Sweet Relief: Determining the Antimicrobial Activity of Medical Grade Honey Against Vaginal Isolates of Candida albicans


Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Test Compounds and Microtiter Plates
2.2. Inoculum Preparation
2.3. Plate Reading
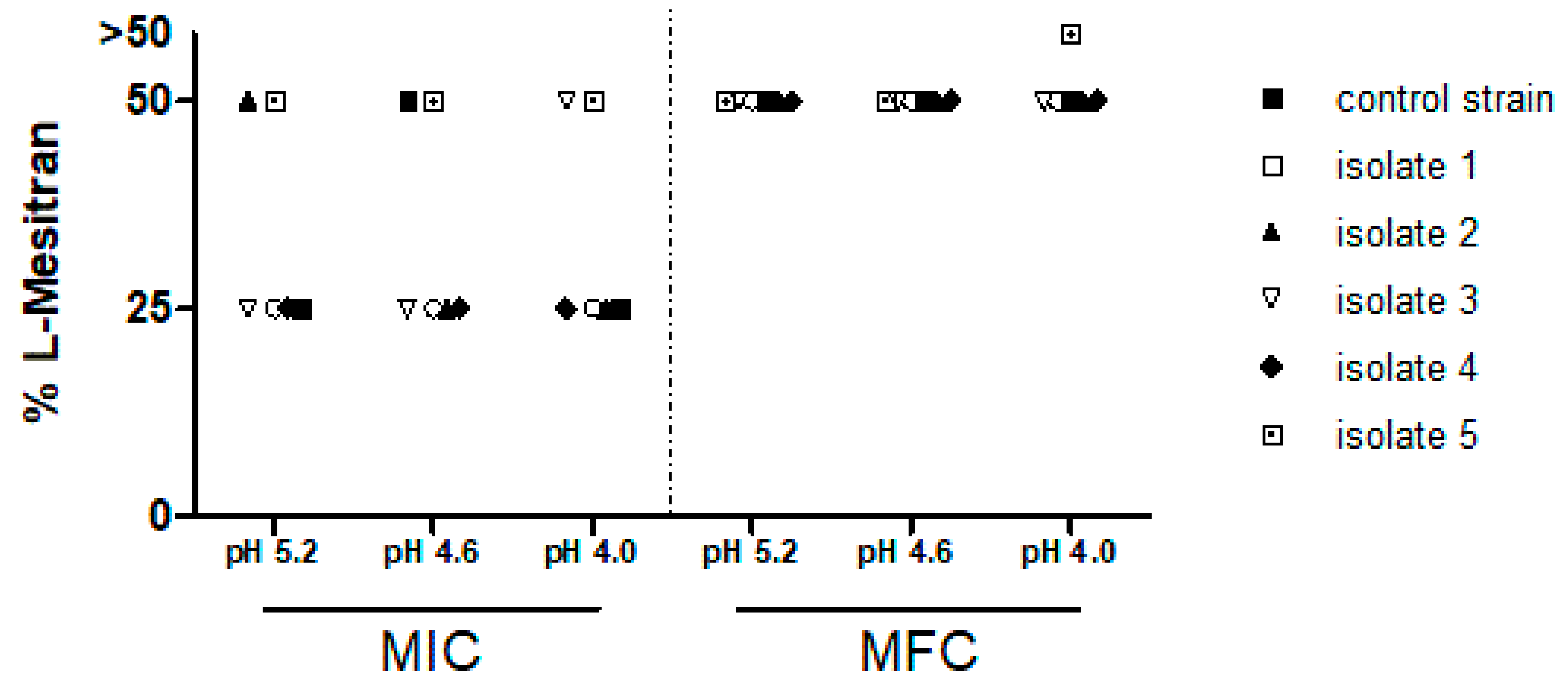
3. Results
4. Discussion
5. Conclusions
Ethics Approval and Consent to Participate
Consent for Publication
Availability of Data and Material
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chong, P.P.; Abdul Hadi, S.R.; Lee, Y.L.; Phan, C.L.; Tan, B.C.; Ng, K.P.; Seow, H.F. Genotyping and drug resistance profile of Candida spp. in recurrent and one-off vaginitis, and high association of non-albicans species with non-pregnant status. Infect. Genet. Evol. 2007, 7, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Cauchie, M.; Desmet, S.; Lagrou, K. Candida and its dual lifestyle as a commensal and a pathogen. Res. Microbiol. 2017, 168, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: a systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Korporaal, H.; Vinkers, M.; van Belkum, A.; van Binsbergen, J.; Lagro-Janssen, T.; Helmerhorst, T.; van der Meijden, W. Vulvovaginal candidiasis: Diagnostic and therapeutic approaches used by Dutch general practitioners AU - Engberts, Maria Karin. Eur. J. Gen. Pract. 2008, 14, 30–33. [Google Scholar] [CrossRef]
- Gardella, C.E.L.; Lentz, G.M. Comprehensive Gynecology; Lentz, G.L.R., Gershenson, D., Valea, F.A., Eds.; Elsevier: Philadelphia, PA, USA, 2012; Volume 7, pp. 524–565. [Google Scholar]
- Workowski, K.A.; Bolan, G.A.; Centers for Disease, C.; Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2015, 64, 1–137. [Google Scholar]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Patterson, T.F. Multidrug-Resistant Candida: Epidemiology, Molecular Mechanisms, and Treatment. J. Infect. Dis. 2017, 216, S445–S451. [Google Scholar] [CrossRef] [PubMed]
- Berkow, E.L.; Lockhart, S.R. Fluconazole resistance in Candida species: a current perspective. Infect. Drug Resist. 2017, 10, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Jull, A.B.; Cullum, N.; Dumville, J.C.; Westby, M.J.; Deshpande, S.; Walker, N. Honey as a topical treatment for wounds. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Willix, D.J.; Molan, P.C.; Harfoot, C.G. A comparison of the sensitivity of wound-infecting species of bacteria to the antibacterial activity of manuka honey and other honey. J. Appl. Bacteriol. 1992, 73, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Molan, P.C. The antibacterial activity of honey: 2. Variation in the potency of the antibacterial activity. N. Z. Bee World 1992, 73, 59–76. [Google Scholar] [CrossRef]
