Clinical and Molecular Prediction of Hepatocellular Carcinoma Risk


Liver Tumor Translational Research Program, Simmons Comprehensive Cancer Center, Division of Digestive and Liver Diseases, Department of Internal Medicine, University of Texas Southwestern Medical Center, 5323 Harry Hines Blvd, Dallas, TX 75390, USA
*
Authors to whom correspondence should be addressed.
J. Clin. Med. 2020, 9(12), 3843; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123843
Submission received: 1 November 2020
/
Revised: 20 November 2020
/
Accepted: 23 November 2020
/
Published: 26 November 2020
(This article belongs to the Special Issue Viral Hepatitis and Risk of Hepatocellular Carcinoma)
Abstract
:Prediction of hepatocellular carcinoma (HCC) risk becomes increasingly important with recently emerging HCC-predisposing conditions, namely non-alcoholic fatty liver disease and cured hepatitis C virus infection. These etiologies are accompanied with a relatively low HCC incidence rate (~1% per year or less), while affecting a large patient population. Hepatitis B virus infection remains a major HCC risk factor, but a majority of the patients are now on antiviral therapy, which substantially lowers, but does not eliminate, HCC risk. Thus, it is critically important to identify a small subset of patients who have elevated likelihood of developing HCC, to optimize the allocation of limited HCC screening resources to those who need it most and enable cost-effective early HCC diagnosis to prolong patient survival. To date, numerous clinical-variable-based HCC risk scores have been developed for specific clinical contexts defined by liver disease etiology, severity, and other factors. In parallel, various molecular features have been reported as potential HCC risk biomarkers, utilizing both tissue and body-fluid specimens. Deep-learning-based risk modeling is an emerging strategy. Although none of them has been widely incorporated in clinical care of liver disease patients yet, some have been undergoing the process of validation and clinical development. In this review, these risk scores and biomarker candidates are overviewed, and strategic issues in their validation and clinical translation are discussed.
1. Introduction
Hepatocellular carcinoma (HCC), the major histological type of liver cancer, is one of the most rapidly increasing causes of cancer-related mortality in the US and the fourth most common cancer death globally [1]. HCC develops in chronically diseased livers with infection of hepatitis viruses (e.g., hepatitis B virus (HBV) and hepatitis C virus (HCV)) and metabolic insults such as alcohol abuse and non-alcoholic fatty liver disease (NAFLD) [2]. These viral and metabolic etiological factors promote progressive liver fibrosis that results in its terminal stage, cirrhosis, which is estimated to affect 1–2% of the global population and be attributed to 1.32 million deaths annually [2,3]. Despite recent development of effective antivirals for HBV and HCV, the risk of HCC cannot be eliminated, especially when advanced liver fibrosis is established [4,5]. There are no therapies to halt disease progression toward HCC in patients with alcohol abuse and NAFLD [2].
Given the substantial risk of HCC and prolonged survival by early HCC detection [6], with curative options available only for tumors diagnosed at an early stage, multiple professional society guidelines recommend regular biannual screening for HCC, using ultrasound with or without serum alpha-fetoprotein (AFP), in all patients with cirrhosis from any etiologies [7,8,9]. However, the recommended screening is not utilized in many cases (utilization rate <25%), and the diagnostic accuracy of ultrasound and AFP is suboptimal [10]; as a consequence, most HCC tumors are diagnosed at late stages, and median survival remains as less than one year [11]. This is in part due to vast size of target population that overwhelms currently available medical resources for the screening. In addition, the guidelines do not account for heterogeneity in HCC risk among the target patient population. This approach leads to over-screening of low-risk patients and under-screening of high-risk patients [11]. Thus, more precise HCC risk prediction in each individual patient will significantly improve the efficacy of the HCC screening by identifying high-risk patients who most need close monitoring for more efficient detection and diagnosis of early stage HCC amenable to curative therapies. Indeed, Markov-model-based simulation analysis showed that individual-risk-based personalized HCC screening (Figure 1) is more cost-effective compared to the current “one-size-fits-all” screening approach, sparing net medical care costs and improving patient survival [12]. HCC risk stratification may inform tailored HCC screening strategy to maximize cost-effectiveness of HCC screening by optimizing intensity of screening tests according to predicted risk [2,13,14]. For example, more frequent HCC screening can be offered to high-risk patients compared to low-risk patients. It may be justifiable to utilize costly but high-performance screening tests such as advanced imaging modalities (e.g., MRI-based examination) and biomarkers (e.g., circulating cell-free methylated DNA and GALAD score) in high-risk patients. Given the limited resources for HCC screening in real-world clinical practice, prioritizing high-risk patients for regular HCC screening will also be a rational approach. This should be a focus of future research in HCC screening and early detection. A modeling-based study showed that this personalized strategy indeed can be a viable approach to enable cost-effective HCC screening [12]. Such individual-risk-based personalized cancer screening has also been sought in other cancer types, including colorectal cancer and breast cancer [15,16]. With the currently recommended HCC screening based on ultrasound in the all-comers setting, alteration of HCC screening frequency did not influence patient outcome in clinical studies [17]. This issue may be carefully revisited based on these experiences when studying new HCC screening modalities with improved performance with consideration about anticipated tumor growth rate. Sparing HCC screening in low-risk patients could substantially mitigate the burden of regularly screening the large patient population at risk. However, such a decision of dropping a subset of patients from regular screening should be carefully made, to minimize risk of late tumor diagnosis, which may incur increased medical-care costs, despite poor prognosis. Furthermore, with the shift of major HCC etiology from communicable viral infection to metabolic disorders accompanied with low HCC incidence rate and disproportionally affecting the communities with low socioeconomic status, outreach effort to the at-risk population will become increasingly important. In this review article, we overview clinical-variable-based HCC risk scores and molecular biomarkers in the literature, some of which are promising candidate tools to enable such risk-based individualized HCC screening.
2. Clinical-Variable-Based HCC Risk Scores
Numerous HCC risk scores have been developed, using clinical variables such as age, sex, laboratory tests, and imaging modalities. We summarized the HCC risk scores and biomarkers that were externally validated in independent patient cohort(s) (Table 1). While some scores were developed for specific HCC etiology, some were trained in regional patients with mixed etiologies; for example, the Toronto HCC risk index (THRI), composed of age, sex, etiology, and platelet count, was externally validated in a cirrhosis cohort [18]. The aMAP (age, male, albumin–bilirubin, and platelets) score, calculated by using age, sex, albumin, total bilirubin, and platelet count, was derived from a cohort of HBV-infected patients and independently validated in nine cohorts with various etiologies [19]. In a large VA patient population, HCC-risk-predictive algorithms were developed according to specific clinical contexts, i.e., HCV infection (pre- and post-antiviral treatment), alcoholic cirrhosis, and NAFLD cirrhosis, and they were implemented in a publicly available web application, HCC risk calculator (hccrisk.com) [20,21,22]. Prognostic performance of the models, measured by concordance index, ranged approximately from 0.60 to 0.80 across various clinical contexts. Among the utilized laboratory tests, AFP is frequently incorporated in several HCC risk scores, especially in the context of therapeutically cured HCV infection (Table 1). This may be because HCV cure diminishes AFP elevation due to non-specific hepatic inflammation caused by active viral replication [23]. Studies have suggested that specific clinical contexts defined by several factors likely affect accuracy of HCC risk prediction. For example, the ever-evolving antiviral therapies for HBV and HCV will substantially alter the baseline HCC risk level depending on the status of viral control [19,24,25]. In addition, as suggested from multiple studies on association of germline genotypes with HCC risk, it is plausible that some of such HCC-risk-associated genotypes are bound to patient race/ethnicity and may guide tailored application of HCC risk prediction by geographic representation of racial/ethnic background. Furthermore, dietary habits and/or food contamination with carcinogens such as aflatoxin could be linked to certain geographic regions, possibly allowing a region-tailored strategy of HCC risk assessment [26]. Proper consideration for these factors and incorporation in the risk-prediction algorithm may improve accuracy of HCC risk prediction and enhance cost-effectiveness of HCC screening tailored by these parameters. While most clinical-variable-based scores were derived based on regression models, a sophisticated machine learning approach has also been utilized. Ioannou et al. identified a recurrent neural network-based clinical score to predict incident HCC within three years in 48,151 HCV-infected patients with cirrhosis and showed the new score outperformed conventional linear-regression-model-based score [27]. Despite the promise of the recently emerging utilization of machine learning and artificial intelligence approach to develop risk-predictive models, several limitations are worth noting. First, methodologies such as multi-layer neural network are prone to overfit data structure of specific training dataset, which may diminish generalizability of the model [28]. In addition, it is possible that the modeling disregard certain patient subgroups depending on the structure of the training set. To mitigate these concerns, it will be increasingly important to ensure transparency of the modeling process and clarification of potential pitfalls [29,30].
Semi-quantitative histological fibrosis stage has been reported to be associated with HCC risk, although sampling variability should be concerned when evaluating the liver biopsy specimen [31]. Quantification of collagen proportionate area in liver biopsy specimen is more quantitative measure of liver fibrosis, which is associated with the risk of hepatocarcinogenesis [32,33,34]. Deep-learning algorithm applied to histological images may have the potential to improve the histopathological morphology-based approach of HCC risk assessment [35,36]. Saillard et al. identified histological features predicting survival after surgical resection, supporting feasibility to extend this approach to predict de novo HCC risk [36]. Liver stiffness measurement (LSM) by ultrasound- or MRI-based elastography has been associated with elevated risk of HCC, especially in the settings of viral hepatitis and cured HCV infection [37,38,39,40]. López et al. recently showed that change in LSM one year after achieving HCV cure, as well as baseline LSM, was independently associated with long-term HCC risk in patients with compensated advanced liver fibrosis [41]. In addition, predictive performance of REACH-B score, a clinical score for HBV-associated HCC risk, can be improved by incorporating LSM into the model [42,43].
3. Molecular HCC Risk Biomarkers
Molecular information has a potential to improve the accuracy of HCC risk prediction, in combination with the clinical HCC risk scores (Table 2). Molecular risk biomarkers can be integrated with clinical variables/scores as composite scores, or serially assessed with clinical risk scores for step-wise enrichment of high-risk patient population. In addition, HCC risk biomarkers may be used as selection markers to identify a subset of patients who will benefit from HCC-preventive intervention. They may also serve as surrogate endpoints in HCC prevention clinical trials when their therapeutic modulation reflects change in future HCC risk.
3.1. Germline DNA Variants
Single nucleotide polymorphism (SNP) is a major type of germline DNA polymorphism with a wide variety of pathogenic implications. Previous genome-wide association studies (GWASs) have revealed several SNPs that are likely associated with genetic susceptibility to HCC [65] (Table 2). Germline SNPs can be easily assessed by using a buccal swab or peripheral blood sample, at any time point, because they do not change throughout life and are increasingly more accessible with decreasing costs over time as a viable tool for potential molecular HCC risk prediction. The association of these SNPs with HCC risk is generally modest (odds ratios (ORs) of ~1.5 or less). However, a combination of multiple SNPs may achieve improved performance in HCC risk estimation [66]. Of note, some SNPs seem to be associated with liver disease etiology, suggesting etiology-dependent mechanisms of hepatocarcinogenesis [67].
Several SNPs are reported to be associated with HCV-related HCC. A SNP of IFNL3 (also known as IL28B, encoding one of the cytokines) is associated with risk of HCC development, especially in patients with or without sustained virologic response (SVR) of HCV infection [68,69,70,71,72]. The SNP was initially identified as a predictor of spontaneous clearance of HCV against interferon-based antiviral therapy, and later was found to be related with IFNL3-IFNL4 haplotype-dependent hepatic inflammation and fibrosis [73,74,75,76,77]. A SNP in MICA gene, an immune-related gene encoding the highly polymorphic major histocompatibility complex class I chain-related protein A, was shown to be related to HCC risk in Japanese HCV-infected patients (adjusted OR, 1.36) [78]. This result was validated in an Asian cohort, whereas opposite results were reported in a Swiss cohort, suggesting that the HCC risk association may be patient-race/ethnicity dependent [79,80,81]. A SNP in DEPDC5 gene, encoding a protein that inhibits the mTORC1 pathway, was identified as associated with HCV-related HCC (adjusted OR, 1.96) in Japanese patients [82]. This SNP was also associated with progression of liver fibrosis in European patients [83]. A SNP in the intron of TLL1 gene, encoding a type of matrix metalloprotease that has relation to the liver development, was associated with HCC risk after SVR by interferon-based antiviral therapy in a Japanese cohort (adjusted hazard ratio (HR), 1.78), whereas this SNP was not associated with HCC risk after SVR by direct-acting antiviral (DAA) in a Caucasian cohort [84,85]. EGF 61*G allele was associated with HCC risk in Eastern and Western patients with HCV or HBV infection (pooled OR, 1.38) [86,87,88].
