

A High-Fidelity Artificial Urological System for the Quantitative Assessment of Endoscopic Skills
 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Fabrication of the Endourological Organ Models
2.2. Validation of the Phantom Using Endoscopy and CT
2.3. Design and Prototyping of Surgical Endoscopic Simulator
2.4. Quantitative Assessment of the Endoscopic Skills by Video Analysis
3. Results
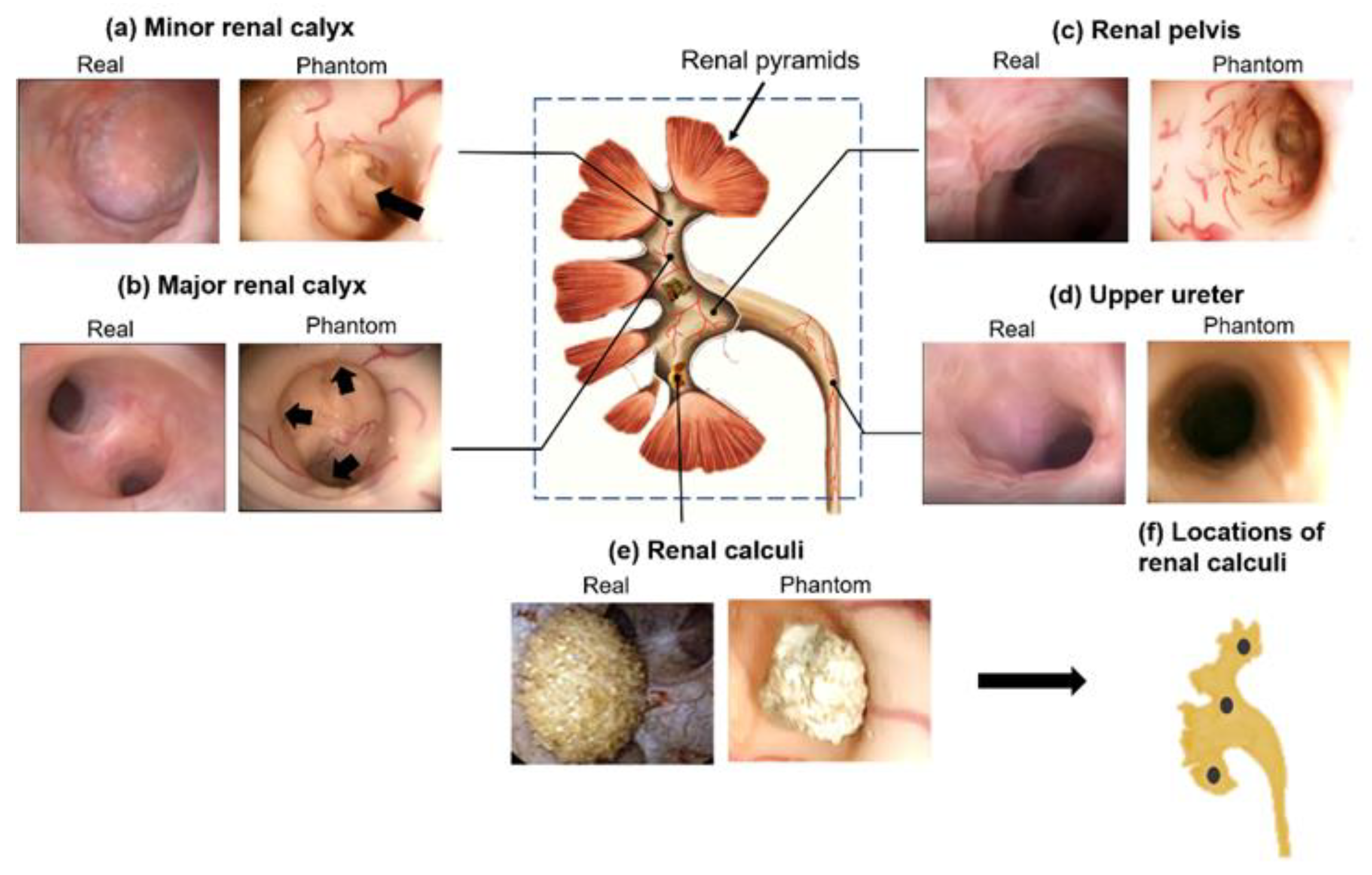
3.1. Endoscopic Validation of the Collecting System Phantom
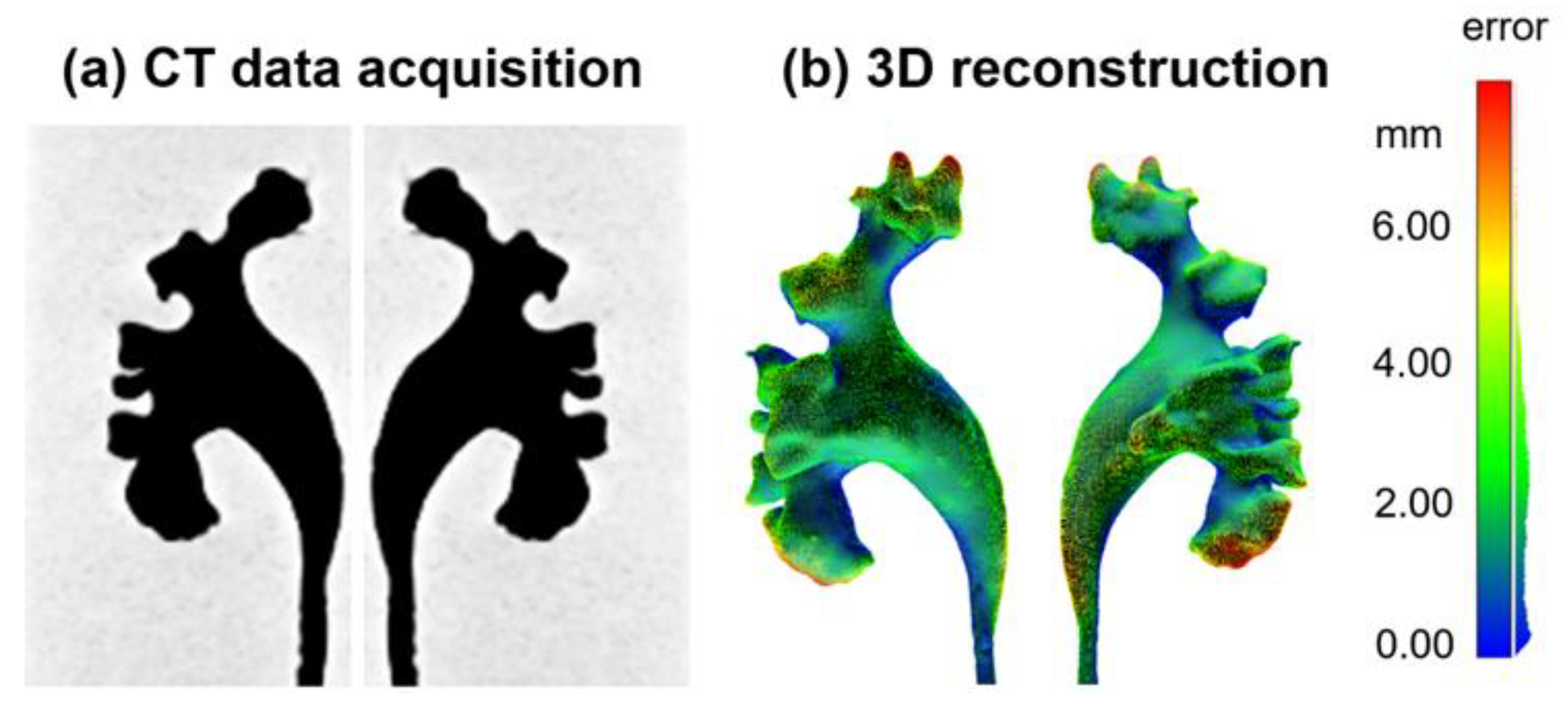
3.2. CT Validation of the Collecting System Phantom
3.3. Ureteroscopy Simulation and Quantitative Assessments of the Endoscopic Skills
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Young, H.H.; McKay, R.W. Congenital Valve Obstruction of the Prostatic Urethra; RR Donnelley: Chicago, IL, USA, 1929. [Google Scholar]
- Skolarikos, A.; Gravas, S.; Laguna, M.P.; Traxer, O.; Preminger, G.M.; de la Rosette, J. Training in Ureteroscopy: A Critical Appraisal of the Literature. BJU Int. 2011, 108, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Manzo, B.O.; Lozada, E.; Manzo, G.; Sánchez, H.M.; Gomez, F.; Figueroa, A.; Gonzalez, A. Radiation-Free Flexible Ureteroscopy for Kidney Stone Treatment. Arab J. Urol. 2019, 17, 200–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Türk, C.; Petřík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU Guidelines on Interventional Treatment for Urolithiasis. Eur. Urol. 2016, 69, 475–482. [Google Scholar] [CrossRef]
- Perez Castro, E.; Osther, P.J.S.; Jinga, V.; Razvi, H.; Stravodimos, K.G.; Parikh, K.; Kural, A.R.; de la Rosette, J.J. Differences in Ureteroscopic Stone Treatment and Outcomes for Distal, Mid-, Proximal, or Multiple Ureteral Locations: The Clinical Research Office of the Endourological Society Ureteroscopy Global Study. Eur. Urol. 2014, 66, 102–109. [Google Scholar] [CrossRef]
- De Coninck, V.; Keller, E.X.; Somani, B.; Giusti, G.; Proietti, S.; Rodriguez-Socarras, M.; Rodríguez-Monsalve, M.; Doizi, S.; Ventimiglia, E.; Traxer, O. Complications of Ureteroscopy: A Complete Overview. World J. Urol. 2020, 38, 2147–2166. [Google Scholar] [CrossRef]
