Nightmares in Patients with Major Depressive Disorder, Bipolar Disorder, and Psychotic Disorders: A Systematic Review

 ,
,
Abstract
:1. Introduction
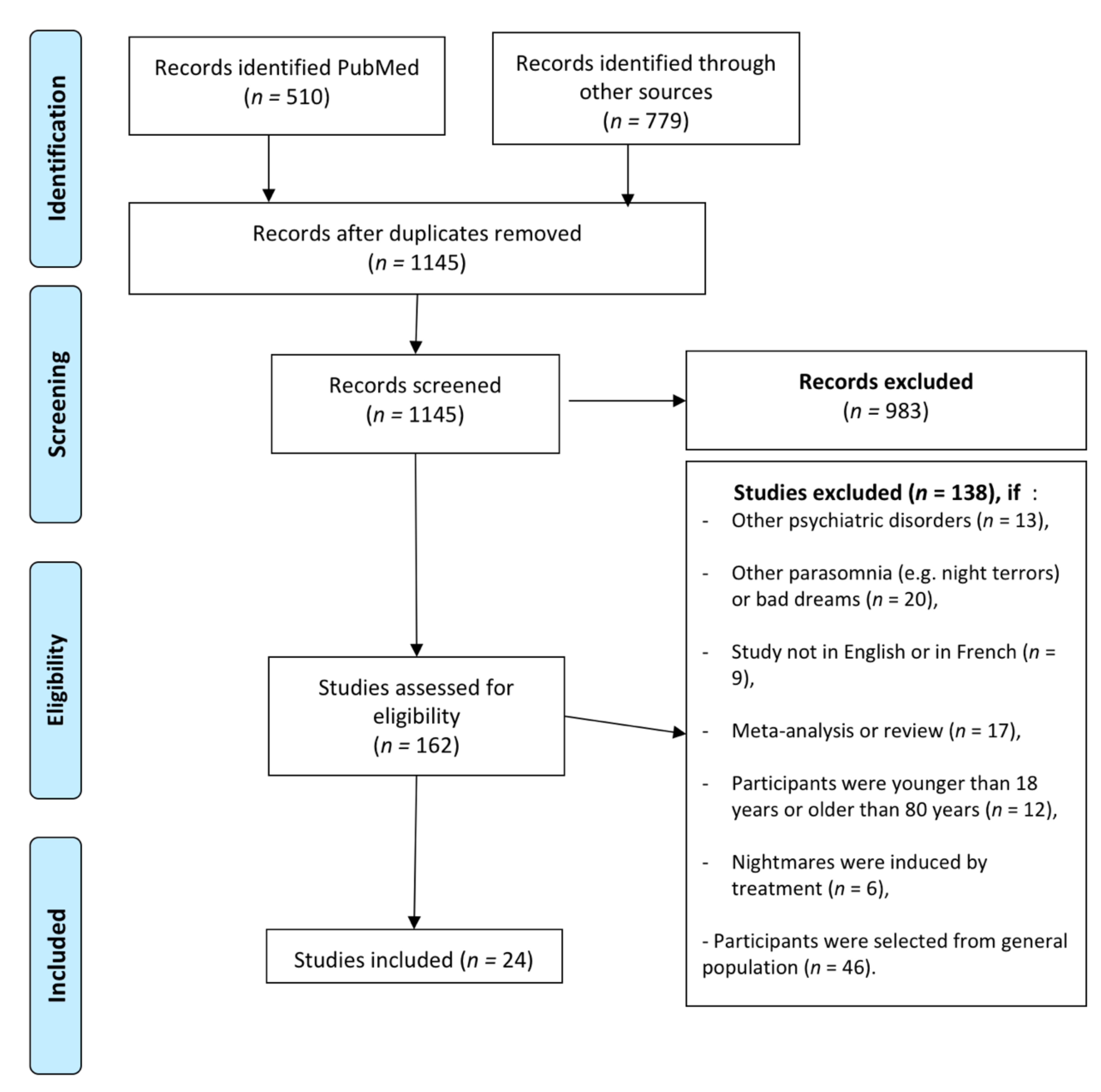
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Frequent-Nightmare Definition
3. Results
3.1. Nightmares and Mood Disorders
3.1.1. Major Depressive Disorders (MDD)
Nightmare Frequency in MDD
Suicidality and Nightmare in MDD
Nightmares and MDD Symptoms
Treatment of Nightmares in MDD
3.1.2. Bi-Polar Disorders
3.2. Nightmares and Psychotic Disorders
3.2.1. Nightmare Frequency in Psychotic Disorders
3.2.2. Nightmares and Psychotic Symptoms
3.2.3. Suicidality and Nightmares in Psychotic Disorders
3.2.4. Treatment of Nightmares in Psychotic Disorders
3.3. Study Comparing MDD and Schizophrenic Patients
4. Discussion
4.1. Clinical and Therapeutic Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Geoffroy, P.A.; Tebeka, S.; Blanco, C.; Dubertret, C.; Le Strat, Y. Shorter and longer durations of sleep are associated with an increased twelve-month prevalence of psychiatric and substance use disorders: Findings from a nationally representative survey of US adults (NESARC-III). J. Psychiatr. Res. 2020, 124, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Krakow, B. Nightmare Complaints in Treatment-Seeking Patients in Clinical Sleep Medicine Settings: Diagnostic and Treatment Implications. Sleep 2006, 29, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Semiz, U.B.; Başoğlu, C.; Ebrinc, S.; Cetin, M. Nightmare disorder, dream anxiety, and subjective sleep quality in patients with borderline personality disorder. Psychiatry Clin. Neurosci. 2008, 62, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Pigeon, W.R.; Pinquart, M.; Conner, K. Meta-Analysis of Sleep Disturbance and Suicidal Thoughts and Behaviors. J. Clin. Psychiatry 2012, 73, e1160–e1167. [Google Scholar] [CrossRef]
- Li, S.X.; Zhang, B.; Li, A.M.; Wing, Y.K. Prevalence and Correlates of Frequent Nightmares: A Community-Based 2-Phase Study. Sleep 2010, 33, 774–780. [Google Scholar] [CrossRef] [Green Version]
- Sandman, N.; Valli, K.; Kronholm, E.; Ollila, H.M.; Revonsuo, A.; Laatikainen, T.; Paunio, T. Nightmares: Prevalence among the Finnish General Adult Population and War Veterans during 1972–2007. Sleep 2013, 36, 1041–1050. [Google Scholar] [CrossRef] [Green Version]
- Janson, C.; Gislason, T.; De Backer, W.; Plaschke, P.; Björnsson, E.; Hetta, J.; Kristbjarnason, H.; Vermeire, P.; Boman, G. Prevalence of sleep disturbances among young adults in three European countries. Sleep 1995, 18, 589–597. [Google Scholar]
- Schredl, M. Nightmare frequency and nightmare topics in a representative German sample. Eur. Arch. Psychiatry Clin. Neurosci. 2010, 260, 565–570. [Google Scholar] [CrossRef]
- Kerkhof, G.A. Epidemiology of sleep and sleep disorders in The Netherlands. Sleep Med. 2017, 30, 229–239. [Google Scholar] [CrossRef]
- Nielsen, T.; Levin, R. Nightmares: A new neurocognitive model. Sleep Med. Rev. 2007, 11, 295–310. [Google Scholar] [CrossRef]
- Forbes, D.; Phelps, A.J.; McHugh, A.F.; Debenham, P.; Hopwood, M.; Creamer, M. Imagery rehearsal in the treatment of posttraumatic nightmares in Australian veterans with chronic combat-related PTSD: 12-month follow-up data. J. Trauma. Stress 2003, 16, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Leskin, G.A.; Woodward, S.H.; Young, H.E.; Sheikh, J.I. Effects of comorbid diagnoses on sleep disturbance in PTSD. J. Psychiatr. Res. 2002, 36, 449–452. [Google Scholar] [CrossRef]
- Neylan, T.C.; Marmar, C.R.; Metzler, T.J.; Weiss, D.S.; Zatzick, D.F.; Delucchi, K.L.; Wu, R.M.; Schoenfeld, F.B. Sleep Disturbances in the Vietnam Generation: Findings from a Nationally Representative Sample of Male Vietnam Veterans. Am. J. Psychiatry 1998, 155, 929–933. [Google Scholar] [CrossRef] [PubMed]
- Levin, R.; Nielsen, T. Disturbed dreaming, posttraumatic stress disorder, and affect distress: A review and neurocognitive model. Psychol. Bull. 2007, 133, 482–528. [Google Scholar] [CrossRef] [Green Version]
- Woo, M. Eye Movement Desensitization and Reprocessing Treatment of Nightmares: A Case Report. J. EMDR Pr. Res. 2014, 8, 129–134. [Google Scholar] [CrossRef]
- Sateia, M.J. International Classification of Sleep Disorders-Third Edition. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Geoffroy, P.A.; Oquendo, M.; Courtet, P.; Blanco, C.; Olfson, M.; Peyre, H.; Lejoyeux, M.; Limosin, F.; Hoertel, N. Sleep complaints are associated with increased suicide risk independently of psychiatric disorders: Results from a national 3-year prospective study. Mol. Psychiatry 2020, 1–11. [Google Scholar] [CrossRef]
