
COVID-19-Associated Mucormycosis (CAM): Case-Series and Global Analysis of Mortality Risk Factors

 ,
,  ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical and Paraclinical Examination
2.2. Literature Review
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Case Series
3.1.1. Case No. 1

3.1.2. Case No. 2

3.1.3. Case No.3

3.1.4. Case No.4
3.1.5. Case No.5
3.1.6. Case No.6
3.1.7. Case No.7
3.2. Literature Review
3.2.1. Demographic Characteristics
3.2.2. Anamnestic Characteristics
3.2.3. Clinical Characteristics
3.2.4. Paraclinical Characteristics
3.2.5. Management and Outcome
3.2.6. Risk of Mortality
4. Discussion
4.1. Is CAM an Interaction between SARS-CoV-2 Virus and Mucor Fungus?
4.2. Are the Medical Anamneses and Treatment Protocols the Missing Keys?
4.3. Is CAM a Healthcare-Associated Condition?
4.4. Strengths
4.5. Limitations
4.6. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roudbary, M.; Kumar, S.; Kumar, A.; Černáková, L.; Nikoomanesh, F.; Rodrigues, C.F. Overview on the prevalence of fungal infections, immune response, and microbiome role in COVID-19 patients. J. Fungi 2021, 7, 720. [Google Scholar] [CrossRef]
- Rawson, T.M.; Wilson, R.C.; Holmes, A. Understanding the role of bacterial and fungal infection in COVID-19. Clin. Microbiol. Infect. 2021, 27, 9–11. [Google Scholar] [CrossRef]
- Riad, A.; Gomaa, E.; Hockova, B.; Klugar, M. Oral candidiasis of COVID-19 patients: Case report and review of evidence. J. Cosmet. Dermatol. 2021, 20, 1580–1584. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Gad, A.; Hockova, B.; Klugar, M. Oral candidiasis in non-severe COVID-19 patients: Call for antibiotic stewardship. Oral Surg. 2020. [Google Scholar] [CrossRef]
- Hocková, B.; Riad, A.; Valky, J.; Šulajová, Z.; Stebel, A.; Slávik, R.; Bečková, Z.; Pokorná, A.; Klugarová, J.; Klugar, M. Oral complications of ICU patients with COVID-19: Case-series and review of two hundred ten cases. J. Clin. Med. 2021, 10, 581. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Liang, G.; Liu, W. Fungal co-infections associated with global COVID-19 pandemic: A clinical and diagnostic perspective from China. Mycopathology 2020, 185, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Ahmadikia, K.; Mahmoudi, S.; Kalantari, S.; Jamalimoghadamsiahkali, S.; Izadi, A.; Kord, M.; Dehghan Manshadi, S.A.; Seifi, A.; Ghiasvand, F.; et al. Oropharyngeal candidiasis in hospitalised COVID-19 patients from Iran: Species identification and antifungal susceptibility pattern. Mycoses 2020, 63, 771–778. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; van de Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; Perlin, D.S.; Lass-Flörl, C.; Hoenigl, M. COVID-19 Associated Pulmonary Aspergillosis (CAPA)—From immunology to treatment. J. Fungi 2020, 6, 91. [Google Scholar] [CrossRef]
- Hussain, S.; Baxi, H.; Riad, A.; Klugarová, J.; Pokorná, A.; Slezáková, S.; Líčeník, R.; Najmi, A.K.; Klugar, M. COVID-19-Associated Mucormycosis (CAM): An updated evidence mapping. Int. J. Environ. Res. Public Health 2021, 18, 340. [Google Scholar] [CrossRef]
- Binder, U.; Maurer, E.; Lass-Flörl, C. Mucormycosis—From the pathogens to the disease. Clin. Microbiol. Infect. 2014, 20, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Jeong, W.; Keighley, C.; Wolfe, R.; Lee, W.L.L.; Slavin, M.A.A.; Kong, D.C.M.C.M.; Chen, S.C.-A.C.A. The epidemiology and clinical manifestations of mucormycosis: A systematic review and meta-analysis of case reports. Clin. Microbiol. Infect. 2019, 25, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. Epidemiology and diagnosis of mucormycosis: An update. J. Fungi 2020, 6, 265. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.; Singh, R. Mucormycosis in India: Unique features. Mycoses 2014, 57, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Prakash, H.; Ghosh, A.K.; Rudramurthy, S.M.; Paul, R.A.; Gupta, S.; Negi, V.; Chakrabarti, A. The environmental source of emerging Apophysomyces variabilis infection in India. Med. Mycol. 2016, 54, 567–575. [Google Scholar] [CrossRef] [Green Version]
- Skiada, A.; Pagano, L.; Groll, A.; Zimmerli, S.; Dupont, B.; Lagrou, K.; Lass-Florl, C.; Bouza, E.; Klimko, N.; Gaustad, P.; et al. Zygomycosis in Europe: Analysis of 230 cases accrued by the registry of the European Confederation of Medical Mycology (ECMM) Working Group on Zygomycosis between 2005 and 2007. Clin. Microbiol. Infect. 2011, 17, 1859–1867. [Google Scholar] [CrossRef] [Green Version]
- Chakrabarti, A.; Das, A.; Mandal, J.; Shivaprakash, M.R.; George, V.K.; Tarai, B.; Rao, P.; Panda, N.; Verma, S.C.; Sakhuja, V. The rising trend of invasive zygomycosis in patients with uncontrolled diabetes mellitus. Med. Mycol. 2006, 44, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaezi, A.; Moazeni, M.; Rahimi, M.T.; de Hoog, S.; Badali, H. Mucormycosis in Iran: A systematic review. Mycoses 2016, 59, 402–415. [Google Scholar] [CrossRef]
- Serris, A.; Danion, F.; Lanternier, F. Disease entities in mucormycosis. J. Fungi 2019, 5, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, R.E.; Kontoyiannis, D.P. Epidemiology and treatment of mucormycosis. Futur. Med. 2013, 8, 1163–1175. [Google Scholar] [CrossRef] [PubMed]
- Kuy, S.; He, C.; Cronin, D.C. Renal mucormycosis: A rare and potentially lethal complication of kidney transplantation. Case Rep. Transplant. 2013, 2013, 915423. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Lewis, R.E. How I treat mucormycosis. Blood 2011, 118, 1216–1224. [Google Scholar] [CrossRef]
- Cornely, O.A.; Arikan-Akdagli, S.; Dannaoui, E.; Groll, A.H.; Lagrou, K.; Chakrabarti, A.; Lanternier, F.; Pagano, L.; Skiada, A.; Akova, M.; et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of mucormycosis 2013. Clin. Microbiol. Infect. 2014, 20, 5–26. [Google Scholar] [CrossRef] [Green Version]
- Riley, T.T.; Muzny, C.A.; Swiatlo, E.; Legendre, D.P. Breaking the mold: A review of mucormycosis and current pharmacological treatment options. Ann. Pharmacother. 2016, 50, 747–757. [Google Scholar] [CrossRef]
- Rokkas, T. Gastrointestinal involvement in COVID-19: A systematic review and meta-analysis. Ann. Gastroenterol. 2020, 33, 355. [Google Scholar] [CrossRef]
- Abrams, J.Y.; Godfred-Cato, S.E.; Oster, M.E.; Chow, E.J.; Koumans, E.H.; Bryant, B.; Leung, J.W.; Belay, E.D. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with SARS-CoV-2: A systematic review. J. Pediatr. 2020, 226, 45–54.e1. [Google Scholar] [CrossRef]
- Al-Khanati, N.M.; Riad, A.; Sahloul, M.E.; Klugar, M. Aphthous-like stomatitis of COVID-19 patients. Braz. J. Oral Sci. 2020, 19, e201354. [Google Scholar] [CrossRef]