HCC-risk-associated SNPs have also been explored in HBV-related HCC. A SNP in KIF1B gene, encoding one of the motor proteins, was first reported to be associated with HCC risk in Chinese HBV-infected patients and validated in five independent Chinese cohorts, whereas the reports from Korea, Japan, and Thailand failed to validate the result [89,90,91]. Another GWAS study from China identified SNPs in STAT4 and HLA-DQB1/HLA-DBA2 (adjusted OR, 1.21 and 1.49, respectively), both of which were associated with progression of liver fibrosis [92,93]. Genomic DNA duplication at chromosome 15q13.3 was identified as a high-risk variant (OR, 12.02) by a germline copy number variation-based GWAS of Chinese HBV carriers, though its prevalence is low (2.3% and 0.2% in HCC cases and controls, respectively) [94].
One of the major SNPs associated with metabolic HCC is PNPLA3 I148M valiant, initially identified as a risk variant for presence of NAFLD [95]. The protein encoded by PNPLA3 is located on lipid droplet in hepatocytes and hepatic stellate cells and elicits hydrolase activity on triglycerides and retinyl esters, respectively [96]. The PNPLA3 I148M variant causes impaired triglyceride mobilization and accumulation of lipid droplet by evading ubiquitylation and by comparative gene identification–58 (CGI–58)–dependent inhibition of adipose triglyceride lipase, resulting in hepatic steatosis [97,98,99]. PNPLA3 rs738409 G allele was associated with elevated HCC risk in NAFLD and alcohol-related liver disease patients [67,100]. The PNPLA3 I148M was also associated with a high liver-related mortality in a large population study and liver cancer-related mortality in patients with NAFLD in the US [101,102] Further, this variant may be associated with HCC risk after achieving SVR with DAA, [103,104] presumably reflecting the association between HCV infection and hepatic steatosis [105].
A SNP in TM6SF2, encoding E167K substitution, was originally identified as one of the NAFLD-associated SNPs [106]. Subsequent studies have revealed its association with the risk of alcoholic cirrhosis and alterations of hepatic steatosis in viral hepatitis [107,108]. The protein encoded by TM6SF2, transmembrane 6 super family member 2A, is a regulator of liver lipid metabolism, and knockdown/knockout of Tm6sf2 in mice caused an increase of hepatic triglyceride content [106,109,110]. TM6SF2 E167K was associated with HCC in alcohol-related cirrhosis [111]. Homozygous minor allele of the locus was associated with an increased risk of NAFLD-HCC as well, although the significance was lost after adjusting for clinical confounding factors [112].
MBOAT7-TMC4 variant rs641738 was initially reported as a risk SNP for alcoholic cirrhosis together with TM6SF2 E167K [106]. This variant also showed an association with the development and severity of NAFLD in Caucasian patients (adjusted OR, 1.30) and with NAFLD-related HCC even in patients without advanced liver fibrosis (adjusted OR, 2.10) [113,114]. MBOAT7 deletion was reported to cause fatty liver by activation of SREBP-1c [115]. A SNP in DYSF gene was associated with an elevated risk of NASH-related HCC in Japanese patients [116]. Short telomeres and germline mutations in TERT gene were observed in NAFLD-related Caucasian HCC patients [117]. A splice variant in HSD17B13 was negatively associated with histological NASH severity, progression to cirrhosis, and HCC development [118,119,120].
The combination of multiple SNPs has also been thought to improve the ability to predict the individual HCC risk. Gellert-Kristensen et al. combined three NAFLD-related SNPs in PNPLA3, TM6SF2, and HSD17B13 and showed the association with HCC by comparing with the general population (OR, 29.0 for the highest risk group compared to the lowest risk group), although application in the general population is unlikely [66]. Degasperi et al. evaluated another combination, consisting of SNPs in PNPLA3, MBOAT7, TM6SF2, and GCKR, that was associated with liver fat content in cirrhosis patients after curing HCV with DAA (adjusted HR, 2.30), although the cutoff to define the high-risk group was not independently validated [103].
3.2. Hepatic Transcriptomic Signatures
Transcriptomic changes in diseased liver tissue have been widely studied as a direct and reliable measure of pathogenic molecular dysregulation associated with HCC risk and liver disease progression [158]. Hepatic tissue transcriptome profiling has been widely used as a reliable resource to explore biological dysregulation associated with patient prognosis and clinical phenotypes. Earlier studies analyzed diseased liver tissues obtained at the time of hepatic surgery performed as treatment of liver tumor [14]. These studies demonstrated the proof of concept that hepatic transcriptomic dysregulation is associated with the risk of developing de novo HCC after the surgical therapies [159]. However, the HCC-risk-predictive performance should be re-evaluated in HCC-naïve patients, for the prediction of future HCC risk. In addition, the benefits of performing liver biopsy should be justified over the potential risk of adverse events caused by the procedure, such as bleeding. Thus, surrogate markers of hepatic transcriptome will overcome the limitation and enable clinically applicable HCC risk prediction with enhanced accuracy based on molecular information. Prognostic liver signature (PLS) is a hepatic transcriptome-based signature including 186 genes, initially derived from resected liver tissues adjacent to curatively treated HCC and was predictive of overall survival and late HCC recurrence after the treatment [159]. Subsequent studies showed that the PLS and its reduced version (32-gene signature) can predict de novo incidents of HCC in HCV-related early stage cirrhosis, as well as de novo HCC recurrence after curative HCC resection in patients with all major HCC etiologies, including HBV, HCV, alcohol abuse, or NAFLD (HRs, 2.65-10.94) [133,134,135]. In addition, PLS enabled quantitative HCC risk estimation even in chronic hepatitis C patients after achieving SVR [134,160]. Of note, the PLS was implemented in an FDA-approved clinical diagnostic assay platform [160]. A hepatic injury and regeneration (HIR) signature was derived from HCC-surrounding liver tissues from HBV-related HCC patients and was validated for late HCC recurrence (adjusted HR, 2.2) in Asian patients [136].
Transcriptome signatures associated with specific cell types and histological features have also been proposed. Hepatic stellate cells (HSCs) are the liver-specific mesenchymal cells that reside in the space of Disse and are the major precursor of myofibroblasts that drive liver fibrogenesis and create carcinogenesis-promoting hepatic tissue microenvironments [161]. Two HSC-associated signatures have been reported with validation in human cohorts [133,134]. A gene expression signature of 12 chemokine genes was reported to be associated with ectopic lymphoid structure (ELS), a tertiary lymphoid structure composed of lymphocytes and dendritic cells [162]. The ELS signature was associated with late HCC recurrence in a human cohort (adjusted HR, 3.58), suggesting its association with de novo HCC in chronically inflamed liver [139]. A 172-gene signature, named immune-mediated cancer field (ICF), was associated with deregulated immune response in liver and the risk of HCC development [140].
3.3. Somatic DNA Mutations in Non-Malignant Liver
Somatic DNA mutations are, in general, implicated as oncogenic drivers in a variety of cancer types, including HCC. Recent studies have suggested that more somatic DNA mutations also accumulate in cirrhotic livers, as compared to healthy livers, and possibly affect propensity of carcinogenic; moreover, they could be detected in liver tissues and in circulation [65,163,164,165]. In addition, a recent study suggested that somatic mutations in PKD1, KMT2D, and ARID1A genes in non-malignant cirrhotic liver protect hepatocytes from malignant transformation [157]. It is noteworthy that the same somatic events, such as the dysregulation of the ARID1A gene, can either promote or suppress HCC initiation and progression depending on the stage of hepatocarcinogenesis. In addition, rodent-model-based studies have suggested that hepatocyte polyploidy confers protection from HCC development, which can be therapeutically induced by modulation of a cytokinesis gene/protein, anillin [166]. To be considered as biomarkers for HCC risk prediction, detectability in clinically accessible specimens will be a key issue for this type of molecular information.
3.4. Circulating Biomolecules
AFP has been reported as a biomarker for not only an early HCC detection but a risk stratification. Hughes et al. revealed that a longitudinal change in AFP can more accurately capture future HCC risk [23]. Further, biological-hypothesis-driven studies have identified several circulating protein biomarkers for HCC risk, including serum insulin-like growth factor I (IGF-I), osteopontin (OPN), and interleukin-6 (IL-6) [152,153,167]. In addition, various types of biomolecules released into body fluids have been suggested as HCC-related biomarkers [14]. In a nested case–control study from a prospective EPIC cohort, including 129 cases and 1:1 matched controls (median follow-up, 6.2 years), untargeted liquid chromatography–mass spectrometry (MS)-based metabolomics identified 14 metabolites associated with long-term HCC risk, including nine high-risk (N1-acetylspermidine, isatin, p-hydroxyphenyllactic acid, tyrosine, sphingosine, L,L-cyclo(leucylprolyl), glycochenodeoxycholic acid, glycocholic acid, and 7-methylguanine) and five low-risk (retinol, dehydroepiandrosterone sulfate, glycerophosphocholine, γ-carboxyethyl hydroxychroman, and creatine) metabolites (ORs for high-risk and low-risk metabolites, 2.16–6.78 and 0.27–0.56, respectively, for incremental one standard deviation) [155].
Cell-free (cf) nucleic acids in circulation have been explored as sources to detect pathogenic alterations, such as DNA mutations, epigenetic modification, and aberrant abundance of miRNA in an organ of interest. These altered molecules likely reflect molecular dysregulations in subclinical pre/neoplastic cells before clinical detection of tumor, and therefore such circulating nucleic acid-based biomarkers will serve for early tumor detection and/or short-term HCC risk prediction. For instance, a recent study from four Chinese centers introduced an assay detecting point mutations in TP53, CTNNB1, AXIN1, and TERT promoter, as well as HBV integration in cfDNA for early detection of HBV-related HCC, which was combined with AFP, des-γ-carboxy prothrombin, and relevant clinical variables, to develop the “HCCscreen” algorithm [141]. In a validation cohort of 331 AFP- and ultrasound-negative individuals, the algorithm identified 24 test positive patients, among whom four were diagnosed with HCC within six to eight months (17% positive predictive value) [157].
4. Conclusions and Future Perspectives
Clinical translation and implementation of HCC risk scores and biomarkers should be based on proper evidence of validation of their risk-predictive performance as outlined in guidance/recommendation in general oncology and HCC care, because a retrospective assessment intrinsically contains biases, such as unmeasured confounders and selection biases [13,168,169]. However, for risk-predictive biomarkers, their prospective evaluation has been the major bottleneck due to the long-term period required for clinical follow-up to observe a sufficient number of clinical outcomes of interest for statistically detectable prognostic association [170]. Such long-term prospective clinical follow-up is costly, and the likelihood of successful validation is generally low. To mitigate the challenge, an alternative strategy has been proposed. Prospective-specimen-collected design, retrospective-blinded-evaluation (PRoBE) design, or prospective–retrospective design aims to prospectively collect biospecimens, with an intention to test unspecified biomarkers, which are subsequently utilized in a retrospective manner, leveraging matured clinical follow-up data [13,64]. Before clinical application of the clinical risk scores and biomarkers, their performance should be fully ascertained on two aspects. First, when a score/biomarker relies on certain devices such as imaging modality or biochemical test, their technical validity should be assessed for reproducibility of the measurements across test dates and sites based on certain technical implementation that will be used in an actual clinical setting. Second, the magnitude of risk association should be assessed in independent patient series, with in-depth consideration on patient demographics and characteristics, to evaluate their effects on the performance. In assessing the real-world cost-effectiveness of a risk-predictive approach, it is important to consider patient/physician acceptability and adherence, particularly because it is known that the HCC screening utilization rate is low due to a variety of patient- and practitioner-related reasons [11]. This can be estimated by incorporating the HCC screening utilization rate into the simulation model, as performed in a recent Markov-model-based cost-effectiveness analysis [12]. In addition, such a modeling approach informs the desired performance of risk score or biomarker to enable cost-effective HCC screening. For generic HCC biomarker evaluation, several resources have been developed, including the Hepatocellular Carcinoma Early Detection Strategy (HEDS) study [171] and Texas Hepatocellular Carcinoma Consortium (THCCC) [172]. These prospective cohorts will accelerate the validation of risk-predictive biomarkers and facilitate their clinical translation upon successful validation. These expanding resources following the PRoBE design are expected to provide more reliable measures of effect size in risk estimation, which will inform the design and required sample size in subsequent interventional studies to examine magnitude of clinical benefit from the risk-stratified approach. Such evidence will eventually support the decision of whether or not the tailored strategy can be incorporated into clinical practice. In conclusion, several promising development of HCC risk scores and biomarkers are underway, and they are expected to transform the “one-size-fits-all” strategy and contribute to the substantial improvement of the poor prognosis of HCC patients in the foreseeable future.
