

Existing and Emerging Approaches to Risk Assessment in Patients with Ascending Thoracic Aortic Dilatation

 ,
,  , ,
, ,  ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Assessment of Aortic Dimensions for Risk Stratification
2.1. Aortic Diameter
2.2. Aortic Size Indexes
2.3. Aortic Length
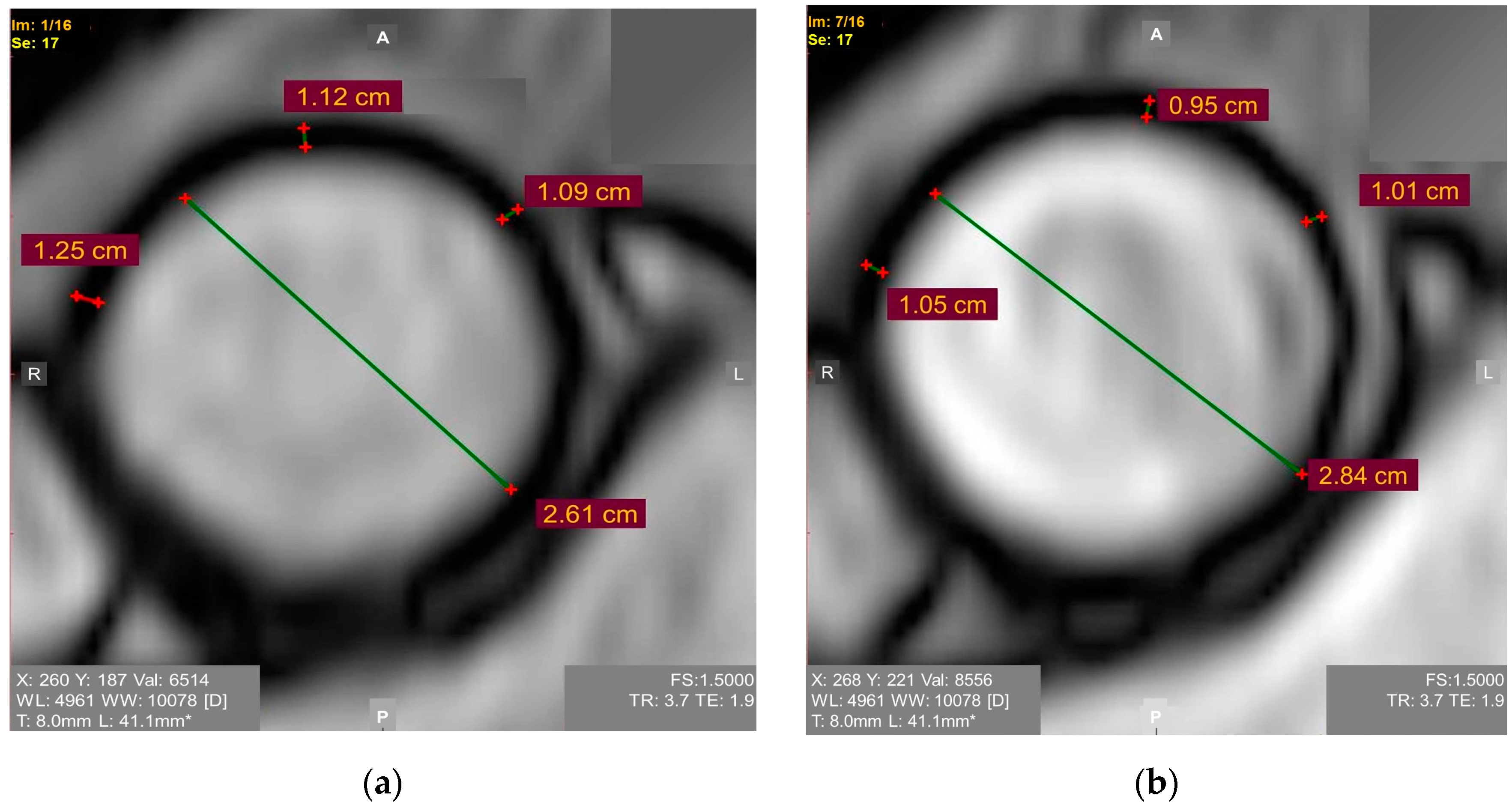
2.4. Measurements of Aortic Dimensions
3. Central Hemodynamic Measurements
4. Biomechanical Properties of Ascending Aorta
