
Persistent Organic Pollutants in Austrian Human Breast Milk Collected between 2013 and 2016
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples and Study Populations
2.1.1. Pilot Study
2.1.2. Follow-Up Study
2.1.3. WHO/UNEP Breast Milk Monitoring Programme
2.2. Chemical Analysis
2.2.1. Analysis of PBDE Congeners (Pilot Study)
2.2.2. Analysis of PFASs (Pilot Study)
2.2.3. Analysis of PFASs (Follow-Up Study)
2.2.4. Analyses of POPs
2.3. Statistical Analysis
2.4. Estimation of Daily Intakes in Infants
3. Results and Discussion
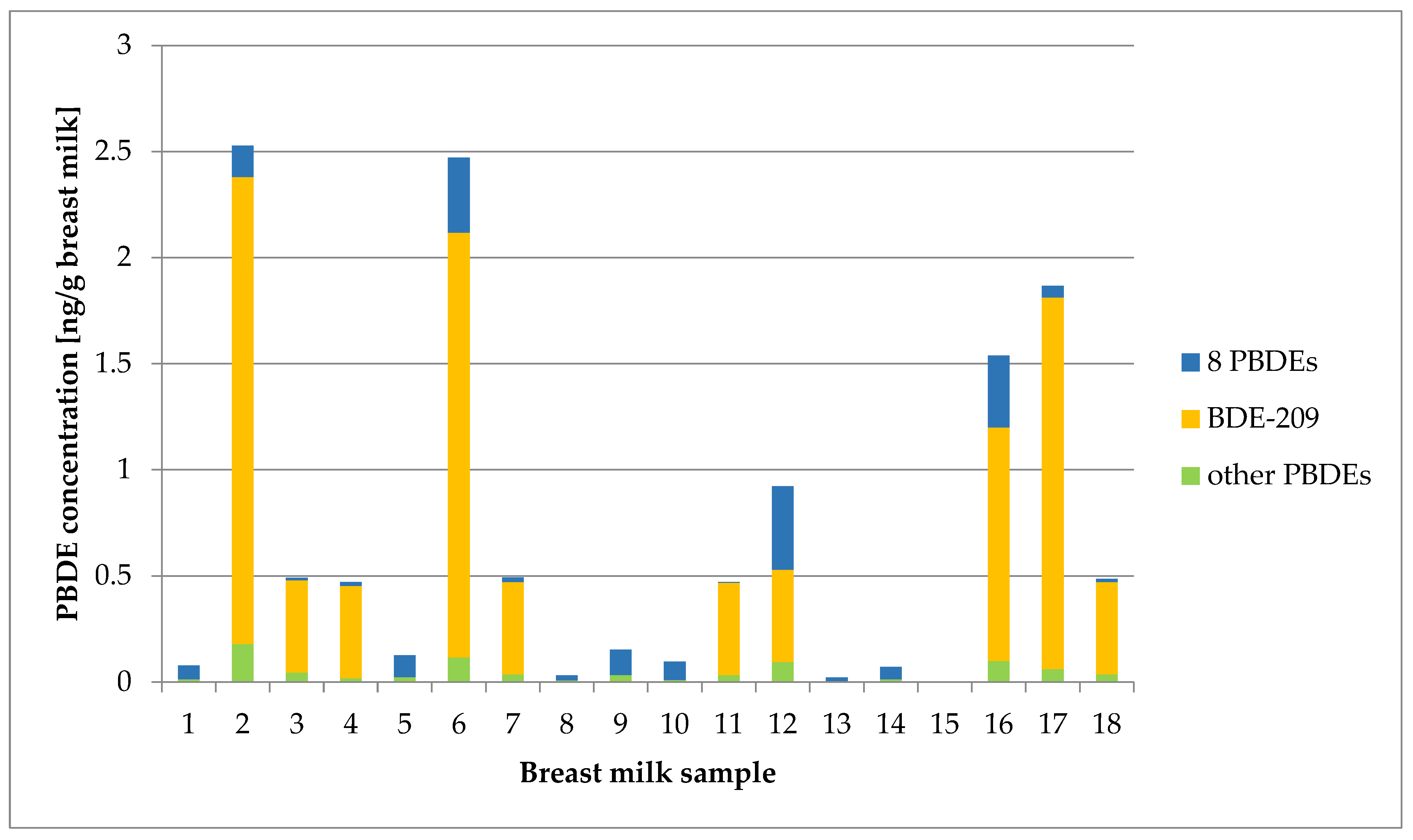
3.1. PBDE Congener Levels
3.1.1. Exposure
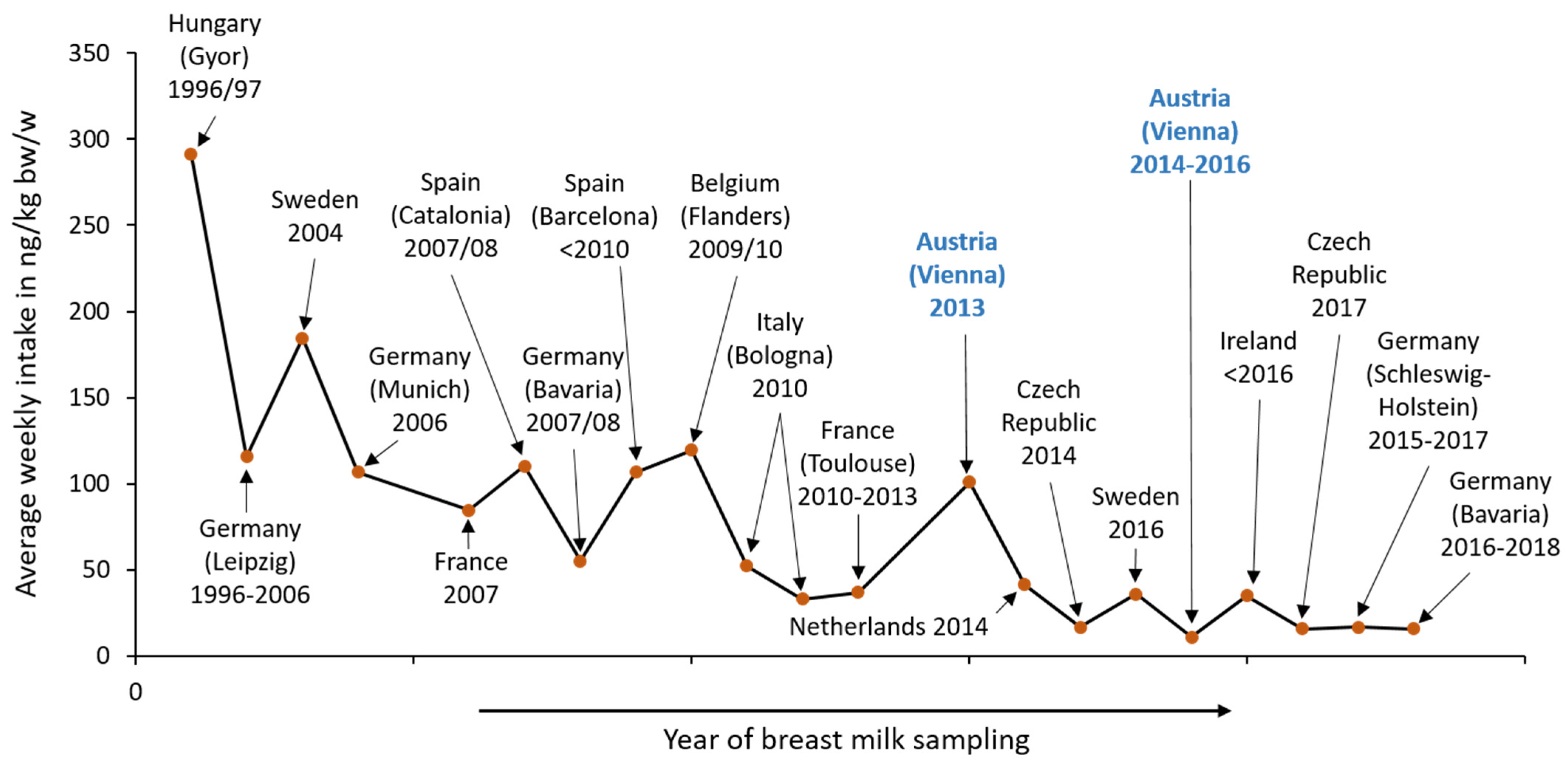
3.1.2. European Studies on PBDEs in Human Breast Milk
3.1.3. Associations with Individual Exposure Data and Health Parameters
3.1.4. Risk Assessment for PBDEs
3.2. PFAS Levels
3.2.1. Exposure
3.2.2. European Studies on PFASs in Human Breast Milk
3.2.3. Risk Assessment for PFAS
3.3. POPs Levels
3.3.1. Exposure
3.3.2. Declining Trends of POPs in Europe
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grummer-Strawn, L.M.; Rollins, N. Summarising the health effects of breastfeeding. Acta Paediatr. 2015, 104, 1–2. [Google Scholar] [CrossRef] [PubMed]
- WHO. Breastfeeding; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/health-topics/breastfeeding#tab=tab_1 (accessed on 2 March 2023).
- ECHA. Understanding POPs; European Chemical Agency: Helsinki, Finland, 2022; Available online: https://echa.europa.eu/en/understanding-pops (accessed on 22 December 2022).
- UNEP. Persistent Organic Pollutants (POPs); United Nations Environment Programme: Nairobi, Kenya, 2022; Available online: https://www.unep.org/explore-topics/chemicals-waste/what-we-do/persistent-organic-pollutants-pops (accessed on 13 November 2022).