Author Contributions
Conceptualization and Writing, N.K., N.F., and Y.H. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Uehara Memorial Foundation (to N.F.) and US NIH (DK099558, CA233794, and CA226052), European Commission (ERC-2014-AdG-671231), and Cancer Prevention and Research Institute of Texas (RR180016) (to Y.H.).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J. Hepatol. 2018, 68, 526–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Tseng, C.-H.; Hsu, Y.-C.; Chen, T.-H.; Ji, F.; Chen, I.-S.; Tsai, Y.-N.; Hai, H.; Thuy, L.T.T.; Hosaka, T.; Sezaki, H.; et al. Hepatocellular carcinoma incidence with tenofovir versus entecavir in chronic hepatitis B: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1039–1052. [Google Scholar] [CrossRef]
- Carrat, F.; Fontaine, H.; Dorival, C.; Simony, M.; Diallo, A.; Hezode, C.; De Ledinghen, V.; Larrey, D.; Haour, G.; Bronowicki, J.-P.; et al. Clinical outcomes in patients with chronic hepatitis C after direct-acting antiviral treatment: A prospective cohort study. Lancet 2019, 393, 1453–1464. [Google Scholar] [CrossRef]
- Zhang, B.-H.; Yang, B.-H.; Tang, Z.-Y. Randomized controlled trial of screening for hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2004, 130, 417–422. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- European Association for The Study of The Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Omata, M.; Cheng, A.-L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.-H.; Chawla, Y.K.; Shiina, S.; et al. Asia—Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [Green Version]
- Tzartzeva, K.; Obi, J.; Rich, N.E.; Parikh, N.D.; Marrero, J.A.; Yopp, A.; Waljee, A.K.; Singal, A.G. Surveillance Imaging and Alpha Fetoprotein for Early Detection of Hepatocellular Carcinoma in Patients with Cirrhosis: A Meta-analysis. Gastroenterology 2018, 154, 1706–1718. [Google Scholar] [CrossRef] [Green Version]
- Wolf, E.; Rich, N.E.; Marrero, J.A.; Parikh, N.D.; Singal, A.G. Utilization of hepatocellular carcinoma surveillance in patients with cirrhosis: A systematic review and meta-analysis. Hepatology 2020. [Google Scholar] [CrossRef] [PubMed]
- Goossens, N.; Singal, A.G.; King, L.Y.; Andersson, K.L.; Fuchs, B.C.; Besa, C.; Taouli, B.; Chung, R.T.; Hoshida, Y. Cost-Effectiveness of Risk Score—Stratified Hepatocellular Carcinoma Screening in Patients with Cirrhosis. Clin. Transl. Gastroenterol. 2017, 8, e101. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Liu, P.-H.; Athuluri-Divakar, S.K.; Zhu, S.; Hoshida, Y. Risk Factors of Hepatocellular Carcinoma for Precision Personalized Care. In Molecular and Translational Medicine; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–25. [Google Scholar]
- Fujiwara, N.; Qian, T.; Koneru, B.; Hoshida, Y. Omics-derived hepatocellular carcinoma risk biomarkers for precision care of chronic liver diseases. Hepatol. Res. 2020, 50, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Levin, B.; Lieberman, D.A.; McFarland, B.; Smith, R.A.; Brooks, D.; Andrews, M.K.S.; Dash, C.; Giardiello, F.M.; Glick, S.; Levin, T.R.; et al. Screening and Surveillance for the Early Detection of Colorectal Cancer and Adenomatous Polyps, 2008: A Joint Guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J. Clin. 2008, 58, 130–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tice, J.A.; Cummings, S.R.; Smith-Bindman, R.; Ichikawa, L.; Barlow, W.E.; Kerlikowske, K. Using Clinical Factors and Mammographic Breast Density to Estimate Breast Cancer Risk: Development and Validation of a New Predictive Model. Ann. Intern. Med. 2008, 148, 337–347. [Google Scholar] [CrossRef] [Green Version]
- Nathani, P.; Gopal, P.; Rich, N.; Yopp, A.; Yokoo, T.; John, B.; Marrero, J.; Parikh, N.; Singal, A.G. Hepatocellular carcinoma tumour volume doubling time: A systemic review and meta-analysis. Gut 2020. [Google Scholar] [CrossRef]
- Sharma, S.A.; Kowgier, M.; Hansen, B.E.; Brouwer, W.P.; Maan, R.; Wong, D.; Shah, H.; Khalili, K.; Yim, C.; Heathcote, E.J.; et al. Toronto HCC risk index: A validated scoring system to predict 10-year risk of HCC in patients with cirrhosis. J. Hepatol. 2018, 68, 92–99. [Google Scholar] [CrossRef]
- Fan, R.; Papatheodoridis, G.; Sun, J.; Innes, H.; Toyoda, H.; Xie, Q.; Mo, S.; Sypsa, V.; Guha, I.N.; Kumada, T.; et al. aMAP risk score predicts hepatocellular carcinoma development in patients with chronic hepatitis. J. Hepatol. 2020, 73, 1368–1378. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Green, P.; Kerr, K.F.; Berry, K. Models estimating risk of hepatocellular carcinoma in patients with alcohol or NAFLD-related cirrhosis for risk stratification. J. Hepatol. 2019, 71, 523–533. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Green, P.K.; Beste, L.A.; Mun, E.J.; Kerr, K.F.; Berry, K. Development of models estimating the risk of hepatocellular carcinoma after antiviral treatment for hepatitis C. J. Hepatol. 2018, 69, 1088–1098. [Google Scholar] [CrossRef]
- Poynard, T.; Peta, V.; Deckmyn, O.; Munteanu, M.; Moussalli, J.; Ngo, Y.; Rudler, M.; Lebray, P.; Pais, R.; Bonyhay, L.; et al. LCR1 and LCR2, two multi-analyte blood tests to assess liver cancer risk in patients without or with cirrhosis. Aliment. Pharmacol. Ther. 2019, 49, 308–320. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.M.; Berhane, S.; De Groot, C.E.; Toyoda, H.; Tada, T.; Kumada, T.; Satomura, S.; Nishida, N.; Kudo, M.; Kimura, T.; et al. Serum Levels of α-Fetoprotein Increased More Than 10 Years Before Detection of Hepatocellular Carcinoma. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Ogawa, C.; Kariyama, K.; Morita, M.; Nouso, K.; Toyoda, H.; Tada, T.; Ochi, M.; Murakami, T.; et al. Proposed a simple score for recommendation of scheduled ultrasonography surveillance for hepatocellular carcinoma after Direct Acting Antivirals: Multicenter analysis. J. Gastroenterol. Hepatol. 2018, 34, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Dalekos, G.N.; Sypsa, V.; Yurdaydin, C.; Buti, M.; Goulis, J.; Calleja, J.L.; Chi, H.; Manolakopoulos, S.; Mangia, G.; et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy. J. Hepatol. 2016, 64, 800–806. [Google Scholar] [CrossRef]
- Caines, A.; Selim, R.; Salgia, R. The Changing Global Epidemiology of Hepatocellular Carcinoma. Clin. Liver Dis. 2020, 24, 535–547. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Tang, W.; Beste, L.A.; Tincopa, M.A.; Su, G.L.; Van, T.; Tapper, E.B.; Singal, A.G.; Zhu, J.; Waljee, A.K. Assessment of a Deep Learning Model to Predict Hepatocellular Carcinoma in Patients with Hepatitis C Cirrhosis. JAMA Netw. Open 2020, 3, e2015626. [Google Scholar] [CrossRef]
- Cabitza, F.; Rasoini, R.; Gensini, G.F. Unintended Consequences of Machine Learning in Medicine. JAMA 2017, 318, 517–518. [Google Scholar] [CrossRef]
- Zou, J.; Schiebinger, L. AI can be sexist and racist—it’s time to make it fair. Nature 2018, 559, 324–326. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.; Kendall, F.; Khozin, S.; Goosen, R.; Hu, J.; Laramie, J.; Ringel, M.; Schork, N. Artificial intelligence and machine learning in clinical development: A translational perspective. NPJ Digit. Med. 2019, 2, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Germani, G.; Hytiroglou, P.; Fotiadu, A.; Burroughs, A.K.; Dhillon, A.P. Assessment of Fibrosis and Cirrhosis in Liver Biopsies: An Update. Semin. Liver Dis. 2011, 31, 82–90. [Google Scholar] [CrossRef]
- Tsochatzis, E.; Bruno, S.; Isgro, G.; Hall, A.; Theocharidou, E.; Manousou, P.; Dhillon, A.P.; Burroughs, A.K.; Luong, T.V. Collagen proportionate area is superior to other histological methods for sub-classifying cirrhosis and determining prognosis. J. Hepatol. 2014, 60, 948–954. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; De Boer, W.B.; Adams, L.A.; MacQuillan, G.; Bulsara, M.K.; Jeffrey, G.P. Image analysis of liver biopsy samples measures fibrosis and predicts clinical outcome. J. Hepatol. 2014, 61, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.-H.; Chen, T.-C.; Teng, X.; Liang, K.-H.; Yeh, C.-T. Automated biphasic morphological assessment of hepatitis B-related liver fibrosis using second harmonic generation microscopy. Sci. Rep. 2015, 5, 12962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.-Y.; Wang, X.; Ding, G.-Y.; Dong, Z.; Han, J.; Guan, Z.; Ma, L.-J.; Zheng, Y.; Zhang, L.; Yu, G.-Z.; et al. Exploring prognostic indicators in the pathological images of hepatocellular carcinoma based on deep learning. Gut 2020. [Google Scholar] [CrossRef] [PubMed]
- Saillard, C.; Schmauch, B.; Laifa, O.; Moarii, M.; Toldo, S.; Zaslavskiy, M.; Pronier, E.; Laurent, A.; Amaddeo, G.; Regnault, H.; et al. Predicting survival after hepatocellular carcinoma resection using deep-learning on histological slides. Hepatology 2020. [Google Scholar] [CrossRef]
- Motosugi, U.; Ichikawa, T.; Koshiishi, T.; Sano, K.; Morisaka, H.; Ichikawa, S.; Enomoto, N.; Matsuda, M.; Fujii, H.; Araki, T. Liver stiffness measured by magnetic resonance elastography as a risk factor for hepatocellular carcinoma: A preliminary case—control study. Eur. Radiol. 2012, 23, 156–162. [Google Scholar] [CrossRef]
- Singh, S.; Fujii, L.L.; Murad, M.H.; Wang, Z.; Asrani, S.K.; Ehman, R.L.; Kamath, P.S.; Talwalkar, J.A. Liver stiffness is associated with risk of decompensation, liver cancer, and death in patients with chronic liver diseases: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 11, 1573–1584. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.H.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.-H.; Kim, B.K. Liver stiffness-based model for prediction of hepatocellular carcinoma in chronic hepatitis B virus infection: Comparison with histological fibrosis. Liver Int. 2014, 35, 1054–1062. [Google Scholar] [CrossRef]
- Wang, J.-H.; Yen, Y.-H.; Yao, C.-C.; Hung, C.-H.; Chen, C.-H.; Hu, T.-H.; Lee, C.-M.; Lu, S.-N. Liver stiffness-based score in hepatoma risk assessment for chronic hepatitis C patients after successful antiviral therapy. Liver Int. 2016, 36, 1793–1799. [Google Scholar] [CrossRef]