4.1. In Vivo Evaluation of Elastic/Biomechanical Properties of Ascending Aorta
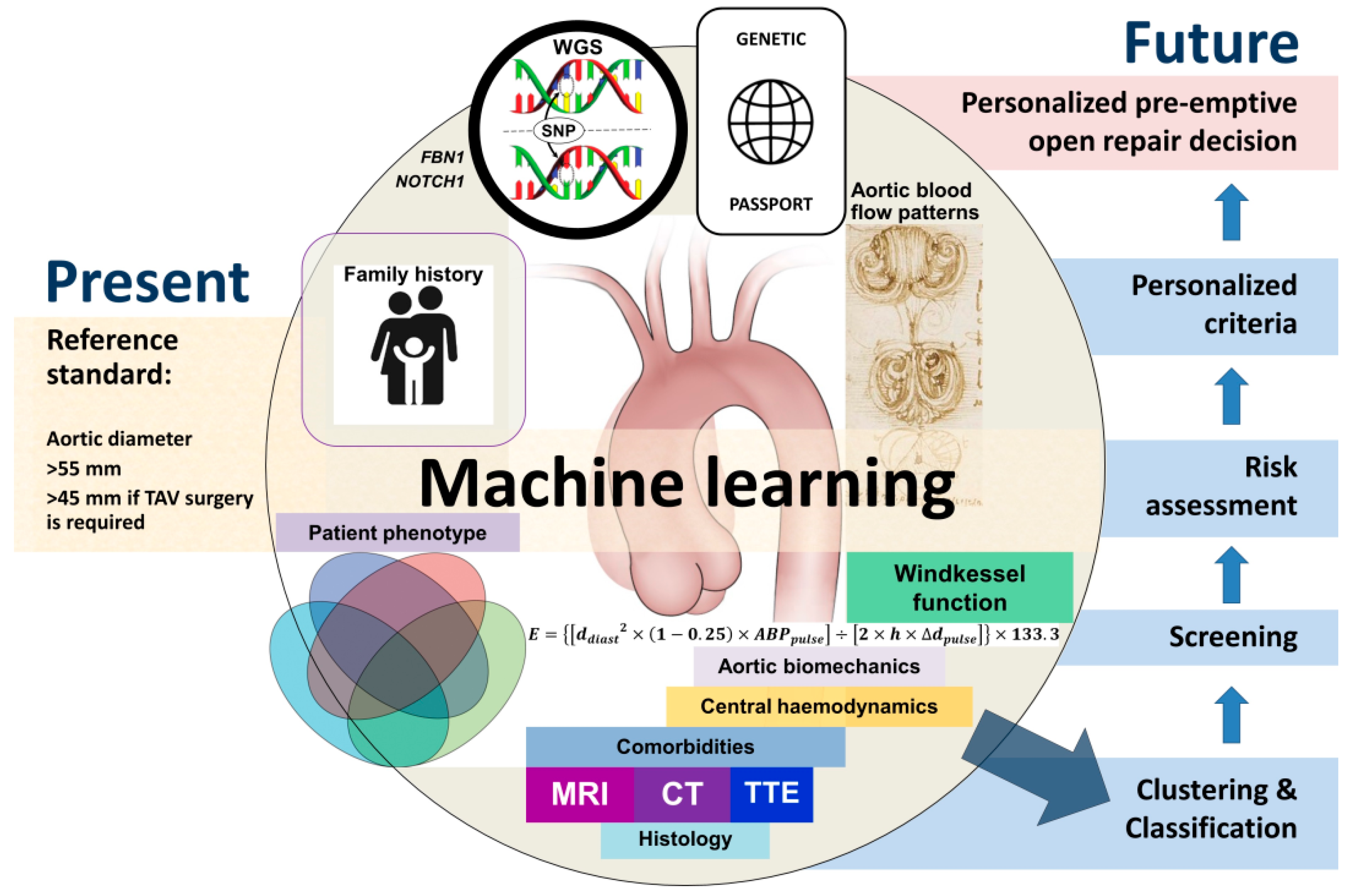
4.2. Young’s Elastic Modulus
- E—Young’s elastic modulus (Pa);
- ddiast—diastolic aortic diameter;
- ∆dpulse—an increase in aortic diameter during systole;
- 0.25—squared Poisson ratio for the aorta wall (Poisson ratio is known to be 0.5);
- h—aorta wall thickness during diastole;
- ABPpulse—pulse arterial blood pressure;
- 133.3—mmHg to Pa conversion factor.