- Fenton, S.E.; Ducatman, A.; Boobis, A.; DeWitt, J.C.; Lau, C.; Ng, C.; Smith, J.S.; Roberts, S.M. Per- and Polyfluoroalkyl Substance Toxicity and Human Health Review: Current State of Knowledge and Strategies for Informing Future Research. Environ. Toxicol. Chem. 2021, 40, 606–630. [Google Scholar] [CrossRef] [PubMed]
- Croes, K.; Colles, A.; Koppen, G.; Govarts, E.; Bruckers, L.; van de Mieroop, E.; Nelen, V.; Covaci, A.; Dirtu, A.C.; Thomsen, C.; et al. Persistent organic pollutants (POPs) in human milk: A biomonitoring study in rural areas of Flanders (Belgium). Chemosphere 2012, 89, 988–994. [Google Scholar] [CrossRef] [PubMed]
- UNEP. Results of the Global Survey on Concentrations in Human Milk of Persistent Organic Pollutants by the United Nations Environment Programme and the World Health Organization; United Nations Environment Programme: Nairobi, Kenya, 2013; Available online: https://www.informea.org/en/results-global-survey-concentrations-human-milk-persistent-organic-pollutants-united-nations (accessed on 15 June 2023).
- Frederiksen, M.; Vorkamp, K.; Thomsen, M.; Knudsen, L.E. Human internal and external exposure to PBDEs—A review of levels and sources. Int. J. Hyg. Environ. Health 2009, 212, 109–134. [Google Scholar] [CrossRef] [PubMed]
- La Guardia, M.J.; Hale, R.C.; Harvey, E. Detailed polybrominated diphenyl ether (PBDE) congener composition of the widely used penta-, octa-, and deca-PBDE technical flame-retardant mixtures. Environ. Sci. Technol. 2006, 40, 6247–6254. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, P.; Viberg, H.; Jakobsson, E.; Orn, U.; Fredriksson, A. A brominated flame retardant, 2,2′,4,4′,5-pentabromodiphenyl ether: Uptake, retention, and induction of neurobehavioral alterations in mice during a critical phase of neonatal brain development. Toxicol. Sci. 2002, 67, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Akortia, E.; Okonkwo, J.O.; Lupankwa, M.; Osae, S.D.; Daso, A.P.; Olukunle, O.I.; Chaudhary, A. A review of sources, levels, and toxicity of polybrominated diphenyl ethers (PBDEs) and their transformation and transport in various environmental compartments. Environ. Rev. 2016, 24, 253–273. [Google Scholar] [CrossRef]
- Besis, A.; Samara, C. Polybrominated diphenyl ethers (PBDEs) in the indoor and outdoor environments—A review on occurrence and human exposure. Environ. Pollut. 2012, 169, 217–229. [Google Scholar] [CrossRef]
- Fromme, H.; Becher, G.; Hilger, B.; Völkel, W. Brominated flame retardants—Exposure and risk assessment for the general population. Int. J. Hyg. Environ. Health 2016, 219, 1–23. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, W.; Song, J.; Ren, Z.; Yuan, H.; Yan, H.; Zhang, J.; Pei, Z.; He, Z. Environmental Characteristics of Polybrominated Diphenyl Ethers in Marine System, with Emphasis on Marine Organisms and Sediments. Biomed. Res. Int. 2016, 2016, 1317232. [Google Scholar] [CrossRef]
- Jakobsson, K.; Fång, J.; Athanasiadou, M.; Rignell-Hydbom, A.; Bergman, A. Polybrominated diphenyl ethers in maternal serum, umbilical cord serum, colostrum and mature breast milk. Insights from a pilot study and the literature. Environ. Int. 2012, 47, 121–130. [Google Scholar] [CrossRef]
- Klinčić, D.; Dvoršćak, M.; Jagić, K.; Mendaš, G.; Herceg Romanić, S. Levels and distribution of polybrominated diphenyl ethers in humans and environmental compartments: A comprehensive review of the last five years of research. Environ. Sci. Pollut. Res. Int. 2020, 27, 5744–5758. [Google Scholar] [CrossRef]
- Mannetje, A.; Coakley, J.; Mueller, J.F.; Harden, F.; Toms, L.-M.; Douwes, J. Partitioning of persistent organic pollutants (POPs) between human serum and breast milk: A literature review. Chemosphere 2012, 89, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Zhai, J.X. Distribution of polybrominated diphenyl ethers in breast milk, cord blood and placentas: A systematic review. Environ. Sci. Pollut. Res. Int. 2017, 24, 21548–21573. [Google Scholar] [CrossRef] [PubMed]
- Gill, U.; Chu, I.; Ryan, J.J.; Feeley, M. Polybrominated diphenyl ethers: Human tissue levels and toxicology. Rev. Environ. Contam. Toxicol. 2004, 183, 55–97. [Google Scholar] [CrossRef] [PubMed]
- Linares, V.; Bellés, M.; Domingo, J.L. Human exposure to PBDE and critical evaluation of health hazards. Arch. Toxicol. 2015, 89, 335–356. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Scientific Opinion on Polybrominated Diphenyl Ethers (PBDEs) in Food. European Food Safety Authority. EFSA J. 2011, 9, 2156. [Google Scholar] [CrossRef]
- Stockholm Convention. All POPs Listed in the Stockholm Convention; Stockholm Convention: Stockholm, Sweden, 2023; Available online: https://chm.pops.int/TheConvention/ThePOPs/ListingofPOPs/tabid/2509/Default.aspx (accessed on 15 June 2023).
