
Real-Life Considerations on Antifungal Treatment Combinations for the Management of Invasive Mold Infections after Allogeneic Cell Transplantation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Objectives
2.3. Patient Identification and Data Collection
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Study Population and Baseline Patient Characteristics with IMI
3.2. Timing, Pathogens, and Clinical Characteristics of IMI
3.3. Antifungal Treatment of IMI
3.3.1. Antifungal Combination Therapies Administered
3.3.2. Antifungal Combination Therapy Changes
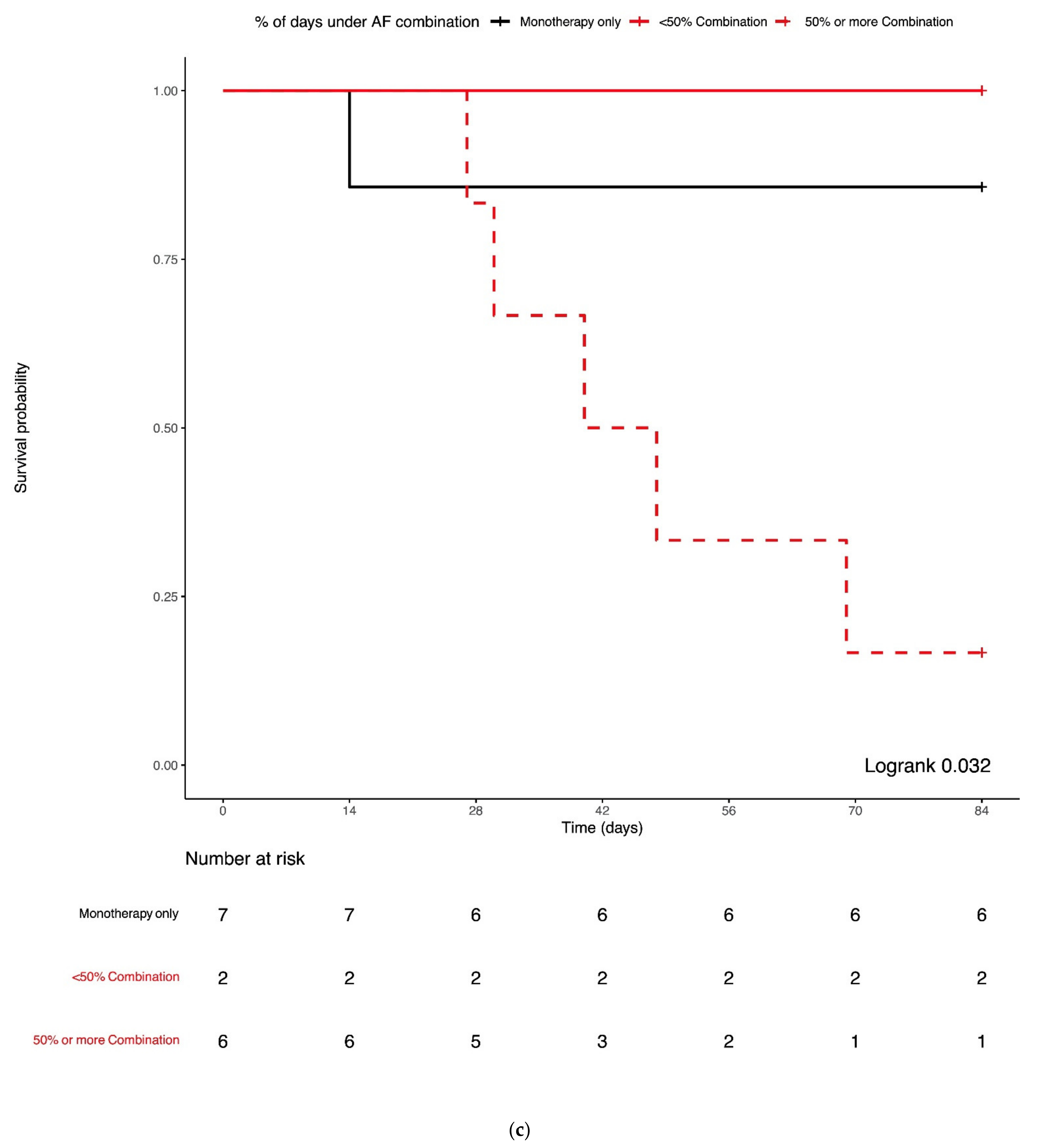
3.4. Combination Antifungal Treatment and IMI Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Upton, A.; Kirby, K.; Carpenter, P.; Boeckh, M.; Marr, K.A. Invasive Aspergillosis following Hematopoietic Cell Transplantation: Outcomes and Prognostic Factors Associated with Mortality. Clin. Infect. Dis. 2007, 44, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Vidal, C.; Upton, A.; Kirby, K.; Marr, K.A. Epidemiology of Invasive Mold Infections in Allogeneic Stem Cell Transplant Recipients: Biological Risk Factors for Infection According to Time after Transplantation. Clin. Infect. Dis. 2008, 47, 1041–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neofytos, D.; Horn, D.; Anaissie, E.; Steinbach, W.; Olyaei, A.; Fishman, J.; Pfaller, M.; Chang, C.; Webster, K.; Marr, K. Epidemiology and Outcome of Invasive Fungal Infection in Adult Hematopoietic Stem Cell Transplant Recipients: Analysis of Multicenter Prospective Antifungal Therapy (PATH) Alliance Registry. Clin. Infect. Dis. 2009, 48, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Kuster, S.; Stampf, S.; Gerber, B.; Baettig, V.; Weisser, M.; Gerull, S.; Medinger, M.; Passweg, J.R.; Schanz, U.; Garzoni, C.; et al. Incidence and outcome of invasive fungal diseases after allogeneic hematopoietic stem cell transplantation: A Swiss transplant cohort study. Transpl. Infect. Dis. 2018, 20, e12981. [Google Scholar] [CrossRef]
- Roth, R.; Masouridi-Levrat, S.; Chalandon, Y.; Mamez, A.C.; Giannotti, F.; Riat, A.; Ficher, A.; Poncet, A.; Glampedakis, E.; Van Delden, C.; et al. Invasive mold infections in allogeneic hematopoietic cell transplant recipients in 2020: Have we made enough progress? In Proceedings of the Swiss Society of Infectious Diseases Annual Meeting, Montreux, Switzerland, 2–3 September 2021. [Google Scholar]
- Kontoyiannis, D.P.; Marr, K.A.; Park, B.J.; Alexander, B.D.; Anaissie, E.J.; Walsh, T.J.; Ito, J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; et al. Prospective Surveillance for Invasive Fungal Infections in Hematopoietic Stem Cell Transplant Recipients, 2001–2006: Overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin. Infect. Dis. 2010, 50, 1091–1100. [Google Scholar] [CrossRef]
