

Microbiological and Clinical Assessments of Suture Materials and Cyanoacrylate Application in Impacted Third Molar Surgeries: A Scoping Review

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Questions
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Research
2.5. Quality Assessment of Included Studies
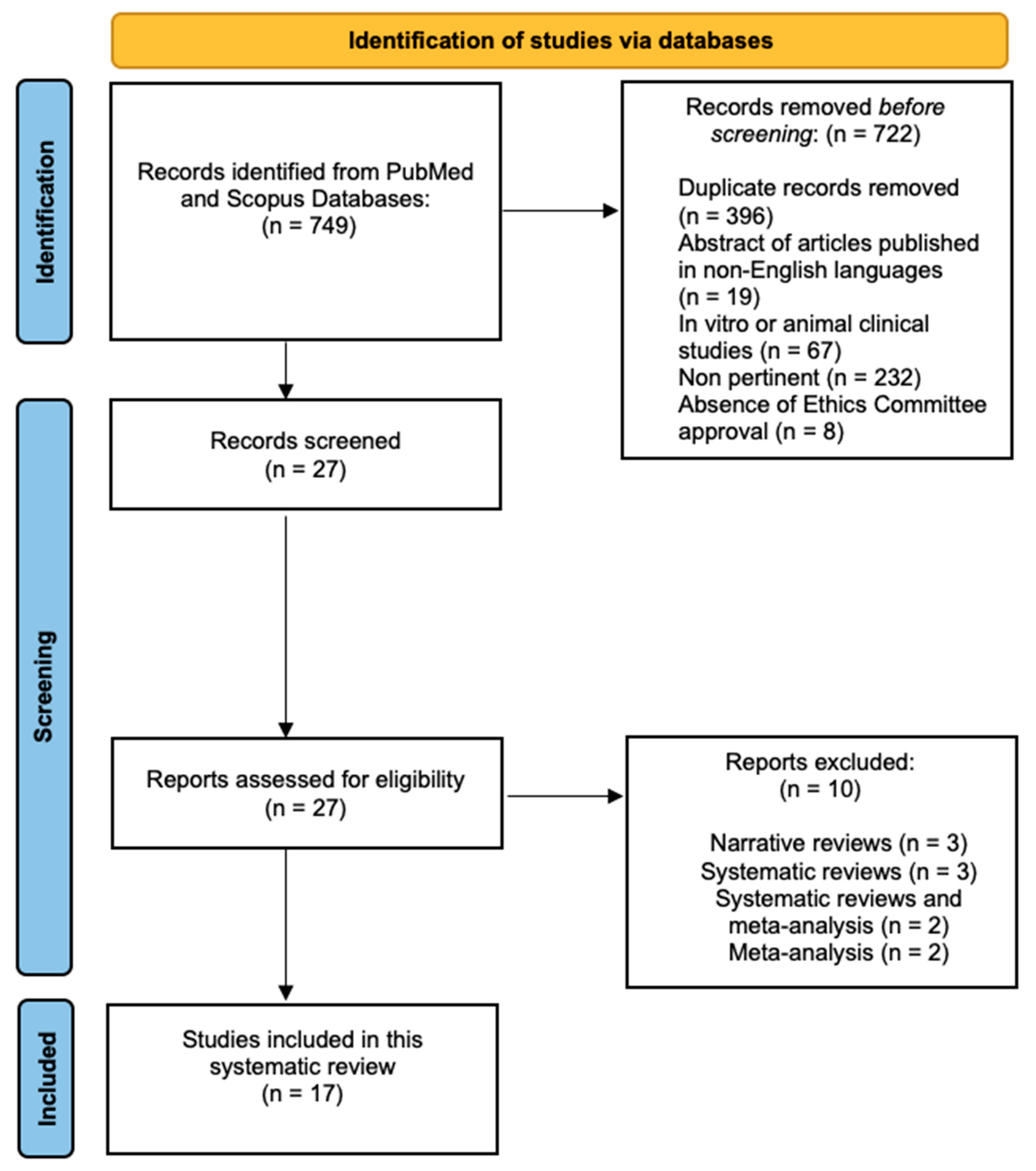
3. Results
Risk of Bias
4. Discussion
4.1. Microbiological Aspects
4.2. Clinical Evaluation
4.3. Cyanoacrylate versus Suture
4.4. Study Limitations and Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sifuentes-Cervantes, J.S.; Carrillo-Morales, F.; Castro-Núñez, J.; Cunningham, L.L.; Van Sickels, J.E. Third molar surgery: Past, present, and the future. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.J.; Silva, L.C.; Melo, M.R.; Santos, J.A.; Santos, T.S. Evaluation of the agreement by examiners according to classifications of third molars. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e281–e286. [Google Scholar] [CrossRef]
- Brown, L.H.; Berkman, S.; Cohen, D.; Kaplan, A.L.; Rosenberg, M. A radiological study of the frequency and distribution of impacted teeth. J. Dent. Assoc. S. Afr. 1982, 37, 627–630. [Google Scholar] [PubMed]
- Fanning, E.A.; Moorrees, C.F. A comparison of permanent mandibular molar formation in Australian Aborigines and Caucasoids. Arch. Oral Biol. 1969, 14, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Hugosan, A.; Kugelberg, C.F. The prevalence of third molars in a Swedish population. An epidemiological study. Community Dent. Health 1988, 5, 121–138. [Google Scholar]
- Hashemipour, M.A.; Tahmasbi-Arashlow, M.T.; Fahimi-Hanzaei, F.F. Incidence of impacted mandibular and maxillary third molars: A radiographic study in Southeast Iran population. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e140–e145. [Google Scholar] [CrossRef]
- Kaya, G.S.; Aslan, M.; Ömezil, M.M.; Dayi, E. Some morphological features related to mandibular third molar impaction. J. Clin. Exp. Dent. 2010, 2, 12–17. [Google Scholar] [CrossRef]
- Hattab, F.N.; Rawashdeh, M.A.; Fahmy, M.S. Impaction status of third molars in Jordanian students. Oral. Surg. Oral Med. Oral Pathol. Oral. Radiol. Endod. 1995, 79, 24–29. [Google Scholar] [CrossRef]
- Haidar, Z.; Shalhoub, S.Y. The incidence of impacted wisdom teeth in a Saudi community. Int. J. Oral Maxillofac. Surg. 1986, 15, 569–571. [Google Scholar] [CrossRef]
- Hassan, A.H. Pattern of third molar impaction in a Saudi population. Clin. Cosmet. Investig. Dent. 2010, 2, 109–113. [Google Scholar] [CrossRef]
- Chiapasco, M.; De Cicco, L.; Marrone, G. Side effects and complications associated with third molar surgery. Oral. Surg. Oral. Med. Oral Pathol. 1993, 76, 412–420. [Google Scholar] [CrossRef]
- Haug, R.H.; Perrott, D.H.; Gonzalez, M.L.; Talwar, R.M. The American Association of Oral and Maxillofacial Surgeons age-related third molar study. J. Oral Maxillofac. Surg. 2005, 63, 1106–1114. [Google Scholar] [CrossRef]
- Sayed, N.; Bakathir, A.; Pasha, M.; Al-Sudairy, S. Complications of Third Molar Extraction: A retrospective study from a tertiary healthcare centre in Oman. Sultan Qaboos Univ. Med. J. 2019, 19, e230–e235. [Google Scholar] [CrossRef]