- EFSA. Scientific Opinion Risk to Human Health Related to the Presence of Perfluoroalkyl Substances in Food. Eur. Food Saf. Auth. J. 2020, 18, 6223. [Google Scholar] [CrossRef]
- OECD. Reconciling Terminology of the Universe of Per- and Polyfluoroalkyl Substances: Recommendations and Practical Guidance; OECD Environment, Organisation for Economic Co-operation and Development. Health Saf. Publ. Ser. Risk Manag. 2021, 61, 1–34. Available online: https://one.oecd.org/document/ENV/CBC/MONO(2021)25/en/pdf (accessed on 2 July 2023).
- OECD. Toward a New Comprehensive Global Database of Per- and Polyfluoroalkyl Substances (PFASs): Summary Report on Updating the OECD, 2007 List of Per- and Polyfluoroalkyl Substances (PFASs); Series on Risk Management 39; Organisation for Economic Co-operation and Development: Paris, France, 2018; Available online: https://one.oecd.org/document/ENV/JM/MONO(2018)7/en/pdf (accessed on 2 July 2023).
- Buck, R.C.; Franklin, J.; Berger, U.; Conder, J.M.; Cousins, I.T.; Voogt, P.; de Jensen, A.A.; Kannan, K.; Mabury, S.A.; van Leeuwen, S.P.J. Perfluoroalkyl and polyfluoroalkyl substances in the environment: Terminology, classification, and origins. Integr. Environ. Assess. Manag. 2011, 7, 513–541. [Google Scholar] [CrossRef]
- EFSA. Perfluorooctane sulfonate (PFOS), perfluorooctanoic acid (PFOA) and their salts. Scientific Opinion of the Panel on Contaminants in the Food chain. Eur. Food Saf. Auth. EFSA J. 2008, 653, 1–131. [Google Scholar] [CrossRef]
- Haug, L.S.; Becher, G. Biomarkers of Exposure: Perfluoroalkyl Compounds. In Biomarkers and Human Biomonitoring; Chapter 3B; Knudsen, L., Merlo, D.F., Eds.; Royal Society of Chemistry: Cambridge, UK, 2011; Volume 1, pp. 234–260. ISBN 978-1-84973-241-3. [Google Scholar]
- Glüge, J.; Scheringer, M.; Cousins, I.T.; DeWitt, J.C.; Goldenman, G.; Herzke, D.; Lohmann, R.; Ng, C.A.; Trier, X.; Wang, Z. An overview of the uses of per- and polyfluoroalkyl substances (PFAS). Environ. Sci. Process. Impacts 2020, 22, 2345–2373. [Google Scholar] [CrossRef]
- Stockholm Convention. Chemicals Proposed for Listing under the Convention. 2022. Available online: http://www.pops.int/TheConvention/ThePOPs/ChemicalsProposedforListing/tabid/2510/Default.aspx (accessed on 3 March 2022).
- D’Hollander, W.; de Voogt, P.; De Coen, W.; Bervoets, L. Perfluorinated substances in human food and other sources of human exposure. Rev. Environ. Contam. Toxicol. 2010, 208, 179–215. [Google Scholar] [CrossRef]
- Olsen, G.W.; Burris, J.M.; Ehresman, D.J.; Froehlich, J.W.; Seacat, A.M.; Butenhoff, J.L.; Zobel, L.R. Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ. Health Perspect. 2007, 115, 1298–1305. [Google Scholar] [CrossRef]
- Lau, C.; Anitole, K.; Hodes, C.; Lai, D.; Pfahles-Hutchens, A.; Seed, J. Perfluoroalkyl acids: A review of monitoring and toxicological findings. Toxicol. Sci. 2007, 99, 366–394. [Google Scholar] [CrossRef]
- Miralles-Marco, A.; Harrad, S. Perfluorooctane sulfonate: A review of human exposure, biomonitoring and the environmental forensics utility of its chirality and isomer distribution. Environ. Int. 2015, 77, 148–159. [Google Scholar] [CrossRef]
- Harada, K.; Inoue, K.; Morikawa, A.; Yoshinaga, T.; Saito, N.; Koizumi, A. Renal clearance of perfluorooctane sulfonate and perfluorooctanoate in humans and their species-specific excretion. Environ. Res. 2005, 99, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, C.; Raffesberg, W.; Weiss, S.; Scharf, S.; Uhl, M. Perfluoroalkylated substances in human urine: Results of a biomonitoring pilot study. Biomonitoring 2017, 4, 1–10. [Google Scholar] [CrossRef]
- Zhang, Y.; Beesoon, S.; Zhu, L.; Martin, J.W. Biomonitoring of perfluoroalkyl acids in human urine and estimates of biological half-life. Environ. Sci. Technol. 2013, 47, 10619–10627. [Google Scholar] [CrossRef] [PubMed]
- Antignac, J.-P.; Veyrand, B.; Kadar, H.; Marchand, P.; Oleko, A.; Le Bizec, B.; Vandentorren, S. Occurrence of perfluorinated alkylated substances in breast milk of French women and relation with socio-demographical and clinical parameters: Results of the ELFE pilot study. Chemosphere 2013, 91, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Awad, R.; Zhou, Y.; Nyberg, E.; Namazkar, S.; Yongning, W.; Xiao, Q.; Sun, Y.; Zhu, Z.; Bergman, Å.; Benskin, J.P. Emerging per- and polyfluoroalkyl substances (PFAS) in human milk from Sweden and China. Environ. Sci. Process. Impacts 2020, 22, 2023–2030. [Google Scholar] [CrossRef]