4.3. Windkessel Function
4.4. Fluid Hemodynamics and Vortical Patterns in Proximal Aorta for Risk Assessment
5. Phenotype
5.1. BAV
5.2. Aortic Arch Variants
5.3. Thumb Palm Test
5.4. Paradoxes
6. Risk Associated with COVID-19 Infection
7. Machine Learning
8. Comments
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zafar, M.A.; Chen, J.F.; Wu, J.; Li, Y.; Papanikolaou, D.; Abdelbaky, M.; Faggion Vinholo, T.; Rizzo, J.A.; Ziganshin, B.A.; Mukherjee, S.K.; et al. Natural history of descending thoracic and thoracoabdominal aortic aneurysms. J. Thorac. Cardiovasc. Surg. 2021, 161, 498–511.e1. [Google Scholar] [CrossRef]
- Zafar, M.A.; Farkas, E.A.; Javier, A.; Anderson, M.; Gilani, O.; Elefteriades, J.A. Are thromboembolic and bleeding complica-tions a drawback for composite aortic root replacement? Ann. Thorac. Surg. 2012, 94, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Bin Mahmood, S.U.; Yousef, S.; Shioda, K.; Faggion Vinholo, T.; Mangi, A.A.; Elefteriades, J.A.; Geirsson, A. Prevalence of incidentally identified thoracic aortic dilations: Insights for screening criteria. Can. J. Cardiol. 2019, 35, 892–898. [Google Scholar] [CrossRef] [PubMed]
- McClure, R.S.; Brogly, S.B.; Lajkosz, K.; Payne, D.; Hall, S.F.; Johnson, A.P. Epidemiology and management of thoracic aortic dissections and thoracic aortic aneurysms in Ontario, Canada: A population-based study. J. Thorac. Cardiovasc. Surg. 2018, 155, 2254–2264.e4. [Google Scholar] [CrossRef] [PubMed]
- Saeyeldin, A.A.; Velasquez, C.A.; Mahmood, S.U.B.; Brownstein, A.J.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. Thoracic aortic an-eurysm: Unlocking the “silent killer” secrets. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Borger, M.A.; Fedak, P.W.M.; Stephens, E.H.; Gleason, T.G.; Girdauskas, E.; Ikonomidis, J.S.; Khoynezhad, A.; Siu, S.C.; Verma, S.; Hope, M.D.; et al. The American Association for Thoracic Surgery consensus guidelines on bicuspid aortic valve-related aortopathy: Full online-only version. J. Thorac. Car-Diovasc. Surg. 2018, 156, e41–e74. [Google Scholar] [CrossRef] [PubMed]
- Mansour, A.M.; Peterss, S.; Zafar, M.A.; Rizzo, J.A.; Fang, H.; Charilaou, P.; Ziganshin, B.A.; Darr, U.M.; Elefteriades, J.A. Prevention of Aortic Dissection Suggests a Diameter Shift to a Lower Aortic Size Threshold for Intervention. Cardiology 2018, 139, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, P.; Gunga, Z.; Niclauss, L.; Delay, D.; Roumy, A.; Pfister, R.; Colombier, S.; Patella, F.; Qanadli, S.D.; Kirsch, M. Type A aortic dissection in aneurysms having modelled pre-dissection maximum diameter below 45 mm: Should we implement current guidelines to improve the survival benefit of prophylactic surgery? Eur. J. Cardiothorac. Surg. 2021, 59, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Ziganshin, B.A.; Zafar, M.A.; Elefteriades, J.A. Descending threshold for ascending aortic aneurysmectomy: Is it time for a “left-shift” in guidelines? J. Thorac. Cardiovasc. Surg. 2019, 157, 37–42. [Google Scholar] [CrossRef]
- Monaghan, K.; Orelaru, F.; Naeem, A.; Ahmad, R.A.; Wu, X.; Kim, K.M.; Fukuhara, S.; Patel, H.J.; Deeb, G.M.; Yang, B. Should We Operate on Thoracic Aortic Aneurysm of 5-5.5cm in Bicuspid Aortic Valve Disease Patients? Cardiol. Cardiovasc. Med. 2021, 5, 651–662. [Google Scholar] [CrossRef]
- Zafar, M.A.; Li, Y.; Rizzo, J.A.; Charilaou, P.; Saeyeldin, A.; Velasquez, C.A.; Mansour, A.M.; Bin Mahmood, S.U.; Ma, W.G.; Brownstein, A.J.; et al. Height alone, rather than body surface area, suffices for risk estimation in ascending aortic aneurysm. J. Thorac. Cardiovasc. Surg. 2018, 155, 1938–1950. [Google Scholar] [CrossRef]
