Inflammatory Proteins and Clinical Response to Psychological Therapy in Patients with Depression: An Exploratory Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
Study Objectives
- (1)
- Levels of inflammatory proteins will not differ between depressed patients who do, and do not, respond to psychological treatment, either prior to treatment (predictors of response) or afterwards (cross-sectional associations)
- (2)
- Inflammatory protein levels will not change between pre- and post-treatment measurements;
- (3)
- Participants categorised as having distinct subtypes of depression (i.e., somatic versus cognitive; bipolar versus unipolar) will not differ from other participants in terms of inflammation or the association between inflammation and treatment response.
2. Methods
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Treatment-Outcome Measures
2.3.2. Depression-Subtype Measures
2.3.3. Additional Exploratory Outcome Measures
2.3.4. Inflammatory Measures
2.4. Data Analysis
2.4.1. Data Cleaning
2.4.2. Main Comparisons
- (a)
- Logistic regressions of pre-treatment protein levels (independent variables) as potential predictors of subsequent response to psychological therapy (dependent variable), adjusting for age, gender and BMI (covariates). Using the same approach, post-treatment protein markers were compared between responders and non-responders.
- (b)
- 2 × 2 mixed-factorial ANOVA analyses to assess potential inflammatory changes occurring between pre- and post-treatment assessments (within-subjects) and between responders and non-responders (time by group interaction).
- (c)
- Analysis of inflammatory associations between participants with a predominantly somatic vs. cognitive depression subtype: between-subjects cross-sectional associations through independent-samples t-tests at each timepoint and protein changes over time between these subgroups assessed using a 2 × 2 mixed-factorial ANOVA test.
- (d)
- Compare bipolar and unipolar depressed participants, using the same methods as above.
- (e)
- Determine whether inflammatory changes were associated with concomitant psychotropic medication use, using the methods outlined in comparison (c) to compare somatic and cognitive subtypes of depression.
- (f)
- Assess inflammatory marker associations with treatment resistance (MSM score), using Pearson’s correlations.
- (g)
- Assess inflammatory associations with overall severity, somatic and cognitive symptom severity subscales separately, using the same methods as above.
3. Results
3.1. Sample Characteristics
3.2. Treatment Characteristics
3.3. Inflammatory Marker Characteristics
3.4. Main Comparisons
3.4.1. Inflammatory Predictors of Response
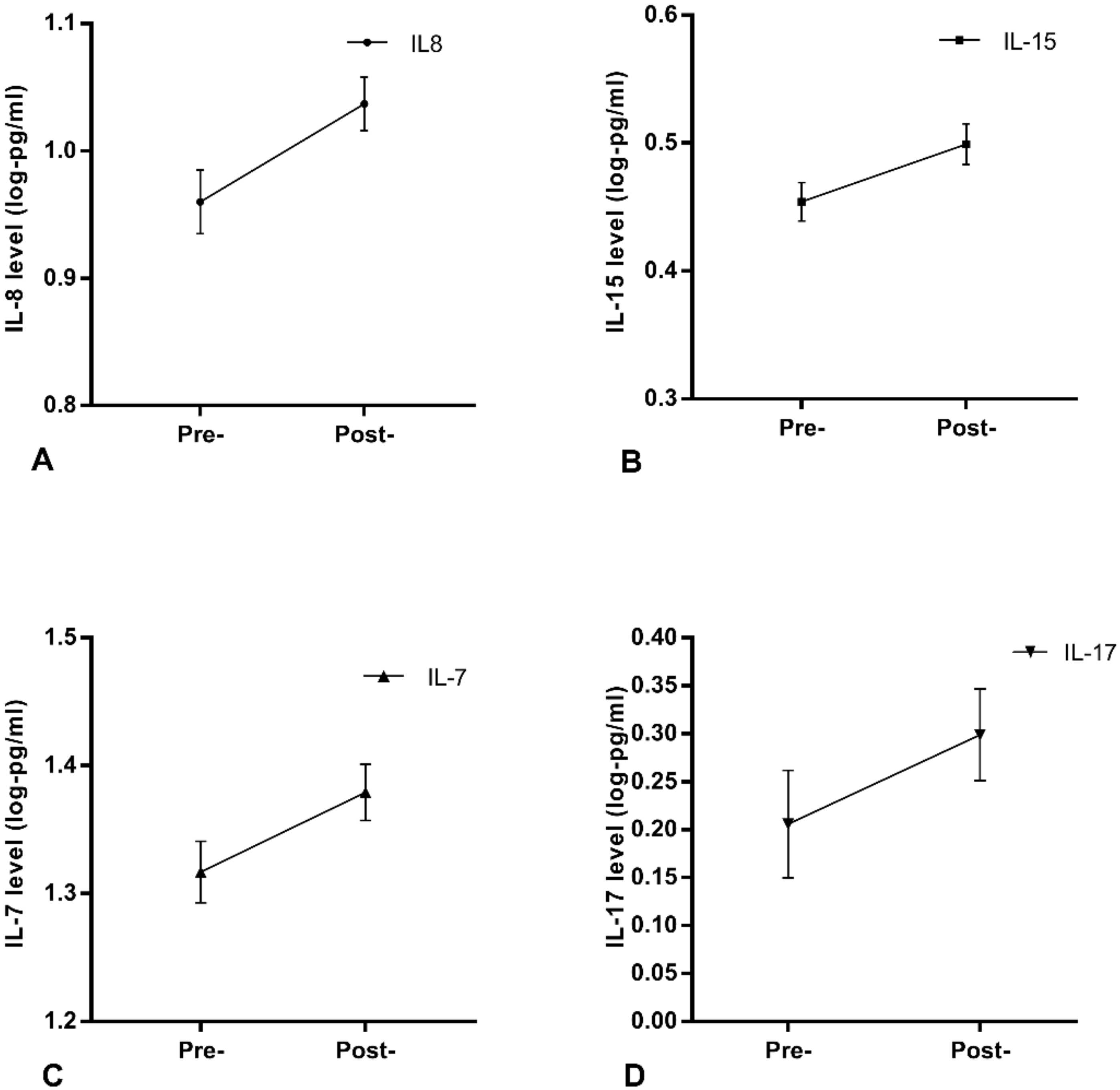
3.4.2. Longitudinal Inflammatory Changes with Treatment
- A: IL-8: Pre-treatment mean = 0.96, SEM = 0.025, Post-treatment mean = 1.037, SEM = 0.021.