- Fiedler, H.; Sadia, M. Regional occurrence of perfluoroalkane substances in human milk for the global monitoring plan under the Stockholm Convention on Persistent Organic Pollutants during 2016-2019. Chemosphere 2021, 277, 130287. [Google Scholar] [CrossRef]
- Zheng, G.; Schreder, E.; Dempsey, J.C.; Uding, N.; Chu, V.; Andres, G.; Sathyanarayana, S.; Salamova, A. Per- and Polyfluoroalkyl Substances (PFAS) in Breast Milk: Concerning Trends for Current-Use PFAS. Environ. Sci. Technol. 2021, 55, 7510–7520. [Google Scholar] [CrossRef] [PubMed]
- DeWitt, J.C.; Peden-Adams, M.M.; Keller, J.M.; Germolec, D.R. Immunotoxicity of perfluorinated compounds: Recent developments. Toxicol. Pathol. 2012, 40, 300–311. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Risk to human health related to the presence of perfluorooctane sulfonic acid and perfluorooctanoic acid in food. Eur. Food Saf. Auth. J. 2018, 16, 05194. [Google Scholar] [CrossRef]
- UNEP. Global Monitoring Plan on Persistent Organic Pollutants: Guidelines for Organization, Sampling and Analysis of Human Milk on Persistent Organic Pollutants; United Nations Environment Programme: Nairobi, Kenya, 2017; Available online: https://wedocs.unep.org/bitstream/handle/20.500.11822/21024/UNEP_Guidance_HumanMilk_2017_En.pdf?sequence=1&isAllowed=y (accessed on 24 April 2023).
- U.S. EPA. Method 1614A—Brominated Diphenyl Ethers in Water, Soil, Sediment, and Tissue by HRGC/HRMS: Engineering and Analysis Division (4303T); United States Environment Protection Agency: Washington, DC, USA, 2010. Available online: https://www.epa.gov/sites/default/files/2015-08/documents/method_1614a_2010.pdf (accessed on 24 April 2023).
- Kuklenyik, Z.; Reich, J.A.; Tully, J.S.; Needham, L.L.; Calafat, A.M. Automated solid-phase extraction and measurement of perfluorinated organic acids and amides in human serum and milk. Environ. Sci. Technol. 2004, 38, 3698–3704. [Google Scholar] [CrossRef] [PubMed]
- DIN 32645:2008-11; Chemical Analysis—Decision Limit, Detection Limit and Determination Limit under Repeatability Conditions—Terms, Methods. Evaluation German Institute for Standardisation: Berlin, Germany, 2008. Available online: https://www.beuth.de/en/standard/din-32645/110729574 (accessed on 15 November 2023).
- Kärrman, A.; Ericson, I.; van Bavel, B.; Darnerud, P.O.; Aune, M.; Glynn, A.; Lignell, S.; Lindström, G. Exposure of perfluorinated chemicals through lactation: Levels of matched human milk and serum and a temporal trend, 1996–2004, in Sweden. Environ. Health Perspect. 2007, 115, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Main, K.M.; Kiviranta, H.; Virtanen, H.E.; Sundqvist, E.; Tuomisto, J.T.; Tuomisto, J.; Vartiainen, T.; Skakkebaek, N.E.; Toppari, J. Flame retardants in placenta and breast milk and cryptorchidism in newborn boys. Environ. Health Perspect. 2007, 115, 1519–1526. [Google Scholar] [CrossRef]
- Polder, A.; Thomsen, C.; Lindström, G.; Løken, K.B.; Skaare, J.U. Levels and temporal trends of chlorinated pesticides, polychlorinated biphenyls and brominated flame retardants in individual human breast milk samples from Northern and Southern Norway. Chemosphere 2008, 73, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Raab, U.; Preiss, U.; Albrecht, M.; Shahin, N.; Parlar, H.; Fromme, H. Concentrations of polybrominated diphenyl ethers, organochlorine compounds and nitro musks in mother’s milk from Germany (Bavaria). Chemosphere 2008, 72, 87–94. [Google Scholar] [CrossRef]
- Lignell, S.; Aune, M.; Darnerud, P.O.; Cnattingius, S.; Glynn, A. Persistent organochlorine and organobromine compounds in mother’s milk from Sweden 1996-2006: Compound-specific temporal trends. Environ. Res. 2009, 109, 760–767. [Google Scholar] [CrossRef] [PubMed]
- Jaraczewska, K.; Lulek, J.; Covaci, A.; Voorspoels, S.; Kaluba-Skotarczak, A.; Drews, K.; Schepens, P. Distribution of polychlorinated biphenyls, organochlorine pesticides and polybrominated diphenyl ethers in human umbilical cord serum, maternal serum and milk from Wielkopolska region, Poland. Sci. Total Environ. 2006, 72, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Antignac, J.-P.; Cariou, R.; Zalko, D.; Berrebi, A.; Cravedi, J.-P.; Maume, D.; Marchand, P.; Monteau, F.; Riu, A.; Andre, F.; et al. Exposure assessment of French women and their newborn to brominated flame retardants: Determination of tri- to deca- polybromodiphenylethers (PBDE) in maternal adipose tissue, serum, breast milk and cord serum. Environ. Pollut. 