
Production of Feline Universal Erythrocytes with Methoxy Polyethylene Glycol
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Feline Blood Samples
2.3. PEGylation of Cell Surface
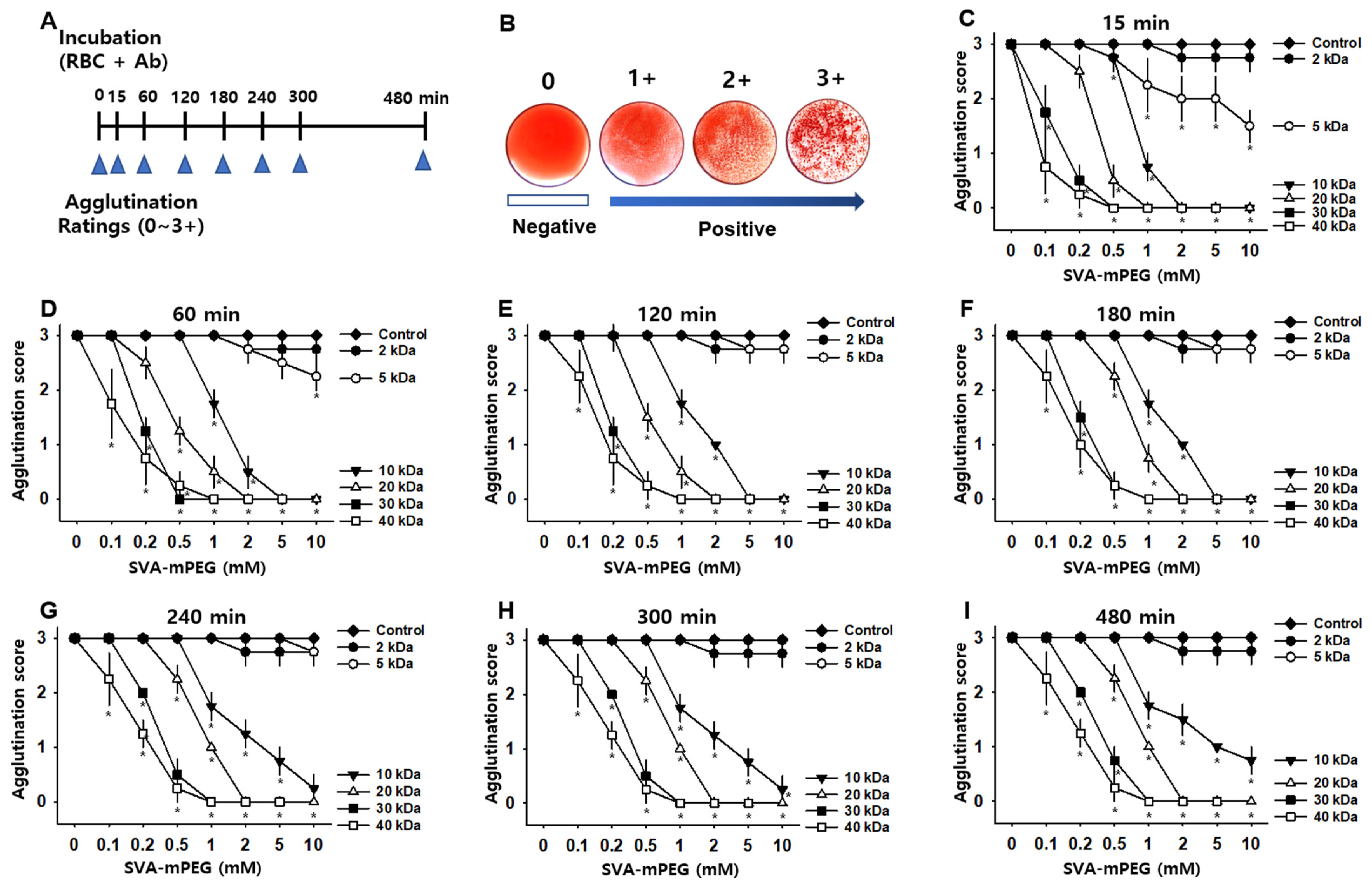
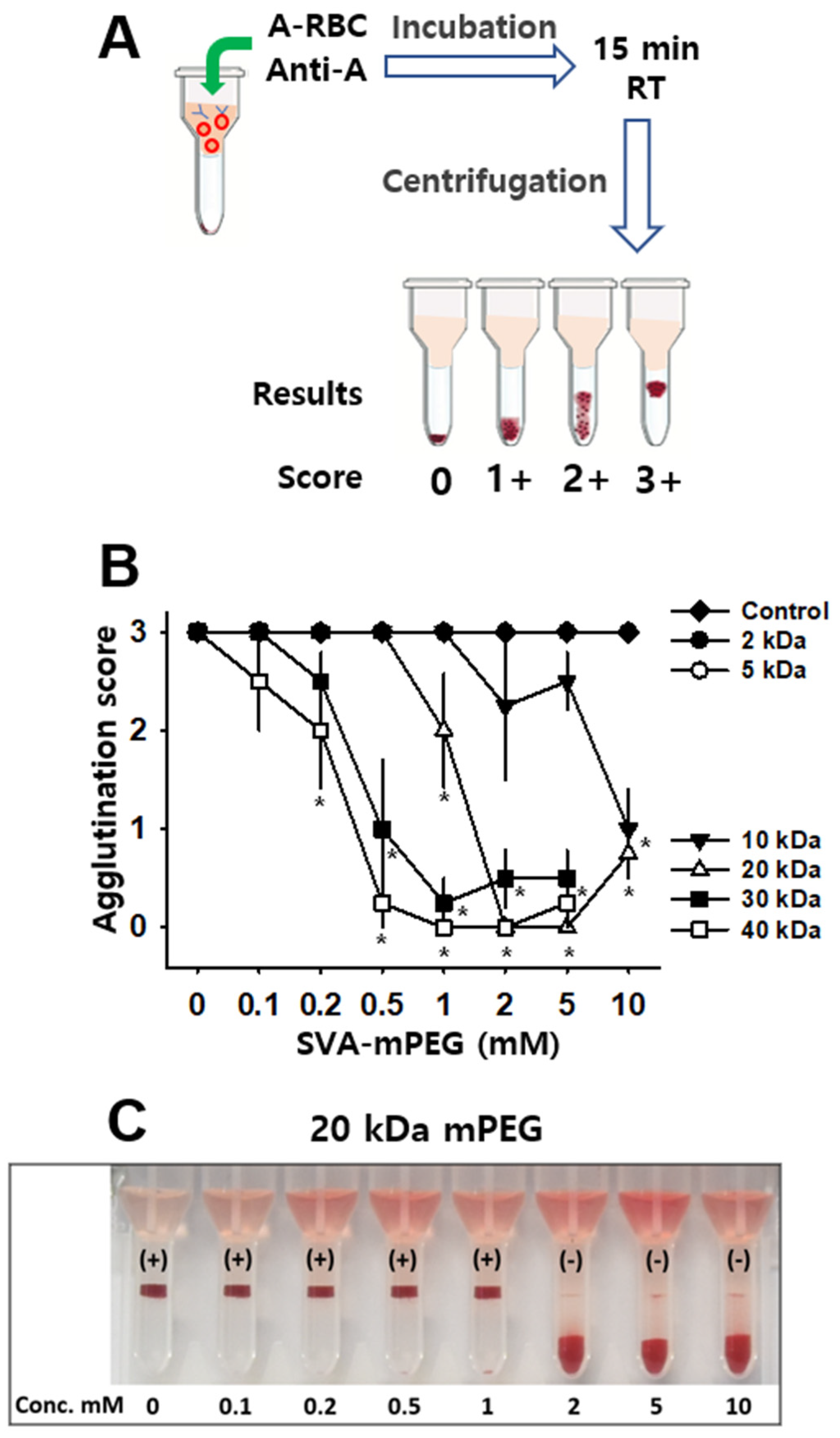
2.4. Agglutination Assay
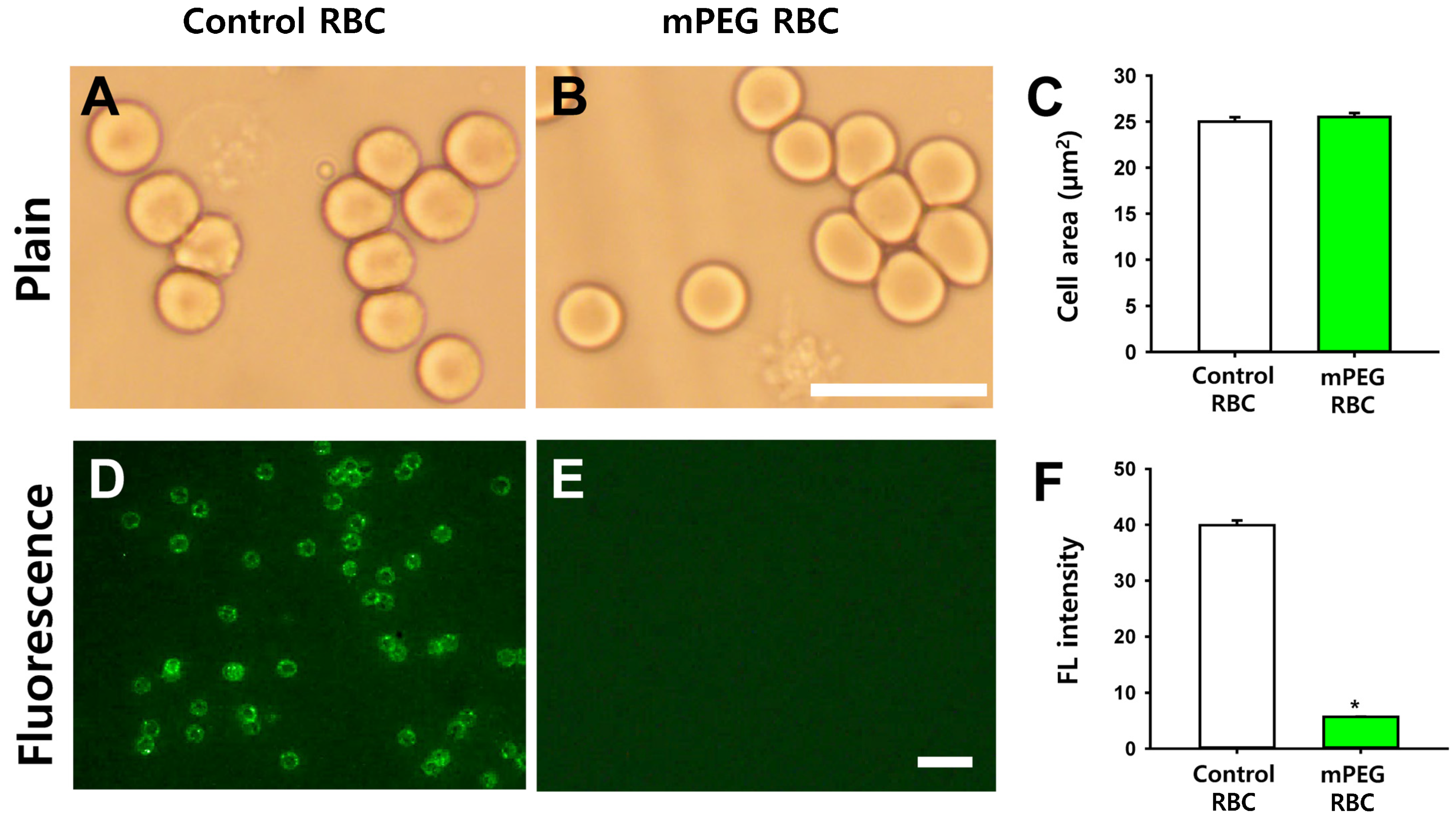
2.5. Morphology of mPEG-Treated RBCs and Immunofluorescence of mPEG-Treated RBCs Incubated with Feline Anti-A Alloantibodies
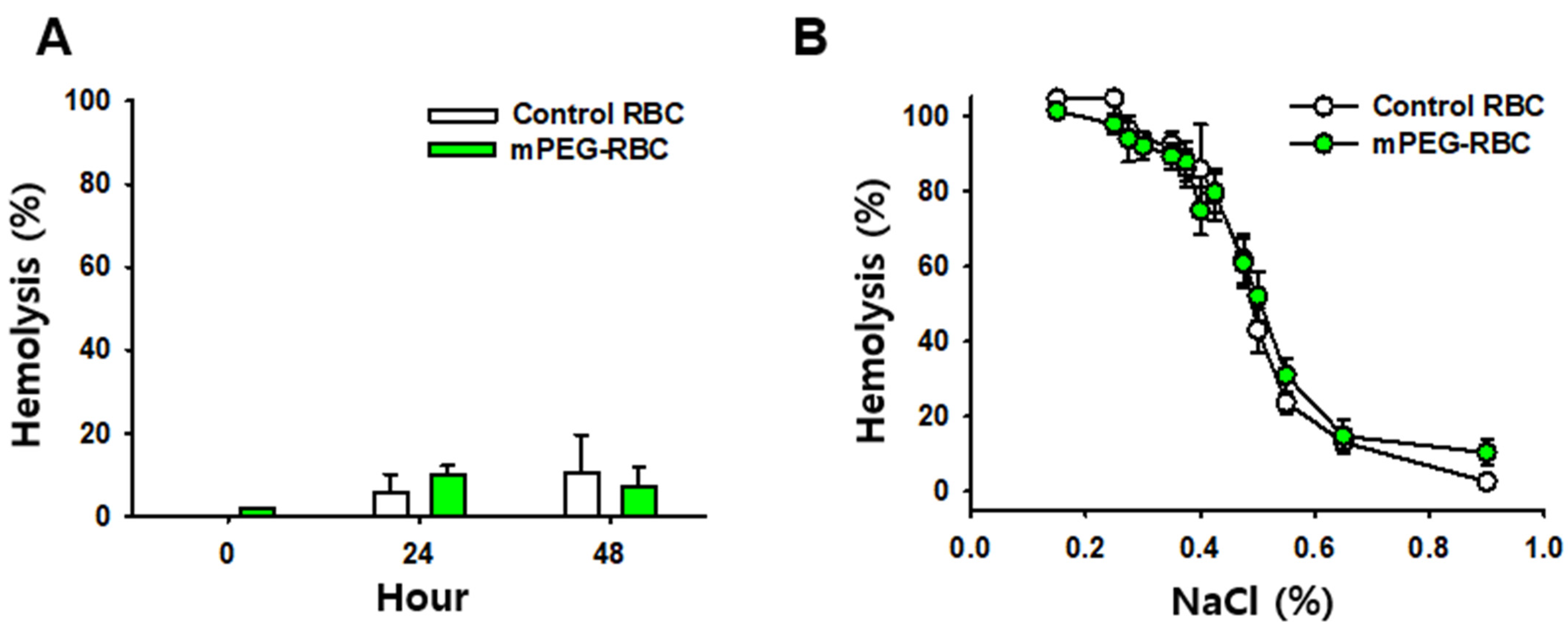
2.6. Measurement of Hemolysis
2.7. Osmotic Fragility Test
2.8. Monocyte Monolayer Assay (MMA)
2.9. Statistical Analysis
3. Results
3.1. Effect of mPEG on Antigenic Recognition
3.2. Morphology of mPEG-Treated RBCs and Inhibition of Antibody Binding by mPEG-Coated RBCs
3.3. Physiochemical Properties of mPEG-Treated RBCs
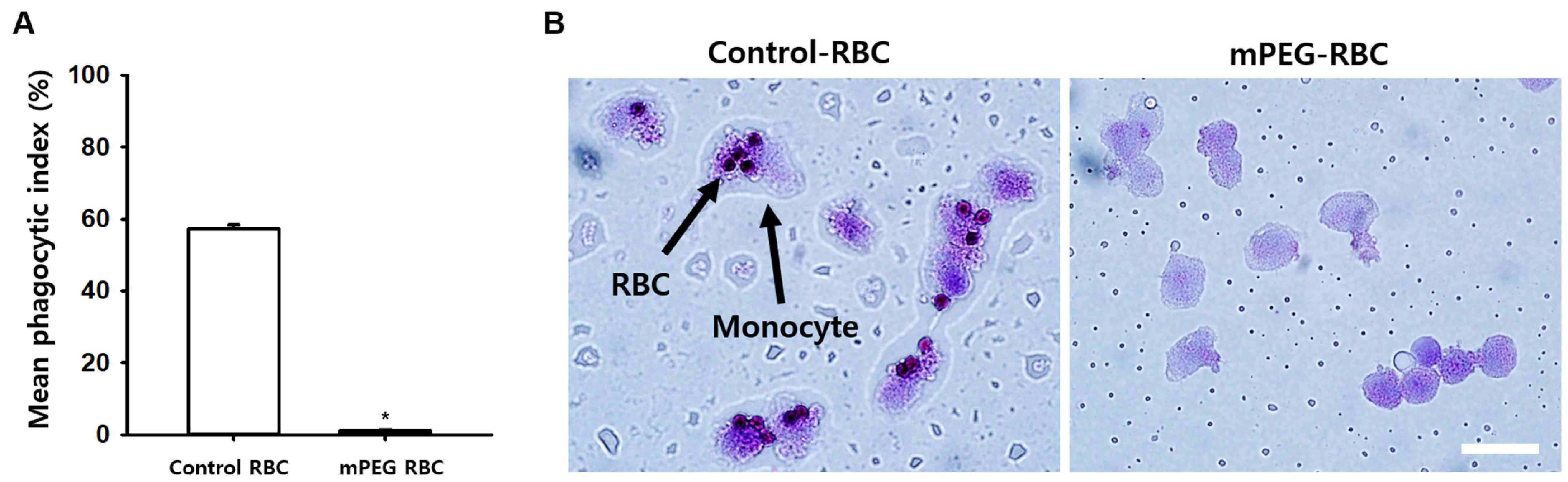
3.4. Effect of PEGylation of Antigen A on Opsonized Erythrocyte Phagocytosis
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Davidow, E.B.; Blois, S.L.; Goy-Thollot, I.; Harris, L.; Humm, K.; Musulin, S.; Nash, K.J.; Odunayo, A.; Sharp, C.R.; Spada, E.; et al. Association of Veterinary Hematology and Transfusion Medicine (AVHTM) Transfusion Reaction Small Animal Consensus Statement (TRACS). Part 1: Definitions and clinical signs. J. Vet. Emerg. Crit. Care (San. Antonio) 