- B: IL-15: Pre-treatment mean = 0.454, SEM = 0.015, Post-treatment mean = 0.499, SEM = 0.016.
- C: IL-7: Pre-treatment mean = 1.317, SEM = 0.024, Post-treatment mean = 1.379, SEM = 0.022.
- D: IL-17: Pre-treatment mean = 0.206, SEM = 0.056, Post-treatment mean = 0.299, SEM = 0.048.
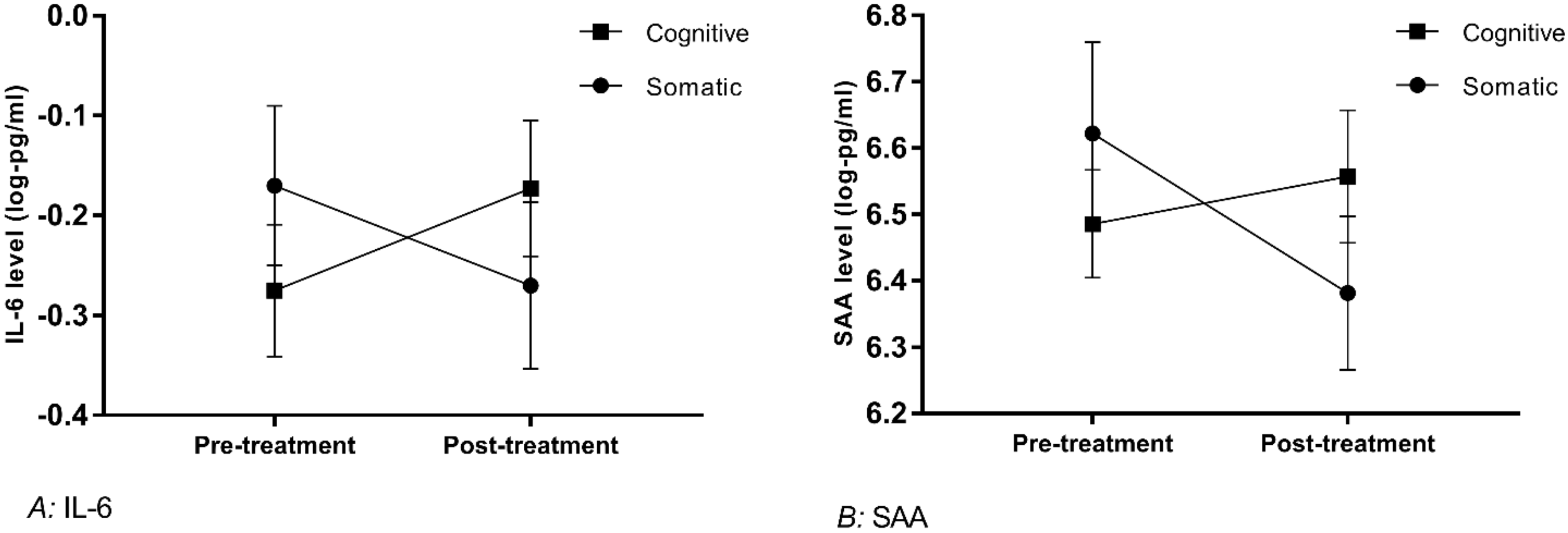
3.4.3. Subgrouping Effects on Inflammatory Associations
- A: IL-6: For clarity of the Figure 2, a value of 1 has been added to protein data in the graph. Log values for participants with a somatic subtype (n = 16): pre-treatment mean = −0.17, SEM = 0.08, post-treatment mean = −0.27, SEM = 0.083. Participants with a cognitive subtype (n = 24): pre-treatment mean = −0.275, SEM = 0.066, post-treatment mean = −0.173, SEM = 0.068.