- Cho, H.; Lynham, A.J.; Hsu, E. Postoperative interventions to reduce inflammatory complications after third molar surgery: Review of the current evidence. Aust. Dent. J. 2017, 62, 412–419. [Google Scholar] [CrossRef]
- Kumar, M.S.; Natta, S.; Shankar, G.; Reddy, S.H.; Visalakshi, D.; Seshiah, G.V. Comparison between Silk Sutures and Cyanoacrylate Adhesive in Human Mucosa—A Clinical and Histological Study. J. Int. Oral Health. 2013, 5, 95–100. [Google Scholar] [PubMed]
- Kundra, R.K.; Newman, S.; Saithna, A.; Lewis, A.C.; Srinivasan, S.; Srinivasan, K. Absorbable or non-absorbable sutures? A prospective, randomised evaluation of aesthetic outcomes in patients undergoing elective day-case hand and wrist surgery. Ann. R. Coll. Surg. Engl. 2010, 92, 665–667. [Google Scholar] [CrossRef] [PubMed]
- Pillai, C.K.; Sharma, C.P. Review paper: Absorbable polymeric surgical sutures: Chemistry, production, properties, biodegradability, and performance. J. Biomater. Appl. 2010, 25, 291–366. [Google Scholar] [CrossRef] [PubMed]
- Byrne, M.; Aly, A. The Surgical Suture. Aesthet. Surg. J. 2019, 39, S67–S72. [Google Scholar] [CrossRef]
- La Scala, G.; Lleo, M.M. Suture in odontoiatria. Fili tradizionali e in PTFE [Sutures in dentistry. Traditional and PTFE materials]. Dent. Cadmos. 1990, 58, 54–58. [Google Scholar]
- Nary Filho, H.; Matsumoto, M.A.; Batista, A.C.; Lopes, L.C.; de Góes, F.C.; Consolaro, A. Comparative study of tissue response to polyglecaprone 25, polyglactin 910 and polytetrafluorethylene suture materials in rats. Braz. Dent. J. 2002, 13, 86–91. [Google Scholar] [CrossRef]
- Parirokh, M.; Asgary, S.; Eghbal, M.J.; Stowe, S.; Kakoei, S. A scanning electron microscope study of plaque accumulation on silk and PVDF suture materials in oral mucosa. Int. Endod. J. 2004, 37, 776–781. [Google Scholar] [CrossRef]
- Otten, J.E.; Wiedmann-Al-Ahmad, M.; Jahnke, H.; Pelz, K. Bacterial colonization on different suture materials—A potential risk for intraoral dentoalveolar surgery. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 74, 627–635. [Google Scholar] [CrossRef]
- Moy, R.L.; Lee, A.; Zalka, A. Commonly used suture materials in skin surgery. Am. Fam. Physician 1991, 44, 2123–2128. [Google Scholar]
- Alexander, R.E. Dental extraction wound management: A case against medicating post-extraction sockets. J. Oral Maxillofac. Surg. 2000, 58, 538–551. [Google Scholar] [CrossRef]
- Lins, R.D.; Gomes, R.C.; Santos, K.S.; Silva, P.V.; Silva, R.T.; Ramos, I.A. Use of cyanoacrylate in the coaptation of edges of surgical wounds. An. Bras. Dermatol. 2012, 87, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis. 2020. Available online: https://synthesismanual.jbi.global (accessed on 16 September 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tool. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 16 September 2023).
- Santos, A.J.F.; Monteiro, J.L.G.C.; Moraes, S.L.D.; Vasconcelos, B.C.E.; Pellizzer, E.P. Clinical comparison of conventional suture and tissue adhesive in third molar surgeries: A systematic review. Gen. Dent. 2023, 75, 25–29. [Google Scholar]