- López, S.A.; Manzano, M.L.; Gea, F.; Gutiérrez, M.L.; Ahumada, A.M.; Devesa, M.J.; Olveira, A.; Polo, B.A.; Márquez, L.; Fernández, I.; et al. A Model Based on Noninvasive Markers Predicts Very Low Hepatocellular Carcinoma Risk After Viral Response in Hepatitis C Virus—Advanced Fibrosis. Hepatology 2020. [Google Scholar] [CrossRef]
- Yang, H.-I.; Yuen, M.-F.; Chan, H.L.-Y.; Han, K.-H.; Chen, P.-J.; Kim, D.; Ahn, S.-H.; Chen, C.-J.; Wong, V.W.; Seto, W. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): Development and validation of a predictive score. Lancet Oncol. 2011, 12, 568–574. [Google Scholar] [CrossRef]
- Lee, H.W.; Yoo, E.J.; Kim, B.K.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.-H. Prediction of Development of Liver-Related Events by Transient Elastography in Hepatitis B Patients With Complete Virological Response on Antiviral Therapy. Am. J. Gastroenterol. 2014, 109, 1241–1249. [Google Scholar] [CrossRef]
- Singal, A.G.; Mukherjee, A.; Elmunzer, B.J.; Higgins, P.D.R.; Lok, A.S.; Zhu, J.; Marrero, J.A.; Waljee, A.K. Machine Learning Algorithms Outperform Conventional Regression Models in Predicting Development of Hepatocellular Carcinoma. Am. J. Gastroenterol. 2013, 108, 1723–1730. [Google Scholar] [CrossRef] [Green Version]
- Flemming, J.A.; Yang, J.D.; Vittinghoff, E.; Kim, W.R.; Terrault, N.A. Risk prediction of hepatocellular carcinoma in patients with cirrhosis: The ADRESS-HCC risk model. Cancer 2014, 120, 3485–3493. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.-S.; Chan, S.L.; Mo, F.; Chan, T.-C.; Loong, H.H.-F.; Wong, G.L.-H.; Lui, Y.Y.-N.; Chan, A.T.-C.; Sung, J.J.-Y.; Yeo, W.; et al. Clinical Scoring System to Predict Hepatocellular Carcinoma in Chronic Hepatitis B Carriers. J. Clin. Oncol. 2010, 28, 1660–1665. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.S.; Kim, S.U.; Song, K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, B.K.; Han, K.-H. Validation of hepatitis B virus-related hepatocellular carcinoma prediction models in the era of antiviral therapy. Hepatology 2015, 62, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.S.; Jang, B.K.; Um, S.H.; Hwang, J.S.; Han, K.-H.; Kim, S.G.; Lee, K.S.; Kim, S.U.; Kim, Y.S.; Lee, J.I. Validation of risk prediction models for the development of HBV-related HCC: A retrospective multi-center 10-year follow-up cohort study. Oncotarget 2017, 8, 113213–113224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.L.H.; Chan, H.L.-Y.; Wong, C.K.-Y.; Leung, C.; Chan, C.Y.; Ho, P.P.-L.; Chung, V.C.-Y.; Chan, Z.C.-Y.; Tse, Y.-K.; Chim, A.M.-L.; et al. Liver stiffness-based optimization of hepatocellular carcinoma risk score in patients with chronic hepatitis B. J. Hepatol. 2014, 60, 339–345. [Google Scholar] [CrossRef]
- Abu-Amara, M.; Cerocchi, O.; Malhi, G.; Sharma, S.; Yim, C.; Shah, H.; Wong, D.K.; Janssen, H.L.A.; Feld, J.J. The applicability of hepatocellular carcinoma risk prediction scores in a North American patient population with chronic hepatitis B infection. Gut 2015, 65, 1347–1358. [Google Scholar] [CrossRef]
- Roberts, L.; Yang, J.D. Faculty Opinions recommendation of Nomograms for risk of hepatocellular carcinoma in patients with chronic hepatitis B virus infection. Fac. Opin. Post Publ. Peer Rev. Biomed. Lit. 2010, 28, 2437–2444. [Google Scholar] [CrossRef]
- Fusco, M.; Piselli, P.; Virdone, S.; Di Cicco, P.; Scognamiglio, P.; De Paoli, P.; Ciullo, V.; Verdirosi, D.; D’Orazio, M.; Maso, L.D.; et al. Infection with hepatitis viruses, FIB-4 index and risk of hepatocellular carcinoma in southern Italy: A population-based cohort study. Infect. Agents Cancer 2016, 11, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suh, B.; Park, S.; Shin, D.W.; Yun, J.M.; Yang, H.-K.; Yu, S.J.; Shin, C.-I.; Kim, J.-S.; Ahn, E.; Lee, H.; et al. High liver fibrosis index FIB-4 is highly predictive of hepatocellular carcinoma in chronic hepatitis B carriers. Hepatology 2015, 61, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Sinn, D.H.; Lee, J.-H.; Kim, K.; Ahn, J.H.; Lee, J.H.; Kim, J.H.; Lee, D.H.; Yoon, J.-H.; Kang, W.; Gwak, G.-Y.; et al. A Novel Model for Predicting Hepatocellular Carcinoma Development in Patients with Chronic Hepatitis B and Normal Alanine Aminotransferase Levels. Gut Liver 2016, 11, 528–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.W.; Park, S.Y.; Lee, M.; Lee, E.J.; Lee, J.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, B.K. An optimized hepatocellular carcinoma prediction model for chronic hepatitis B with well-controlled viremia. Liver Int. 2020, 40, 1736–1743. [Google Scholar] [CrossRef]
- Yu, J.H.; Suh, Y.J.; Jin, Y.-J.; Heo, N.-Y.; Jang, J.W.; You, C.R.; An, H.Y.; Lee, J.-W. Prediction model for hepatocellular carcinoma risk in treatment-naive chronic hepatitis B patients receiving entecavir/tenofovir. Eur. J. Gastroenterol. Hepatol. 2019, 31, 865–872. [Google Scholar] [CrossRef]
- Chang, J.W.; Lee, J.S.; Lee, H.W.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Seo, Y.S.; Lee, H.A.; Na Kim, M.; et al. Validation of risk prediction scores for hepatocellular carcinoma in patients with chronic hepatitis B treated with entecavir or tenofovir. J. Viral Hepat. 2020. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, Y.D.; Lee, M.; Jun, B.G.; Kim, T.S.; Suk, K.T.; Kang, S.H.; Kim, M.Y.; Cheon, G.J.; Kim, D.J.; et al. Modified PAGE-B score predicts the risk of hepatocellular carcinoma in Asians with chronic hepatitis B on antiviral therapy. J. Hepatol. 2018, 69, 1066–1073. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Yip, T.C.-F.; Ho, H.J.; Wong, V.W.; Huang, Y.-T.; El-Serag, H.B.; Lee, T.-Y.; Wu, M.-S.; Lin, J.-T.; Wong, G.L.; et al. Development of a scoring system to predict hepatocellular carcinoma in Asians on antivirals for chronic hepatitis B. J. Hepatol. 2018, 69, 278–285. [Google Scholar] [CrossRef]
- Marot, A.; Vandenbulcke, H.; Knebel, J.-F.; Doerig, C.; Moreno, C.; Deltenre, P. External validation of the nomogram for individualized prediction of hepatocellular carcinoma occurrence in patients with hepatitis C virus-related compensated cirrhosis. Hepatology 2017, 65, 1419–1421. [Google Scholar] [CrossRef]
- Ganne-Carrié, N.; Layese, R.; Bourcier, V.; Cagnot, C.; Marcellin, P.; Guyader, D.; Pol, S.; Larrey, D.; De Lédinghen, V.; Ouzan, D.; et al. Nomogram for individualized prediction of hepatocellular carcinoma occurrence in hepatitis C virus cirrhosis (ANRS CO12 CirVir). Hepatology 2016, 64, 1136–1147. [Google Scholar] [CrossRef]
- Lee, M.-H.; Lu, S.-N.; Yuan, Y.; Yang, H.-I.; Jen, C.-L.; You, S.-L.; Wang, L.-Y.; L’Italien, G.; Chen, C.-J.; REVEAL-HCV Study Group. Development and Validation of a Clinical Scoring System for Predicting Risk of HCC in Asymptomatic Individuals Seropositive for Anti-HCV Antibodies. PLoS ONE 2014, 9, e94760. [Google Scholar] [CrossRef] [Green Version]
- Sinn, D.H.; Kang, D.; Cho, S.J.; Paik, S.W.; Guallar, E.; Cho, J.; Gwak, G.-Y. Risk of hepatocellular carcinoma in individuals without traditional risk factors: Development and validation of a novel risk score. Int. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Simon, R.; Paik, S.; Hayes, D.F. Use of Archived Specimens in Evaluation of Prognostic and Predictive Biomarkers. J. Natl. Cancer Inst. 2009, 101, 1446–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, M.; Bird, T.G.; Nault, J.-C. The landscape of gene mutations in cirrhosis and hepatocellular carcinoma. J. Hepatol. 2020, 72, 990–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gellert-Kristensen, H.; Richardson, T.G.; Smith, G.D.; Nordestgaard, B.G.; Tybjaerg-Hansen, A.; Stender, S. Combined Effect of PNPLA3, TM6SF2, and HSD17B13 Variants on Risk of Cirrhosis and Hepatocellular Carcinoma in the General Population. Hepatology 2020. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Trépo, E.; Nahon, P.; Cao, Q.; Moreno, C.; Letouzé, E.; Imbaud, S.; Gustot, T.; Devière, J.; Debette, S.; et al. PNPLA3 and TM6SF2 variants as risk factors of hepatocellular carcinoma across various etiologies and severity of underlying liver diseases. Int. J. Cancer 2018, 144, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Simili, A.; Mazzella, G.; Ravaioli, F.; Festi, D.; Bacchi-Reggiani, M.L.; Porro, A.; Bazzoli, F.; Azzaroli, F. Interleukin 28 Polymorphisms and Hepatocellular Carcinoma Development after Direct Acting Antiviral Therapy for Chronic Hepatitis C. J. Gastrointest. Liver Dis. 2019, 28, 449–456. [Google Scholar] [CrossRef]
- Asahina, Y.; Tsuchiya, K.; Nishimura, T.; Muraoka, M.; Suzuki, Y.; Tamaki, N.; Yasui, Y.; Hosokawa, T.; Ueda, K.; Nakanishi, H.; et al. Genetic variation near interleukin 28B and the risk of hepatocellular carcinoma in patients with chronic hepatitis C. J. Gastroenterol. 2014, 49, 1152–1162. [Google Scholar] [CrossRef]
- Chang, K.-C.; Tseng, P.-L.; Wu, Y.-Y.; Hung, H.-C.; Huang, C.-C.; Lu, S.-N.; Wang, J.-H.; Lee, C.-M.; Chen, C.-H.; Tsai, M.-C.; et al. A Polymorphism in Interferon L3 Is an Independent Risk Factor for Development of Hepatocellular Carcinoma After Treatment of Hepatitis C Virus Infection. Clin. Gastroenterol. Hepatol. 2015, 13, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Hodo, Y.; Honda, M.; Tanaka, A.; Nomura, Y.; Arai, K.; Yamashita, T.; Sakai, Y.; Mizukoshi, E.; Sakai, A.; Sasaki, M.; et al. Association of Interleukin-28B Genotype and Hepatocellular Carcinoma Recurrence in Patients with Chronic Hepatitis C. Clin. Cancer Res. 2013, 19, 1827–1837. [Google Scholar] [CrossRef] [Green Version]
- Matsuura, K.; Tanaka, Y. Host genetic variations associated with disease progression in chronic hepatitis C virus infection. Hepatol. Res. 2018, 48, 127–133. [Google Scholar] [CrossRef]