- Davies, R.R.; Gallo, A.; Coady, M.A.; Tellides, G.; Botta, D.M.; Burke, B.; Coe, M.P.; Kopf, G.S.; Elefteriades, J.A. Novel measurement of relative aortic size predicts rupture of thoracic aortic aneurysms. Ann. Thorac. Surg. 2006, 81, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, K.K.; Bevilacqua, S.; Aquaro, G.D.; Festa, P.; Ait-Ali, L.; Gasbarri, T.; Solinas, M.; Glauber, M. Functional Magnetic Resonance Imaging in the Evaluation of the Elastic Properties of Ascending Aortic Aneurysm. Braz. J. Cardiovasc. Surg. 2019, 34, 451–457. [Google Scholar] [CrossRef]
- Wu, J.; Zafar, M.A.; Li, Y.; Saeyeldin, A.; Huang, Y.; Zhao, R.; Qiu, J.; Tanweer, M.; Abdelbaky, M.; Gryaznov, A.; et al. Ascending aortic length and risk of aortic adverse events: The neglected dimension. J. Am. Coll. Cardiol. 2019, 74, 1883–1894. [Google Scholar] [CrossRef] [PubMed]
- Heuts, S.; Adriaans, B.P.; Rylski, B.; Mihl, C.; Bekkers, S.C.A.M.; Olsthoorn, J.R.; Natour, E.; Bouman, H.; Berezowski, M.; Kosiorowska, K.; et al. Evaluating the diagnostic accuracy of maximal aortic diameter, length and volume for prediction of aortic dissection. Heart 2020, 106, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Krüger, T.; Sandoval Boburg, R.; Lescan, M.; Oikonomou, A.; Schneider, W.; Vöhringer, L.; Lausberg, H.; Bamberg, F.; Blumenstock, G.; Schlensak, C. Aortic elongation in aortic aneurysm and dissection: The Tübingen Aortic Pathoanatomy (TAIPAN) project. Eur. J. Cardiothorac. Surg. 2018, 54, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemtsovskaja, G.; Pilt, K.; Samarin, A.; Abina, J.; Meigas, K.; Viigimaa, M. Construction of gender-specific regression models for aortic length estimation based on computed tomography images. Health Technol. 2020, 10, 679–687. [Google Scholar] [CrossRef]
- Correa Londono, M.; Trussardi, N.; Obmann, V.C.; Piccini, D.; Ith, M.; von Tengg-Kobligk, H.; Jung, B. Radial self-navigated native magnetic resonance angiography in comparison to navigator-gated contrast-enhanced MRA of the entire thoracic aorta in an aortic patient collective. J. Cardiovasc. Magn. Reason. 2021, 23, 94. [Google Scholar] [CrossRef] [PubMed]
- Poskaite, P.; Pamminger, M.; Kranewitter, C.; Kremser, C.; Reindl, M.; Reiter, G.; Piccini, D.; Dumfarth, J.; Henninger, B.; Tiller, C.; et al. Self-navigated 3D whole-heart MRA for non-enhanced surveillance of thoracic aortic dilation: A comparison to CTA. Magn. Reason. Imaging 2021, 76, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, Y.; Redheuil, A.; Kachenoura, N.; Ambale Venkatesh, B.; Lima, J.A.C. Imaging Insights on the Aorta in Aging. Circ. Cardiovasc. Imaging 2018, 11, e005617. [Google Scholar] [CrossRef] [PubMed]
- Salmasi, M.Y.; Pirola, S.; Mahuttanatan, S.; Fisichella, S.M.; Sengupta, S.; Jarral, O.A.; Oo, A.; O’Regan, D.; Xu, X.Y.; Athanasiou, T. Geometry and flow in ascending aortic aneurysms are influenced by left ventricular outflow tract orientation: Detecting increased wall shear stress on the outer curve of proximal aortic aneurysms. J. Thorac. Cardiovasc. Surg. 2021, S0022-5223(21)00913-2, Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ghulam Ali, S.; Fusini, L.; Dalla Cia, A.; Tamborini, G.; Gripari, P.; Muratori, M.; Mancini, M.E.; Annoni, A.; Formenti, A.; Pepi, M. Technological advancements in echo-cardiographic assessment of thoracic aortic dilatation: Head to head comparison among multidetector computed tomography, 2-dimensional, and 3-dimensional echocardiography measurements. J. Thorac. Imaging 2018, 33, 232–239. [Google Scholar] [CrossRef]