2021, 31, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Koenig, A.; Maglaras, C.H.; Giger, U. Acute hemolytic reaction due to A-B mismatched transfusion in a cat with transient AB blood type. J. Vet. Emerg. Crit. Care 2020, 30, 325–330. [Google Scholar] [CrossRef]
- Hale, A.S. Canine blood groups and their importance in veterinary transfusion medicine. Vet. Clin. N. Am. Small Anim. Pract. 1995, 25, 1323–1332. [Google Scholar] [CrossRef]
- Rozanski, E.; de Laforcade, A.M. Transfusion medicine in veterinary emergency and critical care medicine. Clin. Tech. Small Anim. Pract. 2004, 19, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Blais, M.C.; Berman, L.; Oakley, D.A.; Giger, U. Canine Dal blood type: A red cell antigen lacking in some Dalmatians. J. Vet. Intern. Med. 2007, 21, 281–286. [Google Scholar] [CrossRef]
- Ebelt, A.K.; Fuchs, S.; Weber, C.; Muller, E.; Giger, U. Survey of Blood Groups DEA 1, DEA 4, DEA 5, Dal, and Kai 1/Kai 2 in Different Canine Breeds From a Diagnostic Laboratory in Germany. Front. Vet. Sci. 2020, 7, 85. [Google Scholar] [CrossRef] [PubMed]
- Gavazza, A.; Rossi, G.; Antognoni, M.T.; Cerquetella, M.; Miglio, A.; Mangiaterra, S. Feline blood groups: A systematic review of phylogenetic and geographical origin. Animals 2021, 11, 3339. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, N.M.; Blais, M.C.; Harris, K.; Oakley, D.A.; Aronson, L.R.; Giger, U. A newly recognized blood group in domestic shorthair cats: The Mik red cell antigen. J. Vet. Intern. Med. 2007, 21, 287–292. [Google Scholar] [CrossRef]
- Knottenbelt, C.M. The feline AB blood group system and its importance in transfusion medicine. J. Feline Med. Surg. 2002, 4, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Garratty, G. Progress in modulating the RBC membrane to produce transfusable universal/stealth donor RBCs. Transfus. Med. Rev. 2004, 18, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.D.; Murad, K.L.; Koumpouras, F.; Talbot, M.; Eaton, J.W. Chemical camouflage of antigenic determinants: Stealth erythrocytes. Proc. Natl. Acad. Sci. USA 1997, 94, 7566–7571. [Google Scholar] [CrossRef]
- Scott, M.D.; Toyofuku, W.M.; Yang, X.; Raj, M.; Kang, N. Immunocamouflaged RBC for Alloimmunized Patient. In Transfusion Medicine and Scientific Development; IntechOpen: London, UK, 2017. [Google Scholar]
- Goldstein, J.; Lenny, L.; Davies, D.; Voak, D. Further evidence for the presence of A antigen on group B erythrocytes through the use of specific exoglycosidases. Vox Sang. 1989, 57, 142–146. [Google Scholar] [CrossRef]