- B: SAA: Log values for participants with a somatic subtype (n = 16): pre-treatment mean = 6.62, SEM = 0.14, post-treatment mean = 6.38, SEM = 0.12. Participants with a cognitive subtype (n = 24): pre-treatment mean = 6.49, SEM = 0.08, post-treatment mean = 6.56, SEM = 0.10.
3.4.4. Correction for Multiple Comparisons
3.5. Secondary Comparisons
3.5.1. Cross-Sectional Associations between Inflammatory Markers and Depression Severity
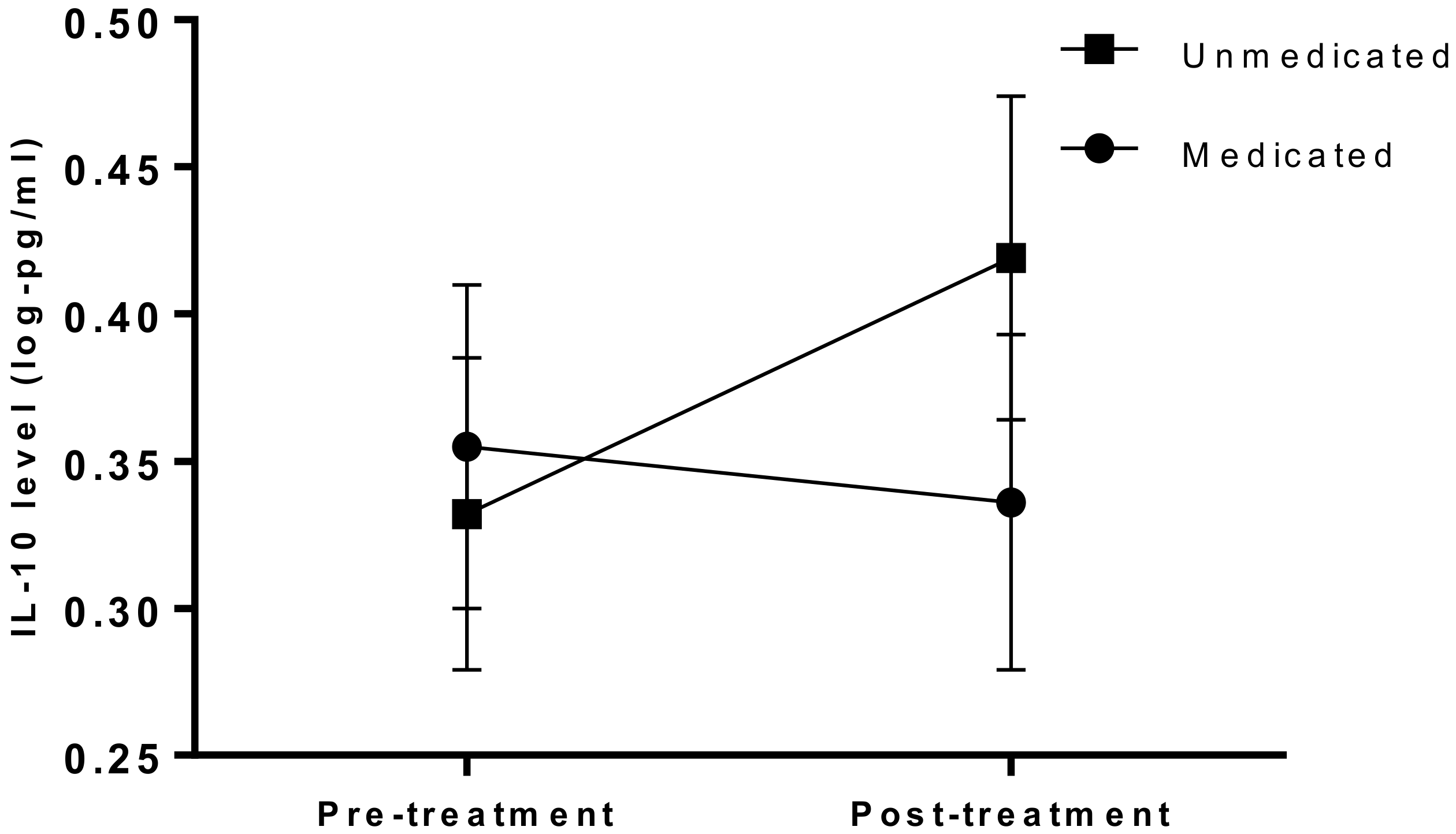
3.5.2. Influences of Concomitant Medication on Inflammation
3.5.3. Associations between Inflammation and Treatment Resistance
4. Discussion
4.1. Inflammatory Relationships with Treatment Response
4.2. Relationships between Inflammation and Depression Severity
4.3. Inflammatory Relationships between Symptom Subtypes
4.4. Inflammatory Relationships between Diagnostic Subtypes
4.5. Longitudinal Changes between Pre- and Post- Therapy Timepoints
4.6. Strengths and Limitations
4.7. Future Recommendations
4.8. Clinical Implications
5. Summary and Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Strawbridge, R.; Young, A.H.; Cleare, A.J. Biomarkers for Depression: Recent Insights, Current Challenges and Future Prospects. Focus 2018, 16, 194–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- I Husain, M.; Strawbridge, R.; Stokes, P.R.; Young, A.H. Anti-inflammatory treatments for mood disorders: Systematic review and meta-analysis. J. Psychopharmacol. 2017, 31, 1137–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, B.D.M.; Daskalakis, Z.J.; Carvalho, A.F.; Strawbridge, R.; Young, A.H.; Mulsant, B.H.; Husain, M.I. Inflammation as a treatment target in mood disorders: Review. BJPsych Open 2020, 6, e60. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.; Bin Wei, Y.; Strawbridge, R.; Bao, Y.-P.; Chang, S.; Shi, L.; Que, J.; Gadad, B.S.; Trivedi, M.H.; Kelsoe, J.R.; et al. Peripheral cytokine levels and response to antidepressant treatment in depression: A systematic review and meta-analysis. Mol. Psychiatry 2019, 25, 339–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, D.G.A.; Caniato, R.N.; Verster, J.C.; Baune, B.T. A psychoneuroimmunological review on cytokines involved in antidepressant treatment response. Hum. Psychopharmacol. Clin. Exp. 2010, 25, 201–215. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, M.S.; Bovbjerg, D.; Renna, M.; Lekander, M.; Mennin, D.; Zachariae, R. Effects of psychological interventions on systemic levels of inflammatory biomarkers in humans: A systematic review and meta-analysis. Brain Behav. Immun. 2018, 74, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Shields, G.S.; Spahr, C.M.; Slavich, G.M. Psychosocial Interventions and Immune System Function: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Psychiatry 2020, 77, 1031–1043. [Google Scholar] [CrossRef]
- Lopresti, A.L. Cognitive behaviour therapy and inflammation: A systematic review of its relationship and the potential implications for the treatment of depression. Aust. N. Z. J. Psychiatry 2017, 51, 565–582. [Google Scholar] [CrossRef]
- Cristea, I.A.; Karyotaki, E.; Hollon, S.D.; Cuijpers, P.; Gentili, C. Biological markers evaluated in randomized trials of psychological treatments for depression: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2019, 101, 32–44. [Google Scholar] [CrossRef]
- Harley, J.; Luty, S.; Carter, J.; Mulder, R.; Joyce, P. Elevated C-reactive protein in depression: A predictor of good long-term outcome with antidepressants and poor outcome with psychotherapy. J. Psychopharmacol. 2009, 24, 625–626. [Google Scholar] [CrossRef]
- Lamers, F.; Milaneschi, Y.; Penninx, B.W.J.H. Chapter 26—Depression Subtypes and Inflammation: Atypical Rather Than Melancholic Depression Is Linked With Immunometabolic Dysregulations. In Inflammation and Immunity in Depression; Baune, B.T., Ed.; Academic Press: Cambridge, MA, USA; pp. 455–471.
- Strawbridge, R.; Young, A.H.; Cleare, A.J. Chapter 27—Inflammation as a Marker of Clinical Response to Treatment: A Focus on Treatment-Resistant Depression. In Inflammation and Immunity in Depression; Baune, B.T., Ed.; Academic Press: Cambridge, MA, USA; pp. 473–487.