- Riad, A.; Kassem, I.; Badrah, M.; Klugar, M. The manifestation of oral mucositis in COVID-19 patients: A case-series. Dermatol. Ther. 2020, 33, e14479. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Boccuzzi, M.; Sagiroglu, D.; Klugar, M.; Krsek, M. Pediatric multisystem inflammatory syndrome temporally associated with SARS-CoV: Oral manifestations and implications. Int. J. Paediatr. Dent. 2020, 31, 35–36. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Kassem, I.; Badrah, M.; Klugar, M. Acute Parotitis as a Presentation of COVID-19? Oral Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.U.; Hanif, M.; Ali, M.J.; Haider, M.A.; Kherani, D.; Memon, G.M.; Karim, A.H.; Sattar, A. Neurological manifestations of COVID-19 (SARS-CoV-2): A review. Front. Neurol. 2020, 11, 518. [Google Scholar] [CrossRef]
- Wollina, U.; Karadağ, A.S.; Rowland-Payne, C.; Chiriac, A.; Lotti, T. Cutaneous signs in COVID-19 patients: A review. Dermatol. Ther. 2020, 33, e13549. [Google Scholar] [CrossRef]
- Wollina, U. Challenges of COVID-19 pandemic for dermatology. Dermatol. Ther. 2020, 33, e13430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riad, A.; Kassem, I.; Issa, J.; Badrah, M.; Klugar, M. Angular cheilitis of COVID-19 patients: A case-series and literature review. Oral Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Kassem, I.; Hockova, B.; Badrah, M.; Klugar, M. Tongue ulcers associated with SARS-CoV-2 infection: A case series. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Riad, A.; Kassem, I.; Hockova, B.; Badrah, M.; Klugar, M. Halitosis in COVID-19 patients. Spec. Care Dent. 2021, 41, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Klugar, M.; Krsek, M. COVID-19 Related oral manifestations, early disease features? Oral Dis. 2020. [Google Scholar] [CrossRef]
- Riad, A.; Kassem, I.; Stanek, J.; Badrah, M.; Klugarova, J.; Klugar, M. Aphthous stomatitis in COVID-19 patients: Case-series and literature review. Dermatol. Ther. 2021, 34, e14735. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal co-infection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, R.; Joshi, S.R.; Misra, A. Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102146. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; The Joanna Briggs Institute: Adelaide, SA, Australia, 2020. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; Allaire, A.; Aronson, J.; Carpenter, J.; Gagnier, J.; et al. The CARE guidelines: Consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013, 2013, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- W.M.A. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- SPSS Inc. IBM SPSS Statistics 27. Available online: https://www.ibm.com/support/pages/node/3006603 (accessed on 14 March 2021).
- Revannavar, S.M.; Supriya, P.; Samaga, L.; Vineeth, K. COVID-19 triggering mucormycosis in a susceptible patient: A new phenomenon in the developing world? BMJ Case Rep. 2021, 14, e241663. [Google Scholar] [CrossRef]
- Mehta, S.; Pandey, A. Rhino-orbital mucormycosis associated with COVID-19. Cureus 2020, 12, e10726. [Google Scholar] [CrossRef] [PubMed]
- Ravani, S.; Agrawal, G.; Leuva, P.; Modi, P.; Amin, K. Rise of the phoenix: Mucormycosis in COVID-19 times. Indian J. Ophthalmol. 2021, 69, 1563–1568. [Google Scholar] [CrossRef] [PubMed]
- Nehara, H.R.; Puri, I.; Singhal, V.; Ih, S.; Bishnoi, B.R.; Sirohi, P. Rhinocerebral mucormycosis in COVID-19 patient with diabetes a deadly trio: Case series from the north-western part of India. Indian J. Med. Microbiol. 2021, 39, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Garg, D.; Muthu, V.; Sehgal, I.S.; Ramachandran, R.; Kaur, H.; Bhalla, A.; Puri, G.D.; Chakrabarti, A.; Agarwal, R. Coronavirus Disease (COVID-19) Associated Mucormycosis (CAM): Case report and systematic review of literature. Mycopathologia 2021, 186, 289–298. [Google Scholar] [CrossRef]
- Hanley, B.; Naresh, K.N.; Roufosse, C.; Nicholson, A.G.; Weir, J.; Cooke, G.S.; Thursz, M.; Manousou, P.; Corbett, R.; Goldin, R.; et al. Histopathological findings and viral tropism in UK patients with severe fatal COVID-19: A post-mortem study. Lancet Microbe 2020, 1, e245–e253. [Google Scholar] [CrossRef]
- Dallalzadeh, L.O.; Ozzello, D.J.; Liu, C.Y.; Kikkawa, D.O.; Korn, B.S. Secondary infection with rhino-orbital cerebral mucormycosis associated with COVID-19. Int. J. Orbital Disord. Oculoplastic Lacrimal Surg. 2021, 1–4. [Google Scholar] [CrossRef]
- Werthman-Ehrenreich, A. Mucormycosis with orbital compartment syndrome in a patient with COVID-19. Am. J. Emerg. Med. 2021, 42, 264.e5–264.e8. [Google Scholar] [CrossRef] [PubMed]
- Placik, D.A.; Taylor, W.L.; Wnuk, N.M. Bronchopleural fistula development in the setting of novel therapies for acute respiratory distress syndrome in SARS-CoV-2 pneumonia. Radiol. Case Rep. 2020, 15, 2378–2381. [Google Scholar] [CrossRef] [PubMed]
- Alekseyev, K.; Didenko, L.; Chaudhry, B. Rhinocerebral Mucormycosis and COVID-19 Pneumonia. J. Med. Cases 2021, 12, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.K.; Ghazarian, Z.; Cendrowski, K.D.; Persichino, J.G. Pulmonary aspergillosis and mucormycosis in a patient with COVID-19. Med. Mycol. Case Rep. 2021, 32, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, A.; Jordan, A.; Olewiler, S.; Wehberg, K.; Cortes, M.; Jackson, B.R. A fatal case of rhizopus azygosporus pneumonia following COVID-19. J. Fungi 2021, 7, 174. [Google Scholar] [CrossRef] [PubMed]
- Maini, A.; Tomar, G.; Khanna, D.; Kini, Y.; Mehta, H.; Bhagyasree, V. Sino-orbital mucormycosis in a COVID-19 patient: A case report. Int. J. Surg. Case Rep. 2021, 82, 105957. [Google Scholar] [CrossRef]
- Khatri, A.; Chang, K.M.; Berlinrut, I.; Wallach, F. Mucormycosis after Coronavirus disease 2019 infection in a heart transplant recipient—Case report and review of literature. J. Mycol. Med. 2021, 31, 101125. [Google Scholar] [CrossRef]
- Do Monte Junior, E.S.; Dos Santos, M.E.L.; Ribeiro, I.B.; de Oliveira Luz, G.; Baba, E.R.; Hirsch, B.S.; Funari, M.P.; De Moura, E.G.H. Rare and fatal gastrointestinal mucormycosis (Zygomycosis) in a COVID-19 patient: A case report. Clin. Endosc. 2020, 53, 746–749. [Google Scholar] [CrossRef] [PubMed]
- Pasero, D.; Sanna, S.; Liperi, C.; Piredda, D.; Branca, G.P.; Casadio, L.; Simeo, R.; Buselli, A.; Rizzo, D.; Bussu, F.; et al. A challenging complication following SARS-CoV-2 infection: A case of pulmonary mucormycosis. Infection 2020, 49, 1055–1060. [Google Scholar] [CrossRef]
- Bellanger, A.P.; Navellou, J.C.; Lepiller, Q.; Brion, A.; Brunel, A.S.; Millon, L.; Berceanu, A. Mixed mold infection with Aspergillus fumigatus and Rhizopus microsporus in a severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) patient. Infect. Dis. Now 2021, 51, 633–635. [Google Scholar] [CrossRef]