- Hoshina, R.; Kishima, H.; Mine, T.; Ishihara, M. Aortic dissection during transoesophageal echocardiography: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Boczar, K.E.; Boodhwani, M.; Beauchesne, L.; Dennie, C.; Chan, K.L.; Wells, G.A.; Coutinho, T. Aortic Stiffness, Central Blood Pressure, and Pulsatile Arterial Load Predict Future Thoracic Aortic Aneurysm Expansion. Hypertension 2021, 77, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Jue, J.; Boodhwani, M.; Beauchesne, L.; Dennie, C.; Nagpal, S.; Chan, K.L.; Coutinho, T. Greater Aortic Stiffness and Pulsatile Arterial Load Are Associated With Larger Thoracic Aortic Aneurysm Size in Women. Circulation 2019, 139, 1124–1126. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.; Ganizada, B.; Debeij, G.; Natour, E.; Maessen, J.; Spronck, B.; Schurgers, L.; Delhaas, T.; Huberts, W.; Bidar, E.; et al. Intra-Operative Video-Based Measurement of Biaxial Strains of the Ascending Thoracic Aorta. Biomedicines 2021, 9, 670. [Google Scholar] [CrossRef]
- Perez-Casares, A.; Dionne, A.; Gauvreau, K.; Prakash, A. Rapid ascending aorta stiffening in bicuspid aortic valve on serial cardiovascular magnetic resonance evaluation: Comparison with connective tissue disorders. J. Cardiovasc. Magn. Reason. 2021, 23, 11. [Google Scholar] [CrossRef] [PubMed]
- Ussov, W.Y.; Ignatenko, G.A.; Bergen, T.A.; Shelkovnikova, T.A.; Bril, K.R.; Khovrin, V.V.; Maksimova, A.S.; Belichenko, O.I.; Trufanov, G.E. Computational evaluation of mechano-elastic properties and of paramagnetic contrast enhancement of thoracic aortic wall in acute myocardial infarction and in non-coronarogenic myocardial damage, from the data of dynamic ECG-gated MRI (MR-elastometry). Transl. Med. = Transl. Med. 2021, 8, 43–58. [Google Scholar] [CrossRef]
- Ussov, W.Y.; Ryumshina, N.I.; Bagriy, A.E.; Sukhareva, A.E.; Maksimova, A.S.; Sinitsyn, V.E.; Falkovskaya, A.Y.; Mordovin, V.F.; Belichenko, O.I. Magnetic resonance con-trast-enhanced imaging of the aortic wall as risk index for acute ischemic cerebral stroke in patients with resistant arterial hypertension. Russ. Electron. J. Radiol. 2020, 10, 108–119. (In Russian) [Google Scholar] [CrossRef]
- Maksimova, A.S.; Lishmanov, Y.B.; Usov, W.Y. Role of magnetic resonance imaging in studies of atherosclerosis of aorta. Russ. Electron. J. Radiol. 2018, 8, 184–193. [Google Scholar] [CrossRef]
- Kozuń, M.; Płonek, T.; Jasiński, M.; Filipiak, J. Effect of dissection on the mechanical properties of human ascending aorta and human ascending aorta aneurysm. Acta Bioeng. Biomech. 2019, 21, 127–134. [Google Scholar]
- Saeyeldin, A.; Zafar, M.A.; Baldassarre, L.A.; Mojibian, H.; Ziganshin, B.A.; Mukherjee, S.K.; Elefteriades, J.A. Aortic delamination-a pos-sible precursor of impending catastrophe. Int. J. Angiol. 2021, 30, 160–164. [Google Scholar] [CrossRef]
- Subramaniam, D.R.; Gutmark, E.; Andersen, N.; Nielsen, D.; Mortensen, K.; Gravholt, C.; Backeljauw, P.; Gutmark-Little, I. Influence of material model and aortic root motion in finite element analysis of two exemplary cases of proximal aortic dissection. J. Biomech. Eng. 2021, 143, 014504. [Google Scholar] [CrossRef]
- Chung, J.C.; Wong, E.; Tang, M.; Eliathamby, D.; Forbes, T.L.; Butany, J.; Simmons, C.A.; Ouzounian, M. Biomechanics of Aortic Dissection: A Comparison of Aortas Associated With Bicuspid and Tricuspid Aortic Valves. J. Am. Heart Assoc. 2020, 9, e016715. [Google Scholar] [CrossRef]
- Tang, M.; Eliathamby, D.; Ouzounian, M.; Simmons, C.A.; Chung, J.C. Dependency of energy loss on strain rate, strain mag-nitude and preload: Towards development of a novel biomarker for aortic aneurysm dissection risk. J. Mech. Behav. Biomed. Mater. 2021, 124, 104736. [Google Scholar] [CrossRef]