- Girmenia, C.; Raiola, A.M.; Piciocchi, A.; Algarotti, A.; Stanzani, M.; Cudillo, L.; Pecoraro, C.; Guidi, S.; Iori, A.P.; Montante, B.; et al. Incidence and Outcome of Invasive Fungal Diseases after Allogeneic Stem Cell Transplantation: A Prospective Study of the Gruppo Italian Trapianto Midollo Osseo (GITMO). Biol. Blood Marrow Transplant. 2014, 20, 872–880. [Google Scholar] [CrossRef]
- Marr, K.A.; Boeckh, M.; Carter, R.A.; Kim, H.W.; Corey, L. Combination Antifungal Therapy for Invasive Aspergillosis. Clin. Infect. Dis. 2004, 39, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Marr, K.A.; Schlamm, H.T.; Herbrecht, R.; Rottinghaus, S.T.; Bow, E.J.; Cornely, O.A.; Heinz, W.J.; Jagannatha, S.; Koh, L.P.; Kontoyiannis, D.P.; et al. Combination antifungal therapy for invasive aspergillosis: A randomized trial. Ann. Intern. Med. 2015, 162, 81–89. [Google Scholar] [CrossRef]
- Livengood, S.J.; Drew, R.H.; Perfect, J.R. Combination Therapy for Invasive Fungal Infections. Curr. Fungal Infect. Rep. 2020, 14, 40–49. [Google Scholar] [CrossRef]
- Kyvernitakis, A.; Torres, H.; Jiang, Y.; Chamilos, G.; Lewis, R.; Kontoyiannis, D. Initial use of combination treatment does not impact survival of 106 patients with haematologic malignancies and mucormycosis: A propensity score analysis. Clin. Microbiol. Infect. 2016, 22, 811.e1–811.e8. [Google Scholar] [CrossRef] [Green Version]
- Reed, C.; Bryant, R.; Ibrahim, A.S.; Edwards Jr, J.; Filler, S.G.; Goldberg, R.; Spellberg, B. Combination polyene-caspofungin treatment of rhino-orbital-cerebral mucormycosis. Clin. Infect. Dis. 2008, 47, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Spellberg, B.; Ibrahim, A.; Roilides, E.; Lewis, R.; Lortholary, O.; Petrikkos, G.; Kontoyiannis, D.P.; Walsh, T.J. Combination Therapy for Mucormycosis: Why, What, and How? Clin. Infect. Dis. 2012, 54, S73–S78. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Hachem, R.; Lewis, R.E.; Rivero, G.A.; Torres, H.A.; Thornby, J.; Champlin, R.; Kantarjian, H.; Bodey, G.P.; Raad, I.I. Efficacy and toxicity of caspofungin in combination with liposomal amphotericin B as primary or salvage treatment of invasive aspergillosis in patients with hematologic malignancies. Cancer 2003, 98, 292–299. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Lewis, R. How I treat mucormycosis. Blood 2011, 118, 1216–1224. [Google Scholar] [CrossRef]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Hoenigl, M.; Levitz, S.M.; Schuetz, A.N.; Zhang, S.X.; Cornely, O.A. All You Need to Know and More about the Diagnosis and Management of Rare Mold Infections. MBio 2021, 12, e02920-20. [Google Scholar] [CrossRef]