- Karimi-Galougahi, M.; Arastou, S.; Haseli, S. Fulminant mucormycosis complicating coronavirus disease 2019 (COVID-19). Int. Forum Allergy Rhinol. 2021, 11, 1029–1030. [Google Scholar] [CrossRef] [PubMed]
- Veisi, A.; Bagheri, A.; Eshaghi, M.; Rikhtehgar, M.H.; Kanavi, M.R.; Farjad, R. Rhino-orbital mucormycosis during steroid therapy in COVID-19 patients: A case report. Eur. J. Ophthalmol. 2021, 11206721211009450. [Google Scholar] [CrossRef]
- Sungurtekin, H.; Sargin, F.; Akbulut, M.; Karaduman, S. Severe rhinocerebral mucormycosis case developed after COVID-19. J. Bacteriol. Parasitol. 2021, 12, 1000386. [Google Scholar]
- Waizel-Haiat, S.; Guerrero-Paz, J.A.; Sanchez-Hurtado, L.; Calleja-Alarcon, S.; Romero-Gutierrez, L. A case of fatal rhino-orbital mucormycosis associated with new onset diabetic ketoacidosis and COVID-19. Cureus 2021, 13, e13163. [Google Scholar] [CrossRef]
- Zurl, C.; Hoenigl, M.; Schulz, E.; Hatzl, S.; Gorkiewicz, G.; Krause, R.; Eller, P.; Prattes, J. Autopsy proven pulmonary mucormycosis due to rhizopus microsporus in a critically ill COVID-19 patient with underlying hematological malignancy. J. Fungi 2021, 7, 88. [Google Scholar] [CrossRef]
- Arana, C.; Ramírez, R.E.C.; Xipell, M.; Casals, J.; Moreno, A.; Herrera, S.; Bodro, M.; Cofan, F.; Diekmann, F.; Esforzado, N. Mucormycosis associated with COVID-19 in two kidney transplant patients. Transpl. Infect. Dis. 2021, e13652. [Google Scholar] [CrossRef]
- Sen, M.; Lahane, S.; Lahane, T.P.; Parekh, R.; Honavar, S.G. Mucor in a viral land: A tale of two pathogens. Indian J. Ophthalmol. 2021, 69, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Tabarsi, P.; Khalili, N.; Pourabdollah, M.; Naeini, A.S.; Ghorbani, J.; Abtahian, Z.; Askari, E. COVID-19 associated rhinosinusitis mucormycosis due to Rhizopus oryzae: A rare but potentially fatal infection occurring after treatment with corticosteroids. Am. J. Trop. Med. Hyg. 2021, 105, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Bayram, N.; Ozsaygılı, C.; Sav, H.; Tekin, Y.; Gundogan, M.; Pangal, E.; Cicek, A.; Özcan, İ. Susceptibility of severe COVID-19 patients to rhino-orbital mucormycosis fungal infection in different clinical manifestations. Jpn. J. Ophthalmol. 2021, 65, 515–525. [Google Scholar] [CrossRef]
- El-Kholy, N.A.; El-Fattah, A.M.A.; Khafagy, Y.W. Invasive fungal sinusitis in post COVID-19 patients: A new clinical entity. Laryngoscope 2021. [Google Scholar] [CrossRef]
- González-Calatayud, M.; Vargas-Ábrego, B.; Gutiérrez-Uvalle, G.E.; López-Romero, S.C.; González-Pérez, L.G.; Carranco-Martínez, J.A.; Raful-Zacarías-Ezzat, J.; Gracida-Mancilla, N.I. Observational study of the suspected or confirmed cases of SARS-CoV-2 infection needing emergency surgical intervention during the first months of the pandemic in a third level hospital: Case series. Ann. Med. Surg. 2020, 60, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Ashour, M.M.; Abdelaziz, T.T.; Ashour, D.M.; Askoura, A.; Saleh, M.I.; Mahmoud, M.S. Imaging spectrum of acute invasive fungal rhino-orbital-cerebral sinusitis in COVID-19 patients: A case series and a review of literature. J. Neuroradiol. 2021, 48, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Gutierrez, C.G.; Martinez, D.V.; Proud, K.C. A case report of COVID-19 associated pulmonary mucormycosis. Arch. Clin. Cases 2020, 7, 46–51. [Google Scholar] [CrossRef]
- Mekonnen, Z.K.; Ashraf, D.C.; Jankowski, T.; Grob, S.R.; Vagefi, M.R.; Kersten, R.C.; Simko, J.P.; Winn, B.J. Acute invasive rhino-orbital mucormycosis in a patient with COVID-19-associated acute respiratory distress syndrome. Ophthal. Plast. Reconstr. Surg. 2021, 37, E40–E42. [Google Scholar] [CrossRef] [PubMed]
- Meshram, H.S.; Kute, V.B.; Chauhan, S.; Desai, S. Mucormycosis in post-COVID-19 renal transplant patients: A lethal complication in follow-up. Transpl. Infect. Dis. 2021, e13663. [Google Scholar] [CrossRef]
- Pakdel, F.; Ahmadikia, K.; Salehi, M.; Tabari, A.; Jafari, R.; Mehrparvar, G.; Rezaie, Y.; Rajaeih, S.; Alijani, N.; Barac, A.; et al. Mucormycosis in patients with COVID-19: A cross-sectional descriptive multicentre study from Iran. Mycoses 2021, 64, 1238–1252. [Google Scholar] [CrossRef] [PubMed]
- Rabagliati, R.; Rodríguez, N.; Núñez, C.; Huete, A.; Bravo, S.; Garcia, P. COVID-19-associated mold infection in critically ill patients, Chile. Emerg. Infect. Dis. 2021, 27, 1454–1456. [Google Scholar] [CrossRef] [PubMed]
- Saldanha, M.; Reddy, R.; Vincent, M.J. Paranasal mucormycosis in COVID-19 patient. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–4. [Google Scholar] [CrossRef]
- Rao, R.; Shetty, A.P.; Nagesh, C.P. Orbital infarction syndrome secondary to rhino-orbital mucormycosis in a case of COVID-19: Clinico-radiological features. Indian J. Ophthalmol. 2021, 69, 1627–1630. [Google Scholar] [CrossRef]
- Krishna, D.S.; Raj, H.; Kurup, P.; Juneja, M. Maxillofacial infections in COVID-19 era-actuality or the unforeseen: 2 case reports. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–4. [Google Scholar] [CrossRef]
- Krishna, V.; Morjaria, J.; Jalandari, R.; Omar, F.; Kaul, S. Autoptic identification of disseminated mucormycosis in a young male presenting with cerebrovascular event, multi-organ dysfunction and COVID-19 infection. IDCases 2021, 25, e01172. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Gokhale, T.; Choudhury, S.S.; Deb, A.K. COVID-19 and orbital mucormycosis. Indian J. Ophthalmol. 2021, 69, 1002–1004. [Google Scholar] [CrossRef] [PubMed]
- Satish, D.; Joy, D.; Ross, A.B. Mucormycosis co-infection associated with global COVID-19: A case series from India. Int. J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 815–820. [Google Scholar] [CrossRef]
- Mishra, N.; Mutya, V.S.S.; Thomas, A.; Rai, G.; Reddy, B.; Mohanan, A.A.; Ray, S.; Thiruvengadem, A.V.; Siddini, V.; Hegde, R. A case series of invasive mucormycosis in patients with COVID-19 infection. Int. J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 867–870. [Google Scholar] [CrossRef]
- Moorthy, A.; Gaikwad, R.; Krishna, S.; Hegde, R.; Tripathi, K.K.; Kale, P.G.; Rao, P.S.; Haldipur, D.; Bonanthaya, K. SARS-CoV-2, uncontrolled diabetes and corticosteroids-an unholy trinity in invasive fungal infections of the maxillofacial region? A retrospective, multi-centric analysis. J. Maxillofac. Oral Surg. 2021, 20, 418–425. [Google Scholar] [CrossRef]
- Sharma, S.; Grover, M.; Bhargava, S.; Samdani, S.; Kataria, T. Post coronavirus disease mucormycosis: A deadly addition to the pandemic spectrum. J. Laryngol. Otol. 2021, 135, 442–447. [Google Scholar] [CrossRef]
- World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 14 March 2021).