- Stran-Lo Giudice, A.F.; Ortiz, A.M.; Sánchez-Labrador, L.; Cortés-Bretón Brinkmann, J.; Cobo-Vázquez, C.M.; Meniz-García, C. Current status of split-mouth controlled clinical trials comparing cyanoacrylate vs. conventional suture after lower third molar surgeries: A systematic literature review. Acta Odontol. Scand. 2023, 81, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Petronis, Ž.; Zigmantavičius, J.; Gervickas, A. Various wound closure ways after impacted lower wisdom teeth removal: A review. Stomatologija 2020, 22, 107–115. [Google Scholar]
- Ma, S.; Li, X.; Zhang, A.; Liu, S.; Zhao, H.; Zhao, H. Efficacy of secondary closure technique after extraction of third molars: A meta-analysis. Br. J. Oral Maxillofac. Surg. 2019, 57, 977–984. [Google Scholar] [CrossRef]
- Bailey, E.; Kashbour, W.; Shah, N.; Worthington, H.V.; Renton, T.F.; Coulthard, P. Surgical techniques for the removal of mandibular wisdom teeth. Cochrane Database Syst. Rev. 2020, 7, CD004345. [Google Scholar]
- Azab, M.; Ibrahim, S.; Li, A.; Khosravirad, A.; Carrasco-Labra, A.; Zeng, L.; Brignardello-Petersen, R. Efficacy of secondary vs primary closure techniques for the prevention of postoperative complications after impacted mandibular third molar extractions: A systematic review update and meta-analysis. J. Am. Dent. Assoc. 2022, 153, 943–956. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, X.; Zhou, Z.; Hao, Y.; Li, H.; Cheng, Y.; Ren, X.; Wang, X. Effects of Impacted Lower Third Molar Extraction on Periodontal Tissue of the Adjacent Second Molar. Ther. Clin. Risk Manag. 2021, 17, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Faris, A.; Khalid, L.; Hashim, M.; Yaghi, S.; Magde, T.; Bouresly, W.; Hamdoon, Z.; Uthman, A.T.; Marei, H.; Al-Rawi, N. Characteristics of Suture Materials Used in Oral Surgery: Systematic Review. Int. Dent. J. 2022, 72, 278–287. [Google Scholar] [CrossRef]
- Raut, V.D.; Kumar, S.; Raut, S.; Bhate, K.; Singh, M.; Kakodkar, P.; Waknis, P. Dehiscence rate in wound closed with cyanoacrylate and black braided silk after surgical removal of impacted third molar: A systematic review and meta-analysis. Oral Surg. 2022, 15, 17–23. [Google Scholar] [CrossRef]
- Borie, E.; Rosas, E.; Kuramochi, G.; Etcheberry, S.; Olate, S.; Weber, B. Oral Applications of Cyanoacrylate Adhesives: A Literature Review. BioMed Res. Int. 2019, 2019, 8217602. [Google Scholar] [CrossRef]
- Etemadi Sh, M.; Rahgozar, S.; Tajmiri, G.; Alizargar, J.; Wu, S.V. Microbiological Evaluation of the Antibacterial Vicryl Suture in the Mandibular Third Molar Surgery. J. Orofac. Sci. 2023, 14, 120–127. [Google Scholar]
- Dragovic, M.; Pejovic, M.; Stepic, J.; Colic, S.; Dozic, B.; Dragovic, S.; Lazarevic, M.; Nikolic, N.; Milasin, J.; Milicic, B. Comparison of four different suture materials in respect to oral wound healing, microbial colonization, tissue reaction and clinical features-randomized clinical study. Clin. Oral Investig. 2020, 24, 1527–1541. [Google Scholar] [CrossRef]
- Banche, G.; Roana, J.; Mandras, N.; Amasio, M.; Gallesio, C.; Allizond, V.; Angeretti, A.; Tullio, V.; Cuffini, A.M. Microbial adherence on various intraoral suture materials in patients undergoing dental surgery. J. Oral Maxillofac. Surg. 2007, 65, 1503–1507. [Google Scholar] [CrossRef]
- Dragović, M.; Pejovic, M.; Stepic, J.; Dragovic, S.; Nikolic, N.; Kuzmanovic Pficer, J.; Colic, S.; Milasin, J. Microbial adherence affinity and clinical characteristics of polypropylene versus silk sutures in oral surgery. Srp. Arh. Za Celok. Lek. 2018, 146, 258–263. [Google Scholar] [CrossRef]