- Allen, K.L.; Molan, P.C.; Reid, G.M. A survey of the antibacterial activity of some New Zealand honeys. J. Pharm. Pharmacol. 1991, 43, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Estevinho, M.L.; Afonso, S.E.; Feás, X. Antifungal effect of lavender honey against Candida albicans, Candida krusei and Cryptococcus neoformans. J. Food Sci. Technol. 2011, 48, 640–643. [Google Scholar] [CrossRef] [PubMed]
- Shokri, H.; Sharifzadeh, A. Fungicidal efficacy of various honeys against fluconazole-resistant Candida species isolated from HIV(+) patients with candidiasis. J. Mycol. Med. 2017, 27, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Mandal, M.D.; Mandal, S. Honey: its medicinal property and antibacterial activity. Asian Pac. J. Trop Biomed. 2011, 1, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Olaitan, P.B.; Adeleke, O.E.; Ola, I.O. Honey: a reservoir for microorganisms and an inhibitory agent for microbes. Afr. Health Sci. 2007, 7, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Moussa, A.; Noureddine, D.; Saad, A.; Abdelmelek, M.; Abdelkader, B. Antifungal activity of four honeys of different types from Algeria against pathogenic yeast: Candida albicans and Rhodotorula sp. Asian Pac. J. Trop. Biomed. 2012, 2, 554–557. [Google Scholar] [CrossRef]
- Ramanauskiene, K.; Stelmakiene, A.; Briedis, V.; Ivanauskas, L.; Jakstas, V. The quantitative analysis of biologically active compounds in Lithuanian honey. Food Chem. 2012, 132, 1544–1548. [Google Scholar] [CrossRef]
- Rasul, A.; Millimouno, F.M.; Ali Eltayb, W.; Ali, M.; Li, J.; Li, X. Pinocembrin: a novel natural compound with versatile pharmacological and biological activities. Biomed. Res. Int 2013, 2013, 379850. [Google Scholar] [CrossRef]
- Uzel, A.; Sorkun, K.; Oncag, O.; Cogulu, D.; Gencay, O.; Salih, B. Chemical compositions and antimicrobial activities of four different Anatolian propolis samples. Microbiol. Res. 2005, 160, 189–195. [Google Scholar] [CrossRef]
- Maddocks, S.E.; Jenkins, R.E. Honey: a sweet solution to the growing problem of antimicrobial resistance? Future Microbiol. 2013, 8, 1419–1429. [Google Scholar] [CrossRef] [PubMed]
- Shan, Y. Medicinal honey in clinical practice: viable alternative or useful adjunct in wound care management? Br. J. Nurs. 2019, 28, S23–S30. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.; Vereecken, A.; Bosmans, E.; Dekeersmaecker, A.; Salembier, G.; Spitz, B. Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: aerobic vaginitis. BJOG 2002, 109, 34–43. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for yeasts. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Files/EUCAST_E_Def_7_3_1_Yeast_testing__definitive.pdf (accessed on 10 April 2019).