- Cukrowicz, K.C.; Otamendi, A.; Pinto, J.V.; Bernert, R.A.; Krakow, B.; Joiner, T.E. The impact of insomnia and sleep disturbances on depression and suicidality. Dreaming 2006, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sjöström, N.; Hetta, J.; Waern, M. Persistent nightmares are associated with repeat suicide attempt. Psychiatry Res. 2009, 170, 208–211. [Google Scholar] [CrossRef]
- Tanskanen, A.; Tuomilehto, J.; Viinamäki, H.; Vartiainen, E.; Lehtonen, J.; Puska, P. Nightmares as Predictors of Suicide. Sleep 2001, 24, 845–848. [Google Scholar] [CrossRef] [Green Version]
- Littlewood, D.; Gooding, P.A.; Panagioti, M.; Kyle, S.D. Nightmares and Suicide in Posttraumatic Stress Disorder: The Mediating Role of Defeat, Entrapment, and Hopelessness. J. Clin. Sleep Med. 2016, 12, 393–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinova, P.; Koychev, I.; Laleva, L.; Kancheva, L.; Tsvetkov, M.; Bilyukov, R.; Vandeva, D.; Felthouse, A.; Koychev, G. Nightmares and suicide: Predicting risk in depression. Psychiatr. Danub. 2014, 26, 159–164. [Google Scholar] [PubMed]
- Ribeiro, J.D.; Yen, S.; Joiner, T.; Siegler, I.C. Capability for suicide interacts with states of heightened arousal to predict death by suicide beyond the effects of depression and hopelessness. J. Affect. Disord. 2015, 188, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horwitz, A.G.; Berona, J.; Czyz, E.K.; Yeguez, C.E.; King, C.A. Positive and Negative Expectations of Hopelessness as Longitudinal Predictors of Depression, Suicidal Ideation, and Suicidal Behavior in High-Risk Adolescents. Suicide Life-Threat. Behav. 2017, 47, 168–176. [Google Scholar] [CrossRef]
- Mume, C.O. Nightmare in schizophrenic and depressed patients. Eur. J. Psychiatry 2009, 23, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Koffel, E.; Watson, D. Unusual sleep experiences, dissociation, and schizotypy: Evidence for a common domain. Clin. Psychol. Rev. 2009, 29, 548–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. For the PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics, (11th Revision); WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Ağargün, M.Y.; Cilli, A.S.; Kara, H.; Tarhan, N.; Kincir, F.; Oz, H. Repetitive and frightening dreams and suicidal behavior in patients with major depression. Compr. Psychiatry 1998, 39, 198–202. [Google Scholar] [CrossRef]
- Agargun, M.Y.; Besiroglu, L.; Cilli, A.S.; Güleç, M.; Aydin, A.; Inci, R.; Selvi, Y. Nightmares, suicide attempts, and melancholic features in patients with unipolar major depression. J. Affect. Disord. 2007, 98, 267–270. [Google Scholar] [CrossRef]
- Besiroglu, L.; Agargun, M.Y.; Inci, R. Nightmares and terminal insomnia in depressed patients with and without melancholic features. Psychiatry Res. 2005, 133, 285–287. [Google Scholar] [CrossRef]
- Thünker, J.; Pietrowsky, R. Effectiveness of a manualized imagery rehearsal therapy for patients suffering from nightmare disorders with and without a comorbidity of depression or PTSD. Behav. Res. Ther. 2012, 50, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Li, S.X.; Lam, S.P.; Chan, J.W.Y.; Yu, M.W.M.; Wing, Y.-K. Residual Sleep Disturbances in Patients Remitted From Major Depressive Disorder: A 4-Year Naturalistic Follow-up Study. Sleep 2012, 35, 1153–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, Y.-C.; Huang, M.-C.; Chen, H.-C.; Lu, M.-K.; Chiu, Y.-H.; Shen, W.W.; Lu, R.-B.; Kuo, P.-H. Familiality and clinical outcomes of sleep disturbances in major depressive and bipolar disorders. J. Psychosom. Res. 2014, 76, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Agargun, M.Y.; Kara, H.; Inci, R. Nightmares associated with the onset of mania: Three case reports. Sleep Hypn. 2003, 5, 192–196. [Google Scholar]
- Li, S.X.; Lam, S.P.; Zhang, J.; Yu, M.W.M.; Chan, J.W.Y.; Chan, C.S.Y.; Espie, C.A.; Freeman, D.; Mason, O.; Wing, Y.K. Sleep Disturbances and Suicide Risk in an 8-Year Longitudinal Study of Schizophrenia-Spectrum Disorders. Sleep 2016, 39, 1275–1282. [Google Scholar] [CrossRef]
- Reeve, S.; Sheaves, B.; Freeman, D. Sleep Disorders in Early Psychosis: Incidence, Severity, and Association with Clinical Symptoms. Schizophr. Bull. 2019, 45, 287–295. [Google Scholar] [CrossRef]
- Fennig, S.; Salganik, E.; Chayat, M. Psychotic Episodes and Nightmares: A Case Study. J. Nerv. Ment. Dis. 1992, 180, 60. [Google Scholar] [CrossRef]
- Levin, R. Nightmares and Schizotypy. Psychiatry 1998, 61, 206–216. [Google Scholar] [CrossRef]
- Lusignan, F.-A.; Zadra, A.; Dubuc, M.-J.; Daoust, A.-M.; Mottard, J.-P.; Godbout, R. Dream content in chronically-treated persons with schizophrenia. Schizophr. Res. 2009, 112, 164–173. [Google Scholar] [CrossRef]
- Michels, F.; Schilling, C.; Rausch, F.; Eifler, S.; Zink, M.; Meyer-Lindenberg, A.; Schredl, M. Nightmare frequency in schizophrenic patients, healthy relatives of schizophrenic patients, patients at high risk states for psychosis, and healthy controls. Int. J. Dream Res. 2014, 7, 9–13. [Google Scholar]