- Schaffner, A.; Frick, P.G. The Effect of Ketoconazole on Amphotericin B in a Model of Disseminated Aspergillosis. J. Infect. Dis. 1985, 151, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Polak, A.; Dixon, D.M. Fungistatic and Fungicidal Effects of Amphotericin B, Ketoconazole and Fluconazole (UK 49, 858) against Histoplasma capsulatum in vitro and in vivo. Mycoses 2009, 30, 186–194. [Google Scholar] [CrossRef]
- Katragkou, A.; McCarthy, M.; Meletiadis, J.; Petraitis, V.; Moradi, P.W.; Strauss, G.E.; Fouant, M.M.; Kovanda, L.L.; Petraitiene, R.; Roilides, E.; et al. In VitroCombination of Isavuconazole with Micafungin or Amphotericin B Deoxycholate against Medically Important Molds. Antimicrob. Agents Chemother. 2014, 58, 6934–6937. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2019, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Candoni, A.; Aversa, F.; Busca, A.; Cesaro, S.; Girmenia, C.; Luppi, M.; Rossi, G.; Venditti, A.; Nosari, A.M.; Pagano, L. Combination antifungal therapy for invasive mould diseases in haematologic patients. An update on clinical data. J. Chemother. 2014, 27, 1–12. [Google Scholar] [CrossRef]
- Candoni, A.; Caira, M.; Cesaro, S.; Busca, A.; Giacchino, M.; Fanci, R.; Delia, M.; Nosari, A.; Bonini, A.; Cattaneo, C.; et al. Multicentre surveillance study on feasibility, safety and efficacy of antifungal combination therapy for proven or probable invasive fungal diseases in haematological patients: The SEIFEM real-life combo study. Mycoses 2013, 57, 342–350. [Google Scholar] [CrossRef] [Green Version]
- Patterson, T.F.; Thompson, I.I.I.G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.E.; Verweij, P.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef] [Green Version]
- Segal, B.H.; Herbrecht, R.; Stevens, D.A.; Ostrosky-Zeichner, L.; Sobel, J.; Viscoli, C.; Walsh, T.J.; Maertens, J.; Patterson, T.F.; Perfect, J.R.; et al. Defining Responses to Therapy and Study Outcomes in Clinical Trials of Invasive Fungal Diseases: Mycoses Study Group and European Organization for Research and Treatment of Cancer Consensus Criteria. Clin. Infect. Dis. 2008, 47, 674–683. [Google Scholar] [CrossRef]
- Hachem, R.; Gomes, M.; El Helou, G.; El Zakhem, A.; Kassis, C.; Ramos, E.; Jiang, Y.; Chaftari, A.-M.; Raad, I.I. Invasive aspergillosis caused by Aspergillus terreus: An emerging opportunistic infection with poor outcome independent of azole therapy. J. Antimicrob. Chemother. 2014, 69, 3148–3155. [Google Scholar] [CrossRef] [Green Version]