- Taylor, J.; Hyare, J.; Stelfox, P.; Williams, M.; Lees, R.; Maley, M. Multi-centre evaluation of pre-transfusional routine tests using 8-column format gel cards (DG Gel(R)). Transfus. Med. 2011, 21, 90–98. [Google Scholar] [CrossRef]
- Spada, E.; Perego, R.; Baggiani, L.; Proverbio, D. Comparison of conventional tube and gel-based agglutination tests for AB system blood typing in cat. Front. Vet. Sci. 2020, 23, 2020. [Google Scholar] [CrossRef]
- Barshtein, G.; Gural, A.; Manny, N.; Zelig, O.; Yedgar, S.; Arbell, D. Storage-induced damage to red blood cell mechanical properties can be only partially reversed by rejuvenation. Transfus Med Hemother 2014, 41, 197–204. [Google Scholar] [CrossRef]
- Murad, K.L.; Mahany, K.L.; Brugnara, C.; Kuypers, F.A.; Eaton, J.W.; Scott, M.D. Structural and functional consequences of antigenic modulation of red blood cells with methoxypoly(ethylene glycol). Blood 1999, 93, 2121–2127. [Google Scholar] [CrossRef]
- Kyluik-Price, D.L.; Li, L.; Scott, M.D. Comparative efficacy of blood cell immunocamouflage by membrane grafting of methoxypoly(ethylene glycol) and polyethyloxazoline. Biomaterials 2014, 35, 412–422. [Google Scholar] [CrossRef]
- Rossi, N.A.; Constantinescu, I.; Kainthan, R.K.; Brooks, D.E.; Scott, M.D.; Kizhakkedathu, J.N. Red blood cell membrane grafting of multi-functional hyperbranched polyglycerols. Biomaterials 2010, 31, 4167–4178. [Google Scholar] [CrossRef]