- Karlović, D.; Serretti, A.; Vrkić, N.; Martinac, M.; Marčinko, D. Serum concentrations of CRP, IL-6, TNF-α and cortisol in major depressive disorder with melancholic or atypical features. Psychiatry Res. 2012, 198, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.; Ormstad, H.; Aass, H.C.D.; Malt, U.F.; Bendz, L.T.; Sandvik, L.; Brundin, L.; Andreassen, O.A. The plasma levels of various cytokines are increased during ongoing depression and are reduced to normal levels after recovery. Psychoneuroendocrinology 2014, 45, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Capuron, L.; Su, S.; Miller, A.H.; Bremner, J.D.; Goldberg, J.; Vogt, G.J.; Maisano, C.; Jones, L.; Murrah, N.V.; Vaccarino, V. Depressive Symptoms and Metabolic Syndrome: Is Inflammation the Underlying Link? Biol. Psychiatry 2008, 64, 896–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penninx, B.W.; Milaneschi, Y.; Lamers, F.; Vogelzangs, N. Understanding the somatic consequences of depression: Biological mechanisms and the role of depression symptom profile. BMC Med. 2013, 11, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duivis, H.E.; Vogelzangs, N.; Kupper, N.; De Jong, P.J.; Penninx, B.W. Differential association of somatic and cognitive symptoms of depression and anxiety with inflammation: Findings from the Netherlands Study of Depression and Anxiety (NESDA). Psychoneuroendocrinology 2013, 38, 1573–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Eeden, W.A.; Van Hemert, A.M.; Carlier, I.V.E.; Penninx, B.W.J.H.; Lamers, F.; Fried, E.I.; Schoevers, R.; Giltay, E.J. Basal and LPS-stimulated inflammatory markers and the course of individual symptoms of depression. Transl. Psychiatry 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Supasitthumrong, T.; Teixeira, A.L.; Vieira, E.L.; Gattaz, W.F.; Benseñor, I.M.; A Lotufo, P.; Lafer, B.; Berk, M.; Carvalho, A.F.; et al. Differences in the immune-inflammatory profiles of unipolar and bipolar depression. J. Affect. Disord. 2020, 262, 8–15. [Google Scholar] [CrossRef]
- Becking, K.; Spijker, A.T.; Hoencamp, E.; Penninx, B.W.J.H.; Schoevers, R.A.; Boschloo, L. Disturbances in Hypothalamic-Pituitary-Adrenal Axis and Immunological Activity Differentiating between Unipolar and Bipolar Depressive Episodes. PLoS ONE 2015, 10, e0133898. [Google Scholar] [CrossRef]
- Strawbridge, R.; Hodsoll, J.; Powell, T.R.; Hotopf, M.; Hatch, S.L.; Breen, G.; Cleare, A.J. Inflammatory profiles of severe treatment-resistant depression. J. Affect. Disord. 2019, 246, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, N.; Hotopf, M.; Breen, G.; Cleare, A.J.; Grey, N.; Hepgul, N.; King, S.; Moran, P.; Pariante, C.; Wingrove, J.; et al. Predicting outcome following psychological therapy in IAPT (PROMPT): A naturalistic project protocol. BMC Psychiatry 2014, 14, 170. [Google Scholar] [CrossRef] [Green Version]
- Hepgul, N.; King, S.; Amarasinghe, M.; Breen, G.; Grant, N.; Grey, N.; Hotopf, M.; Moran, P.; Pariante, C.M.; Tylee, A.; et al. Clinical characteristics of patients assessed within an Improving Access to Psychological Therapies (IAPT) service: Results from a naturalistic cohort study (Predicting Outcome Following Psychological Therapy; PROMPT). BMC Psychiatry 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 59. [Google Scholar]
- Forty, L.; Kelly, M.; Jones, L.; Jones, I.; Barnes, E.; Caesar, S.; Fraser, C.; Gordon-Smith, K.; Griffiths, E.; Craddock, N.; et al. Reducing the Hypomania Checklist (HCL-32) to a 16-item version. J. Affect. Disord. 2010, 124, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A Manual of Guidelines to Score the Modified Cumulative Illness Rating Scale and Its Validation in Acute Hospitalized Elderly Patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar] [PubMed]
- Fekadu, A.; Wooderson, S.C.; Markopoulou, K. The Maudsley Staging Method for treatment-resistant depression: Prediction of longer-term outcome and persistence of symptoms. J. Clin. Psychiatry 2009, 70, 952–957. [Google Scholar] [CrossRef]