- Australian Government, National Health and Medical Research Council. Australian Guidelines for the Clinical Care of People with COVID-19. Available online: https://www.clinicalguidelines.gov.au/register/australian-guidelines-clinical-care-people-covid-19 (accessed on 17 September 2020).
- Roden, M.M.; Zaoutis, T.E.; Buchanan, W.L.; Knudsen, T.A.; Sarkisova, T.A.; Schaufele, R.L.; Sein, M.; Sein, T.; Chiou, C.C.; Chu, J.H.; et al. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin. Infect. Dis. 2005, 41, 634–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restrepo, A.; Salazar, M.E.; Cano, L.E.; Price Stover, E.; Feldman, D.; Stevens, D.A. Estrogens inhibit mycelium-to-yeast transformation in the fungus Paracoccidioides brasiliensis: Implications for resistance of females to Paracoccidioidomycosis. Infect. Immun. 1984, 46, 346–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prakash, H.; Chakrabarti, A. Global epidemiology of mucormycosis. J. Fungi 2019, 5, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prakash, H.; Ghosh, A.K.; Rudramurthy, S.M.; Singh, P.; Xess, I.; Savio, J.; Pamidimukkala, U.; Jillwin, J.; Varma, S.; Das, A.; et al. A prospective multicenter study on mucormycosis in India: Epidemiology, diagnosis, and treatment. Med. Mycol. 2019, 57, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Dolatabadi, S.; Ahmadi, B.; Rezaei-Matehkolaei, A.; Zarrinfar, H.; Skiada, A.; Mirhendi, H.; Nashibi, R.; Niknejad, F.; Nazeri, M.; Rafiei, A.; et al. Mucormycosis in Iran: A six-year retrospective experience. J. Mycol. Med. 2018, 28, 269–273. [Google Scholar] [CrossRef]
- Stemler, J.; Hamed, K.; Salmanton-García, J.; Rezaei-Matehkolaei, A.; Gräfe, S.K.; Sal, E.; Zarrouk, M.; Seidel, D.; Khedr, R.A.; Ben-Ami, R.; et al. Mucormycosis in the Middle East and North Africa: Analysis of the FungiScope® registry and cases from the literature. Mycoses 2020, 63, 1060–1068. [Google Scholar] [CrossRef]
- Nithyanandam, S.; Jacob, M.S.; Battu, R.R.; Thomas, R.K.; Correa, M.A.; D’Souza, O. Rhino-orbito-cerebral mucormycosis. A retrospective analysis of clinical features and treatment outcomes. Indian J. Ophthalmol. 2003, 51, 231–236. [Google Scholar] [PubMed]
- Chander, J.; Kaur, M.; Singla, N.; Punia, R.P.S.; Singhal, S.K.; Attri, A.K.; Alastruey-Izquierdo, A.; Stchigel, A.M.; Cano-Lira, J.F.; Guarro, J. Mucormycosis: Battle with the deadly enemy over a five-year period in India. J. Fungi 2018, 4, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- How Common are Fungal Diseases? Leading International Fungal Education (LIFE): Cheshire, UK, 2019.
- Zaki, S.M.; Elkholy, I.M.; Elkady, N.A.; Abdel-Ghany, K. Mucormycosis in Cairo, Egypt: Review of 10 reported cases. Med. Mycol. 2014, 52, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 24 September 2021).