- Le, Y.; Toyofuku, W.M.; Scott, M.D. Immunogenicity of murine mPEG-red blood cells and the risk of anti-PEG antibodies in human blood donors. Exp. Hematol. 2017, 47, 36–47.e2. [Google Scholar] [CrossRef]
- Scott, M.D.; Chen, A.M. Beyond the red cell: Pegylation of other blood cells and tissues. Transfus. Clin. Biol. 2004, 11, 40–46. [Google Scholar] [CrossRef]
- Fruijtier-Polloth, C. Safety assessment on polyethylene glycols (PEGs) and their derivatives as used in cosmetic products. Toxicology 2005, 214, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Noumsi, G.T.; Kwok, Y.Y.; Moulds, J.M.; Scott, M.D. Inhibition of phagocytic recognition of anti-D opsonized Rh D+ RBC by polymer-mediated immunocamouflage. Am. J. Hematol. 2015, 90, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Mosbah, I.B.; Franco-Gou, R.; Abdennebi, H.B.; Hernandez, R.; Escolar, G.; Saidane, D.; Rosello-Catafau, J.; Peralta, C. Effects of polyethylene glycol and hydroxyethyl starch in University of Wisconsin preservation solution on human red blood cell aggregation and viscosity. Transplant. Proc. 2006, 38, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Le, Y.; Scott, M.D. Immunocamouflage: The biophysical basis of immunoprotection by grafted methoxypoly(ethylene glycol) (mPEG). Acta Biomater. 2010, 6, 2631–2641. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.N.; Branch, D.R. Use of a Monocyte Monolayer Assay to Evaluate Fcgamma Receptor-mediated Phagocytosis. J. Vis. Exp. 2017, 2, 55039. [Google Scholar]