- Sala-Pérez, S.; López-Ramírez, M.; Quinteros-Borgarello, M.; Valmaseda-Castellón, E.; Gay-Escoda, C. Antibacterial suture vs silk for the surgical removal of impacted lower third molars. A randomized clinical study. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e95–e102. [Google Scholar] [CrossRef]
- Balakrishna, R.; Poojary, D.R.A.; Sali, S.; Moharana, A.K.; Deepak, T.S. Single blind, randomized study comparing clinical equivalence of Trusilk® and Mersilk® silk sutures for mucosal closure following surgical removal of mesioangular impacted mandibular third molar. F1000Research 2022, 11, 689. [Google Scholar] [CrossRef]
- Oladega, A.A.; James, O.; Adeyemo, W.L. Cyanoacrylate tissue adhesive or silk suture for closure of surgical wound following removal of an impacted mandibular third molar: A randomized controlled study. J. Cranio-Maxillofac. Surg. 2019, 47, 93–98. [Google Scholar] [CrossRef]
- Bucci, M.; Borgonovo, A.; Bianchi, A.; Zanellato, A.; Re, D. Microbiological analysis of bacterial plaque on three different threads in oral surgery. Minerva Stomatol. 2017, 66, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Gazivoda, D.; Pelemiš, D.; Vujašković, G. A clinical study on the influence of suturing material on oral wound healing. Vojnosanit. Pregl. 2015, 72, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Thoniyottupurayil, N.; Rao, H.T.; Sequeira, J. Tissue Adhesive or Suture for Wound Closure Following Surgical Removal of an Impacted Mandibular Third Molar: A Randomized Comparative Study. World J. Dent. 2022, 13, 587–593. [Google Scholar] [CrossRef]
- Pelia, A.K.; Kaur, T.; Kapila, S.; Dhawan, A.; Singh Bhullar, R. Efficacy of Isoamyl 2-Cyanoacrylate Tissue Adhesive and 3-0 Vicryl Rapide Sutures in Impacted Mandibular Third Molar Surgery: A Comparative Study. AMEI’s Curr. Trends Diagn. Treat. 2021, 5, 80–84. [Google Scholar]
- Joshi, A.D.; Saluja, H.; Mahindra, U.; Halli, R. A comparative study: Efficacy of tissue glue and sutures after impacted mandibular third molar removal. J. Maxillofac. Oral Surg. 2011, 10, 310–315. [Google Scholar] [CrossRef] [PubMed]
- El-Rewainy, M.A.; Osman, S.M.; Hassan, N.E. The use of n-butyl cyanoacrylate adhesive in the closure of mucoperiosteal flap after the surgical extraction of impacted mandibular third molar. Alex. Dent. J. 2015, 40, 152–159. [Google Scholar] [CrossRef]
- Ghoreishian, M.; Gheisari, R.; Fayazi, M. Tissue adhesive and suturing for closure of the surgical wound after removal of impacted mandibular third molars: A comparative study. Oral. Surg. Oral. Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, e14–e16. [Google Scholar] [CrossRef]
- Parrini, S.; Bovicelli, A.; Chisci, G. Microbiological Retention on PTFE versus Silk Suture: A Quantitative Pilot Study in Third Molar Surgery. Antibiotics 2023, 12, 562. [Google Scholar] [CrossRef]
- Yaman, D.; Paksoy, T.; Ustaoğlu, G.; Demirci, M. Evaluation of Bacterial Colonization and Clinical Properties of Different Suture Materials in Dentoalveolar Surgery. J. Oral Maxillofac. Surg. 2022, 80, 313–326. [Google Scholar] [CrossRef]