- Thomas, D.L.; Thio, C.L.; Martin, M.P.; Qi, Y.; Ge, D.; O’Huigin, C.; Kidd, J.; Kidd, K.; Khakoo, S.I.; Alexander, G.; et al. Genetic variation in IL28B and spontaneous clearance of hepatitis C virus. Nat. Cell Biol. 2009, 461, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Suppiah, V.; Moldovan, M.; Ahlenstiel, G.; Berg, T.; Weltman, M.; Abate, M.L.; Riordan, S. IL28B is associated with response to chronic hepatitis C interferon-α and ribavirin therapy. Nat. Genet. 2009, 41, 1100–1104. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Nishida, N.; Sugiyama, M.; Kurosaki, M.; Matsuura, K.; Sakamoto, N.; Nakagawa, M.; Korenaga, M.; Hino, K.; Hige, S.; et al. Genome-wide association of IL28B with response to pegylated interferon-α and ribavirin therapy for chronic hepatitis C. Nat. Genet. 2009, 41, 1105–1109. [Google Scholar] [CrossRef] [PubMed]
- Ge, D.; Fellay, J.; Thompson, A.J.; Simon, J.S.; Shianna, K.V.; Urban, T.J.; Heinzen, E.L.; Qiu, P.; Bertelsen, A.H.; Muir, A.J.; et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nat. Cell Biol. 2009, 461, 399–401. [Google Scholar] [CrossRef]
- Eslam, M.; McLeod, D.; Kelaeng, K.S.; Mangia, A.; Berg, T.; Thabet, K.; Irving, W.L.; Dore, G.J.; Sheridan, D.; Grønbæk, H.; et al. IFN-λ3, not IFN-λ4, likely mediates IFNL3-IFNL4 haplotype-dependent hepatic inflammation and fibrosis. Nat. Genet. 2017, 49, 795–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, V.; Kato, N.; Urabe, Y.; Takahashi, A.; Muroyama, R.; Hosono, N.; Otsuka, M.; Tateishi, R.; Omata, M.; Nakagawa, H.; et al. Genome-wide association study identifies a susceptibility locus for HCV-induced hepatocellular carcinoma. Nat. Genet. 2011, 43, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Hai, H.; Tamori, A.; Thuy, L.T.T.; Yoshida, K.; Hagihara, A.; Kawamura, E.; Uchida-Kobayashi, S.; Morikawa, H.; Enomoto, M.; Murakami, Y.; et al. Polymorphisms in MICA, but not in DEPDC5, HCP5 or PNPLA3, are associated with chronic hepatitis C-related hepatocellular carcinoma. Sci. Rep. 2017, 7, 11912. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Huang, C.-Y.; Yeh, M.-L.; Wang, S.-C.; Chen, K.-Y.; Ko, Y.-M.; Lin, C.-C.; Tsai, Y.-S.; Tsai, P.-C.; Lin, Z.-Y.; et al. Genetics Variants and Serum Levels of MHC Class I Chain-related A in Predicting Hepatocellular Carcinoma Development in Chronic Hepatitis C Patients Post Antiviral Treatment. EBioMedicine 2017, 15, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Lange, C.M.; Bibert, S.; Dufour, J.-F.; Cellerai, C.; Cerny, A.; Heim, M.H.; Kaiser, L.; Malinverni, R.; Müllhaupt, B.; Negro, F.; et al. Comparative genetic analyses point to HCP5 as susceptibility locus for HCV-associated hepatocellular carcinoma. J. Hepatol. 2013, 59, 504–509. [Google Scholar] [CrossRef]
- Miki, D.; Ochi, H.; Hayes, C.N.; Abe, H.; Yoshima, T.; Aikata, H.; Ikeda, K.; Kumada, H.; Toyota, J.; Morizono, T.; et al. Variation in the DEPDC5 locus is associated with progression to hepatocellular carcinoma in chronic hepatitis C virus carriers. Nat. Genet. 2011, 43, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Burza, M.A.; Motta, B.M.; Mancina, R.M.; Pingitore, P.; Pirazzi, C.; Lepore, S.M.; Spagnuolo, R.; Doldo, P.; Russo, C.; Lazzaro, V.; et al. DEPDC5 variants increase fibrosis progression in Europeans with chronic hepatitis C virus infection. Hepatology 2015, 63, 418–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuura, K.; Sawai, H.; Ikeo, K.; Ogawa, S.; Iio, E.; Isogawa, M.; Shimada, N.; Komori, A.; Toyoda, H.; Kumada, T.; et al. Genome-Wide Association Study Identifies TLL1 Variant Associated With Development of Hepatocellular Carcinoma After Eradication of Hepatitis C Virus Infection. Gastroenterology 2017, 152, 1383–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Degasperi, E.; Galmozzi, E.; Facchetti, F.; Farina, E.; D’Ambrosio, R.; Soffredini, R.; Iavarone, M.; Lampertico, P. TLL1 variants do not predict hepatocellular carcinoma development in HCV cirrhotic patients treated with direct-acting antivirals. J. Viral Hepat. 2019, 26, 1233–1236. [Google Scholar] [CrossRef]
- Tanabe, K.K.; Lemoine, A.; Finkelstein, D.M.; Kawasaki, H.; Fujii, T.; Chung, R.T.; Lauwers, G.Y.; Kulu, Y.; Muzikansky, A.; Kuruppu, D.; et al. Epidermal Growth Factor Gene Functional Polymorphism and the Risk of Hepatocellular Carcinoma in Patients With Cirrhosis. JAMA 2008, 299, 53–60. [Google Scholar] [CrossRef]
- Abu Dayyeh, B.K.; Yang, M.; Fuchs, B.C.; Karl, D.L.; Yamada, S.; Sninsky, J.J.; O’Brien, T.R.; Dienstag, J.L.; Tanabe, K.K.; Chung, R.T. A Functional Polymorphism in the Epidermal Growth Factor Gene is Associated with Risk for Hepatocellular Carcinoma. Gastroenterology 2011, 141, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Jiang, G.; Yu, K.; Shao, L.; Yu, X.; Hu, C.; Qian, P.; Xie, H.; Li, J.; Zheng, J.; Zheng, S. Association between epidermal growth factor gene +61A/G polymorphism and the risk of hepatocellular carcinoma: A meta-analysis based on 16 studies. BMC Cancer 2015, 15, 314. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Zhai, Y.; Hu, Z.; Wu, C.; Qian, J.; Jia, W.; Ma, F.; Huang, W.; Yu, L.; Yue, W.; et al. Genome-wide association study identifies 1p36.22 as a new susceptibility locus for hepatocellular carcinoma in chronic hepatitis B virus carriers. Nat. Genet. 2010, 42, 755–758. [Google Scholar] [CrossRef]
- Sawai, H.; Nishida, N.; Mbarek, H.; Matsuda, K.; Mawatari, Y.; Yamaoka, M.; Hige, S.; Kang, J.-H.; Abe, K.; Mochida, S.; et al. No association for Chinese HBV-related hepatocellular carcinoma susceptibility SNP in other East Asian populations. BMC Med. Genet. 2012, 13, 47. [Google Scholar] [CrossRef] [Green Version]
- Sopipong, W.; Tangkijvanich, P.; Payungporn, S.; Posuwan, N.; Poovorawan, Y. The KIF1B (rs17401966) Single Nucleotide Polymorphism is not Associated with the Development of HBV-related Hepatocellular Carcinoma in Thai Patients. Asian Pac. J. Cancer Prev. 2013, 14, 2865–2869. [Google Scholar] [CrossRef] [Green Version]
- Jiang, D.-K.; Sun, J.; Cao, G.; Liu, Y.; Lin, D.; Gao, Y.-Z.; Ren, W.-H.; Long, X.-D.; Zhang, H.; Ma, X.-P.; et al. Genetic variants in STAT4 and HLA-DQ genes confer risk of hepatitis B virus—related hepatocellular carcinoma. Nat. Genet. 2013, 45, 72–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, D.-K.; Ma, X.-P.; Wu, X.; Peng, L.; Yin, J.; Dan, Y.; Huang, H.-X.; Ding, D.-L.; Zhang, L.-Y.; Shi, Z.; et al. Genetic variations in STAT4,C2,HLA-DRB1 and HLA-DQ associated with risk of hepatitis B virus-related liver cirrhosis. Sci. Rep. 2015, 5, 16278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, P.; Yang, A.; Wang, R.; Xia, X.; Zhai, Y.; Li, Y.; Yang, F.; Cui, Y.; Xie, W.; Liu, Y.; et al. Germline Duplication of SNORA18L5 Increases Risk for HBV-related Hepatocellular Carcinoma by Altering Localization of Ribosomal Proteins and Decreasing Levels of p53. Gastroenterology 2018, 155, 542–556. [Google Scholar] [CrossRef] [PubMed]
- Romeo, S.; Kozlitina, J.; Xing, C.; Pertsemlidis, A.; Cox, D.; Pennacchio, L.A.; Boerwinkle, E.; Cohen, J.C.; Hobbs, H.H. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat. Genet. 2008, 40, 1461–1465. [Google Scholar] [CrossRef] [Green Version]
- Trépo, E.; Romeo, S.; Zucman-Rossi, J.J.; Nahon, P. PNPLA3 gene in liver diseases. J. Hepatol. 2016, 65, 399–412. [Google Scholar] [CrossRef] [Green Version]
- Basuray, S.; Smagris, E.; Cohen, J.C.; Hobbs, H.H. The PNPLA3 variant associated with fatty liver disease (I148M) accumulates on lipid droplets by evading ubiquitylation. Hepatology 2017, 66, 1111–1124. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Kory, N.; Basuray, S.; Cohen, J.C.; Hobbs, H.H. PNPLA3, CGI-58, and Inhibition of Hepatic Triglyceride Hydrolysis in Mice. Hepatology 2019, 69, 2427–2441. [Google Scholar] [CrossRef] [Green Version]
- Basuray, S.; Wang, Y.; Smagris, E.; Cohen, J.C.; Hobbs, H.H. Accumulation of PNPLA3 on lipid droplets is the basis of associated hepatic steatosis. Proc. Natl. Acad. Sci. USA 2019, 116, 9521–9526. [Google Scholar] [CrossRef] [Green Version]
- Grimaudo, S.; Pipitone, R.M.; Pennisi, G.; Celsa, C.; Cammà, C.; Di Marco, V.; Barcellona, M.R.; Boemi, R.; Enea, M.; Giannetti, A.; et al. Association between PNPLA3 rs738409 C>G Variant and Liver-Related Outcomes in Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 935–944. [Google Scholar] [CrossRef]
- Unalp-Arida, A.; Ruhl, C.E. Patatin-Like Phospholipase Domain-Containing Protein 3 I148M and Liver Fat and Fibrosis Scores Predict Liver Disease Mortality in the U.S. Population. Hepatology 2020, 71, 820–834. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Scribani, M.; Raymond, P.; Harnois, D.M.; Keaveny, A.P.; Ahmed, A.; Kim, D. PNPLA3 Gene Polymorphism and Liver- and Extrahepatic Cancer—Related Mortality in the United States. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Degasperi, E.; Galmozzi, E.; Pelusi, S.; D’Ambrosio, R.; Soffredini, R.; Borghi, M.; Perbellini, R.; Facchetti, F.; Iavarone, M.; SanGiovanni, A.; et al. Hepatic fat—Genetic risk score predicts hepatocellular carcinoma in HCV cirrhotic patients treated with DAAs. Hepatology 2020. [Google Scholar] [CrossRef] [PubMed]
- Miki, D.; Akita, T.; Kurisu, A.; Kawaoka, T.; Nakajima, T.; Hige, S.; Karino, Y.; Toyoda, H.; Kumada, T.; Tsuge, M.; et al. PNPLA3 and HLA-DQB1 polymorphisms are associated with hepatocellular carcinoma after hepatitis C virus eradication. J. Gastroenterol. 2020, 55, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, E.; Takayama, K.; Hiramine, S.; Hayashi, T.; Toyoda, K. Association between steatohepatitis biomarkers and hepatocellular carcinoma after hepatitis C elimination. Aliment. Pharmacol. Ther. 2020, 52, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A. Faculty Opinions recommendation of Exome-wide association study identifies a TM6SF2 variant that confers susceptibility to nonalcoholic fatty liver disease. Fac. Opin. Post Publ. Peer Rev. Biomed. Lit. 2015, 46, 352–356. [Google Scholar] [CrossRef]
- Bucher, S.S.; Stickel, F.; Trépo, E.; Way, M.M.; Herrmann, A.; Nischalke, H.D.; Brosch, M.M.; Rosendahl, J.J.; Berg, T.; Ridinger, M.M.; et al. A genome-wide association study confirms PNPLA3 and identifies TM6SF2 and MBOAT7 as risk loci for alcohol-related cirrhosis. Nat. Genet. 2015, 47, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Mangia, A.; Berg, T.; Chan, H.L.Y.; Irving, W.L.; Dore, G.J.; Abate, M.L.; Bugianesi, E.; Adams, L.A.; Najim, M.A.; et al. Diverse impacts of the rs58542926 E167K variant in TM6SF2 on viral and metabolic liver disease phenotypes. Hepatology 2016, 64, 34–46. [Google Scholar] [CrossRef] [Green Version]