- Sheaves, B.; Onwumere, J.; Keen, N.; Stahl, D.; Kuipers, E. Nightmares in Patients with Psychosis: The Relation with Sleep, Psychotic, Affective, and Cognitive Symptoms. Can. J. Psychiatry 2015, 60, 354–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shorkey, C.; Himle, D.P. Systematic desensitization treatment of a recurring nightmare and related insomnia. J. Behav. Ther. Exp. Psychiatry 1974, 5, 97–98. [Google Scholar] [CrossRef]
- Sheaves, B.; Onwumere, J.; Keen, N.; Kuipers, E. Treating your worst nightmare: A case-series of imagery rehearsal therapy for nightmares in individuals experiencing psychotic symptoms. Cogn. Behav. Ther. 2015, 8. [Google Scholar] [CrossRef]
- Sheaves, B.; Porcheret, K.; Tsanas, A.; Espie, C.A.; Foster, R.G.; Freeman, D.; Harrison, P.J.; Wulff, K.; Goodwin, G.M. Insomnia, Nightmares, and Chronotype as Markers of Risk for Severe Mental Illness: Results from a Student Population. Sleep 2016, 39, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Sheaves, B.; Holmes, E.A.; Rek, S.; Taylor, K.M.; Nickless, A.; Waite, F.; Germain, A.; Espie, C.A.; Harrison, P.J.; Foster, R.; et al. Cognitive Behavioural Therapy for Nightmares for Patients with Persecutory Delusions (Nites): An Assessor-Blind, Pilot Randomized Controlled Trial. Can. J. Psychiatry 2019, 64, 686–696. [Google Scholar] [CrossRef] [Green Version]
- Sjöström, N.; Waern, M.; Hetta, J. Nightmares and Sleep Disturbances in Relation to Suicidality in Suicide Attempters. Sleep 2007, 30, 91–95. [Google Scholar] [CrossRef]
- Lamis, D.A.; Innamorati, M.; Erbuto, D.; Berardelli, I.; Montebovi, F.; Serafini, G.; Amore, M.; Krakow, B.; Girardi, P.; Pompili, M. Nightmares and suicide risk in psychiatric patients: The roles of hopelessness and male depressive symptoms. Psychiatry Res. 2018, 264, 20–25. [Google Scholar] [CrossRef]
- Hombali, A.; Seow, E.; Yuan, Q.; Chang, S.H.S.; Satghare, P.; Kumar, S.; Verma, S.K.; Mok, Y.M.; Chong, S.A.; Subramaniam, M. Prevalence and correlates of sleep disorder symptoms in psychiatric disorders. Psychiatry Res. 2019, 279, 116–122. [Google Scholar] [CrossRef]
- Khurshid, K.A. Comorbid Insomnia and Psychiatric Disorders: An Update. Innov. Clin. Neurosci. 2018, 15, 28–32. [Google Scholar] [PubMed]
- Geoffroy, P.A.; Hoertel, N.; Etain, B.; Bellivier, F.; Delorme, R.; Limosin, F.; Peyre, H. Insomnia and hypersomnia in major depressive episode: Prevalence, sociodemographic characteristics and psychiatric comorbidity in a population-based study. J. Affect. Disord. 2018, 226, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.D.; Thompson, A.; King, L.; Corbett, B.; Shnaider, P.; Cyr, K.S.; Nelson, C.; Sareen, J.; Elhai, J.D.; Zamorski, M. Insomnia, psychiatric disorders and suicidal ideation in a National Representative Sample of active Canadian Forces members. BMC Psychiatry 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadorff, M.R.; Lambdin, K.K.; Germain, A. Pharmacological and non-pharmacological treatments for nightmare disorder. Int. Rev. Psychiatry 2014, 26, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Rek, S.; Sheaves, B.; Freeman, D. Nightmares in the general population: Identifying potential causal factors. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1123–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andorko, N.D.; Millman, Z.B.; Klingaman, E.A.; Medoff, D.; Kline, E.R.; Devylder, J.E.; Reeves, G.; Schiffman, J. Association between sleep, childhood trauma and psychosis-like experiences. Schizophr. Res. 2018, 199, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.; Lereya, S.T.; Lewis, G.; Zammit, S.; Fisher, H.L.; Wolke, D. Childhood sleep disturbance and risk of psychotic experiences at 18: UK birth cohort. Br. J. Psychiatry 2015, 207, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Gieselmann, A.; Aoudia, M.A.; Carr, M.; Germain, A.; Gorzka, R.; Holzinger, B.; Kleim, B.; Krakow, B.; Kunze, A.E.; Lancee, J.; et al. Aetiology and treatment of nightmare disorder: State of the art and future perspectives. J. Sleep Res. 2019, 28, e12820. [Google Scholar] [CrossRef] [Green Version]
- Schredl, M.; Göritz, A.S. Nightmare Themes: An Online Study of Most Recent Nightmares and Childhood Nightmares. J. Clin. Sleep Med. 2018, 14, 465–471. [Google Scholar] [CrossRef]
- Nisha, A.R.; Rochelle, S.Z.; Sanford, H.A.; Kenneth, R.C.; Susmita, C.; Anoop, K.; Rama, K.M.; Kannan, R.; David, A.K.; Sabin, R.B.; et al. Best practice guide for the treatment of nightmare disorder in adults. J. Clin. Sleep Med. 2010, 6, 389–401. [Google Scholar]
- Schredl, M. The Mannheim Dream Questionnaire (MADRE): Retest reliability, age and gender effects. Int. J. Dream Res. 2014, 7, 141–147. [Google Scholar]