- Nicolás, F.E.; Murcia, L.; Navarro, E.; Navarro-Mendoza, M.I.; Pérez-Arques, C.; Garre, V. Mucorales species and macrophages. J. Fungi 2020, 6, 94. [Google Scholar] [CrossRef]
- Spellberg, B.; Edwards, J.; Ibrahim, A. Novel perspectives on mucormycosis: Pathophysiology, presentation, and management. Clin. Microbiol. Rev. 2005, 18, 556–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoenigl, M. Invasive fungal disease complicating coronavirus disease 2019: When it rains, it spores. Clin. Infect. Dis. 2021, 73, e1645–e1648. [Google Scholar] [CrossRef] [PubMed]
- Cunha, C.; Carvalho, A.; Esposito, A.; Bistoni, F.; Romani, L. DAMP signaling in fungal infections and diseases. Front. Immunol. 2012, 3, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szarpak, L.; Chirico, F.; Pruc, M.; Szarpak, L.; Dzieciatkowski, T.; Rafique, Z. Mucormycosis—A serious threat in the COVID-19 pandemic? J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef]
- Antoniadou, A. Outbreaks of zygomycosis in hospitals. Clin. Microbiol. Infect. 2009, 15, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holzel, H.; Macqueen, S.; MacDonald, A.; Alexander, S.; Campbell, C.K.; Johnson, E.M.; Warnock, D.W. Rhizopus microsporus in wooden tongue depressors: A major threat or minor inconvenience? J. Hosp. Infect. 1998, 38, 113–118. [Google Scholar] [CrossRef]
- Shorten, R.J.; Gillespie, S.H.; Sule, O.; Lipman, M.; McHugh, T.D. Molecular strain typing of M. tuberculosis isolates from a suspected outbreak involving a faulty bronchoscope. J. Hosp. Infect. 2005, 61, 86–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsuwaida, K. Primary cutaneous mucormycosis complicating the use of adhesive tape to secure the endotracheal tube. Can. J. Anesth. 2002, 49, 880–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. 1 | Case No. 2 | Case No. 3 | Case No. 4 | Case No. 5 | Case No. 6 | Case No. 7 | |
|---|---|---|---|---|---|---|---|
| Age, Gender | 56, Male | 61, Female | 66, Male | 52, Male | 58, Male | 68, Female | 47, Male |
| Anamnesis | Diabetes Mellitus | Diabetes Mellitus | Diabetes mellitus; chronic hypertension | Diabetes mellitus; cardiovascular disease | Diabetes mellitus | Diabetes mellitus; Stable angina | Healthy |
| Blood Glucose (I) | 350 mg/dL | 400 mg/dL | 320 mg/dL | 300 mg/dL | 450 mg/dL | 300 mg/dL | 160 mg/dL |
| Vaccinated | No | No | No | No | No | No | No |
| COVID-19 Symptoms | Fever; cough; shortness of breath, diarrhea | Fever; cough; SpO2: 85% | Fever; cough; diarrhea; SpO2: 80% | Fever; cough; shortness of breath; SpO2: 86% | Fever; shortness of breath; SpO2: 90% | Fever; cough; shortness of breath, diarrhea | Fever; cough; shortness of breath, diarrhea |
| COVID-19 Treatment | Azithromycin; dexamethasone; salbutamol sulphate (Farcolin); paracetamol; acetaminophen (Amol); enoxaparin sodium (Clexane); zinc | Azithromycin; dexamethasone; salbutamol sulphate (Farcolin); paracetamol; acetaminophen (Amol); enoxaparin sodium (Clexane); zinc | Azithromycin; dexamethasone; salbutamol sulphate (Farcolin); paracetamol; acetaminophen (Amol); enoxaparin sodium (Clexane); zinc | Azithromycin; dexamethasone; salbutamol sulphate (Farcolin); paracetamol; acetaminophen (Amol); enoxaparin sodium (Clexane); zinc | Azithromycin; dexamethasone; salbutamol sulphate (Farcolin); paracetamol; acetaminophen (Amol); enoxaparin sodium (Clexane); zinc | Azithromycin; dexamethasone; salbutamol sulphate (Farcolin); paracetamol; acetaminophen (Amol); enoxaparin sodium (Clexane); zinc | Azithromycin; dexamethasone; salbutamol sulphate (Farcolin); paracetamol; acetaminophen (Amol); enoxaparin sodium (Clexane); zinc |