- Mahdessian, H.; Taxiarchis, A.; Popov, S.; Silveira, A.; Franco-Cereceda, A.; Hamsten, A.; Eriksson, P.; Hooft, F.V. TM6SF2 is a regulator of liver fat metabolism influencing triglyceride secretion and hepatic lipid droplet content. Proc. Natl. Acad. Sci. USA 2014, 111, 8913–8918. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.; Lu, H.; Guo, Y.; Zhu, T.; Garcia-Barrio, M.T.; Jiang, Z.; Willer, C.J.; Zhang, J.; Chen, Y.E. Hepatic Transmembrane 6 Superfamily Member 2 Regulates Cholesterol Metabolism in Mice. Gastroenterology 2016, 150, 1208–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stickel, F.; Buch, S.; Nischalke, H.D.; Weiss, K.H.; Gotthardt, D.; Fischer, J.; Rosendahl, J.; Marot, A.; Elamly, M.; Casper, M.; et al. Genetic variants in PNPLA3 and TM6SF2 predispose to the development of hepatocellular carcinoma in individuals with alcohol-related cirrhosis. Am. J. Gastroenterol. 2018, 113, 1475–1483. [Google Scholar] [CrossRef]
- Liu, Y.-L.; Reeves, H.L.; Burt, A.D.; Tiniakos, D.G.; McPherson, S.W.; Leathart, J.B.S.; Allison, M.E.D.; Alexander, G.J.; Piguet, A.-C.; Anty, R.; et al. TM6SF2 rs58542926 influences hepatic fibrosis progression in patients with non-alcoholic fatty liver disease. Nat. Commun. 2014, 5, 4309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancina, R.M.; Dongiovanni, P.; Petta, S.; Pingitore, P.; Meroni, M.; Rametta, R.; Borén, J.; Montalcini, T.; Pujia, A.; Wiklund, O.; et al. The MBOAT7-TMC4 Variant rs641738 Increases Risk of Nonalcoholic Fatty Liver Disease in Individuals of European Descent. Gastroenterology 2016, 150, 1219–1230. [Google Scholar] [CrossRef] [Green Version]
- Donati, B.; Dongiovanni, P.; Romeo, S.; Meroni, M.; McCain, M.; Miele, L.; Petta, S.; Maier, S.; Rosso, C.; De Luca, L.; et al. MBOAT7 rs641738 variant and hepatocellular carcinoma in non-cirrhotic individuals. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, M.; Chandrasekaran, P.; Rong, S.; Fu, X.; Mitsche, M. Hepatic Deletion of Mboat7 (Lpiat1) Causes Activation of SREBP-1c and Fatty Liver. J. Lipid Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Shima, T.; Mizuno, M.; Mitsumoto, Y.; Umemura, A.; Kanbara, Y.; Tanaka, S.; Sumida, Y.; Yasui, K.; Takahashi, M.; et al. Risk estimation model for nonalcoholic fatty liver disease in the Japanese using multiple genetic markers. PLoS ONE 2018, 13, e0185490. [Google Scholar] [CrossRef] [PubMed]
- Donati, B.; Pietrelli, A.; Pingitore, P.; Dongiovanni, P.; Caddeo, A.; Walker, L.; Baselli, G.; Pelusi, S.; Rosso, C.; Vanni, E.; et al. Telomerase reverse transcriptase germline mutations and hepatocellular carcinoma in patients with nonalcoholic fatty liver disease. Cancer Med. 2017, 6, 1930–1940. [Google Scholar] [CrossRef]
- Abul-Husn, N.S.; Cheng, X.; Li, A.H.; Xin, Y.; Schurmann, C.; Stevis, P.; Liu, Y.; Kozlitina, J.; Stender, S.; Wood, G.C.; et al. A Protein-TruncatingHSD17B13Variant and Protection from Chronic Liver Disease. N. Engl. J. Med. 2018, 378, 1096–1106. [Google Scholar] [CrossRef]
- Ma, Y.; Belyaeva, O.V.; Brown, P.M.; Fujita, K.; Valles, K.; Karki, S.; De Boer, Y.S.; Koh, C.; Chen, Y.; Du, X.; et al. 17-Beta Hydroxysteroid Dehydrogenase 13 Is a Hepatic Retinol Dehydrogenase Associated With Histological Features of Nonalcoholic Fatty Liver Disease. Hepatology 2019, 69, 1504–1519. [Google Scholar] [CrossRef]
- Gellert-Kristensen, H.; Nordestgaard, B.G.; Tybjaerg-Hansen, A.; Stender, S. High Risk of Fatty Liver Disease Amplifies the Alanine Transaminase—Lowering Effect of a HSD17B13 Variant. Hepatology 2020, 71, 56–66. [Google Scholar] [CrossRef]
- Qin, S.; Wang, J.; Zhou, C.; Xu, Y.; Zhang, Y.; Wang, X.; Wang, S. The influence of interleukin 28B polymorphisms on the risk of hepatocellular carcinoma among patients with HBV or HCV infection: An updated meta-analysis. Medicine 2019, 98, e17275. [Google Scholar] [CrossRef]
- Luo, X.; Wang, Y.; Shen, A.; Deng, H.; Ye, M. Relationship between the rs2596542 polymorphism in the MICA gene promoter and HBV/HCV infection-induced hepatocellular carcinoma: A meta-analysis. BMC Med. Genet. 2019, 20, 142. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Ma, N.; Zhao, D.; Gao, X.; Zhang, X.; Yang, L.; Liu, D.; Dianwu, L. Correlation between the DEPDC5 rs1012068 polymorphism and the risk of HBV-related hepatocellular carcinoma. Clin. Res. Hepatol. Gastroenterol. 2019, 43, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Iio, E.; Matsuura, K.; Shimada, N.; Atsukawa, M.; Itokawa, N.; Abe, H.; Kato, K.; Takaguchi, K.; Senoh, T.; Eguchi, Y.; et al. TLL1 variant associated with development of hepatocellular carcinoma after eradication of hepatitis C virus by interferon-free therapy. J. Gastroenterol. 2018, 54, 339–346. [Google Scholar] [CrossRef]
- Luo, Y.-Y.; Zhang, H.; Huang, A.; Hu, J. Association between KIF1B rs17401966 genetic polymorphism and hepatocellular carcinoma susceptibility: An updated meta-analysis. BMC Med. Genet. 2019, 20, 59. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, K.; Liu, C.; Chen, J. Meta-analysis reveals an association between signal transducer and activator of transcription-4 polymorphism and hepatocellular carcinoma risk. Hepatol. Res. 2017, 47, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Song, C.; Jiang, D.; Jin, T.; Dai, J.; Zhu, L.; An, J.; Liu, Y.; Ma, S.; Qin, N.; et al. Hepatitis B virus genotype, mutations, human leukocyte antigen polymorphisms and their interactions in hepatocellular carcinoma: A multi-centre case-control study. Sci. Rep. 2015, 5, 16489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singal, A.G.; Manjunath, H.; Yopp, A.C.; Beg, M.S.; Marrero, J.A.; Gopal, P.; Waljee, A.K. The Effect of PNPLA3 on Fibrosis Progression and Development of Hepatocellular Carcinoma: A Meta-analysis. Am. J. Gastroenterol. 2014, 109, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Tang, S.; Zhang, J.; Mei, T.-T.; Guo, H.-Q.; Wei, X.-H.; Zhang, W.-Y.; Liu, Y.-L.; Liang, S.; Fan, Z.-P.; Ma, L.-X.; et al. Association of TM6SF2 rs58542926 T/C gene polymorphism with hepatocellular carcinoma: A meta-analysis. BMC Cancer 2019, 19, 1128 . [Google Scholar] [CrossRef]
- De Benedittis, C.; Bellan, M.; Crevola, M.; Boin, E.; Barbaglia, M.N.; Mallela, V.R.; Ravanini, P.; Ceriani, E.; Fangazio, S.; Sainaghi, P.P.; et al. Interplay of PNPLA3 and HSD17B13 Variants in Modulating the Risk of Hepatocellular Carcinoma among Hepatitis C Patients. Gastroenterol. Res. Pract. 2020, 2020, 4216451. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Trépo, E.; Nahon, P.; Cao, Q.; Moreno, C.; Letouzé, E.; Imbeaud, S.; Bayard, Q.; Gustot, T.; Deviere, J.; et al. A 17-Beta-Hydroxysteroid Dehydrogenase 13 Variant Protects from Hepatocellular Carcinoma Development in Alcoholic Liver Disease. Hepatology 2019, 70, 231–240. [Google Scholar] [CrossRef]
- Stickel, F.; Lutz, P.; Buch, S.; Nischalke, H.D.; Silva, I.; Rausch, V.; Fischer, J.; Weiss, K.H.; Gotthardt, D.; Rosendahl, J.; et al. Genetic Variation in HSD17B13 Reduces the Risk of Developing Cirrhosis and Hepatocellular Carcinoma in Alcohol Misusers. Hepatology 2020, 72, 88–102. [Google Scholar] [CrossRef] [PubMed]
- King, L.Y.; Canasto-Chibuque, C.; Johnson, K.B.; Yip, S.; Chen, X.; Kojima, K.; Deshmukh, M.; Venkatesh, A.; Tan, P.S.; Sun, X.; et al. A genomic and clinical prognostic index for hepatitis C-related early-stage cirrhosis that predicts clinical deterioration. Gut 2015, 64, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Wei, L.; Song, W.M.; Higashi, T.; Ghoshal, S.; Kim, R.S.; Bian, C.B.; Yamada, S.; Sun, X.; Venkatesh, A.; et al. Molecular Liver Cancer Prevention in Cirrhosis by Organ Transcriptome Analysis and Lysophosphatidic Acid Pathway Inhibition. Cancer Cell 2016, 30, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Hoshida, Y.; Villanueva, A.; SanGiovanni, A.; Sole, M.; Hur, C.; Andersson, K.L.; Chung, R.T.; Gould, J.; Kojima, K.; Gupta, S.; et al. Prognostic Gene Expression Signature for Patients With Hepatitis C—Related Early-Stage Cirrhosis. Gastroenterology 2013, 144, 1024–1030. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Sohn, B.H.; Lee, H.-S.; Kim, S.-B.; Yoo, J.E.; Park, Y.-Y.; Jeong, W.; Lee, S.S.; Park, E.S.; Kaseb, A.; et al. Genomic Predictors for Recurrence Patterns of Hepatocellular Carcinoma: Model Derivation and Validation. PLoS Med. 2014, 11, e1001770. [Google Scholar] [CrossRef]
- Ji, J.; Eggert, T.; Budhu, A.; Forgues, M.; Takai, A.; Dang, H.; Ye, Q.; Lee, J.-S.; Kim, J.H.; Greten, T.F.; et al. Hepatic stellate cell and monocyte interaction contributes to poor prognosis in hepatocellular carcinoma. Hepatology 2015, 62, 481–495. [Google Scholar] [CrossRef] [Green Version]
- Henderson, N.; Dy, Z.; Goossens, N.; Guo, J.; Tsai, M.-C.; Chou, H.-I.; Altunkaynak, C.; Sangiovanni, A.; Iavarone, M.; Colombo, M.; et al. Faculty Opinions recommendation of A hepatic stellate cell gene expression signature associated with outcomes in hepatitis C cirrhosis and hepatocellular carcinoma after curative resection. Fac. Opin. Post Publ. Peer Rev. Biomed. Lit. 2016, 65, 1754–1764. [Google Scholar] [CrossRef]
- Finkin, S.; Yuan, D.; Stein, I.; Taniguchi, K.; Weber, A.; Unger, K.; Browning, J.L.; Goossens, N.; Nakagawa, S.; Gunasekaran, G.; et al. Ectopic lymphoid structures function as microniches for tumor progenitor cells in hepatocellular carcinoma. Nat. Immunol. 2015, 16, 1235–1244. [Google Scholar] [CrossRef]
- Moeini, A.; Torrecilla, S.; Tovar, V.; Montironi, C.; Andreu-Oller, C.; Peix, J.; Higuera, M.; Pfister, D.; Ramadori, P.; Pinyol, R.; et al. An Immune Gene Expression Signature Associated with Development of Human Hepatocellular Carcinoma Identifies Mice That Respond to Chemopreventive Agents. Gastroenterology 2019, 157, 1383–1397. [Google Scholar] [CrossRef] [Green Version]