- Krakow, B.; Schrader, R.; Tandberg, D.; Hollifield, M.; Koss, M.P.; Yau, C.; Cheng, D.T. Nightmare frequency in sexual assault survivors with PTSD. J. Anxiety Disord. 2002, 16, 175–190. [Google Scholar] [CrossRef]
- Wichniak, A.; Wierzbicka, A.; Walęcka, M.; Jernajczyk, W. Effects of Antidepressants on Sleep. Curr. Psychiatry Rep. 2017, 19, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors Years | Study Design | Aims | n | Age (Years) | Sex F | Diagnosis Criteria for Psychiatric Disorder | Nightmares: Diagnosis and Severity | Other Evaluation | Main Results | Comments |
|---|---|---|---|---|---|---|---|---|---|---|
| Agargu, 1998 [29] | Controlled study | To examine the association between repetitive and frightening dreams and suicidal tendency in patients with major depression | MDD, n = 29 | 31.6 | 69% (0) | DSM-III-R criteria for major depression | All patients received an oral definition of nightmare. Nightmare frequency Frequent nightmare if ≥2/week | SADS suicide subscale ≥ 3 BDI | Mean suicidality score was higher in MDD patients with nightmares than in the control group: 4.2 vs. 2.9 in the second group, p = 0.014. 72% of patients with nightmares classified as being suicidal vs. 47% in the non-nightmare group. | Controlled group: depressed patients with dreams but no nightmares (n = 31) |
| Agargun, 2003 [30] | Cases reports | To discuss relationship between dreams and the first episode of the illness in term of mood regulatory functions of dream | ME, n = 3 | 29.0 | 33.3% (n = 3) | DSM-IV criteria | - | - | All patients had one nightmare before decompensation of their first manic episode | |
| Besiroglu, 2004 [31] | Controlled study | To investigate the relationship between nightmares ant terminal insomnia un unipolar depressed patients with melancholic features | MDD, n= 82 (unipolar) | 32.4 | 58.5% (n = 48) | DSM-IV criteria | All patients received an oral definition of nightmare. Nightmare frequency Frequent nightmare if ≥ 2/week | HDRS (items 6, 7 and 8 for insomnia) | Nightmares were more frequent in the melancholic feature group (90%, n = 74), than in non-melancholic group (56%, n = 42), p < 0.001. Nightmares were significantly more frequent in the patients with terminal insomnia than without (regardless of melancholic features): 90.1% vs. 19.4% respectively (p < 0.001). | Controlled group: depressed patients without melancholic features (n = 75) |
| Agargun, 2007 [32] | Controlled study | To examines the relationship among nightmares, suicide attempts and melancholic features in unipolar major depressed patients | MDD, n = 100 | 32.1 | 51% (n = 51) | DSM-IV criteria | ICSD-R criteria. All patients received an oral definition of nightmare Nightmare frequency Frequent nightmare if ≥ 2/week | Suicide attempt during current episode (≥1) HDRS (items 6, 7 and 8 for insomnia) | MDD with melancholic features: 28% (n = 28) suicide attempt during current episode; significant difference between melancholic patients with and without suicidal attempt in terms of frequency of middle and terminal insomnia and nightmares (nightmares, n = 27 (96%) in suicide attempt group, vs. n = 57 (79%) in non-suicide attempt group (p = 0.036)). No significant difference in the non-melancholic group for suicide attempt in term of nightmares and insomnia. Nightmares more common in MDD with melancholic feature (n = 84, 84%) than non-melancholic features (n = 28, 57%); p = 0.001. Nightmares more frequent in patients with suicidal attempt (n = 33.86%), than non-attempters (n = 79, 71%); p = 0.039. | Controlled group: depressed patients without melancholic features (n = 49) |
| Thünker, 2012 [33] | Cohort | To test the effectiveness of standardized nightmare therapy (based on IRT) in patients suffering from nightmares only, or with depression or PTSD. | MDD, n = 21 | 30.0 | - | ND | Self-questionnaire (nightmare frequency, anxiety during nightmares and daytime distress (7-point scale)) | Overall improvement of therapy on a 7-point scale | Decrease of nightmare frequency after intervention in MDD patients; decrease of anxiety after intervention | 8 therapy session of 50 min each |