- Noumsi, G.T.; Billingsley, K.L.; Moulds, J.M. Successful transfusion of antigen positive blood to alloimmunised patients using a monocyte monolayer assay. Transfus. Med. 2015, 25, 92–100. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.K.; Ahn, D.B.; Jang, H.B.; Ma, J.; Xing, J.; Yoon, J.W.; Lee, K.H.; Lee, D.M.; Kim, C.H.; Kim, H.Y. Production of Feline Universal Erythrocytes with Methoxy Polyethylene Glycol. J. Funct. Biomater. 2023, 14, 476. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14090476
Kim HK, Ahn DB, Jang HB, Ma J, Xing J, Yoon JW, Lee KH, Lee DM, Kim CH, Kim HY. Production of Feline Universal Erythrocytes with Methoxy Polyethylene Glycol. Journal of Functional Biomaterials. 2023; 14(9):476. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14090476
Chicago/Turabian StyleKim, Hyung Kyu, Dan Bi Ahn, Han Byeol Jang, Jing Ma, Juping Xing, Joo Won Yoon, Kyung Hee Lee, Dong Min Lee, Chang Hyun Kim, and Hee Young Kim. 2023. "Production of Feline Universal Erythrocytes with Methoxy Polyethylene Glycol" Journal of Functional Biomaterials 14, no. 9: 476. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14090476