- Weinberg, J.J.; Ansong, K.; Smith, A.D. Complications of Ureteroscopy in Relation to Experience: Report of Survey and Author Experience. J. Urol. 1987, 137, 384–385. [Google Scholar] [CrossRef]
- Aydin, A.; Raison, N.; Khan, M.S.; Dasgupta, P.; Ahmed, K. Simulation-Based Training and Assessment in Urological Surgery. Nat. Rev. Urol. 2016, 13, 503–519. [Google Scholar] [CrossRef] [PubMed]
- Mains, E.; Tang, B.; Golabek, T.; Wiatr, T.; Ross, G.; Duncan, A.; Howie, D.; Tait, I.; Chłosta, P.; Kata, S.G. Ureterorenoscopy Training on Cadavers Embalmed by Thiel’s Method: Simulation or a Further Step towards Reality? Initial Report. Cent. Eur. J. Urol. 2017, 70, 81–87. [Google Scholar]
- Soria, F.; Morcillo, E.; Serrano, A.; Cansino, R.; Rioja, J.; Fernandez, I.; de la Cruz, J.; van Cleynenbreugel, B.; Sanchez-Margallo, F.M. Development and Validation of a Novel Skills Training Model for Retrograde Intrarenal Surgery. J. Endourol. 2015, 29, 1276–1281. [Google Scholar] [CrossRef]
- Dolmans, V.E.M.G.; Schout, B.M.A.; de Beer, N.A.M.; Bemelmans, B.L.H.; Scherpbier, A.J.J.A.; Hendrikx, A.J.M. The Virtual Reality Endourologic Simulator Is Realistic and Useful for Educational Purposes. J. Endourol. 2009, 23, 1175–1181. [Google Scholar] [CrossRef]
- Blankstein, U.; Lantz, A.G.; Honey, R.J.D.; Pace, K.T.; Ordon, M.; Lee, J.Y. Simulation-Based Flexible Ureteroscopy Training Using a Novel Ureteroscopy Part-Task Trainer. Can. Urol. Assoc. J. 2015, 9, 331. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Zhang, Q.; Deng, J.; Cai, Y.; Huang, J.; Li, F.; Xiong, K. A Shortage of Cadavers: The Predicament of Regional Anatomy Education in Mainland China. Anat. Sci. Educ. 2018, 11, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Niedzielska, I.; Bąk, M.; Niedzielski, D.; Okła, H.; Gabor, J.; Stanula, A.; Paluch, J.; Swinarew, A.S. Temporomandibular Joint Prostheses: Optimal Materials for the Optimal Stomatognathic System Performance—Preliminary Study. J. Funct. Biomater. 2021, 12, 7. [Google Scholar] [CrossRef]