- Glampedakis, E.; Cassaing, S.; Fekkar, A.; Dannaoui, E.; Bougnoux, M.-E.; Bretagne, S.; Neofytos, D.; Schreiber, P.W.; Hennequin, C.; Morio, F.; et al. Invasive Aspergillosis Due to Aspergillus Section Usti: A Multicenter Retrospective Study. Clin. Infect. Dis. 2021, 72, 1379–1385. [Google Scholar] [CrossRef]
- Greene, R.E.; Schlamm, H.T.; Oestmann, J.-W.; Stark, P.; Durand, C.; Lortholary, O.; Wingard, J.R.; Herbrecht, R.; Ribaud, P.; Patterson, T.F.; et al. Imaging Findings in Acute Invasive Pulmonary Aspergillosis: Clinical Significance of the Halo Sign. Clin. Infect. Dis. 2007, 44, 373–379. [Google Scholar] [CrossRef]
- Cornely, O.; Maertens, J.; Bresnik, M.; Ebrahimi, R.; Ullmann, A.J.; Bouza, E.; Heussel, C.P.; Lortholary, O.; Rieger, C.; Boehme, A.; et al. Liposomal Amphotericin B as Initial Therapy for Invasive Mold Infection: A Randomized Trial Comparing a High-Loading Dose Regimen with Standard Dosing (AmBiLoad Trial). Clin. Infect. Dis. 2007, 44, 1289–1297. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients N = 47 | IA N = 33 1 | Non-IA IMI N = 15 1 | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age at IMI diagnosis, median (IQR) | 57 (41–61) | 57 (42–61) | 56 (43–61) | 0.72 |
| Sex, Female | 19 (40) | 12 (36) | 7 (47) | 0.53 |
| Underlying disease leading to HCT | ||||
| Acute leukemia 1 | 27 (59) | 16 (49) | 12 (82) | 0.06 |
| Myelodysplastic syndrome | 6 (12) | 5 (15) | 1 (6) | 0.65 |
| Lymphoma | 6 (12) | 5 (15) | 1 (6) | 0.65 |
| Other 2 | 8 (17) | 7 (21) | 1 (6) | 0.41 |
| HCT-related characteristics | ||||
| Conditioning regimen, myeloablative | 9 (19) | 4 (12) | 5 (33) | 0.12 |
| HCT source, bone marrow | 8 (17) | 5 (15) | 3 (20) | 0.69 |
| Donor-related characteristics | ||||
| Matched related 1 | 10 (22) | 8 (25) | 3 (20) | 1 |
| Matched unrelated | 26 (55) | 16 (48) | 10 (67) | 0.35 |
| Mismatched related | 3 (6) | 3 (9) | 1 | |
| Haplo-identical | 8 (17) | 6 (18) | 2 (13) | 0.54 |
| CMV D/R serologic status | ||||
| D-R- | 10 (22) | 7 (21) | 3 (20) | 1 |
| D-R+/D+R+ 1 | 31 (66) | 22 (67) | 10 (67) | 1 |
| D+R- | 6 (12) | 4 (12) | 2 (13) | 1 |
| GvHD | ||||
| Acute GvHD ≥ grade 2 1 | 31 (66) | 23 (70) | 9 (60) | 0.53 |
| Chronic GvHD | 12 (24) | 9 (27) | 3 (20) | 0.73 |
| All Patients N = 47 | IA N = 33 1 | Non-IA IMI N = 15 1 | p-Value | |
|---|---|---|---|---|
| Timing of IMI post-HCT | ||||
| Post-HCT day IMI diagnosis, median (IQR) | 189 (19–376) | 173 (21–364) | 218 (16–344) | 0.84 |
| EORTC–MSGERC Classification 2 | ||||
| Probable IMI | 37 (77) | 28 (85) | 9 (60) | 0.07 |
| Proven IMI | 11 (23) | 5 (15) | 6 (40) | 0.07 |
| Extent of infection | ||||
| Single site | 36 (77) | 27 (82) | 10 (66) | 0.28 |
| Disseminated (>1 sites) | 11 (23) | 6 (19) | 5 (34) | 0.28 |
| Sites of infection 3 | ||||
| Lung | 43 (91) | 30 (91) | 13 (87) | 0.64 |