- Croghan, C.W.; Egeghy, P.P. Methods of Dealing with Values Below the Limit of Detection using SAS. South. SAS User Group 2003, 22, 24. [Google Scholar]
- Streiner, D.L.; Norman, G.R. Correction for multiple testing: Is there a resolution? Chest 2011, 140, 16–18. [Google Scholar] [CrossRef]
- Simes, R.J. An improved Bonferroni procedure for multiple tests of significance. Biometrika 1986, 73, 751–754. [Google Scholar] [CrossRef]
- Gyani, A.; Shafran, R.; Layard, R.; Clark, D.M. Enhancing recovery rates: Lessons from year one of IAPT. Behav. Res. Ther. 2013, 51, 597–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennabi, D.; Aouizerate, B.; El-Hage, W.; Doumy, O.; Moliere, F.; Courtet, P.; Nieto, I.; Bellivier, F.; Bubrovsky, M.; Vaiva, G.; et al. Risk factors for treatment resistance in unipolar depression: A systematic review. J. Affect. Disord. 2015, 171, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.W.; Marwood, L.; Greer, B.; Strawbridge, R.; Cleare, A.J. Predictors of response to augmentation treatment in patients with treatment-resistant depression: A systematic review. J. Psychopharmacol. 2019, 33, 1323–1339. [Google Scholar] [CrossRef]
- Yoshimura, R.; Hori, H.; Ikenouchi-Sugita, A.; Umene-Nakano, W.; Ueda, N.; Nakamura, J. Higher plasma interleukin-6 (IL-6) level is associated with SSRI- or SNRI-refractory depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2009, 33, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Lanquillon, S.; Krieg, J.-C.; Bening-Abu-Shach, U.; Vedder, H. Cytokine Production and Treatment Response in Major Depressive Disorder. Neuropsychopharmacology 2000, 22, 370–379. [Google Scholar] [CrossRef]
- Kurokouchi, K.; Kambe, F.; Yasukawa, K.O.U.; Izumi, R.; Ishiguro, N.; Iwata, H.; Seo, H. TNF-alpha increases expression of IL-6 and ICAM-1 genes through activation of NF-kappaB in osteoblast-like ROS17/2.8 cells. J. Bone Miner. Res. 1998, 13, 1290–1299. [Google Scholar] [CrossRef]
- Harjunpää, H.; Asens, M.L.; Guenther, C.; Fagerholm, S.C. Cell Adhesion Molecules and Their Roles and Regulation in the Immune and Tumor Microenvironment. Front. Immunol. 2019, 10, 1078. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, S.M.; Scully, P.; Fitzgerald, P.; Scott, L.V.; Dinan, T.G. Plasma cytokine profiles in depressed patients who fail to respond to selective serotonin reuptake inhibitor therapy. J. Psychiatr. Res. 2007, 41, 326–331. [Google Scholar] [CrossRef]
- Chang, H.H.; Lee, I.H.; Gean, P.W.; Lee, S.-Y.; Chi, M.H.; Yang, Y.K.; Lu, R.-B.; Chen, P.S. Treatment response and cognitive impairment in major depression: Association with C-reactive protein. Brain, Behav. Immun. 2012, 26, 90–95. [Google Scholar] [CrossRef]
- Schleifer, S.J.; Keller, S.E.; Bartlett, J.A. Depression and immunity: Clinical factors and therapeutic course. Psychiatry Res. 1999, 85, 63–69. [Google Scholar] [CrossRef]
- Köhler, C.A.; Freitas, T.H.; Maes, M.; De Andrade, N.Q.; Liu, C.S.; Fernandes, B.S.; Stubbs, B.; Solmi, M.; Veronese, N.; Herrmann, N.; et al. Peripheral cytokine and chemokine alterations in depression: A meta-analysis of 82 studies. Acta Psychiatry Scand. 2017, 135, 373–387. [Google Scholar]
- Angst, J.; Azorin, J.M.; Bowden, C.L.; Perugi, G.; Vieta, E.; Gamma, A.; Young, A.H.; for the BRIDGE Study Group. Prevalence and characteristics of undiagnosed bipolar disorders in patients with a major depressive episode: The BRIDGE study. Arch. Gen. Psychiatry 2011, 68, 791–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelps, J.R.; Ghaemi, S.N. Improving the diagnosis of bipolar disorder: Predictive value of screening tests. J. Affect. Disord. 2006, 92, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Qazi, B.S.; Tang, K.; Qazi, A. Recent Advances in Underlying Pathologies Provide Insight into Interleukin-8 Expression-Mediated Inflammation and Angiogenesis. Int. J. Inflamm. 2011, 2011, 908468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fornaro, M.; Rocchi, G.; Escelsior, A.; Contini, P.; Martino, M. Might different cytokine trends in depressed patients receiving duloxetine indicate differential biological backgrounds. J. Affect. Disord. 2012, 145, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Hernández, M.E.; Mendieta, D.; Martinez-Fong, D.; Loría, F.; Moreno, J.; Estrada, I.; Bojalil, R.; Pavón, L. Variations in circulating cytokine levels during 52 week course of treatment with SSRI for major depressive disorder. Eur. Neuropsychopharmacol. 2008, 18, 917–924. [Google Scholar] [CrossRef]