- Qu, C.; Wang, Y.; Wang, P.; Chen, K.; Wang, M.; Zeng, H.; Lu, J.; Song, Q.; Diplas, B.H.; Tan, D.; et al. Detection of early-stage hepatocellular carcinoma in asymptomatic HBsAg-seropositive individuals by liquid biopsy. Proc. Natl. Acad. Sci. USA 2019, 116, 6308–6312. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Hann, H.-W.; Ye, Z.; Hann, R.S.; Wan, S.; Ye, X.; Block, P.D.; Li, B.; Myers, R.; Wang, X.; et al. Prospective evidence of a circulating microRNA signature as a non-invasive marker of hepatocellular carcinoma in HBV patients. Oncotarget 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.-H.; Liang, K.-H.; Chien, R.-N.; Hu, T.-H.; Lin, K.-H.; Hsu, C.-W.; Lin, C.-L.; Pan, T.-L.; Ke, P.-Y.; Yeh, C.-T. A Circulating MicroRNA Signature Capable of Assessing the Risk of Hepatocellular Carcinoma in Cirrhotic Patients. Sci. Rep. 2017, 7, 523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.-C.; Yang, H.-I.; Wang, Q.; Chen, C.-J.; Santella, R.M. Plasma DNA methylation marker and hepatocellular carcinoma risk prediction model for the general population. Carcinogenesis 2017, 38, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhelst, X.; Vanderschaeghe, D.; Castéra, L.; Raes, T.; Geerts, A.; Francoz, C.; Colman, R.; Durand, F.; Callewaert, N.; Van Vlierberghe, H. A Glycomics-Based Test Predicts the Development of Hepatocellular Carcinoma in Cirrhosis. Clin. Cancer Res. 2017, 23, 2750–2758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinkai, N.; Nojima, M.; Iio, E.; Matsunami, K.; Toyoda, H.; Murakami, S.; Inoue, T.; Ogawa, S.; Kumada, T.; Tanaka, Y. High levels of serum Mac-2-binding protein glycosylation isomer (M2BPGi) predict the development of hepatocellular carcinoma in hepatitis B patients treated with nucleot(s)ide analogues. J. Gastroenterol. 2018, 53, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.-C.; Peng, C.-Y.; Hsu, Y.-C.; Su, T.-H.; Wang, C.-C.; Liu, C.-J.; Yang, H.-C.; Yang, W.-T.; Lin, C.-H.; Yu, M.-L.; et al. Baseline Mac-2 Binding Protein Glycosylation Isomer Level Stratifies Risks of Hepatocellular Carcinoma in Chronic Hepatitis B Patients with Oral Antiviral Therapy. Liver Cancer 2020, 9, 1–14. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Jun, T.; Huang, Y.-T.; Yeh, M.-L.; Lee, C.-L.; Ogawa, S.; Cho, S.-H.; Lin, J.-T.; Yu, M.-L.; Nguyen, M.H.; et al. Serum M2BPGi level and risk of hepatocellular carcinoma after oral anti-viral therapy in patients with chronic hepatitis B. Aliment. Pharmacol. Ther. 2018, 48, 1128–1137. [Google Scholar] [CrossRef]
- Yamasaki, K.; Tateyama, M.; Abiru, S.; Komori, A.; Nagaoka, S.; Saeki, A.; Hashimoto, S.; Sasaki, R.; Bekki, S.; Kugiyama, Y.; et al. Elevated serum levels of Wisteria floribunda agglutinin-positive human Mac-2 binding protein predict the development of hepatocellular carcinoma in hepatitis C patients. Hepatology 2014, 60, 1563–1570. [Google Scholar] [CrossRef] [Green Version]
- Aleksandrova, K.; Boeing, H.; Nöthlings, U.; Jenab, M.; Fedirko, V.; Kaaks, R.; Lukanova-McGregor, A.; Trichopoulou, A.; Trichopoulos, D.; Boffetta, P.; et al. Inflammatory and metabolic biomarkers and risk of liver and biliary tract cancer. Hepatology 2014, 60, 858–871. [Google Scholar] [CrossRef]
- Ohishi, W.; Cologne, J.B.; Fujiwara, S.; Suzuki, G.; Hayashi, T.; Niwa, Y.; Akahoshi, M.; Ueda, K.; Tsuge, M.; Chayama, K. Serum interleukin-6 associated with hepatocellular carcinoma risk: A nested case-control study. Int. J. Cancer 2014, 134, 154–163. [Google Scholar] [CrossRef]
- Nakagawa, H.; Maeda, S.; Yoshida, H.; Tateishi, R.; Masuzaki, R.; Ohki, T.; Hayakawa, Y.; Kinoshita, H.; Yamakado, M.; Kato, N.; et al. Serum IL-6 levels and the risk for hepatocarcinogenesis in chronic hepatitis C patients: An analysis based on gender differences. Int. J. Cancer 2009, 125, 2264–2269. [Google Scholar] [CrossRef] [PubMed]
- Mazziotti, G.; Sorvillo, F.; Morisco, F.; Carbone, A.; Rotondi, M.; Stornaiuolo, G.; Precone, D.F.; Cioffi, M.; Gaeta, G.B.; Caporaso, N.; et al. Serum insulin-like growth factor I evaluation as a useful tool for predicting the risk of developing hepatocellular carcinoma in patients with hepatitis C virus-related cirrhosis: A prospective study. Cancer 2002, 95, 2539–2545. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.-H.; Cheng, M.-L.; Lo, C.-J.; Lin, Y.-H.; Lai, M.-W.; Lin, W.-R.; Yeh, C.-T. Plasma phenylalanine and glutamine concentrations correlate with subsequent hepatocellular carcinoma occurrence in liver cirrhosis patients: An exploratory study. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Stepien, M.; Keski-Rahkonen, P.; Kiss, A.; Robinot, N.; Duarte-Salles, T.; Murphy, N.; Perlemuter, G.; Viallon, V.; Tjønneland, A.; Rostgaard-Hansen, A.L.; et al. Metabolic perturbations prior to hepatocellular carcinoma diagnosis: Findings from a prospective observational cohort study. Int. J. Cancer 2020. [Google Scholar] [CrossRef] [PubMed]
- Luo, P.; Yin, P.; Hua, R.; Tan, Y.; Li, Z.; Qiu, G.; Yin, Z.; Xie, X.; Wang, X.; Chen, W.; et al. A Large-scale, multicenter serum metabolite biomarker identification study for the early detection of hepatocellular carcinoma. Hepatology 2018, 67, 662–675. [Google Scholar] [CrossRef]
- Fujiwara, N.; Liu, P.H.; Athuluri-Divakar, S.K.; Zhu, S.; Hoshida, Y. Risk Factors of Hepatocellular Carcinoma for Precision Personalized Care. In Hepatocellular Carcinoma: Translational Precision Medicine Approaches; Hoshida, Y., Ed.; Humana Press: Totowa, NJ, USA; Springer Nature: Cham, Switzerland, 2019. [Google Scholar]
- Mardinoglu, A.; Boren, J.; Smith, U.; Uhlen, M.; Nielsen, J. Systems biology in hepatology: Approaches and applications. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 365–377. [Google Scholar] [CrossRef]
- Hoshida, Y.; Villanueva, A.; Kobayashi, M.; Peix, J.; Chiang, D.Y.; Camargo, A.; Gupta, S.; Moore, J.; Wrobel, M.J.; Lerner, J.; et al. Gene Expression in Fixed Tissues and Outcome in Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 1995–2004. [Google Scholar] [CrossRef] [Green Version]
- Ono, A.; Goossens, N.; Finn, R.S.; Schmidt, W.N.; Thung, S.N.; Im, G.Y.; Hoshida, Y.; Precision Liver Cancer Prevention Consortium. Persisting risk of hepatocellular carcinoma after hepatitis C virus cure monitored by a liver transcriptome signature. Hepatology 2017, 66, 1344–1346. [Google Scholar] [CrossRef] [Green Version]
- Higashi, T.; Friedman, S.L.; Hoshida, Y. Hepatic stellate cells as key target in liver fibrosis. Adv. Drug Deliv. Rev. 2017, 121, 27–42. [Google Scholar] [CrossRef]
- Coppola, D.; Nebozhyn, M.; Khalil, F.; Dai, H.; Yeatman, T.; Loboda, A.; Mulé, J.J. Unique Ectopic Lymph Node-Like Structures Present in Human Primary Colorectal Carcinoma Are Identified by Immune Gene Array Profiling. Am. J. Pathol. 2011, 179, 37–45. [Google Scholar] [CrossRef]
- Zhu, M.; Lu, T.; Jia, Y.; Luo, X.; Gopal, P.; Li, L.; Odewole, M.; Renteria, V.; Singal, A.G.; Jang, Y.; et al. Somatic Mutations Increase Hepatic Clonal Fitness and Regeneration in Chronic Liver Disease. Cell 2019, 177, 608–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, S.F.; Roberts, N.D.; Wylie, L.A.; Moore, L.; Aitken, S.J.; Davies, S.E.; Sanders, M.A.; Ellis, P.; Alder, C.; Hooks, Y.; et al. Somatic mutations and clonal dynamics in healthy and cirrhotic human liver. Nat. Cell Biol. 2019, 574, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Watt, G.P.; Stevenson, H.L.; Calderone, T.L.; Fisher-Hoch, S.P.; Ye, Y.; Wu, X.; Vierling, J.M.; Beretta, L. Telomerase reverse transcriptase mutations in plasma DNA in patients with hepatocellular carcinoma or cirrhosis: Prevalence and risk factors. Hepatol. Commun. 2018, 2, 718–731. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-H.; Zhang, S.; Zhu, M.; Lu, T.; Chen, K.; Wen, Z.; Wang, S.; Xiao, G.; Luo, D.; Jia, Y.; et al. Mice With Increased Numbers of Polyploid Hepatocytes Maintain Regenerative Capacity But Develop Fewer Hepatocellular Carcinomas Following Chronic Liver Injury. Gastroenterology 2020, 158, 1698–1712. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Salles, T.; Misra, S.; Stepien, M.; Plymoth, A.; Muller, D.C.; Overvad, K.; Olsen, A.; Tjønneland, A.; Baglietto, L.; Severi, G.; et al. Circulating Osteopontin and Prediction of Hepatocellular Carcinoma Development in a Large European Population. Cancer Prev. Res. 2016, 9, 758–765. [Google Scholar] [CrossRef] [Green Version]
- Pepe, M.S.; Feng, Z.; Janes, H.; Bossuyt, P.M.; Potter, J.D. Pivotal Evaluation of the Accuracy of a Biomarker Used for Classification or Prediction: Standards for Study Design. J. Natl. Cancer Inst. 2008, 100, 1432–1438. [Google Scholar] [CrossRef] [Green Version]
- Pepe, M.S.; Etzioni, R.; Feng, Z.; Potter, J.D.; Thompson, M.L.; Thornquist, M.D.; Winget, M.; Yasui, Y. Phases of Biomarker Development for Early Detection of Cancer. J. Natl. Cancer Inst. 2001, 93, 1054–1061. [Google Scholar] [CrossRef] [Green Version]
- Ren, A.H.; Fiala, C.A.; Diamandis, E.; Kulasingam, V. Pitfalls in cancer biomarker discovery and validation with emphasis on circulating tumor DNA. Cancer Epidemiol. Biomark. Prev. 2020, 4, 256–269. [Google Scholar] [CrossRef] [Green Version]
- Borges, K.A.; Dai, J.; Parikh, N.D.; Schwartz, M.; Nguyen, M.H.; Roberts, L.R.; Befeler, A.S.; Srivastava, S.; Rinaudo, J.A.; Feng, Z.; et al. Rationale and design of the Hepatocellular carcinoma Early Detection Strategy study: A multi-center longitudinal initiative of the National Cancer Institute’s Early Detection Research Network. Contemp. Clin. Trials 2019, 76, 49–54. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Kanwal, F.; Feng, Z.; Marrero, J.A.; Khaderi, S.; Singal, A.G. Risk Factors for Cirrhosis in Contemporary Hepatology Practices—Findings from the Texas Hepatocellular Carcinoma Consortium Cohort. Gastroenterology 2020, 159, 376–377. [Google Scholar] [CrossRef]
Figure 1.
Stratified hepatocellular carcinoma (HCC) screening tailored by predicted individual HCC risk.
Figure 1.
Stratified hepatocellular carcinoma (HCC) screening tailored by predicted individual HCC risk.


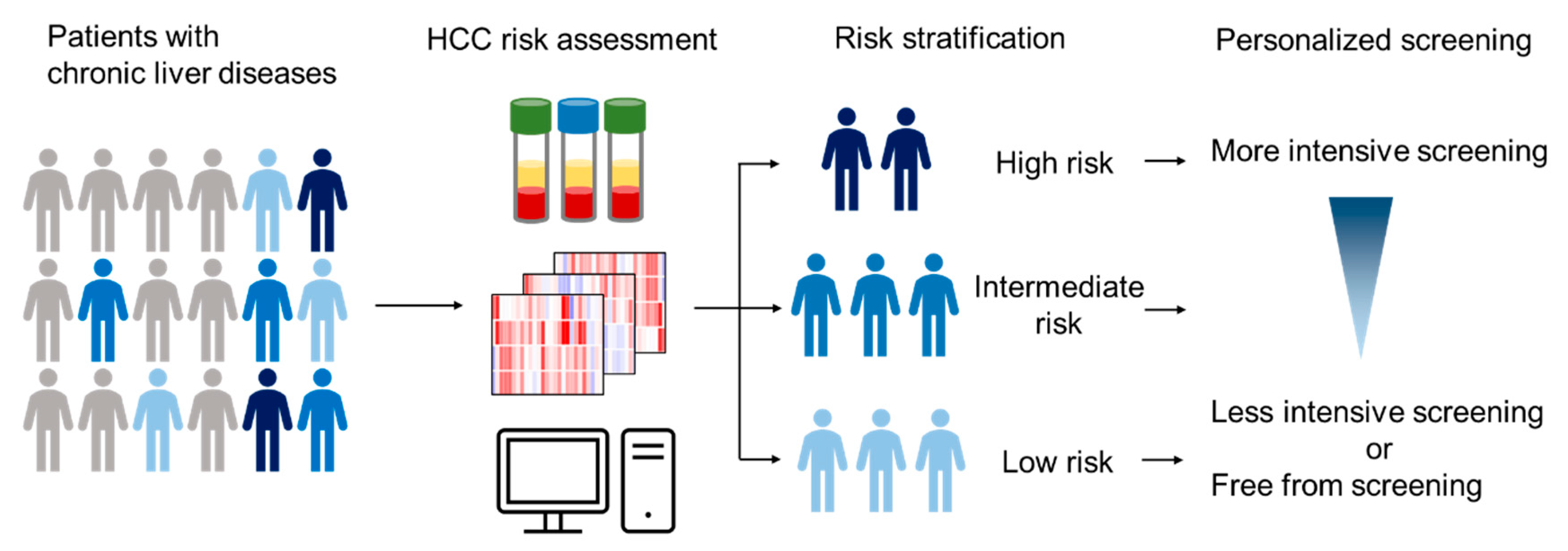{kind=link}
Table 1.
Clinical HCC risk scores.