- Mahat, A.K.; Yadav, R.; Yadav, A.K.; Acharya, P.; Dongol, A.; Sagtani, A.; Jaisani, M.R. A Comparative Study of the Effect of Sutureless Versus Multiple Sutures Technique on Complications following Third Molar Surgery in Nepalese Subpopulation. Int. J. Dent. 2020, 2020, 9314762. [Google Scholar] [CrossRef]
- Alkadi, S.; Stassen, L. Effect of One-Suture and Sutureless Techniques on Postoperative Healing After Third Molar Surgery. J. Oral Maxillofac. Surg. 2019, 77, 703.e1–703.e16. [Google Scholar] [CrossRef] [PubMed]
- Leknes, K.N.; Selvig, K.A.; Bøe, O.E.; Wikesjö, U.M. Tissue reactions to sutures in the presence and absence of anti-infective therapy. J. Clin. Periodontol. 2005, 32, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Chisci, G.; Capuano, A.; Parrini, S. Alveolar Osteitis and Third Molar Pathologies. J. Oral Maxillofac. Surg. 2018, 76, 235–236. [Google Scholar] [CrossRef] [PubMed]
- Charbit, Y.; Hitzig, C.; Bolla, M.; Bitton, C.; Bertrand, M.F. Comparative study of physical properties of three suture materials: Silk, e-PTFE (Gore-Tex), and PLA/PGA (Vicryl). Biomed. Instrum. Technol. 1999, 33, 71–75. [Google Scholar]
- Fowler, J.R.; Perkins, T.A.; Buttaro, B.A.; Truant, A.L. Bacteria adhere less to barbed monofilament than braided sutures in a contaminated wound model. Clin. Orthop. Relat. Res. 2013, 471, 665–671. [Google Scholar] [CrossRef]
- Rothenburger, S.; Spangler, D.; Bhende, S.; Burkley, D. In Vitro Antimicrobial Evaluation of Coated VICRYL* Plus Antibacterial Suture (Coated Polyglactin 910 with Triclosan) using Zone of Inhibition Assays. Surg. Infect. 2002, 3, S79–S87. [Google Scholar] [CrossRef]
- Asher, R.; Chacartchi, T.; Tandlich, M.; Shapira, L.; Polak, D. Microbial accumulation on different suture materials following oral surgery: A randomized controlled study. Clin. Oral Investig. 2019, 23, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, F.; Potenza, C.; Puddu, P.; Sera, F.; Masini, C.; Abeni, D. Suture materials and other factors associated with tissue reactivity, infection, and wound dehiscence among plastic surgery outpatients. Plast. Reconstr. Surg. 2001, 107, 38–45. [Google Scholar] [CrossRef]
- Kakoei, S.; Baghaei, F.; Dabiri, S.; Parirokh, M.; Kakooei, S. A comparative in vivo study of tissue reactions to four suturing materials. Iran. Endod. J. 2010, 5, 69–73. [Google Scholar]
- Soufdoost, R.S.; Mosaddad, S.A.; Salari, Y.; Yazdanian, M.; Tebyanian, H.; Tahmasebi, E.; Yazdanian, A.; Karami, A.; Barkhordari, A. Surgical Suture Assembled with Tadalafil/Polycaprolactone Drug-Delivery for Vascular Stimulation Around Wound: Validated in a Preclinical Model. Biointerface Res. Appl. Chem. 2020, 10, 6317–6327. [Google Scholar]
- Javed, F.; Al-Askar, M.; Almas, K.; Romanos, G.E.; Al-Hezaimi, K. Tissue reactions to various suture materials used in oral surgical interventions. ISRN Dent. 2012, 2012, 762095. [Google Scholar] [CrossRef] [PubMed]
- Ayyıldız, S.N.; Ayyıldız, A. Cyanoacrylic tissue glues: Biochemical properties and their usage in urology. Turk. J. Urol. 2017, 43, 14–24. [Google Scholar] [CrossRef]
- Xu, J.; Chen, C.; Gan, S.; Liao, Y.; Fu, R.; Hou, C.; Yang, S.; Zheng, Z.; Chen, W. The Potential Value of Probiotics after Dental Implant Placement. Microorganisms 2023, 11, 1845. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Gallo, S.; Zampetti, P.; Cuggia, G.; Scribante, A. Domiciliary Use of Chlorhexidine vs. Postbiotic Gels in Patients with Peri-Implant Mucositis: A Split-Mouth Randomized Clinical Trial. Appl. Sci. 2022, 12, 2800. [Google Scholar] [CrossRef]