| Onset (II) | After 4 days of COVID-19 recovery | After two weeks of COVID-19 recovery | After four weeks of COVID-19 recovery | After four weeks of COVID-19 recovery | After two weeks of COVID-19 diagnosis | After three days of COVID-19 diagnosis | After 18 days of COVID-19 diagnosis |
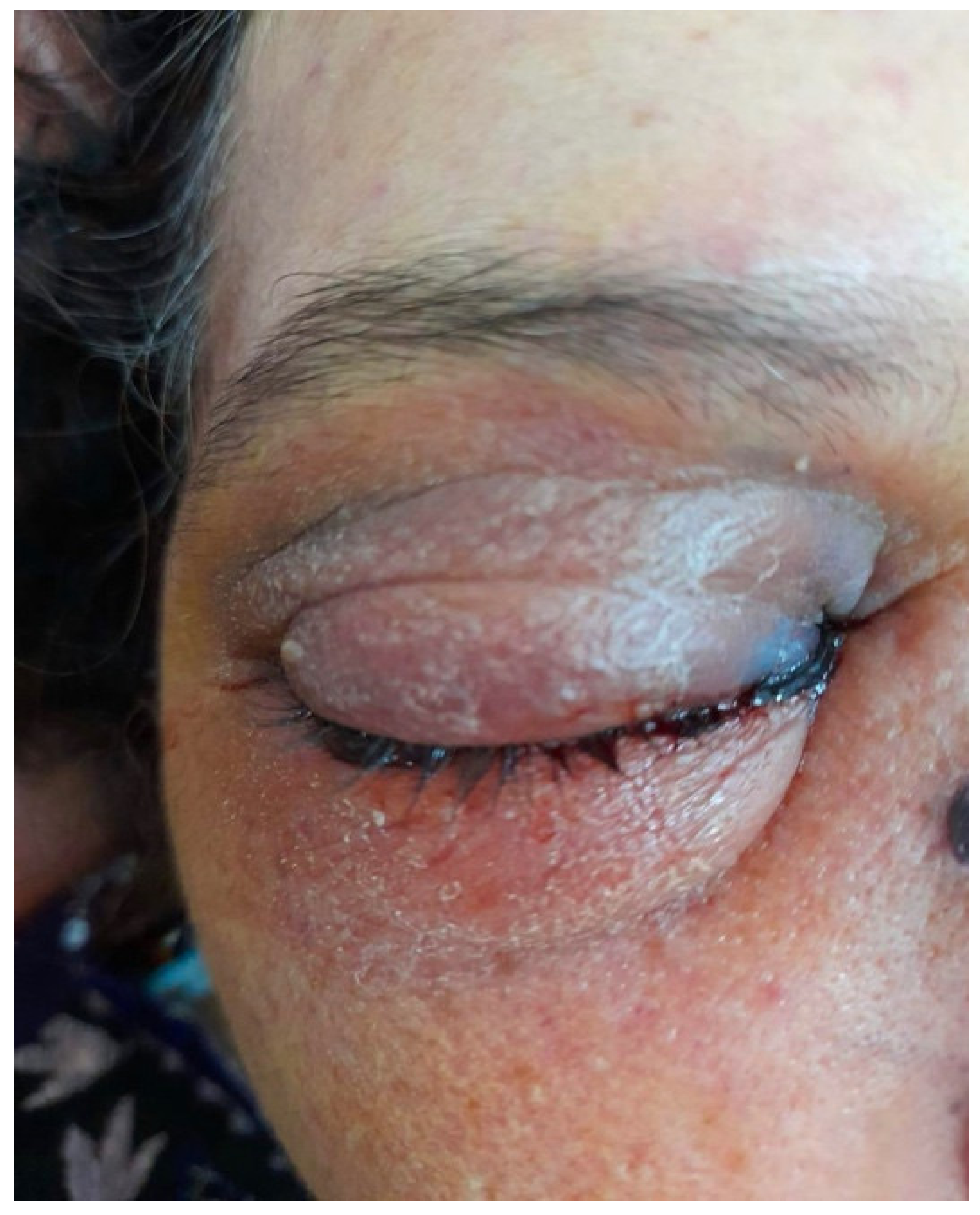
| Clinical Features | Fever; necrosis and ulceration of hard palate (Figure 1) | Fever; unilateral periorbital swelling (Figure 2) | Nasal stiffness; oral malodor; periorbital ulceration; nasal sidewalls discolouration | Nasal sidewalls ulceration and necrosis | Fever; periorbital cellulitis | GCS deterioration | Dyspnea, GCS deterioration; oral fungus; periorbital discoloration |
| Neurologic Symptoms | Slurred speech; perioral numbness | Slurred speech; seizure; periorbital numbness | Numbness in the affected side of the face; lethargy | Slurred speech; periorbital numbness | No neurologic symptoms were reported | Seizure; coma | Seizure; coma |
| Mucormycosis | Rhino-cerebral | Rhino-cerebral | Rhino-cerebral | Rhino-cerebral | Rhino-cerebral | Rhino-cerebral | Rhino-cerebral |
| Radiographic Features | CBCT: Hypertrophied nasal conchae; opacified maxillary sinus; and irregular palatal destruction (Figure 2) | CT: Hypertrophied nasal conchae; sinus involvement with opacification; and bony erosions | CT: Facial bone destruction (Figure 3); sequestration with empty osteocytic lacunae | CT: Hypertrophied nasal conchae; sinus involvement and bilateral destruction of the maxillary sinus | CT: Sinusoidal sinus abscess invaded the orbital bone compressing the optic nerve (Figure 1) | CT: invasive sinusitis with opacities and bony erosion in the anterior wall; | CBCT: CT showed hypertrophied nasal conchae, sinus involved with opacities and bony erosion in the anterior wall; |
| Microbiologic Features | Palatal Specimen Biopsy: ribbon-like spores; branching and non-septate bends; angiodestruction (Figure 3) | Biopsy Specimen: ribbon-like spores; branching and non-septate bends; angiodestruction, areas of bony sequestration with empty osteocytic lacunae. | Biopsy Specimen: ribbon-like spores; branching and non-septate bends; angiodestruction, areas of bony | Biopsy specimen: ribbon-like spores; branching and granulation tissue infiltrated with inflammatory | N/A | RT-PCR: positive for Mucorales | RT-PCR: positive for Mucorales |
| Hospitalised | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Treatment | Hospitalisation; LAmB (4 mg/kg/day); and surgical debridement | Hospitalisation; LAmB (4 mg/kg/day); and surgical debridement | Hospitalisation; LAmB (4 mg/kg/day); surgical debridement; and soft tissue laser to improve healing | Hospitalisation; LAmB (4 mg/kg/day); surgical debridement; and soft tissue laser to improve healing | Hospitalisation; LAmB (4 mg/kg/day); and surgical debridement | Hospitalisation; LAmB (4 mg/kg/day) | Hospitalisation; LAmB (4 mg/kg/day) |
| Follow-up | 4 weeks | 6 weeks | 5 weeks | 4 weeks | 5 weeks | 4 weeks | 4 weeks |
| Outcome | Improved | Improved | Improved | Stable | Stable | Improved | Improved |
| Variable | Outcome | Reported Frequency (n) | Valid Percentage (%) |
|---|---|---|---|
| Study Design | Case Report | 29 | 70.7 |
| Case Series | 11 | 26.8 | |
| Cross-sectional | 1 | 2.4 | |
| Gender | Female | 34 | 25.6 |
| Male | 99 | 74.4 | |
| Age | ≤55 years-old | 56 | 51.4 |
| >55 years-old | 53 | 48.6 | |
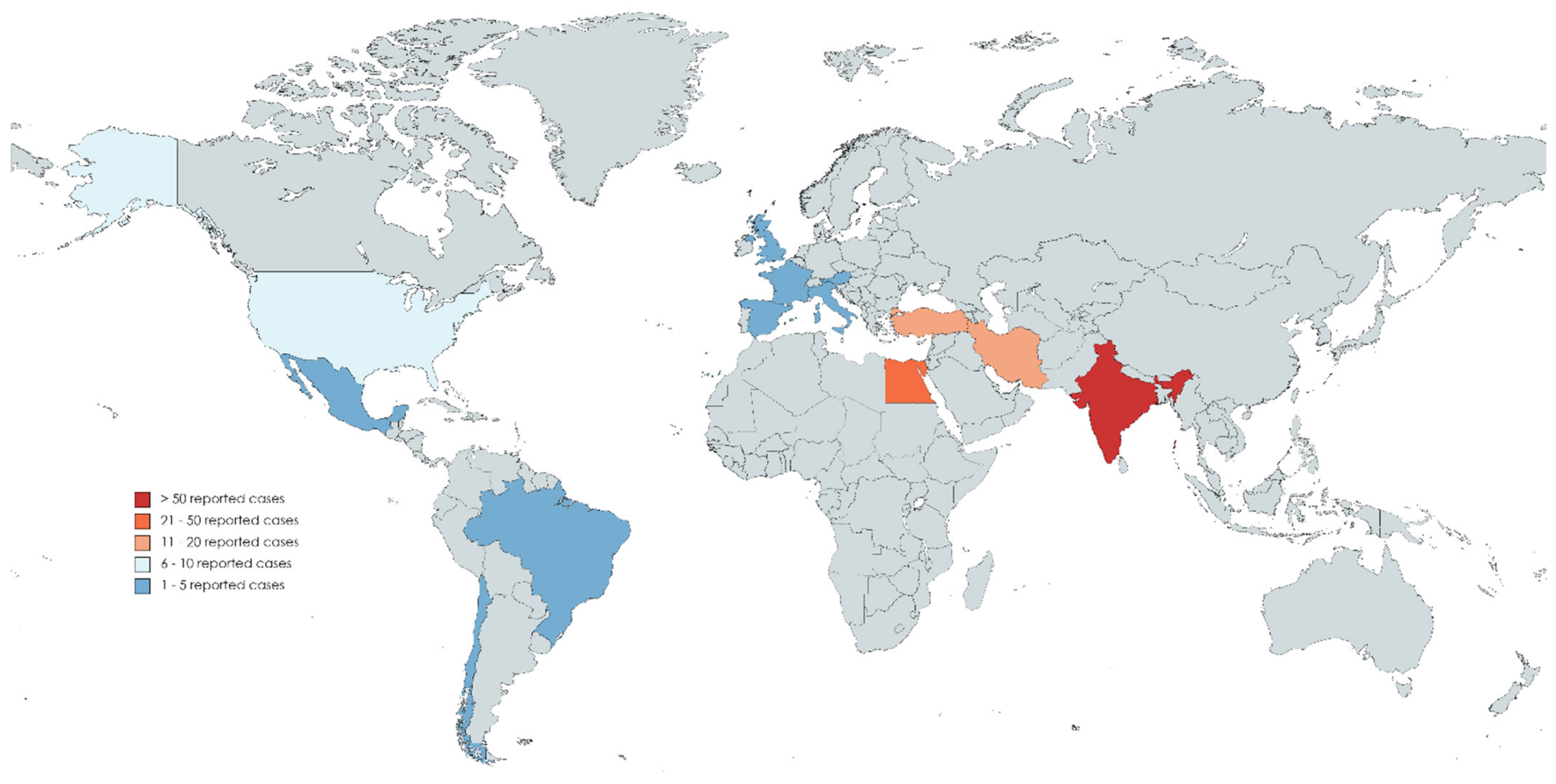
| Country | Austria | 1 | 0.5 |
| Brazil | 1 | 0.5 | |
| Chile | 1 | 0.5 | |
| Egypt | 34 | 17.8 | |
| France | 1 | 0.5 | |
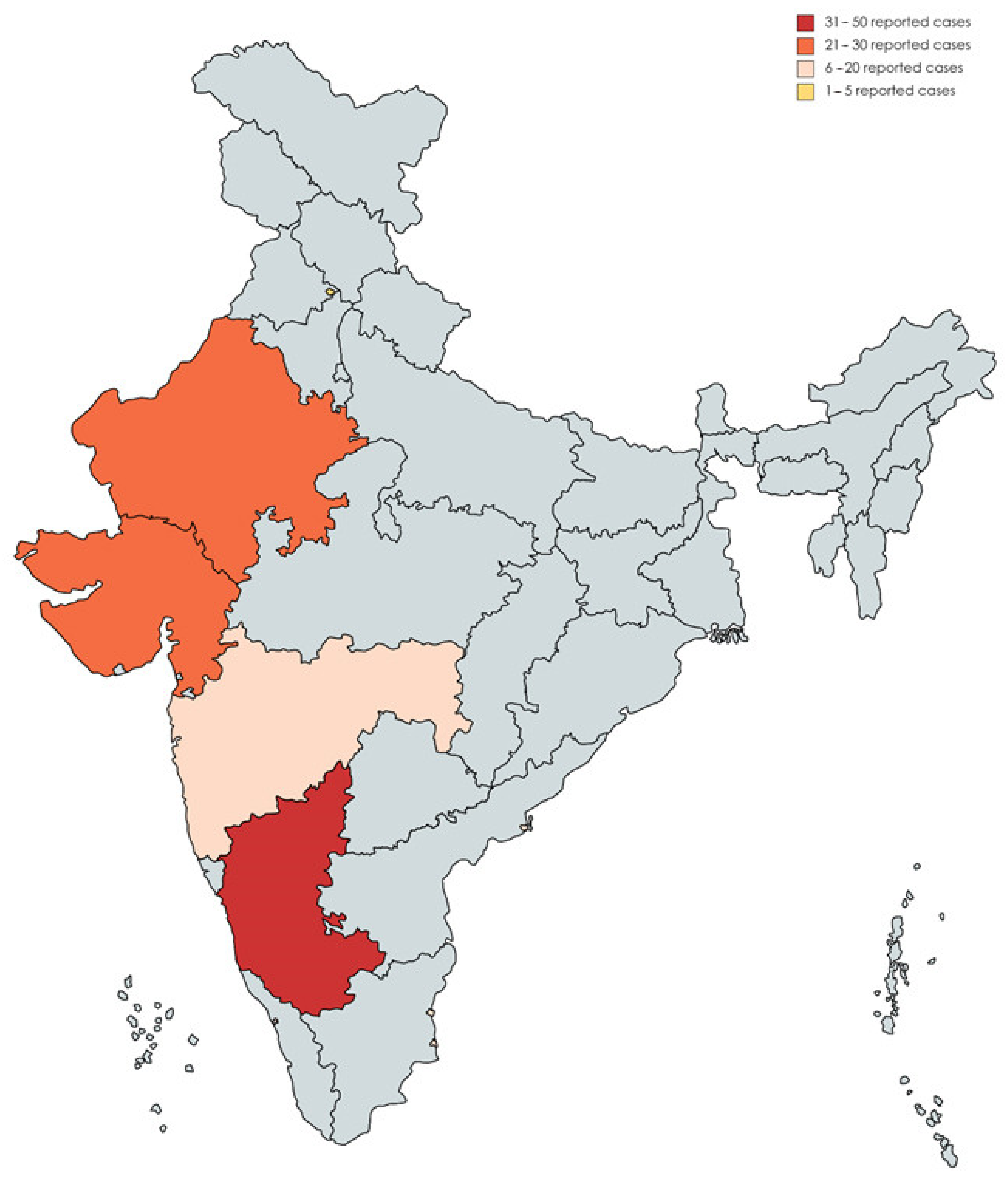
| India | 106 | 55.5 | |
| Iran | 19 | 9.9 | |