- Bissell, M.M.; Dall’Armellina, E.; Choudhury, R.P. Flow vortices in the aortic root: In Vivo 4D-MRI confirms predictions of Leonardo da Vinci. Eur. Heart J. 2014, 35, 1344. [Google Scholar] [CrossRef] [Green Version]
- Manchester, E.L.; Pirola, S.; Salmasi, M.Y.; O’Regan, D.P.; Athanasiou, T.; Xu, X.Y. Analysis of Turbulence Effects in a Pa-tient-Specific Aorta with Aortic Valve Stenosis. Cardiovasc. Eng. Technol. 2021, 12, 438–453. [Google Scholar] [CrossRef]
- van Ooij, P.; Farag, E.S.; Blanken, C.P.S.; Nederveen, A.J.; Groenink, M.; Planken, R.N.; Boekholdt, S.M. Fully quantitative mapping of abnormal aortic velocity and wall shear stress direction in patients with bicuspid aortic valves and repaired coarctation using 4D flow cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reason. 2021, 23, 9. [Google Scholar] [CrossRef]
- De Nisco, G.; Tasso, P.; Calò, K.; Mazzi, V.; Gallo, D.; Condemi, F.; Farzaneh, S.; Avril, S.; Morbiducci, U. Deciphering ascending thoracic aortic aneurysm hemodynamics in relation to biomechanical properties. Med. Eng. Phys. 2020, 82, 119–129. [Google Scholar] [CrossRef]
- Emerel, L.; Thunes, J.; Kickliter, T.; Billaud, M.; Phillippi, J.A.; Vorp, D.A.; Maiti, S.; Gleason, T.G. Predissection-derived geometric and distensibility indices reveal increased peak longitudinal stress and stiffness in patients sustaining acute type A aortic dissection: Implications for predicting dissection. J. Thorac. Cardiovasc. Surg. 2019, 158, 355–363. [Google Scholar] [CrossRef]
- Suwa, K.; Rahman, O.A.; Bollache, E.; Rose, M.J.; Rahsepar, A.A.; Carr, J.C.; Collins, J.D.; Barker, A.J.; Markl, M. Effect of aortic valve disease on 3D hemo-dynamics in patients with aortic dilation and trileaflet aortic valve morphology. J. Magn. Reason. Imaging 2020, 51, 481–491. [Google Scholar] [CrossRef]
- Catalano, C.; Agnese, V.; Gentile, G.; Raffa, G.M.; Pilato, M.; Pasta, S. Atlas-Based Evaluation of Hemodynamic in Ascending Thoracic Aortic Aneurysms. Appl. Sci. 2022, 12, 394. [Google Scholar] [CrossRef]
- Jayendiran, R.; Campisi, S.; Viallon, M.; Croisille, P.; Avril, S. Hemodynamics alteration in patient-specific dilated ascending thoracic aortas with tricuspid and bicuspid aortic valves. J. Biomech. 2020, 110, 109954. [Google Scholar] [CrossRef]
- Wisneski, A.D.; Mookhoek, A.; Chitsaz, S.; Hope, M.D.; Guccione, J.M.; Ge, L.; Tseng, E.E. Bicuspid aortic valve-associated ascending thoracic aortic aneurysm: Patient-specific finite element analysis. J. Heart Valve Dis. 2015, 24, 714–721. [Google Scholar]
- Gauer, S.; Balint, B.; Kollmann, C.; Federspiel, J.M.; Henn, D.; Bandner-Risch, D.; Schmied, W.; Schäfers, H.J. Dysregulation of endothelial nitric oxide synthase does not depend on hemodynamic alterations in bicuspid aortic valve aortopathy. J. Am. Heart Assoc. 2020, 9, e016471. [Google Scholar] [CrossRef]
- Sundström, E.; Jonnagiri, R.; Gutmark-Little, I.; Gutmark, E.; Critser, P.; Taylor, M.D.; Tretter, J.T. Effects of normal variation in the rotational position of the aortic root on hemodynamics and tissue biomechanics of the thoracic aorta. Cardiovasc. Eng. Technol. 2020, 11, 47–58. [Google Scholar] [CrossRef]
- Goto, T.; Fukuda, I.; Inamura, T.; Shirota, M.; Minakawa, M. Flow analysis during mock circulation in normal and aortic arch aneurysm models through an aortic cannula toward the aortic arch and root. J. Artif. Organs. 2021, 24, 442–449. [Google Scholar] [CrossRef]
- Numata, S.; Itatani, K.; Kanda, K.; Doi, K.; Yamazaki, S.; Morimoto, K.; Manabe, K.; Ikemoto, K.; Yaku, H. Blood flow analysis of the aortic arch using computational fluid dynamics. Eur. J. Cardiothorac. Surg. 2016, 49, 1578–1585. [Google Scholar] [CrossRef] [Green Version]