- Deng, X.; Gould, M.; Azam Ali, M. A review of current advancements for wound healing: Biomaterial applications and medical devices. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 2542–2573. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| References (Authors, Year of Publication) | Random Sequence Generation | Allocation Concealment | Blinding | Incomplete Outcome Data | Selective Reporting |
|---|---|---|---|---|---|
| Etemadi et al., 2022 [39] |  | | | | |
| Dragovic et al., 2020 [40] | |  | | | |
| Banche et al., 2007 [41] | | | | | |
| Dragovic et al., 2018 [42] | | | | | |
| Sala-Perez et al., 2016 [43] | | | | | |
| Balakrishna et al., 2022 [44] | | | | | |
| Oladega et al., 2019 [45] | | | | | |
| Bucci et al., 2017 [46] | | | | | |
| Gazivoda et al., 2015 [47] | | | | | |
| Thoniyottupurayil et al., 2022 [48] | | | | | |
| Pelia et al., 2021 [49] | | | | | |
| Joshi et al., 2011 [50] | | | | | |
| El-rewainy et al., 2015 [51] | | | | | |
| Ghoreishian et al., 2009 [52] | | | | | |
| Parrini et al., 2023 [53] | | | | | |
| Yaman et al., 2022 [54] | | | | | |
| Otten et al., 2005 [22] | | | | | |
| References (Authors, Year of Publication, Origin of the Research, and Study Design) | N° of Patients and % Women Mean Age (Years), Mean (SD or Range) | Inclusion and Exclusion Criteria | Suture Materials |
|---|---|---|---|
| Etemadi et al., 2022 Iran RCT [39] | 27 W: 77.78% 23.7 ± 3.1 | Exclusion criteria: Systemic illnesses treated with systemic or oral medications that can disrupt the usual oral microbiota and colonization, tobacco and substance dependency, alcohol dependency, preexisting intraoral inflammation prior to the surgical procedure, pregnancy, breastfeeding, documented or suspected allergies to suture materials or other study-related materials, suture loss occurring within the first week, the presence of removable oral prosthetics, and instances of post-surgery infection or other scenarios warranting antibiotic treatment. |
|
| Dragovic et al., 2020 Serbia RCT [40] | 32 W: 65.62% 18–25 | Exclusion criteria: N.R. |
|
| Banche et al., 2007 Italy RCT [41] | 60 W: N.R. N.R. | Exclusion criteria: N.R. |
|
| Dragovic et al., 2018 Serbia RCT [42] | 10 W: 100% 21–27 | Exclusion criteria: N.R. |
|
| Sala-Perez et al., 2016 Spain RCT [43] | 20 W: 50% 18–35 23.6 ± 4.77 | Exclusion criteria: Individuals with systemic conditions (such as immune suppression, current infections, diabetes mellitus, or hematinic disorders), pregnant individuals, substance abusers, and patients exhibiting a considerable alcohol consumption. |
|
| Balakrishna et al., 2022 India RCT [44] | Group 1: 65 W: 66.15% Group 2: 64 W: 64.06% Group 1: 27.96 ± 5.75 Group 2: 27.87 ± 6.14 | Exclusion criteria: individuals with pericoronitis or complicated impacted third molars, pregnant or lactating females, noncompliant patients. Silk-allergic subjects, patients with a medical history including systemic diseases such as diabetes mellitus, tuberculosis, hemostatic disorders, osteoporosis, or unstable/life-threatening conditions, or those currently undergoing radiation therapy were excluded. Participants taking any form of local or systemic medications, including aspirin, or undergoing anticoagulant therapy within 30 days before surgery, or with a history of substance abuse, were also excluded. Furthermore, individuals already enrolled in another research study or actively engaged in investigations conducted by the same investigator or center. |