2009, 157, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, M.A.-E.; Harrad, S. Polybrominated diphenyl ethers in UK human milk: Implications for infant exposure and relationship to external exposure. Environ. Int. 2014, 63, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Bramwell, L.; Fernandes, A.; Rose, M.; Harrad, S.; Pless-Mulloli, T. PBDEs and PBBs in human serum and breast milk from cohabiting UK couples. Chemosphere 2014, 116, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, S.; Kim, E.; Lee, I.-S.; Choi, G.; Kim, H.-J.; Park, J.; Jae Lee, J.; Choi, S.; Young Kim, S.; et al. Polybrominated diphenyl ethers (PBDEs) in breast milk of Korea in 2011: Current contamination, time course variation, influencing factors and health risks. Environ. Res. 2013, 126, 76–83. [Google Scholar] [CrossRef]
- Daniels, J.L.; Pan, I.-J.; Jones, R.; Anderson, S.; Patterson, D.G.; Needham, L.L.; Sjödin, A. Individual characteristics associated with PBDE levels in U.S. human milk samples. Environ. Health Perspect. 2010, 118, 155–160. [Google Scholar] [CrossRef]
- WHO/UNEP. Global Monitoring Plan for Persistent Organic Pollutants under the Stockholm Convention Article 16 on Effectiveness Evaluation—Third Regional Monitoring Report Western Europe and Others Group (WEOG) Region 2021; World Health Organization/United Nations Environment Programme: Nairobi, Kenya, 2021; Available online: https://chm.pops.int/Implementation/GlobalMonitoringPlan/MonitoringReports/tabid/525/Default.aspx (accessed on 23 May 2022).
- Zhao, X.; Peng, S.; Xiang, Y.; Yang, Y.; Li, J.; Shan, Z.; Teng, W. Correlation between Prenatal Exposure to Polybrominated Diphenyl Ethers (PBDEs) and Infant Birth Outcomes: A Meta-Analysis and an Experimental Study. Int. J. Environ. Res. Public Health 2017, 14, 268. [Google Scholar] [CrossRef]
- Chao, H.-R.; Wang, S.-L.; Lee, W.-J.; Wang, Y.-F.; Päpke, O. Levels of polybrominated diphenyl ethers (PBDEs) in breast milk from central Taiwan and their relation to infant birth outcome and maternal menstruation effects. Environ. Int. 2007, 33, 239–245. [Google Scholar] [CrossRef]
- Miranda, M.L.; Anthopolos, R.; Wolkin, A.; Stapleton, H.M. Associations of birth outcomes with maternal polybrominated diphenyl ethers and thyroid hormones during pregnancy. Environ. Int. 2015, 85, 244–253. [Google Scholar] [CrossRef]
- Zhao, Y.; Song, Q.; Ge, W.; Jin, Y.; Chen, S.; Zhao, Y.; Xiao, X.; Zhang, Y. Associations between in utero exposure to polybrominated diphenyl ethers, pathophysiological state of fetal growth and placental DNA methylation changes. Environ. Int. 2019, 133, 105255. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.G.; Giordano, G. Is decabromodiphenyl ether (BDE-209) a developmental neurotoxicant? NeuroToxicology 2011, 32, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Herbstman, J.B.; Mall, J.K. Developmental Exposure to Polybrominated Diphenyl Ethers and Neurodevelopment. Curr. Environ. Health Rep. 2014, 1, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Poston, R.G.; Saha, R.N. Epigenetic Effects of Polybrominated Diphenyl Ethers on Human Health. Int. J. Environ. Res. Public Health 2019, 16, 2703. [Google Scholar] [CrossRef]
- Völkel, W.; Genzel-Boroviczény, O.; Demmelmair, H.; Gebauer, C.; Koletzko, B.; Twardella, D.; Raab, U.; Fromme, H. Perfluorooctane sulphonate (PFOS) and perfluorooctanoic acid (PFOA) in human breast milk: Results of a pilot study. Int. J. Hyg. Environ. Health 2008, 211, 440–446. [Google Scholar] [CrossRef]
- Kärrman, A.; Domingo, J.L.; Llebaria, X.; Nadal, M.; Bigas, E.; van Bavel, B.; Lindström, G. Biomonitoring perfluorinated compounds in Catalonia, Spain: Concentrations and trends in human liver and milk samples. Environ. Sci. Pollut. Res. Int. 2010, 17, 750–758. [Google Scholar] [CrossRef]
- Guerranti, C.; Perra, G.; Corsolini, S.; Focardi, S.E. Pilot study on levels of perfluorooctane sulfonic acid (PFOS) and perfluorooctanoic acid (PFOA) in selected foodstuffs and human milk from Italy. Food Chem. 2013, 140, 197–203. [Google Scholar] [CrossRef]
- WHO/UNEP. Global Monitoring Plan for Persistent Organic Pollutants under the Stockholm Convention Article 16 on Effectiveness Evaluation—First Regional Monitoring Report Western Europe and Others Group (WEOG) Region 2008; World Health Organisation/United Nations Environment Programme: Geneva, Switzerland; Nairobi, Kenya, 2009; Available online: https://chm.pops.int/Implementation/GlobalMonitoringPlan/MonitoringReports/tabid/525/Default.aspx (accessed on 15 July 2023).