| Italy | 1 | 0.5 | |
| Mexico | 2 | 1 | |
| Spain | 2 | 1 | |
| Turkey | 12 | 6.3 | |
| UK | 2 | 1 | |
| USA | 9 | 4.7 | |
| Economic Rank | Low income | 0 | 0 |
| Lower-middle income | 159 | 83.2 | |
| Upper-middle income | 15 | 7.9 | |
| High income | 17 | 8.9 |
| Variable | Outcome | Reported Frequency (n) | Valid Percentage (%) |
|---|---|---|---|
| Comorbidities | Diabetes Mellitus | 87 | 79.1 |
| Chronic Hypertension | 33 | 30 | |
| Renal Disease/Failure | 15 | 13.6 | |
| Cardiovascular Disease | 11 | 10 | |
| Thyroid Disease | 6 | 5.5 | |
| Asthma | 4 | 3.6 | |
| Hematologic Malignancy | 4 | 3.6 | |
| Organ Transplantation | 3 | 2.7 | |
| Anxiety Disorder | 2 | 1.8 | |
| Hepatic Disease | 2 | 1.8 | |
| Cerebral Infraction | 1 | 0.9 | |
| Chronic Obstructive Pulmonary Disease | 1 | 0.9 | |
| Hyperlipidemia | 1 | 0.9 | |
| Myelodysplastic Syndrome | 1 | 0.9 | |
| Tuberculosis | 1 | 0.9 | |
| Total | 100 | 90.9 | |
| COVID-19 Severity | Mild | 9 | 18.4 |
| Moderate | 13 | 26.5 | |
| Severe | 20 | 40.8 | |
| Critic | 7 | 14.3 | |
| Not Reported | 61 | 55.5 | |
| COVID-19 Medication | Steroids | 71 | 64.5 |
| Remdesivir | 20 | 18.2 | |
| Antibiotics | 14 | 12.7 | |
| Tocilizumab | 6 | 5.5 | |
| Oseltamivir | 3 | 2.7 | |
| Lopinavir/Ritonavir | 2 | 1.8 | |
| Hydroxychloroquine | 2 | 1.8 |
| Variable | Outcome | Reported Frequency (n) | Valid Percentage (%) |
|---|---|---|---|
| Side | Unilateral | 81 | 90 |
| Bilateral | 9 | 10 | |
| Location | Orbits | 80 | 74.8 |
| Paranasal Sinuses | 77 | 72 | |
| Central Nervous System | 22 | 20.4 | |
| Nasal Cavity | 20 | 18.5 | |
| Lung | 10 | 9.3 | |
| Palate | 2 | 1.9 | |
| Heart | 1 | 0.9 | |
| Gastrointestinal Tract | 1 | 0.9 | |
| Kidney | 1 | 0.9 | |
| Limb | 1 | 0.9 | |
| Signs and Symptoms | Loss/Decrease of Vision | 48 | 44.4 |
| Ptosis | 45 | 41.7 | |
| Facial Edema | 32 | 29.6 | |
| Necrotic Tissue | 30 | 27.8 | |
| Ophthalmoplegia | 19 | 17.6 | |
| Sinusitis | 17 | 15.7 | |
| Palatal Eschar | 14 | 13 | |
| Fixed/Decreased Pupil/Ocular Movement | 13 | 12 | |
| Chemosis | 11 | 10.2 | |
| Rhinorrhea | 4 | 3.7 | |
| Ulceration | 3 | 2.8 | |
| Pus | 3 | 3.2 | |
| Diplopia | 1 | 0.9 | |
| Facial Cellulitis | 1 | 0.9 |
| Variable | Outcome | Reported Frequency (n) | Valid Percentage (%) |
|---|---|---|---|
| Method | Biopsy | 103 | 93.6 |
| CBCT/CT/MRI | 100 | 90.9 | |
| Histopathology | 7 | 6.4 | |
| Autopsy | 3 | 2.7 | |
| Genus | Mucor | 32 | 54.2 |
| Rhizopus | 23 | 39 | |
| Aspergillus | 5 | 8.5 | |
| Lichtheimia | 2 | 3.4 | |
| Not Reported | 59 | 53.6 |
| Variable | Outcome | Reported Frequency (n) | Valid Percentage (%) |
|---|---|---|---|
| Surgical Intervention | Yes | 81 | 77.9 |
| No | 23 | 22.1 | |
| Not Reported | 6 | 5.5 | |
| Medication | Amphotericin B | 99 | 92.5 |
| Posaconazole | 5 | 4.7 | |
| Isavuconazole | 4 | 3.7 | |
| Voriconazole | 2 | 1.9 | |
| Itraconazole | 1 | 0.9 | |
| Not Reported | 3 | 2.7 | |
| Outcome | Improved | 52 | 48.1 |
| Unchanged | 6 | 5.6 | |
| Death | 50 | 46.3 | |
| Not Reported | 2 | 1.8 |
| Variable | Outcome | Mortality (n = 50) | Survival (n = 58) | Sig. |
|---|---|---|---|---|
| Gender | Female | 11 (22%) | 15 (25.9%) | 0.640 |
| Male | 39 (78%) | 43 (74.1%) | ||
| Age | ≤55 years-old | 29 (58%) | 28 (48.3%) | 0.272 |
| >55 years-old | 21 (42%) | 30 (51.7%) | ||
| Economy | Low and Lower-middle Income | 26 (52%) | 50 (86.2%) | <0.001 |
| Upper-middle and High Income | 24 (48%) | 8 (13.8%) | ||
| Comorbidities | Diabetes | 34 (68%) | 51 (87.9%) | 0.012 |
| Chronic Hypertension | 16 (32%) | 17 (29.3%) | 0.762 | |
| Renal Disease/Failure | 8 (16%) | 7 (12.1%) | 0.556 | |
| Cardiovascular Disease | 5 (10%) | 6 (10.3%) | 0.953 | |