| Sinus | 5 (11) | 3 (9) | 2 (13) | 0.64 |
| Brain | 2 (4) | 1 (3) | 1 (6) | 0.53 |
| Skin/soft tissues | 5 (11) | 2 (6) | 3 (20) | 0.32 |
| Other 4 | 6 (12) | 4 (12) | 2 (13) | 1 |
| IMI pathogens | ||||
| Aspergillus spp 5 | 33 (69) | 33 (100) | ||
| Mucorales species | 9 (19) | 9 (60) | ||
| Fusarium spp. | 2 (4) | 2 (13) | ||
| Other 6 | 4 (8) | 4 (27) | ||
| Outcomes 7 | ||||
| Death by week 6 | 11 (23) | 7 (21) | 4 (29) | 0.70 |
| Death by week 12 | 14 (30) | 8 (24) | 6 (40) | 0.30 |
| Death by week 24 | 24 (51) | 17 (52) | 7 (50) | 1 |
| Death by day 365 | 30 (64) | 20 (61) | 10 (71) | 0.53 |
| Days from IMI diagnosis to death, median (IQR) | 130 (45–494) | 123 (67-497) | 150 (44–390) | 0.94 |
| All Patients N = 47 | IA N = 33 1 | Non-IA IMI N = 15 1 | p-Value | |
|---|---|---|---|---|
| Time from IMI to treatment initiation, median (IQR) | 0 (1–3) | 0 (0–2) | 2 (0.5–4) | 0.08 |
| Type of treatment | ||||
| Monotherapy only | 23 (49) | 16 (48) | 7 (47) | 1 |
| Combination therapy only | 4 (9) | 2 (7) | 2 (13) | 0.57 |
| Monotherapy/combination treatment | 20 (42) | 15 (45) | 6 (40) | 0.75 |
| Treatment duration | ||||
| Overall treatment duration in days, median (IQR) | 112 (40–208) | 112 (60–195) | 99 (28–250) | 0.30 |
| Time to combination treatment initiation | ||||
| Post-IMI diagnosis day, median (IQR) | 8 (2–19) | 9 (2–34) | 6 (2 -8) | 0.46 |
| Administration within first 7 days from IMI diagnosis | 11 (23) | 7 (21) | 4 (27) | 0.70 |
| Administration within first 14 days from IMI diagnosis | 17 (36) | 10 (30) | 7 (47) | 0.33 |
| Administration for ≥7 days during first 28 days from IMI diagnosis | 14 (30) | 7 (21) | 7 (47) | 0.09 |
| Courses of combination treatment | ||||
| Combination courses per patient, median (IQR) | 2 (1–3) | 1 (1–3) | 2 (1–2) | 0.87 |
| Patients with 1 combination course | 12 (26) | 9 (27) | 3 (20) | 0.67 |
| Patients with >1 combination courses | 12 (26) | 8 (24) | 5 (33) | 0.67 |
| Indication for combination treatment initiation 2 | ||||
| Severe IMI | 18 (38) | 10 (30) | 9 (60) | 0.54 |
| Pathogen identification lacking | 5 (11) | 1 (3) | 4 (27) | 0.14 |
| Antifungal susceptibility lacking | 14 (30) | 10 (30) | 4 (27) | 0.33 |
| Combination until therapeutic azole serum concentration | 6 (13) | 5 (15) | 1 (7) | 0.38 |
| Types of treatment combinations 2 | ||||
| Azole/echinocandin | 8 (17) | 5 (15) | 3 (20) | 1 |
| Azole/amphotericin-B | 13 (28) | 8 (24) | 6 (40) | 0.49 |
| Amphotericin B/echinocandin | 10 (21) | 8 (24) | 2 (13) | 0.43 |
| Azole/amphotericin-B/echinocandin | 5 (11) | 3 (9) | 2 (13) | 1 |
| Duration of combination treatment | ||||
| Cumulative days, median (IQR) | 28 (7–47) | 14 (6–50) | 28 (21–34) | 0.18 |