- WHO/UNEP. Global Monitoring Plan for Persistent Organic Pollutants under the Stockholm Convention Article 16 of Effectiveness Evaluation—2nd Regional Monitoring Report Western Europe and Others Group (WEOG) Region 2015; World Health Organization/United Nations Environment Programme: Geneva, Switzerland; Nairobi, Kenya, 2015; Available online: https://chm.pops.int/Implementation/GlobalMonitoringPlan/MonitoringReports/tabid/525/Default.aspx (accessed on 16 July 2023).
- Fiedler, H. Metadata Analysis of Persistent Organic Pollutants in National Pools of Human Milk in Support of the Stockholm Convention Implementation. Environ. Health 2023, 1, 41–52. [Google Scholar] [CrossRef]
- Umweltbundesamt. Referenzwerte Für Organochlorpestizide und PCB in Frauenmilch; Umweltbundesamt: Dessau-Roßlau, Germany, 2009; Available online: https://www.umweltbundesamt.de/sites/default/files/medien/1/dokumente/tab-frauenmilch_2009_0.pdf (accessed on 22 December 2022).
- WHO. Human Biomonitoring: Facts and Figures; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2015; Available online: https://iris.who.int/handle/10665/164588 (accessed on 15 July 2023).
- Umweltbundesamt. Factsheet HBM Value for HBCD; Umweltbundesamt: Dessau-Roßlau, Germany, 2015; Available online: https://www.umweltbundesamt.de/sites/default/files/medien/378/dokumente/hbcd_factsheet_fuer_hbm.pdf (accessed on 23 July 2023).
- Gyllenhammar, I.; Aune, M.; Fridén, U.; Cantillana, T.; Bignert, A.; Lignell, S.; Glynn, A. Are temporal trends of some persistent organochlorine and organobromine compounds in Swedish breast milk slowing down? Environ. Res. 2021, 197, 111117. [Google Scholar] [CrossRef]
- DeVito, M.; Bokkers, B.; van Duursen, M.B.M.; van Ede, K.; Feeley, M.; Antunes Fernandes Gáspár, E.; Haws, L.; Kennedy, S.; Peterson, R.E.; Hoogenboom, R.; et al. The 2022 world health organization reevaluation of human and mammalian toxic equivalency factors of polychlorinated dioxins, dibenzofurans and biphenyls. Regul. Toxicol. Pharmacol. 2024, 146, 105525. [Google Scholar] [CrossRef]
- EFSA. Risk for animal and human health related to the presence of dioxins and dioxin-like PCBs in feed and food. Eur. Food Saf. Auth. J. 2018, 16, 05333. [Google Scholar] [CrossRef]
- Ingelido, A.M.; Ballard, T.; Dellatte, E.; Di Domenico, A.; Ferri, F.; Fulgenzi, A.R.; Herrmann, T.; Iacovella, N.; Miniero, R.; Päpke, O.; et al. Polychlorinated biphenyls (PCBs) and polybrominated diphenyl ethers (PBDEs) in milk from Italian women living in Rome and Venice. Chemosphere 2007, 67, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Kazda, R.; Hajšlová, J.; Poustka, J.; Čajka, T. Determination of polybrominated diphenyl ethers in human milk samples in the Czech Republic: Comparative study of negative chemical ionization mass spectrometry and time-of-flight high-resolution mass spectrometry. Anal. Chim. Acta 2004, 520, 237–243. [Google Scholar] [CrossRef]
- Gómara, B.; Herrero, L.; Ramos, J.J.; Mateo, J.R.; Fernández, M.A.; García, J.F.; González, M.J. Distribution of polybrominated diphenyl ethers in human umbilical cord serum, paternal serum, maternal serum, placentas, and breast milk from Madrid population, Spain. Environ. Sci. Technol. 2007, 41, 6961–6968. [Google Scholar] [CrossRef]
- Thomsen, C.; Stigum, H.; Frøshaug, M.; Broadwell, S.L.; Becher, G.; Eggesbø, M. Determinants of brominated flame retardants in breast milk from a large scale Norwegian study. Environ. Int. 2010, 36, 68–74. [Google Scholar] [CrossRef]
- Bordajandi, L.R.; Abad, E.; González, M.J. Occurrence of PCBs, PCDD/Fs, PBDEs and DDTs in Spanish breast milk: Enantiomeric fraction of chiral PCBs. Chemosphere 2008, 70, 567–575. [Google Scholar] [CrossRef]
- Gómara, B.; Herrero, L.; Pacepavicius, G.; Ohta, S.; Alaee, M.; González, M.J. Occurrence of co-planar polybrominated/chlorinated biphenyls (PXBs), polybrominated diphenyl ethers (PBDEs) and polychlorinated biphenyls (PCBs) in breast milk of women from Spain. Chemosphere 2011, 83, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Chovancová, J.; Čonka, K.; Kočan, A.; Sejáková, Z.S. PCDD, PCDF, PCB and PBDE concentrations in breast milk of mothers residing in selected areas of Slovakia. Chemosphere 2011, 83, 1383–1390. [Google Scholar] [CrossRef]