- Ong, C.W.; Wee, I.; Syn, N.; Ng, S.; Leo, H.L.; Richards, A.M.; Choong, A.M.T.L. Computational fluid dynamics modeling of hemodynamic parameters in the human diseased aorta: A systematic review. Ann. Vasc. Surg. 2020, 63, 336–381. [Google Scholar] [CrossRef]
- Ziganshin, B.A.; Elefteriades, J.A. Guilt by association: A paradigm for detection of silent aortic disease. Ann. Cardiothorac. Surg. 2016, 5, 174–187. [Google Scholar] [CrossRef] [Green Version]
- Chewcharat, A.; Hamaya, R.; Thongprayoon, C.; Cato, L.D.; Mao, M.A.; Cheungpasitporn, W. The association between simple renal cyst and aortic diseases: A systematic review and meta-analysis of observational studies. J. Evid. Based Med. 2020, 13, 265–274. [Google Scholar] [CrossRef]
- Brownstein, A.J.; Bin Mahmood, S.U.; Saeyeldin, A.; Velasquez Mejia, C.; Zafar, M.A.; Li, Y.; Rizzo, J.A.; Dahl, N.K.; Erben, Y.; Ziganshin, B.A.; et al. Simple renal cysts and bovine aortic arch: Markers for aortic disease. Open Heart 2019, 6, e000862. [Google Scholar] [CrossRef]
- Olsson, C.; Eriksson, P.; Franco-Cereceda, A. Association between thoracic aortic disease and inguinal hernia. J. Am. Heart Assoc. 2014, 3, e001040. [Google Scholar] [CrossRef] [Green Version]
- Argan, O.; Avci, E.; Yildirim, T.; Safak, O. Epicardial adipose tissue is a predictor of ascending aortic dilatation in hypertensive patients, but not paracardial adipose tissue. BMC Cardiovasc. Disord. 2020, 20, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longi, F.; Orelaru, F.; Clemence, J., Jr.; Naeem, A.; Wu, X.; Yang, B. Outcomes of Bicuspid Aortic Valve Thoracic Aorta (4.0-4.5cm) After Aortic Valve Replacement. Ann. Thorac. Surg. 2022, 113, 1521–1528. [Google Scholar] [CrossRef]
- Dumfarth, J.; Chou, A.S.; Ziganshin, B.A.; Bhandari, R.; Peterss, S.; Tranquilli, M.; Mojibian, H.; Fang, H.; Rizzo, J.A.; Elefteriades, J.A. Atypical aortic arch branching variants: A novel marker for thoracic aortic disease. J. Thorac. Cardiovasc. Surg. 2015, 149, 1586–1592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brownstein, A.J.; Rajaee, S.; Erben, Y.; Li, Y.; Rizzo, J.A.; Lyall, V.; Mojibian, H.; Ziganshin, B.A.; Elefteriades, J.A. Natural history of aneurysmal aortic arch branch vessels in a single tertiary referral center. J. Vasc. Surg. 2018, 68, 1631–1639.e1. [Google Scholar] [CrossRef]
- Blumel, R.; Patel, K.; Rizzo, J.A.; Mok, S.; Barrett, A.; Wu, J.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. Accuracy of the “thumb-palm test” for detection of ascending aortic aneurysm. Am. J. Cardiol. 2021, 150, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. Diabetes mellitus: Is it protective against aneurysm? A narrative review. Cardiology 2018, 141, 107–122. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Zhao, S.; Wang, L.; Yang, K.; Xiao, W.; Clifford, S.P.; Huang, J.; Chen, X. Cardiovascular changes in patients with COVID-19 from Wuhan, China. Front Cardiovasc. Med. 2020, 7, 150. [Google Scholar] [CrossRef] [PubMed]
- Ostberg, N.P.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. The genetics of thoracic aortic aneurysms and dissection: A clinical perspective. Biomolecules 2020, 10, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faggion Vinholo, T.; Zafar, M.A.; Papanikolaou, D.; Chung, J.; Ellauzi, H.; Ziganshin, B.A.; Elefteriades, J.A. Direct measurement of as-cending aortic diameter by intraoperative caliper assessment. J. Thorac. Cardiovasc. Surg. 2021, 161, e143–e146. [Google Scholar] [CrossRef] [PubMed]