| Azole/echinocandin days, median (IQR) | 11 (8–15) | 12 (8–16) | 10 (9–13) | 0.78 |
| Azole/amphotericin-B days, median (IQR) | 12 (5–32) | 7 (5–13) | 25 (13–37) | 0.19 |
| Echinocandin/amphotericin-B days, median (IQR) | 19 (7–65) | 33 (11–74) | 6 (5–7) | 0.08 |
| Azole/echinocandin/amphotericin-B days, median (IQR) | 10 (8–17) | 10 (9–15) | 12 (9–14) | 0.80 |
| All Treatment Courses N = 163 | Monotherapy Courses N = 115 | Combination Courses N = 48 | p-Value | |
|---|---|---|---|---|
| Treatment initiation reasons 1 | ||||
| Clinical efficacy | 122 (75) | 80 (70) | 42 (88) | 0.02 |
| IA suspicion | 46 (28) | 36 (31) | 10 (21) | 0.19 |
| Non-IA IMI suspicion | 12 (7) | 8 (7) | 4 (8) | 0.74 |
| Switch to targeted therapy | 43 (26) | 24 (21) | 19 (40) | <0.01 |
| Low azole concentration in serum | 10 (6) | 3 (3) | 9 (19) | <0.01 |
| Stable or progressive IMI | 27 (17) | 13 (11) | 14 (30) | <0.01 |
| Improvement in IMI | 4 (2) | 4 (3) | ||
| Toxicity | 39 (24) | 34 (30) | 5 (10) | <0.01 |
| Renal toxicity | 9 (6) | 8 (7) | 1 (2) | 0.28 |
| Liver toxicity | 17 (10) | 14 (12) | 3 (6) | 0.40 |
| Neurologic toxicity | 4 (2) | 4 (3) | ||
| Cutaneous toxicity | 2 (1) | 2 (3) | ||
| QT interval prolongation | 1 (1) | 1 (1) | ||
| Drug interactions | 6 (4) | 5 (4) | 1 (2) | 0.67 |
| Increased azole concentration in serum | 1 (1) | 1 (1) | ||
| Logistical reasons | 6 (4) | 6 (5) | ||
| Change from IV to PO | 4 (2) | 4 (3) | ||
| Costs and insurance coverage | 2 (1) | 2 (3) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glampedakis, E.; Roth, R.; Masouridi-Levrat, S.; Chalandon, Y.; Mamez, A.-C.; Giannotti, F.; Van Delden, C.; Neofytos, D. Real-Life Considerations on Antifungal Treatment Combinations for the Management of Invasive Mold Infections after Allogeneic Cell Transplantation. J. Fungi 2021, 7, 811. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7100811
Glampedakis E, Roth R, Masouridi-Levrat S, Chalandon Y, Mamez A-C, Giannotti F, Van Delden C, Neofytos D. Real-Life Considerations on Antifungal Treatment Combinations for the Management of Invasive Mold Infections after Allogeneic Cell Transplantation. Journal of Fungi. 2021; 7(10):811. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7100811
Chicago/Turabian StyleGlampedakis, Emmanouil, Romain Roth, Stavroula Masouridi-Levrat, Yves Chalandon, Anne-Claire Mamez, Federica Giannotti, Christian Van Delden, and Dionysios Neofytos. 2021. "Real-Life Considerations on Antifungal Treatment Combinations for the Management of Invasive Mold Infections after Allogeneic Cell Transplantation" Journal of Fungi 7, no. 10: 811. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7100811