Induced Oxidative DNA Damage Is Related to Prospective Cardiovascular Risk. J. Clin. Med. 2020, 9, 3783. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113783
Waller C, Rhee D-S, Gröger M, Rappel M, Maier T, Müller M, Rottler E, Nerz K, Nerz C, Brill S, et al. Social Stress-Induced Oxidative DNA Damage Is Related to Prospective Cardiovascular Risk. Journal of Clinical Medicine. 2020; 9(11):3783. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113783
Chicago/Turabian StyleWaller, Christiane, Dae-Sup Rhee, Michael Gröger, Manuela Rappel, Tanja Maier, Markus Müller, Edit Rottler, Katharina Nerz, Christopher Nerz, Sebastian Brill, and et al. 2020. "Social Stress-Induced Oxidative DNA Damage Is Related to Prospective Cardiovascular Risk" Journal of Clinical Medicine 9, no. 11: 3783. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113783