- A Hiles, S.; Baker, A.L.; De Malmanche, T.; Attia, J. Interleukin-6, C-reactive protein and interleukin-10 after antidepressant treatment in people with depression: A meta-analysis. Psychol. Med. 2012, 42, 2015–2026. [Google Scholar] [CrossRef]
- Kounali, D.Z.; Button, K.S.; Lewis, G.; Ades, A.E. The relative responsiveness of test instruments can be estimated using a meta-analytic approach: An illustration with treatments for depression. J. Clin. Epidemiol. 2016, 77, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, A.; Ferrari, C.; Uher, R.; Bocchio-Chiavetto, L.; Riva, M.A.; Pariante, C.M. Absolute Measurements of Macrophage Migration Inhibitory Factor and Interleukin-1-β mRNA Levels Accurately Predict Treatment Response in Depressed Patients. Int. J. Neuropsychopharmacol. 2016, 19. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, A.; Turner, L.; Mariani, N.; Enache, D.; Hastings, C.; Kose, M.; Lombardo, G.; McLaughlin, A.P.; Ferrari, C.; Lopizzo, N.; et al. Whole-blood expression of inflammasome- and glucocorticoid-related mRNAs correctly separates treatment-resistant depressed patients from drug-free and responsive patients in the BIODEP study. Transl. Psychiatry 2020, 10, 232. [Google Scholar] [CrossRef]
- Cattaneo, A.; Gennarelli, M.; Uher, R.; Breen, G.; Farmer, A.; Aitchison, K.J.; Craig, I.W.; Anacker, C.; Zunsztain, P.A.; McGuffin, P.; et al. Candidate Genes Expression Profile Associated with Antidepressants Response in the GENDEP Study: Differentiating between Baseline ‘Predictors’ and Longitudinal ‘Targets’. Neuropsychopharmacology 2013, 38, 377–385. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Full Sample N = 96 | Responders n = 47 | Non-Responders n = 49 | p-Value * | |
|---|---|---|---|---|
| Gender n female (%) | 68 (72%) | 36 (77%) | 32 (65%) | |
| Age Mean age (range) | 37.7 (18–77) | 35.5 (19–71) | 39.8 (18–77) | |
| BMI Mean BMI (range) | 25.8 (16–47) a | 25.2 (16–47) | 26.1 (18–45) | |
| Symptom subtypen somatic (%) | 26 (33%) b | 12 (31%) | 14 (36%) | |
| Bipolar status n bipolar spectrum (%) | 30 (31%) | 15 (32%) | 15 (31%) | |
| Childhood trauma severity Mean CTQ score (range) | 52.2 (28–114) c | 52 (28–114) | 52.5 (28–102) | |
| Physical illness Mean MCIRS score (range) | 16.4 (13–28) d | 16.3 (13–28) | 16.8 (13–25) | |
| Psychiatric medication n medicated (%) | 45 (47%) | 18 (38%) | 27 (55%) | |
| Treatment-resistance Mean MSM score (range) | 5.82 (3–10) | 5.82 (3.5–9) | 5.82 (3–10) | |
| Pre-treatment depression severity Mean PHQ9 score (range) | 18.4 (10–27) | 17.4 (10–25) | 19.4 (10–27) | 0.022 |
| Post-treatment depression severity Mean PHQ9 score (range) | 10.9 (0–27) | 5 (0–21) | 16.5 (10–27) | <0.001 |
| Number of therapy sessions Mean number (range) | 11.9 (4–35) e | 10.8 (4–32) | 13.2 (4–35) | |
| Number of psychiatric comorbidities Mean number (range) | 3.2 (0–7) | 2.6 (0–7) | 3.6 (0–7) | 0.015 |
| Pre-Treatment Comparison | Post-Treatment Comparison | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Protein | OR | 95% CI Lower Upper | p | adj. p | OR | 95% CI Lower Upper | p | adj. p | ||
| TNFα | 0.007 | −9.686 | −1.006 | 0.016 | 0.138 | 0.064 | −10.210 | 2.810 | 0.310 | 0.466 |
| IL-6 | 0.149 | −3.496 | −0.453 | 0.011 | 0.138 | 0.062 | −7.081 | −0.682 | 0.027 | 0.157 |
| CRP | 0.531 | −1.418 | 0.145 | 0.091 | 0.419 | 0.216 | −3.308 | −0.446 | 0.006 | 0.067 |
| IL-10 | 0.629 | −1.786 | 0.783 | 0.417 | 0.779 | 0.313 | −3.415 | 1.191 | 0.239 | 0.466 |
| IL-8* | 0.393 | −3.430 | 1.681 | 0.440 | 0.779 | 0.038 | −10.259 | 0.846 | 0.148 | 0.369 |
| IL-12 | 0.992 | −1.940 | 1.773 | 0.991 | 0.991 | 1.974 | −3.401 | 3.312 | 0.609 | 0.643 |