| Li, 2012 [34] | Prospective cohort | To investigate the prevalence and persistence of nocturnal sleep symptoms, and examine sociodemographic, clinical and psychosocial correlates of residual sleep disturbances in remitted depressed patients and investigate association of functional outcomes and suicidal ideation with residual sleep disturbances in remitted depressed patients. | 362 | 44.6 | 81.7% (n = 296) | ICD-10 criteria | Sleep questionnaire for insomnia and nightmare (5-point scale) Nightmare Distress Questionnaire (NDQ) | Suicide evaluation: MINI suicidality module | Patients with nightmares and insomnia had fewer chance to be in remission of MDD at 4 years (29.8% of remission in patients with nightmares (n= 36) vs. 47.3% of remission in patients without nightmares (n = 114), p < 0.01). Frequent nightmare at baseline was significantly associated with residual nightmare at follow up (OR = 5.17, 95% CI (13.35–19.9)) after controlling for sociodemographic factors and psychiatric comorbidity. Suicidal ideation was significantly associated with residual nightmares (OR = 8.40, 95% CI (1.79–39.33)) after controlling for confounding factors | There were no definition of nightmares |
| Marinova, 2014 [22] | Cohort | To test the hypothesis that nightmares are associated with an elevated suicidal risk in depressed patients | RDD, n = 44 BD, n = 8 | 24 to 75 | 53.8% (n = 28) | ICD-10 criteria | Nightmare: defined as unpleasant dream Dream questionnaire Nightmare yes/non (no measure of frequency) | Question 3 of HDRS for suicidality | Difference between RDD and BD: 64% of RDD had nightmares vs. 25% of BD (p < 0.044). In RDD subgroup, patients with nightmares had significantly higher average score on the HDRS item on suicide risk (2.36) than those without nightmare (1.00), p < 0.005. They had history of suicide attempts significantly more frequently (35% vs. 6%, p < 0.05). No differences in the BD subgroup. | No differentiation bad dreams and nightmares |
| Woo, 2014 [35] | Case report | To describe EMDR treatment of nightmare and highlights various aspects of EMDR therapy | MDD, n = 1 | 36 | 100% (n = 1) | Clinical examination | 4–5/weeks for 9 years | - | Better after four sessions of EMDR | - |
| Lai, 2014 [36] | Cohort | To examine whether patients with BD and MDD exhibit different sleep problems and to what extent their relatives have sleep complaints | BD, n = 363 MDD, n = 157 | 35.5 (BD), 45.6 (MDD) | 52.3% (n = 190) for BD, 68.9% (n = 108) for MDD | DSM-IV criteria | PSQI for sleep quality | - | Frequent nightmares in patients with MDD or BD were associated to a higher risk of suicidal ideations (OR = 2.88) and attempts (OR = 1.89) after adjustment for age at interview and sex. | - |
| Authors Years | Type of Article | Aims | n | Age (Years) | Sex F | Diagnosis Criteria | Nightmares: Diagnosis and Severity | Other Evaluation | Main Results | Comments |
|---|---|---|---|---|---|---|---|---|---|---|
| Shorkey, 1974 [37] | Case report | Treatment of recurrent nightmare with desensitization | Schizophrenia, n = 1 | 38 | 0% (n = 0) | Clinical examination | Daily nightmares | - | In the nightmare, the devil was a snake; treatment by desensitization of fears of snakes, with efficacy on nightmares (no nightmares avec 2 years follow up) | |
| Fennig, 1992 [38] | Brief Report | Presentation of a patient which had a transition from nightmare to brief psychotic episode | BPE, n= 1 | 78 | 0% (n = 0) | Clinical examination | Recurrent nightmare for 3 years | - | Brief psychotic episode occurring after a nightmare, with same thematic; treatment by TRIAZOLAM 25 mg/d and OXAZEPAM 20 mg/d with no recurrence after 6 months follow up | |
| Levin, 1998 [39] | Case report | To illustrate how the nightmare may presage the underlying psychological disorganization during the period of psychic decompensation | Schizophrenia, n = 1 | 40 | 100% (n = 1) | DSM-IV criteria | - | Insomnia and nightmare the week before relapse; same thematic of delusion and hallucination, than in nightmares preceding decompensation. | The patient remained able to differentiate her nightmares from her waking hallucinations and her waking life. | |
| Lusignan, 2009 [40] | Controlled study | To investigate dream content in patients with schizophrenia using both questionnaire and laboratory REM sleep awakenings | Schizophrenia, n = 14 | 25.5 | (n = 1) | DSM-IV-TR criteria | Oral definition of nightmares Dream questionnaire (11 items self-report): nightmare frequency and dream emotions | 3 consecutive nights in sleep laboratory; dream report collected following awakenings from REM sleep | Self-report questionnaire: patients with schizophrenia reported nightmares more frequently (4.1 vs. 2.1, p = 0.006) and more nightmare per year (22.8 vs. 3.5, p = 0.003). No significant difference for bad dreams, dream recall, lucid dreaming, control of dreams or physical sensation during dreams. Laboratory measures: 92 awakenings from REM sleep, with 78 dream reports (no difference between 2 groups in dream reports, and white dream) | Control group, n = 15. No difference in polysomnographic measures in both groups. |