| Risk Score | Variables | Study Design | Registry * | Endpoint (HCC) | Major Etiology | Region/Country | Race | Cirrhosis ** | Validation ☨ | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| UM regression model | Machine-learning (23 clinical variables) | Cohort | Prospective–retrospective | Development | HCV, cryptogenic, alcohol, other | USA | Caucasian, Black, Hispanic | 100% + 41% | External | [44] |
| aMAP risk score | Age, sex, albumin–bilirubin, platelets | Cohort | Prospective–retrospective | Development | HBV, HCV, HCV after SVR, non-viral | International | Asian, Caucasian | 19.3% + 11.4–100% | External | [19] |
| ADRESS-HCC | Age, diabetes, race, etiology, sex, Child-Pugh score | Cohort | Retrospective | Development | HCV, alcohol, NASH, HBV, other | USA | Non-Hispanic white, Hispanic/Latino, African American, Asian | 100% + 100%, 100% | External | [45] |
| THRI | Age, sex, etiology, platelets | Cohort | Retrospective | Development | Viral, steatohepatitis, PBC, AIH | Canada | n.r. | 100% + 100% | External | [18] |
| Hughes et al. | AFP | Cohort | Prospective–retrospective | Development | HCV, HBV | Japan, Scotland | n.r. | n.r. | External | [23] |
| CU-HCC | Age, albumin, bilirubin, HBV-DNA, cirrhosis | Cohort | Prospective–retrospective | Development | HBV | Hong Kong | n.r. | 38% | External | [46] |
| LSM-HCC | Liver stiffness, age, albumin, HBV-DNA | Cohort | Prospective | Development | HBV | Hong Kong | n.r. | 31% | External ‡ | [47,48,49] |
| REACH-B | Sex, age, ALT, HBeAg, HBV-DNA | Cohort | Prospective–retrospective | Development | HBV | Asia | n.r. | 0% + 18% | External | [42] |
| NGM1-HCC | Sex, age, family history of HCC, alcohol, ALT, HBeAg | Cohort | Prospective–retrospective | Development | HBV | Taiwan | n.r. | n.r. | External ‡ | [50,51] |
| NGM2-HCC | Sex, age, family history of HCC, alcohol, ALT, HBV-DNA | Cohort | Prospective–retrospective | Development | HBV | Taiwan | n.r. | n.r. | External ‡ | [50,51] |
| GAG-HCC | Age, sex, HBV-DNA, core promoter mutations, cirrhosis | Cohort | Retrospective | Development | HBV | Taiwan | n.r. | 15% | External ‡ | [35,40,41] |
| FIB-4 | FIB-4 (AST, ALT, platelets, age) | Cohort | Retrospective | Development | HBV | S. Korea | n.r. | 10% | External ‡ | [52,53] |
| PAGE-B | Age, sex, platelets | Cohort | Retrospective | Development | HBV treated with NA | Europe | Caucasian | 20% + 48% * | External | [25] |
| D2AS risk score | HBV-DNA, sex, age | Cohort | Retrospective | Development | HBV | S. Korea | Asian | 0% | External | [54] |
| CAMPAS model score | Cirrhosis, age, sex, platelets, albumin, liver stiffness | Cohort | Retrospective | Development | HBV treated with NA | S. Korea | Asian | 40% | External | [55] |
| AASL-HCC score | Age, albumin, sex, cirrhosis | Cohort | Retrospective | Development | HBV treated with NA | S. Korea | Asian | 39% + 39% | External | [56] |
| modified PAGE-B | Age, sex, platelets, albumin | Cohort | Retrospective | Development | HBV treated with NA | S. Korea | Asian | 19% + 20% | External ‡ | [57,58] |
| CAMD score | Cirrhosis, age, sex, diabetes mellitus | Cohort | Retrospective | Development | HBV treated with NA | Taiwan, Hong Kong | Asian | 26% + 7% | External | [59] |
| Ganne-Carri et al. | Age, alcohol, platelets, GGT, SVR | Cohort | Prospective–retrospective | Development | HCV | France | n.r. | 100% | External ‡ | [60,61] |
| REVEAL-HCV | Age, ALT, AST/ALT ratio, HCV-RNA, cirrhosis, HCV genotype | Cohort | Prospective–retrospective | Development | HCV | Taiwan | n.r. | 1% + 7% | External | [62] |
| ADRES score | SVR24, sex, FIB-4 index, AFP | Cohort | Retrospective | Development | HCV-SVR treated with DAA | Japan | Asian | n.r. | External | [24] |
| Sinn et al. | Age, sex, smoking, diabetes, total cholesterol, ALT | Cohort | Retrospective | Development | non-HCV, HBV, alcohol | S. Korea | Asian | general population | External | [63] |
* “Prospective–retrospective” indicates a retrospective analysis of prospectively collected cohort in the past [64]. ** Training + validation. ☨ Validation: “Internal”, validation in patients from the same institution(s); “External”, validation in patients from independent institution(s). ‡ Validated by subsequent study. AFP, alpha-fetoprotein; AIH, autoimmune hepatitis; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DAA, direct-acting antiviral agent; GGT, gamma-glutamyltransferase; HbA1c, glycosylated hemoglobin, type A1c; HBV, hepatitis B virus; HBeAg, hepatitis B e antigen; HCV, hepatitis C virus; HCC, hepatocellular carcinoma; NA, nucleoside/nucleotide analogues; NASH, non-alcoholic steatohepatitis; n.r., not reported; PBC, primary biliary cholangitis; SVR, sustained virologic response; UM regression model, University of Michigan regression model; aMAP, age, male, albumin–bilirubin, and platelets risk score; ADRESS-HCC, age, diabetes, race, etiology of cirrhosis, sex, and severity of liver dysfunction HCC; THRI, Toronto hepatocellular carcinoma risk index; CU-HCC, Chinese University-HCC; LSM-HCC, liver stiffness measurement for HCC; REACH-B, risk estimation for hepatocellular carcinoma in chronic hepatitis B; NGM1 or 2-HCC, nomogram 1 or 2-HCC; GAG-HCC, guide with age, gender, HBV-DNA, core promoter mutations and cirrhosis-HCC; FIB-4, fibrosis-4; PAGE-B, platelets, age, gender-HBV; CAMPAS model score, cirrhosis on ultrasonography, age, male gender, platelet count, albumin and liver stiffness; AASL-HCC score, age, albumin, sex, liver cirrhosis HCC score; CAMD score, cirrhosis, age, male sex, and diabetes mellitus score; REVEAL-HCV, risk evaluation of viral load elevation and associated liver disease/cancer in HCV; ADRES score, after DAAs recommendation for surveillance score.
Table 2.
Molecular HCC risk biomarkers.
| Type of Biomarker | Biomarkers/Scores | Variables | Study Design | Assessment *, ** | Endpoint (HCC) | Major Etiology | Region/Country | Race | Cirrhosis ☨,‡ | Combined Clinical Variables | Validation § | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SNP | ||||||||||||
| EGF | EGF 61AG (rs4444903, A>G) | Case–control (Meta-analysis) | Retrospective | Presence | HBV, HCV | France, Italy, China, Egypt, Japan, USA | Asian, European, African | n.r. | n.a. | External | [88] | |
| IFNL3 | IFNL3 (rs12979860: C>T, rs8099917: T>G) | Case–control, cohort (Meta-analysis) | Retrospective | Presence | HCV, HBV | Multiple (Asia, Europe) | n.r. | n.r. | n.a. | External ☨☨ | [68,121] | |
| MICA | MICA (rs2596542, C>T) | Case–control (Meta-analysis) | Retrospective | Presence | HCV, HBV | Egypt, China, Japan, Vietnam, Italy, Switzerland | Asian, European | 14% | n.a. | External | [122] | |
| DEPDC5 | DEPDC5 (rs1012068: T>G) | Case–control | Retrospective | Presence | HCV | Japan | Asian | n.r. | n.a. | No | [123] | |
| TLL1 | TLL1 (rs17047200: A>T) | Case–control | Retrospective | Presence | HCV after SVR treated with IFN | Japan | Asian | 25% + 20% (F3-4) | Age, albumin, AFP after SVR | External ☨☨ | [84,124] | |
| KIF1B or 1p36.22 | KIF1B or 1p36.22 (rs17401966, A>G) | Case–control (Meta-analysis) | Retrospective | Presence | HBV | China, Japan, S. Korea, Thailand | Asian | n.r. | n.a. | External | [125] | |
| STAT4 | STAT4 (rs7574865, G>T) | Case–control (Meta-analysis) | Retrospective | Presence | HBV | Thailand, China, Vietnam, S. Korea | Asian | n.r. | n.a. | External | [126] | |
| HLA-DQB1/HLA-DBA2 | HLA-DQB1/HLA-DBA2 (rs9275319 A>G) | Case–control | Retrospective | Presence | HBV | China | Asian | n.r. | n.a. | External ☨☨ | [92,127] | |
| PNPLA3 | PNPLA3 (rs738409: C>G) | Case–control, cohort (Meta-analysis) | Retrospective | Presence | NAFLD, alcohol, HCV | Europe, Japan | Caucasian | n.r. | n.a. | External | [128] | |
| TM6SF2 | TM6SF2 (rs58542926: C>T) | Case–control (Meta-analysis) | Retrospective | Presence | Alcohol | Italy, Thailand, France, Germany | Caucasian | n.r. | n.a. | External | [129] | |
| MBOAT7 | MBOAT7 (rs641738: C>T) | Case–control | Retrospective | Presence | NAFLD | Italy | Caucasian | 28 % (F3–4) | n.a. | No | [114] | |
| HSD17B13 | HSD17B13 (rs72613567: TA) | Case–control | Retrospective | Presence | Alcohol | Germany | Caucasian | 100% | n.a. | External ☨☨ | [130,131,132] | |
| Score of SNPs | ||||||||||||
| Genetic risk score | SNPs of PNPLA3, TM6SF2, HSD17B13 | Cohort | Prospective-retrospective | Development | General population | Denmark, UK | Caucasian + n.r. | 0.4% + 0.1% | Alcohol cirrhosis, ALT | External | [66] | |
| Fat-genetic risk score (hepatic fat genetic risk score) | SNPs of PNPLA3, TM6SF2, MBOAT7, GCKR, and hepatic fat content | Cohort | Prospective-retrospective | Development, recurrence | HCV treated with DAA | Italy | Italian, Egyptian | 100% | Sex, diabetes, albumin | No | [103] | |
| Tissue transcriptome | ||||||||||||
| Prognostic liver signature (PLS) | 186-gene signature | Cohort | Prospective-retrospective | Development, recurrence | HCV | Training Italy, Validation USA | Asian, Caucasian | 100% | AFP, vascular invasion, bilirubin, platelet, Child–Pugh class, AJCC stage | External ☨☨ | [133,134,135] | |
| HIR gene signature | 233/65-gene signature | Cohort | Retrospective | Late/early recurrence | HBV | S. Korea, Hong Kong, China | Asian | 53% + 63% + 93% | n.a. | External | [136] | |
| Activated HSC gene signature | 37-gene signature | Cohort | Retrospective | Recurrence | HBV | China | Asian | 91% | Child-Pugh staging | External | [137] | |
| HSC signature | 122-gene signature | Cohort | Prospective-retrospective, retrospective | Development | HCV, HBV | USA | Caucasian, Asian | 100% | Bilirubin, platelets | Internal | [138] | |
| Ectopic lymphoid structure signature | 12-gene signature | Cohort | Retrospective | Late recurrence | HCV | Germany | Asian | 52% | n.a. | No | [139] | |
| Immune mediated cancer field signature | 172-gene signature | Cohort | Retrospective | Development | HCV | International | Caucasian | n.r. | Bilirubin | No | [140] | |
| Circulating | ||||||||||||
| cfDNA | mutations of 4 genes, HBV integration | Cohort | Retrospective | Development | HBV | China | Asian | 11% | AFP, US | Internal | [141] | |
| miRNA | 7/8 miRNAs | Cohort | Prospective | Development | HBV | USA | Asian | 35% | AFP | No | [142] | |
| miRNA | 5 miRNAs | Cohort | Prospective-retrospective | Development | HBV, HCV | Taiwan | Asian | 100% | HCV | No | [143] | |
| DNA methylation | TBX2 hypermethylation | Nested case–control | PRoBE | Development | HBV, HCV, alcohol | Taiwan | Asian | n.r. | n.a. | No | [144] | |
| GlycoHCCRiskScore | serum protein N-glycans | Case–control | Prospective-retrospective | Development | HCV | Belgium | Caucasian | 100% | n.a. | No | [145] | |
| Serum glycan | M2BPGi | Cohort | Retrospective | Development | HCV | Japan | Asian | 17% | F4, AFP, age, response to IFN therapy | External ☨☨ | [146,147,148,149] | |
| Cytokine | IL-6 | Cohort | Prospective-retrospective | Development | HCV | Japan | Asian | n.r. | Sex, age, platelets (female), AFP, prothrombin time activity (male), alcohol, BMI (female) | External ☨☨ | [150,151,152] | |
| Protein | IGF-1 | Cohort | Prospective | Development | HCV | Italy | Caucasian | 100% | n.a. | No | [153] | |
| HCC risk score | 2 amino acids (Phe, Gln) | Cohort | Retrospective | Development | HBV, HCV | Taiwan | Asian | n.r. | age, HCV | No | [154] | |
| Metabolites | 14 metabolites | Nested case–control | Prospective-retrospective | Development | HBV, HCV, Alcohol | Europe | n.r. | n.r. | n.a. | No | [155] | |
| Metabolites | 2 metabolites (phenylalanyl-tryptophan, glycocholate) | Nested case–control | PRoBE | Development | HBV | China | Asian | n.r. | AFP | No | [156] |
* “Prospective-retrospective” indicates a retrospective analysis of prospectively collected cohort in the past [64]. ** PRoBE, prospective specimen collection, retrospective blinded evaluation study design [157]. ☨ Case: control. ‡ Training + validation. § Validation: “Internal”, validation in patients from the same institution(s); “External”, validation in patients from independent institution(s). ☨☨ Validated by subsequent study. AFP, alpha-fetoprotein; AJCC, American Joint Committee on Cancer; cfDNA, circulating free DNA; DAA, direct-acting antiviral agent; HBV, hepatitis B virus; HCV, hepatitis C virus; HCC, hepatocellular carcinoma; HIR, hepatic injury and regeneration gene expression; HSC, hepatic stellate cell; IFN, interferon; M2BPGi, mac-2 binding protein glycosylation isomer; miRNA, microRNA; n.a., not applicable; NA, nucleoside/nucleotide analogue; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; n.r., not reported; SNP, single-nucleotide polymorphism; SVR, sustained virologic response; US, ultrasound.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kubota, N.; Fujiwara, N.; Hoshida, Y. Clinical and Molecular Prediction of Hepatocellular Carcinoma Risk. J. Clin. Med. 2020, 9, 3843. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123843
AMA Style
Kubota N, Fujiwara N, Hoshida Y. Clinical and Molecular Prediction of Hepatocellular Carcinoma Risk. Journal of Clinical Medicine. 2020; 9(12):3843. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123843
Chicago/Turabian StyleKubota, Naoto, Naoto Fujiwara, and Yujin Hoshida. 2020. "Clinical and Molecular Prediction of Hepatocellular Carcinoma Risk" Journal of Clinical Medicine 9, no. 12: 3843. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123843
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.