| IL-7 | 1.080 | −2.171 | 2.780 | 0.954 | 0.991 | 0.094 | −7.587 | 1.901 | 0.257 | 0.466 |
| IL-15 | 1.896 | −3.022 | 4.221 | 0.728 | 0.887 | 0.016 | −11.896 | 1.615 | 0.150 | 0.369 |
| IL-16 | 0.871 | −2.823 | 2.524 | 0.915 | 0.991 | 0.225 | −6.226 | 3.171 | 0.504 | 0.592 |
| IL-17 | 1.626 | −0.799 | 1.811 | 0.409 | 0.779 | 1.232 | −1.760 | 2.338 | 0.817 | 0.831 |
| MCP1 | 0.611 | −3.312 | 1.886 | 0.733 | 0.887 | 0.072 | −10.644 | 1.082 | 0.285 | 0.466 |
| MCP4 | 0.754 | −2.467 | 1.757 | 0.783 | 0.901 | 0.016 | −10.689 | −0.680 | 0.025 | 0.157 |
| Mip1b | 0.188 | −4.530 | 0.563 | 0.174 | 0.572 | 0.924 | −4.747 | 4.327 | 0.962 | 0.962 |
| Eotaxin | 0.517 | −2.944 | 1.393 | 0.485 | 0.783 | 0.432 | −4.118 | 1.907 | 0.553 | 0.604 |
| sICAM1 | 0.010 | −9.293 | −0.557 | 0.018 | 0.138 | 0.002 | −14.894 | −0.371 | 0.037 | 0.159 |
| sVCAM1 | 0.278 | −6.311 | 3.308 | 0.577 | 0.783 | 0.011 | −15.061 | 2.040 | 0.247 | 0.466 |
| SAA | 0.639 | −1.527 | 0.735 | 0.425 | 0.779 | 0.264 | −4.406 | 0.067 | 0.112 | 0.323 |
| TARC * | 0.453 | −2.512 | 0.733 | 0.304 | 0.779 | 0.030 | −6.469 | −1.723 | 0.003 | 0.067 |
| Tie2 | 0.076 | −6.965 | −0.134 | 0.140 | 0.537 | 0.185 | −8.260 | 1.213 | 0.370 | 0.466 |
| IP-10 | 0.348 | −4.120 | 0.870 | 0.382 | 0.779 | 0.153 | −7.253 | 2.033 | 0.348 | 0.466 |
| IFNγ | 5.205 | 0.102 | 3.755 | 0.042 | 0.242 | 5.743 | −0.338 | 4.334 | 0.079 | 0.271 |
| Eotaxin3 | 0.781 | −1.184 | 0.725 | 0.579 | 0.783 | 0.343 | −4.240 | 0.590 | 0.290 | 0.466 |
| TNFβ * | 0.765 | −1.255 | 0.576 | 0.553 | 0.783 | 0.621 | −2.251 | 1.013 | 0.509 | 0.592 |
| Protein | Before vs. after Treatment | Treatment x Response Interaction | ||||
|---|---|---|---|---|---|---|
| F | p | adj. p | F | p | adj. p | |
| TNFα | 0.023 | 0.880 | 0.950 | 0.015 | 0.902 | 0.909 |
| IL-6 | 0.004 | 0.950 | 0.950 | 0.032 | 0.859 | 0.909 |
| CRP | 0.022 | 0.883 | 0.950 | 0.068 | 0.795 | 0.909 |
| IL-10 | 3.164 | 0.082 | 0.236 | 2.167 | 0.147 | 0.676 |
| IL-8 | 14.600 | 0.0009 | 0.021 | 2.352 | 0.132 | 0.676 |
| IL-12 | 0.842 | 0.363 | 0.816 | 0.542 | 0.465 | 0.901 |
| IL-7 | 7.181 | 0.010 | 0.077 | 0.188 | 0.666 | 0.901 |
| IL-15 | 9.826 | 0.003 | 0.035 | 0.345 | 0.560 | 0.901 |
| IL-16 | 0.328 | 0.511 | 0.840 | 2.301 | 0.136 | 0.676 |
| IL-17 | 5.049 | 0.027 | 0.167 | 3.058 | 0.087 | 0.676 |
| MCP1 | 3.322 | 0.075 | 0.236 | 1.455 | 0.234 | 0.769 |
| MCP4 | 0.110 | 0.742 | 0.948 | 0.074 | 0.787 | 0.909 |
| Mip1b | 0.557 | 0.459 | 0.816 | 0.013 | 0.909 | 0.909 |
| Eotaxin | 0.170 | 0.682 | 0.948 | 0.287 | 0.595 | 0.901 |
| sICAM1 | 0.173 | 0.680 | 0.948 | 0.015 | 0.903 | 0.909 |
| sVCAM1 | 2.850 | 0.098 | 0.250 | 2.628 | 0.112 | 0.676 |
| SAA | 0.688 | 0.411 | 0.816 | 0.349 | 0.558 | 0.901 |
| TARC | 0.553 | 0.461 | 0.816 | 0.333 | 0.567 | 0.901 |
| Tie2 | 0.008 | 0.928 | 0.950 | 0.851 | 0.361 | 0.901 |
| IP-10 | 0.076 | 0.784 | 0.949 | 0.224 | 0.638 | 0.901 |
| IFNγ | 3.440 | 0.070 | 0.236 | 0.301 | 0.586 | 0.901 |
| Eotaxin3 | 0.142 | 0.708 | 0.948 | 0.019 | 0.892 | 0.909 |
| TNFβ | 3.403 | 0.071 | 0.236 | 1.532 | 0.222 | 0.769 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strawbridge, R.; Marwood, L.; King, S.; Young, A.H.; Pariante, C.M.; Colasanti, A.; Cleare, A.J. Inflammatory Proteins and Clinical Response to Psychological Therapy in Patients with Depression: An Exploratory Study. J. Clin. Med. 2020, 9, 3918. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123918
Strawbridge R, Marwood L, King S, Young AH, Pariante CM, Colasanti A, Cleare AJ. Inflammatory Proteins and Clinical Response to Psychological Therapy in Patients with Depression: An Exploratory Study. Journal of Clinical Medicine. 2020; 9(12):3918. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123918
Chicago/Turabian StyleStrawbridge, Rebecca, Lindsey Marwood, Sinead King, Allan H. Young, Carmine M. Pariante, Alessandro Colasanti, and Anthony J. Cleare. 2020. "Inflammatory Proteins and Clinical Response to Psychological Therapy in Patients with Depression: An Exploratory Study" Journal of Clinical Medicine 9, no. 12: 3918. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123918