| Michels, 2014 [41] | Controlled study | To investigate nightmare frequency and its correlates in patients with schizophrenia | Schizophrenia, n = 17 | 32.9 | 47.0% (n = 8) | ND | DDNSI for frequency of nightmares (0 = never to 7 = several times a week) and intensity (distress) | ISI for insomnia C-SSRS for suicide BDI | Higher frequency of nightmares in patients with schizophrenia (3.65, p = 0.0145), and ARMS patients (3.79, p = 0.003) than HC No significant correlation between BDI and nightmare frequency No significant correlation between PANNS and nightmare frequency | Comparison with 14 patients with at risk mental states for psychosis (ARMS) and 17 healthy relatives of patients |
| Sheaves, 2015 [42] | Case series | To assess the acceptability and feasibility of Imagery Rehearsal (IR) for the treatment of nightmares in the context of psychosis | p, n= 6 | 39.7 | 66.6% (n = 4) | ND | 7 points rating scale for nightmare intensity, vividness and distress, and if recurrent (yes/no) Mean of 4.4 per week | - | 5/6 participants attended 4–6 sessions of IR. Mean nightmare related distress across the week decreased from 5.43 to 4.28; improvement on vividness and intensity of nightmares; no decrease of nightmare frequency, but patients described a change in emotional response. | Participants with PTSD were not excluded from the study IR method: psychoeducation, collaboratively planning a rescript of the nightmare, elaborating the rescript with sensory detail through guided imagery and daily practice of the new dream script; 4–6 sessions |
| Sheaves, 2015 [43] | Cohort | To examine the prevalence of nightmares in people with psychosis and to describe the link between nightmares and sleep quality, psychotic, affective and cognitive symptoms | p, n= 40 | 41.9 | 62.5% (n = 25) | ND | Nightmare frequency 7 points rating scale for nightmare intensity, vividness and distress, and if recurrent (yes/no) | PSQI for sleep quality | At least one nightmare in the past 14 nights in 28 patients (70%). 22/40 (55.0%) patients experienced at least weekly nightmares. Nightmare frequency was associated with poorer sleep: large positive correlation between nightmare frequency and PSQI while controlling for antipsychotic dose; nightmare frequency was negatively correlate with sleep efficiency. Nightmare distress, rather than frequency, is a best account for the association between nightmares and daytime impairment: correlation between nightmare distress and delusional severity, depression, anxiety, and stress. | n = 17 (42.5%) of patients screened positive for PTSD; 11/17 (65%) reported weekly nightmares. This was not significantly higher than the 10/20 (50%) participants who reported weekly nightmare but did not screen positive for PTSD. No difference in nightmare distress between PTSD and without PTSD. |
| Chiu, 2016 [44] | Cohort | To explore the lived experience of sleep problems in people with schizophrenia-spectrum disorders | 14 | ND | 50% (n = 7) | ND | - | n = 7 (50%) of patients reported nightmares | - | |
| Li, 2016 [45] | Cohort | To examine the prevalence of sleep disturbances, particularly frequent insomnia and nightmares, and their prospective associations with the risk of suicide attempts in patients with schizophrenia spectrum disorder | p, n = 388 (Schizophrenia n = 308) | 41.0 | 54.9% (n = 213) | ICD-10 criteria | Frequent nightmare was defined as having nightmares of at least once a week in the past year Sleep questionnaire for insomnia and nightmares (5-point scale for frequency) | - | At baseline: 19.3% frequent insomnia and 9.0% frequent nightmares. Comorbid insomnia and nightmare reported in 3.4%. Patients with frequent nightmare were more likely to report frequent insomnia (37.1% vs. 17.6%, p < 0.01). Patients with frequent insomnia were more likely to have comorbid nightmare disturbances (17.3%, vs. 7.0%, p < 0.01). The complaint of frequent nightmares was associated with a lifetime history of suicide attempts (42.9% vs. 19.3%); it did not predict an increased risk of suicide attempt over the follow up period. | 8 years observational study on consecutively recruited cohort of psychiatric outpatients with schizophrenia spectrum diagnosis Comorbidity of insomnia and nightmare disturbances was significantly associated with an increased risk of suicide attempts, not only in lifetime (p < 0.001), but also during the 8 years follow up period (p < 0.01). |
| Reeve, 2018 [46] | Cohort | To report on the presence, severity and treatment of sleep disorders in patients with non-affective psychosis | p, n = 60 | 23.7 | 35.0% (n = 21) | DSM-5 | ICSD-2, ICSD-3 Diagnostic Interview for Sleep Patterns and Disorders | Actigraphy (wrist-based activity monitoring device) and sleep diary for 7 days | 80% (n = 48) of participants received a positive screen or diagnosis for at least one sleep disorder: insomnia was the most frequent (n = 30. 50%), then nightmare (n = 29, 48.3%). Comorbidity: average of 3.3 sleep disorder per patient. n = 30 (33%) had bot insomnia and nightmares. Severity of nightmares: Mild n = 2 (6.9%), moderate n = 11 (37.9%), severe n = 16 (55.2%); Night terror, nightmare disorder and RLS were the disorders least commonly discussed with a clinician (50%). | No significantly difference in antipsychotic dose between patients with and without nightmares. |