- Egan, M.E.; Lipsky, M.S. Diagnosis of vaginitis. Am. Fam Physician 2000, 62, 1095–1104. [Google Scholar] [PubMed]
- Banaeian-Borujeni, S.; Mobini, G.R.; Pourgheysari, B.; Validi, M. Comparison of the effect of honey and miconazole against Candida albicans in vitro. Adv. Biomed. Res. 2013, 2, 57. [Google Scholar] [CrossRef] [PubMed]
- Carter, D.A.; Blair, S.E.; Irish, J.; Shokohi, T. Honey has an antifungal effect against Candida species. Med. Mycology 2006, 44, 289–291. [Google Scholar] [CrossRef]
- Kuncic, M.K.; Jaklic, D.; Lapanje, A.; Gunde-Cimerman, N. Antibacterial and antimycotic activities of Slovenian honeys. Br. J. Biomed. Sci. 2012, 69, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Moussa, A.; Noureddine, D.; Hammoudi, S.M.; Saad, A.; Bourabeh, A.; Houari, H. Additive potential of ginger starch on antifungal potency of honey against Candida albicans. Asian Pac. J. Trop Biomed. 2012, 2, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Shahzad, S.; Ashraf, M.A.; Sajid, M.; Shahzad, A.; Rafique, A.; Mahmood, M.S. Evaluation of synergistic antimicrobial effect of vitamins (A, B1, B2, B6, B12, C, D, E and K) with antibiotics against resistant bacterial strains. J. Glob. Antimicrob. Resist. 2018, 13, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.; Tabrez, E.; Peela, J.; Honnavar, P.D.; Tabrez, S.S.M. Vitamin C: A Preventative, Therapeutic Agent Against Helicobacter pylori. Cureus 2018, 10, e3062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierpaoli, E.; Cirioni, O.; Barucca, A.; Orlando, F.; Silvestri, C.; Giacometti, A.; Provinciali, M. Vitamin E supplementation in old mice induces antimicrobial activity and improves the efficacy of daptomycin in an animal model of wounds infected with methicillin-resistant Staphylococcus aureus. J. Antimicrob. Chemother. 2011, 66, 2184–2185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Provinciali, M.; Cirioni, O.; Orlando, F.; Pierpaoli, E.; Barucca, A.; Silvestri, C.; Ghiselli, R.; Scalise, A.; Brescini, L.; Guerrieri, M.; et al. Vitamin E improves the in vivo efficacy of tigecycline and daptomycin in an animal model of wounds infected with meticillin-resistant Staphylococcus aureus. J. Med. Microbiol. 2011, 60, 1806–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallio, J.; Jaakkola, M.; Maki, M.; Kilpelainen, P.; Virtanen, V. Vitamin C inhibits staphylococcus aureus growth and enhances the inhibitory effect of quercetin on growth of Escherichia coli in vitro. Planta Med. 2012, 78, 1824–1830. [Google Scholar] [CrossRef] [PubMed]
- Verghese, R.; Mathew, S.; David, A. Antimicrobial activity of Vitamin C demonstrated on uropathogenic Escherichia coli and Klebsiella pneumonia. J. Curr. Res. Sci. Med. 2017, 3, 88. [Google Scholar]
- Avci, P.; Freire, F.; Banvolgyi, A.; Mylonakis, E.; Wikonkal, N.M.; Hamblin, M.R. Sodium ascorbate kills Candida albicans in vitro via iron-catalyzed Fenton reaction: importance of oxygenation and metabolism. Future microbial. 2016, 11, 1535–1547. [Google Scholar] [CrossRef] [PubMed]
- Helgadóttir, S.; Pandit, S.; Mokkapati, V.R.S.S.; Westerlund, F.; Apell, P.; Mijakovic, I. Vitamin C Pretreatment Enhances the Antibacterial Effect of Cold Atmospheric Plasma. Front. Cell. Infect. Microbiol. 2017, 7, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keen, M.A.; Hassan, I. Vitamin E in dermatology. Indian Dermatol. Online J. 2016, 7, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Hanna, C.; Fraunfelder, F.T.; Cable, M.; Hardberger, R.E. The effect of ophthalmic ointments on corneal wound healing. Am. J. Ophthalmol. 1973, 76, 193–200. [Google Scholar] [CrossRef]