|
| Oladega et al., 2019 Nigeria RCT [45] | 120 W: 62.5% 27.3 ± 6.9 | Exclusion criteria: N.R. |
|
| Bucci et al., 2017 Italy RCT [46] | 30 W: N.R. 16–63 | Exclusion criteria: N.R. |
|
| Gazivoda et al., 2015 Serbia RCT [47] | 96 W: N.R. N.R. | Exclusion criteria: N.R. |
|
| Thoniyottupurayil et al., 2022 India RCT [48] | 14 W: N.R. 18–35 | Exclusion criteria: Individuals who were either pregnant or breastfeeding, those displaying symptoms of pericoronitis or active infections, individuals with harmful behaviors such as smoking and excessive alcohol consumption, and individuals with inadequate oral hygiene. |
|
| Pelia et al., 2021 India Controlled study [49] | 60 W: 55% 18–40 | Exclusion criteria: Patients affected by systemic diseases, smokers. |
|
| Joshi et al., 2011 India Controlled study [50] | 30 W: 63.33% 20–32 | Exclusion criteria: N.R. |
|
| El-rewainy et al., 2015 Egypt Controlled study [51] | 20 W: 40% 18–30 24 | Exclusion criteria: Individuals affected by systemic diseases, pregnant or breastfeeding. Patients with signs of pericoronitis or active infection. Smoking or addicted subjects and oral respirators. |
|
| Ghoreishian et al., 2009 Iran Controlled study [52] | 16 W: 56.25% 18–24 | Exclusion criteria: N.R. |
|
| Parrini et al., 2023 Italy Prospective study [53] | 10 W: 30% 25–40 31 | Exclusion criteria: Smoking and diabetes mellitus. |
|
| Yaman et al., 2022 Turkey Prospective study [54] | 43 W: 74.41% N.R. | Exclusion criteria: Pregnant or lactating females; patients taking anticoagulant medications, patients affected by systemic viral, bacterial, or fungal infections; and smokers. |
|
| Otten et al., 2005 Germany Prospective study [22] | 11 W: N.R. N.R. | Exclusion criteria: N.R. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scribante, A.; Ghizzoni, M.; Pellegrini, M.; Poli, P.P.; Maiorana, C.; Spadari, F. Microbiological and Clinical Assessments of Suture Materials and Cyanoacrylate Application in Impacted Third Molar Surgeries: A Scoping Review. J. Funct. Biomater. 2023, 14, 529. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14100529
Scribante A, Ghizzoni M, Pellegrini M, Poli PP, Maiorana C, Spadari F. Microbiological and Clinical Assessments of Suture Materials and Cyanoacrylate Application in Impacted Third Molar Surgeries: A Scoping Review. Journal of Functional Biomaterials. 2023; 14(10):529. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14100529
Chicago/Turabian StyleScribante, Andrea, Martina Ghizzoni, Matteo Pellegrini, Pier Paolo Poli, Carlo Maiorana, and Francesco Spadari. 2023. "Microbiological and Clinical Assessments of Suture Materials and Cyanoacrylate Application in Impacted Third Molar Surgeries: A Scoping Review" Journal of Functional Biomaterials 14, no. 10: 529. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14100529