| Sheave, 2019 [47] | Randomized Control trial | To test the potential benefits of imagery focused cognitive behavioral therapy (CBT) for nightmares on nightmare severity and persecutory delusions. | 24 patients with weekly nightmares and persecutory delusions in the context of a diagnosis of non-affective psychosis. | 41.0 | 42% (n = 10) | DDNSI Sleep Condition Indicator (SCI) | PSQI for sleep quality | Large effect size reductions in nightmares and insomnia post treatment (4 weeks) (DDNSI d = −1.06; SCI d = −1.4) maintained at follow up (8 weeks). Post-treatment improvements were observed in paranoia (GPTS), affective symptoms (DASS-21), dissociation (DES-B), and emotional wellbeing (WEMWBS). There were no changes in hallucinations (CAPS) or activity levels (time budget). | 12 treatment, 12 control. Core technique was imagery rehearsal training. Additional strategies included: psychoeducation about nightmares, reducing pre-sleep hyperarousal, increasing coping skills, reducing preoccupation with nightmares, stabilizing REM sleep. |
| Authors Years | Type of Article | Aims | Diagnosis | n | Age (Years) | Sex F | Diagnosis Criteria | Nightmares | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Sjöström, 2007 [48] | Cohort | To examine the prevalence of specific sleep disturbances in suicide attempters and to test the associations between specific sleep disturbances and suicidality | MDD, n = 55 (33.3%), other depression n = 20 (12.1%); psychotic disorder n = 11 (6.6%), alcohol/substance misuse disorder n = 41 (24.8%); anxiety disorder and other disturbance n = 27 (16.3%) | 165 | 35.3 | 78% (n = 129) | DSM-IV | How often do you experience nightmare from 1 to 5 Uppsala Sleep Inventory (USI) for sleep disturbance | Frequent nightmares were less common in patients who scored 0 on all 5 suicidality items (12%) than in those scoring ≥1 on any suicidality item (45%); p <0.001 |
| Sjöström, 2009 [19] | Prospective cohort | To determine whether those who reported sleep disturbances in general and frequent nightmares in particular were at increased risk of repeat suicide attempt | MDD, n = 55 (33.3%), other depression n = 20 (12.1%); psychotic disorder n = 11 (6.6%), alcohol/substance misuse disorder n = 41 (24.8%); anxiety disorder and other disturbance n = 27 (16.3%) | 165 | 35.3 | 78% (n = 129) | DSM-IV | How often do you experience nightmare from 1 to 5 | Repeaters had more frequent nightmare than non-repeaters (n = 22 (52%) vs. n = 26 (30%), p = 0.002). 98 patients completed a 2 month follow up: persistent nightmare were about 3 times more common in repeaters (n = 13 (46%), vs. n = 10 (14%) p = 0.001) |
| Mume, 2009 [25] | Controlled study | To highlight nightmare in healthy individuals and to demonstrate its possible association with psychopathology, using schizophrenia and depressive episode as examples | Schizophrenia (n = 54), major depressive disorder (n = 40) | 94 | 42.6 (schizophrenic patients), 43.1 (MDD patients) | - | - | Did you experience nightmare in the past one year? Yes/No/ if yes, how many times did you experience it in the past one year? | 9/54 (16.7%) of schizophrenic patients experienced nightmare in the previous years, and 7/40 (17.5%) MDD patients (vs 6/123 (4.9%) HC). Significantly more frequent in psychiatric patients (17%) than HC (p = 0.0007); no significant difference between schizophrenic and MDD patients. Number of nightmare schizophrenic patients mean 42.7 (sd = 6.3); 44.6 (sd = 5.9) for MDD, and 18 (sd = 6.6) for HC, p < 0.05. |
| Lamis, 2018 [49] | Cohort | To test the hopelessness theory of suicide risk in psychiatric patients who may or may not experiencing nightmares. | Non-affective psychosis (23.3%), Bipolar I (26.2%), bipolar II (3.5%), MDD (11.6%), schizoaffective disorder (23.3%), other (12.8%) | 172 | 39.15 | n = 91 | DSM-IV-TR criteria + MINI Beck Hopelessness Scale (BHS) | DDNSI for frequency and severity of nightmares. | Patients who reported monthly to weekly nightmares (compared to patients who reported yearly or no nightmare) were younger and more likely to have been hospitalized for a recent suicide attempt. They also had higher scores on BHS and MINI suicide risk. Severe hopelessness in 44% of frequent nightmares vs. 22.6% |
| Main Results Regarding Nightmares | Studies | |||
|---|---|---|---|---|
| Mood disorders | Depression | Frequency | • Nightmares are more frequent in patients with MDD and melancholic features than without. | Besiroglu, 2004 [31] |