| Thyroid Disease | 3 (6%) | 3 (5.2%) | 1.000 * | |
| Asthma | 3 (6%) | 1 (1.7%) | 0.334 * | |
| Hematologic Malignancy | 3 (6%) | 1 (1.7%) | 0.334 * | |
| Organ Transplantation | 1 (2%) | 2 (3.4%) | 1.000 * | |
| Total | 45 (90%) | 53 (91.4%) | 1.000 * | |
| COVID-19 Medication | Steroids | 32 (64%) | 38 (65.5%) | 0.869 |
| Remdesivir | 8 (16%) | 12 (20.7%) | 0.532 | |
| Antibiotics | 8 (16%) | 6 (10.3%) | 0.383 | |
| Tocilizumab | 4 (8%) | 2 (3.4%) | 0.412 * | |
| Total | 37 (82.2%) | 41 (87.2%) | 0.503 | |
| Onset | Concurrent (0 days) | 16 (37.2%) | 27 (62.8%) | 0.174 |
| Latent (≥ 1 day) | 29 (50.9%) | 28 (49.1%) | ||
| Side | Unilateral | 35 (44.3%) | 44 (55.7%) | 0.294 * |
| Bilateral | 6 (66.7%) | 3 (33.3%) | ||
| Location | Orbits | 33 (68.8%) | 45 (78.9%) | 0.234 |
| Paranasal Sinuses | 31 (64.6%) | 44 (77.2%) | 0.154 | |
| Central Nervous System | 11 (22.9%) | 11 (19%) | 0.618 | |
| Nasal Cavity | 4 (8.3%) | 16 (27.6%) | 0.012 | |
| Lung | 8 (16.7%) | 2 (3.4%) | 0.041 * | |
| Palate | 0 (0%) | 2 (3.4%) | 0.500 * | |
| Signs and Symptoms | Loss/Decrease of Vision | 18 (37.5%) | 29 (50%) | 0.197 |
| Ptosis | 22 (45.8%) | 22 (37.9%) | 0.411 | |
| Facial Edema | 13 (27%) | 18 (31%) | 0.656 | |
| Necrotic Tissue | 15 (31.3%) | 15 (25.9%) | 0.540 | |
| Ophthalmoplegia | 10 (20.8%) | 9 (15.5%) | 0.478 | |
| Sinusitis | 6 (12.5%) | 11 (19%) | 0.367 | |
| Palatal Eschar | 6 (12.5%) | 8 (13.8%) | 0.845 | |
| Fixed/Decreased Pupil/Ocular Movement | 6 (12.5%) | 6 (10.3%) | 0.727 | |
| Chemosis | 3 (6.3%) | 7 (12.1%) | 0.343 * | |
| Diagnosis Method | Biopsy | 45 (91.8%) | 57 (98.3%) | 0.177 * |
| CBCT/CT/MRI | 48 (98%) | 50 (96.2%) | 1.000 * | |
| Histopathology | 1 (2%) | 6 (10.3%) | 0.122 * | |
| Genus | Mucor | 14 (50%) | 18 (58.1%) | 0.535 |
| Rhizopus | 12 (42.9%) | 11 (35.5%) | 0.562 | |
| Surgical Intervention | Yes | 35 (44.3%) | 44 (55.7%) | 0.302 |
| No | 13 (56.5%) | 10 (43.5%) | ||
| Mucormycosis Medication | Amphotericin B | 43 (89.6%) | 55 (96.5%) | 0.242 * |
| Posaconazole | 1 (2.1%) | 4 (7%) | 0.372 * | |
| Isavuconazole | 1 (2.1%) | 3 (5.3%) | 0.623 * | |
| Voriconazole | 1 (2.1%) | 1 (1.8%) | 1.000 * | |
| Itraconazole | 0 (0%) | 1 (1.7%) | 1.000 * |
| CAM Mortality Risk Factor (Predictor) | B (SE) | OR (CI 95%) | Sig. | |
|---|---|---|---|---|
| Economy | Upper-middle and High Income | 1.753 (0.474) | 5.769 (2.276–14.622) | <0.001 |
| Comorbidities | Diabetes | −1.232 (0.504) | 0.292 (0.109–0.784) | 0.015 |
| Location | Nasal Cavity | −1.433 (0.599) | 0.239 (0.074–0.772) | 0.017 |
| Lung | 1.723 (0.817) | 5.600 (1.129–27.785) | 0.035 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riad, A.; Shabaan, A.A.; Issa, J.; Ibrahim, S.; Amer, H.; Mansy, Y.; Kassem, I.; Kassem, A.B.; Howaldt, H.-P.; Klugar, M.; et al. COVID-19-Associated Mucormycosis (CAM): Case-Series and Global Analysis of Mortality Risk Factors. J. Fungi 2021, 7, 837. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7100837
Riad A, Shabaan AA, Issa J, Ibrahim S, Amer H, Mansy Y, Kassem I, Kassem AB, Howaldt H-P, Klugar M, et al. COVID-19-Associated Mucormycosis (CAM): Case-Series and Global Analysis of Mortality Risk Factors. Journal of Fungi. 2021; 7(10):837. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7100837
Chicago/Turabian StyleRiad, Abanoub, Alshaimaa Ahmed Shabaan, Julien Issa, Sally Ibrahim, Hatem Amer, Yossef Mansy, Islam Kassem, Amira Bisher Kassem, Hans-Peter Howaldt, Miloslav Klugar, and et al. 2021. "COVID-19-Associated Mucormycosis (CAM): Case-Series and Global Analysis of Mortality Risk Factors" Journal of Fungi 7, no. 10: 837. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7100837