- Oliveira, A.M.P.; Devesa, J.S.P.; Hill, P.B. In vitro efficacy of a honey-based gel against canine clinical isolates of Staphylococcus pseudintermedius and Malassezia pachydermatis. Vet. Dermatol. 2018, 29, 180-e165. [Google Scholar] [CrossRef]
- Sengupta, A.; Behera, J. Comprehensive view on chemistry, manufacturing & applications of lanolin extracted from wool pretreatment. Am. J. Eng. Res. 2014, 3, 33–43. [Google Scholar]
- Sobel, J.D. Vulvovaginal candidosis. Lancet (London, England) 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- Calderone, R.A.; Fonzi, W.A. Virulence factors of Candida albicans. Trends Microbiol. 2001, 9, 327–335. [Google Scholar] [CrossRef]
- Stone, L. Medilan: a hypoallergenic lanolin for emollient therapy. Br. J. Nurs. 2000, 9, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.W.; Steel, I. Investigations into biomechanisms of the moisturizing function of lanolin. J. Cosmet Sci. 1993, 44, 181–195. [Google Scholar]
- Kenechukwu, F.C.; Attama, A.A.; Ibezim, E.C.; Nnamani, P.O.; Umeyor, C.E.; Uronnachi, E.M.; Momoh, M.A.; Akpa, P.A.; Ozioko, A.C. Novel Intravaginal Drug Delivery System Based on Molecularly PEGylated Lipid Matrices for Improved Antifungal Activity of Miconazole Nitrate. Biomed. Res. Int. 2018, 2018, 3714329. [Google Scholar] [CrossRef]
- Drake, S.M.; Evans, B.A.; Gerken, A. Vaginal pH and microflora related to yeast infections and treatment. Br. J. Vener. Dis. 1980, 56, 107–110. [Google Scholar] [CrossRef]
- Darvishi, M.; Jahdi, F.; Hamzegardeshi, Z.; Goodarzi, S.; Vahedi, M. The Comparison of vaginal cream of mixing yogurt, honey and clotrimazole on symptoms of vaginal candidiasis. Glob. J. Health Sci. 2015, 7, 108–116. [Google Scholar] [CrossRef]
- Seifinadergoli, Z.; Nahidi, F.; Safaiyan, A.; Javadzadeh, Y.; Eteraf-Oskouei, T. Comparison of the efficacy of honey gel and clotrimazole cream in the treatment of vaginal candidiasis symptoms: a randomized clinical trial. Electron. Physician 2018, 10, 6904–6911. [Google Scholar] [CrossRef] [Green Version]
- Boon, M.E. Schimmelverhalen. In Weg van de groenesteeg; Boon, M.E., Beck, S., van Coevorden, R.S., Melkert, P., Eds.; Coulomb Press Leyden: Leiden, The Netherlands, 2002. [Google Scholar]
- Human Tissue Act 2004. Available online: https://www.legislation.gov.uk/ukpga/2004/30/contents (accessed on 10 April 2019).


{kind=link}
| Test compound and Composition | Concentrations Tested | Equivalent Honey Concentration | Tested pH Levels |
|---|---|---|---|
| Raw honey used in L-Mesitran 1 | 40%, 20%, 10%, 5% | 40%, 20%, 10%, 5% | 5.2, 4.6, 4.0 |
| L-Mesitran soft wound gel 2 | 50%, 25%, 12.5%, 6.25% | 20%, 10%, 5%, 2.5% | 5.2, 4.6, 4.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hermanns, R.; Cremers, N.A.J.; Leeming, J.P.; van der Werf, E.T. Sweet Relief: Determining the Antimicrobial Activity of Medical Grade Honey Against Vaginal Isolates of Candida albicans. J. Fungi 2019, 5, 85. https://0-doi-org.brum.beds.ac.uk/10.3390/jof5030085
Hermanns R, Cremers NAJ, Leeming JP, van der Werf ET. Sweet Relief: Determining the Antimicrobial Activity of Medical Grade Honey Against Vaginal Isolates of Candida albicans. Journal of Fungi. 2019; 5(3):85. https://0-doi-org.brum.beds.ac.uk/10.3390/jof5030085
Chicago/Turabian StyleHermanns, Renée, Niels A.J. Cremers, John P. Leeming, and Esther T. van der Werf. 2019. "Sweet Relief: Determining the Antimicrobial Activity of Medical Grade Honey Against Vaginal Isolates of Candida albicans" Journal of Fungi 5, no. 3: 85. https://0-doi-org.brum.beds.ac.uk/10.3390/jof5030085