- Weerakkody, R.; Ross, D.; Parry, D.A.; Ziganshin, B.; Vandrovcova, J.; Gampawar, P.; Abdullah, A.; Biggs, J.; Dumfarth, J.; Ibrahim, Y.; et al. Targeted genetic analysis in a large cohort of familial and sporadic cases of aneurysm or dissection of the thoracic aorta. Genet. Med. 2018, 20, 1414–1422. [Google Scholar] [CrossRef]
- Mariscalco, G.; Debiec, R.; Elefteriades, J.A.; Samani, N.J.; Murphy, G.J. Systematic review of studies that have evaluated screening tests in relatives of patients affected by nonsyndromic thoracic aortic disease. J. Am. Heart Assoc. 2018, 7, e009302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostina, A.S.; Uspensky, V.E.; Irtyuga, O.B.; Ignatieva, E.V.; Freylikhman, O.; Gavriliuk, N.D.; Moiseeva, O.M.; Zhuk, S.; Tomilin, A.; Kostareva, A.A.; et al. Notch-dependent EMT is attenuated in patients with aortic aneurysm and bicuspid aortic valve. Biochim. Biophys. Acta 2016, 1862, 733–740. [Google Scholar] [CrossRef]
- Wu, B.; Li, J.; Wang, Y.; Cheng, Y.; Wang, C.; Shu, X. Recurrent germline mutations as genetic markers for aortic root dilatation in bicuspid aortic valve patients. Heart Vessels 2021, 36, 530–540. [Google Scholar] [CrossRef]
- Wang, Y.; Barbacioru, C.C.; Shiffman, D.; Balasubramanian, S.; Iakoubova, O.; Tranquilli, M.; Albornoz, G.; Blake, J.; Mehmet, N.N.; Ngadimo, D.; et al. Gene expression signature in peripheral blood detects thoracic aortic aneurysm. PLoS ONE 2007, 2, e1050. [Google Scholar] [CrossRef] [PubMed]
- Çiftel, M.; Ateş, N.; Yılmaz, O. Investigation of endothelial dysfunction and arterial stiffness in multisystem inflammatory syndrome in children. Eur. J. Pediatr. 2022, 181, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Pirruccello, J.P.; Chaffin, M.D.; Chou, E.L.; Fleming, S.J.; Lin, H.; Nekoui, M.; Khurshid, S.; Friedman, S.F.; Bick, A.G.; Arduini, A.; et al. Deep learning enables genetic analysis of the human thoracic aorta. Nat. Genet. 2022, 54, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Liu, M.; Martin, C.; Elefteriades, J.A.; Sun, W. A machine learning approach to investigate the relationship between shape features and numerically predicted risk of ascending aortic aneurysm. Biomech. Model. Mechanobiol. 2017, 16, 1519–1533. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.B. Surgery: Predicting acute type B aortic dissection-size does not matter. Nat. Rev. Cardiol. 2011, 8, 362. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.D.; Bordoni, B. Embryology, Aortic Arch. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK553173/ (accessed on 17 August 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anfinogenova, N.D.; Sinitsyn, V.E.; Kozlov, B.N.; Panfilov, D.S.; Popov, S.V.; Vrublevsky, A.V.; Chernyavsky, A.; Bergen, T.; Khovrin, V.V.; Ussov, W.Y. Existing and Emerging Approaches to Risk Assessment in Patients with Ascending Thoracic Aortic Dilatation. J. Imaging 2022, 8, 280. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8100280
Anfinogenova ND, Sinitsyn VE, Kozlov BN, Panfilov DS, Popov SV, Vrublevsky AV, Chernyavsky A, Bergen T, Khovrin VV, Ussov WY. Existing and Emerging Approaches to Risk Assessment in Patients with Ascending Thoracic Aortic Dilatation. Journal of Imaging. 2022; 8(10):280. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8100280
Chicago/Turabian StyleAnfinogenova, Nina D., Valentin E. Sinitsyn, Boris N. Kozlov, Dmitry S. Panfilov, Sergey V. Popov, Alexander V. Vrublevsky, Alexander Chernyavsky, Tatyana Bergen, Valery V. Khovrin, and Wladimir Yu. Ussov. 2022. "Existing and Emerging Approaches to Risk Assessment in Patients with Ascending Thoracic Aortic Dilatation" Journal of Imaging 8, no. 10: 280. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8100280