- Tappa, K.; Jammalamadaka, U. Novel Biomaterials Used in Medical 3D Printing Techniques. J. Funct. Biomater. 2018, 9, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sander, I.; Liepert, T.; Doney, E.; Leevy, W.; Liepert, D. Patient Education for Endoscopic Sinus Surgery: Preliminary Experience Using 3D-Printed Clinical Imaging Data. J. Funct. Biomater. 2017, 8, 13. [Google Scholar] [CrossRef] [Green Version]
- Villa, L.; Somani, B.K.; Sener, T.E.; Cloutier, J.; Cloutier, J.; Butticè, S.; Marson, F.; Ploumidis, A.; Proietti, S.; Traxer, O. Comprehensive Flexible Ureteroscopy (FURS) Simulator for Training in Endourology: The K-Box Model. Cent. European J. Urol. 2016, 69, 118–120. [Google Scholar] [CrossRef] [Green Version]
- Al-Jabir, A.; Aydin, A.; Abe, T.; Raison, N.; Khan, M.S.; Dasgupta, P.; Ahmed, K. Validation of the Advanced Scope Trainer for Flexible Ureterorenoscopy Training. J. Urol. 2017, 110, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Hong, D.; Kim, H.; Kim, T.; Kim, Y.-H.; Kim, N. Development of Patient Specific, Realistic, and Reusable Video Assisted Thoracoscopic Surgery Simulator Using 3D Printing and Pediatric Computed Tomography Images. Sci. Rep. 2021, 11, 6191. [Google Scholar] [CrossRef]
- Ock, J.; Gwon, E.; Kim, D.; Kim, S.; Kim, N. Patient-Specific and Hyper-Realistic Phantom for an Intubation Simulator with a Replaceable Difficult Airway of a Toddler Using 3D Printing. Sci. Rep. 2020, 10, 10631. [Google Scholar] [CrossRef]
- Adams, F.; Qiu, T.; Mark, A.; Fritz, B.; Kramer, L.; Schlager, D.; Wetterauer, U.; Miernik, A.; Fischer, P. Soft 3D-Printed Phantom of the Human Kidney with Collecting System. Ann. Biomed. Eng. 2017, 45, 963–972. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.; Adams, F.; Palagi, S.; Gengenbacher, A.; Schlager, D.; Müller, P.-F.; Gratzke, C.; Miernik, A.; Fischer, P.; Qiu, T. A High-Fidelity Phantom for the Simulation and Quantitative Evaluation of Transurethral Resection of the Prostate. Ann. Biomed. Eng. 2020, 48, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Li, D.; Jeong, M.; Yu, T.; Ma, Z.; Afat, S.; Grund, K.-E.; Qiu, T. Soft Liver Phantom with a Hollow Biliary System. Ann. Biomed. Eng. 2021, 49, 2139–2149. [Google Scholar] [CrossRef] [PubMed]