| Agargun 2007 [32] | ||||
| • Nightmares are more frequent in unipolar depression than bipolar depression | Marinova, 2014 [22] | |||
| Suicide | • Higher suicidality score in MDD patients with frequent nightmares * than without | Agargun, 1998 [29] | ||
| • More suicidal ideation in MDD patients with frequent nightmares ** than without | Li, 2012 [34] | |||
| • More suicidal attempts in MDD patients with melancholic features with frequent nightmares * than without | Agargun 2007 [32] | |||
| • More suicidal ideation and attempts in unipolar MDD and bipolar MDD in patients with frequent nightmares **** | Lai, 2014 [36] | |||
| Marinova, 2014 [22] | ||||
| Treatment | • Decrease of nightmare frequency and anxiety after IRT intervention in MDD patients | Thünker, 2012 [33] | ||
| • Improvement of nightmare frequency inn 36 MDD patients after four sessions of EMDR | Woo, 2014 [35] | |||
| Evolution | • Patients with frequent nightmares ** were less in remission at four years than those without nightmares | Li, 2012 [34] | ||
| Mania | • Three patients had nightmares as prodromal symptoms of their first manic episode | Agargun, 2003 [30] | ||
| Psychotic disorders | Frequency | • Nightmares are more frequent in patient with schizophrenia than in healthy controls | Lusignan, 2009 [40] | |
| Michels, 2014 [41] | ||||
| • Frequency of frequent nightmares ** ranging from 9 to 55% | Sheaves, 2015 [43] | |||
| Chiu, 2016 [44] | ||||
| Li, 2016 [45] | ||||
| • Comorbid insomnia and nightmares are frequent in schizophrenia ∘ Patients with frequent nightmares ** were more likely to report frequentinsomnia ∘ Patients with frequent insomnia were more likely to have comorbid nightmares | Li, 2016 [45] | |||
| • Nightmares are the second most frequent sleep disorder, after insomnia, in patients with schizophrenia. | Reeve, 2018 [46] | |||
| Symptoms | • Same themes of delusion and hallucination than in nightmares preceding psychotic decompensation (two reports) | Levin, 1998 [39] | ||
| Fennig, 1992 [38] | ||||
| • No significant correlations between depressive symptoms (assessed with BDI) and nightmare frequency • No significant correlations between psychotic symptoms (assessed with PANNS) and nightmare frequency | Michels, 2014 [41] | |||
| • Nightmare distress, rather than frequency, is the best marker for the association between nightmares and daytime impairment: significant correlations between nightmare distress and delusional severity, depression, anxiety, and stress. | Sheaves, 2015 [43] | |||
| Suicide | • Patients with frequent nightmares ** have more lifetime of suicide history and increase risk of suicide attempts | Li, 2016 [45] | ||
| Treatment | • Efficacy of treatment by desensitization (one report) • Improvement of IRT on emotional response, not on nightmare frequency | Shorkey, 1974 [37] | ||
| Sheaves, 2015 [42] | ||||
| • Imagery focused cognitive behavioral therapy: large effect size reductions in nightmares and insomnia post treatment (4 weeks) | Sheave, 2019 [47] | |||
| Comparing studies | Frequency | • Significantly more frequent in psychiatric patients (schizophrenia and MDD) than healthy controls • No significant differences between patients with schizophrenia and MDD | Mume, 2009 [25] | |
| Suicide | • Higher suicidality scores (assessed with SUAS) in patients with frequent nightmares than without (MDD, schizophrenia) | Sjöström, 2007 [48] | ||
| • Patients with more than one past suicide attempts had more frequent nightmares**** than those with first suicide attempts | Sjöström, 2009 [19] | |||
| • Patients who reported monthly to weekly nightmares were younger and more likely to have been hospitalized for a recent suicide attempt. • Severe hopelessness more frequent in patients with nightmares | Lamis, 2018 [49] | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akkaoui, M.A.; Lejoyeux, M.; d’Ortho, M.-P.; Geoffroy, P.A. Nightmares in Patients with Major Depressive Disorder, Bipolar Disorder, and Psychotic Disorders: A Systematic Review. J. Clin. Med. 2020, 9, 3990. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123990
Akkaoui MA, Lejoyeux M, d’Ortho M-P, Geoffroy PA. Nightmares in Patients with Major Depressive Disorder, Bipolar Disorder, and Psychotic Disorders: A Systematic Review. Journal of Clinical Medicine. 2020; 9(12):3990. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123990
Chicago/Turabian StyleAkkaoui, Marine Ambar, Michel Lejoyeux, Marie-Pia d’Ortho, and Pierre A. Geoffroy. 2020. "Nightmares in Patients with Major Depressive Disorder, Bipolar Disorder, and Psychotic Disorders: A Systematic Review" Journal of Clinical Medicine 9, no. 12: 3990. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9123990