- Abou-Elela, A. Epidemiology, Pathophysiology, and Management of Uric Acid Urolithiasis: A Narrative Review. J. Adv. Res. 2017, 8, 513–527. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, N.D. Developmental Biology of the Human Kidney. Semin. Fetal Neonatal Med. 2008, 13, 125–132. [Google Scholar] [CrossRef]
- Ozimek, T.; Cordes, J.; Wiessmeyer, J.R.; Schneider, M.H.; Hupe, M.C.; Gilbert, N.; Merseburger, A.S.; Kramer, M.W. Steep Infundibulopelvic Angle as a New Risk Factor for Flexible Ureteroscope Damage and Complicated Postoperative Course. J. Endourol. 2018, 32, 597–602. [Google Scholar] [CrossRef]
- Karim, S.S.; Hanna, L.; Geraghty, R.; Somani, B.K. Role of Pelvicalyceal Anatomy in the Outcomes of Retrograde Intrarenal Surgery (RIRS) for Lower Pole Stones: Outcomes with a Systematic Review of Literature. Urolithiasis 2020, 48, 263–270. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Kareem, Z.; Tak, G.; Patil, A.; Ganpule, A.; Sabnis, R.; Desai, M. Validity of a Novel Chicken and Porcine Model for Laparoscopic Neobladder Reconstruction. J. Endourol. 2021, 35, 109–115. [Google Scholar] [CrossRef]
- Hamilton, E.C.; Scott, D.J.; Fleming, J.B.; Rege, R.V.; Laycock, R.; Bergen, P.C.; Tesfay, S.T.; Jones, D.B. Comparison of Video Trainer and Virtual Reality Training Systems on Acquisition of Laparoscopic Skills. Surg. Endosc. Other Interv. Tech. 2002, 16, 406–411. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.Y.; Tan, X.; Jeong, M.; Li, D.; Miernik, A.; Qiu, T. A High-Fidelity Artificial Urological System for the Quantitative Assessment of Endoscopic Skills. J. Funct. Biomater. 2022, 13, 301. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb13040301
Kim DY, Tan X, Jeong M, Li D, Miernik A, Qiu T. A High-Fidelity Artificial Urological System for the Quantitative Assessment of Endoscopic Skills. Journal of Functional Biomaterials. 2022; 13(4):301. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb13040301
Chicago/Turabian StyleKim, Do Yeon, Xiangzhou Tan, Moonkwang Jeong, Dandan Li, Arkadiusz Miernik, and Tian Qiu. 2022. "A High-Fidelity Artificial Urological System for the Quantitative Assessment of Endoscopic Skills" Journal of Functional Biomaterials 13, no. 4: 301. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb13040301