- Fromme, H.; Fuchs, V.; Albrecht, M.; Aschenbrenner, B.; Röhl, C.; Janitzki, N.; Herber-Jonat, S.; Wöckner, M.; Völkel, W.; Flemmer, A.W.; et al. Polychlorinated dioxins and dibenzofurans (PCDD/F), polybrominated dioxins and dibenzofurans (PBDD/F), polychlorinated biphenyls (PCB), polybrominated diphenyl ethers (PBDE), and per- and polyfluoroalkyl substances (PFAS) in German breast milk samples (LUPE 8). Sci. Total Environ. 2022, 825, 154066. [Google Scholar] [CrossRef] [PubMed]
- Roosens, L.; D’Hollander, W.; Bervoets, L.; Reynders, H.; van Campenhout, K.; Cornelis, C.; van den Heuvel, R.; Koppen, G.; Covaci, A. Brominated flame retardants and perfluorinated chemicals, two groups of persistent contaminants in Belgian human blood and milk. Environ. Pollut. 2010, 158, 2546–2552. [Google Scholar] [CrossRef]
- Raab, U.; Albrecht, M.; Preiss, U.; Völkel, W.; Schwegler, U.; Fromme, H. Organochlorine compounds, nitro musks and perfluorinated substances in breast milk—Results from Bavarian Monitoring of Breast Milk 2007/8. Chemosphere 2013, 93, 461–467. [Google Scholar] [CrossRef]
- Llorca, M.; Farré, M.; Picó, Y.; Teijón, M.L.; Alvarez, J.G.; Barceló, D. Infant exposure of perfluorinated compounds: Levels in breast milk and commercial baby food. Environ. Int. 2010, 36, 584–592. [Google Scholar] [CrossRef]
- Barbarossa, A.; Masetti, R.; Gazzotti, T.; Zama, D.; Astolfi, A.; Veyrand, B.; Pession, A.; Pagliuca, G. Perfluoroalkyl substances in human milk: A first survey in Italy. Environ. Int. 2013, 51, 27–30. [Google Scholar] [CrossRef]
- Cariou, R.; Veyrand, B.; Yamada, A.; Berrebi, A.; Zalko, D.; Durand, S.; Pollono, C.; Marchand, P.; Leblanc, J.-C.; Antignac, J.-P.; et al. Perfluoroalkyl acid (PFAA) levels and profiles in breast milk, maternal and cord serum of French women and their newborns. Environ. Int. 2015, 84, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Zeilmaker, M.J.; Moermond, C.; Brandon, E.; Hoogerhuis, P.; Razenberg, L.; Janssen, M. Persistent Organic Pollutants in Human Milk in the Netherlands; National Institute for Public Health and the Environment, Ministry of Health, Welfare and Sport: Bilthoven, The Netherlands, 2020; Available online: https://www.rivm.nl/bibliotheek/rapporten/2020-0025.pdf (accessed on 23 July 2023).
- Černá, M.; Grafnetterová, A.P.; Dvořáková, D.; Pulkrabová, J.; Malý, M.; Janoš, T.; Vodrážková, N.; Tupá, Z.; Puklová, V. Biomonitoring of PFOA, PFOS and PFNA in human milk from Czech Republic, time trends and estimation of infant’s daily intake. Environ. Res. 2020, 188, 109763. [Google Scholar] [CrossRef]
- Abdallah, M.A.-E.; Wemken, N.; Drage, D.S.; Tlustos, C.; Cellarius, C.; Cleere, K.; Morrison, J.J.; Daly, S.; Coggins, M.A.; Harrad, S. Concentrations of perfluoroalkyl substances in human milk from Ireland: Implications for adult and nursing infant exposure. Chemosphere 2020, 246, 125724. [Google Scholar] [CrossRef] [PubMed]
- ATSDR. Minimal Risk Levels (MRLs) List. Agency for Toxic Substances and Disease Registry, U.S. Department of Health & Human Services, USA. 2018. Available online: https://www.atsdr.cdc.gov/mrls/mrllist.asp (accessed on 23 July 2023).
- EFSA (European Food Safety Authority). Chlordane as undesirable substance in animal feed—Scientific Opinion of the Panel on Contaminants in the Food Chain. EFSA J. 2007, 582, 1–53. [Google Scholar] [CrossRef]
- EFSA (European Food Safety Authority). Opinion of the Scientific Panel on contaminants in the food chain [CONTAM] related to aldrin and dieldrin as undesirable substance in animal feed. EFSA J. 2005, 285, 1–43. [Google Scholar] [CrossRef]
- EFSA (European Food Safety Authority). Opinion of the Scientific Panel on contaminants in the food chain [CONTAM] related to DDT as an undesirable substance in animal feed. EFSA J. 2006, 433, 1–69. [Google Scholar] [CrossRef]
- EFSA (European Food Safety Authority). Opinion of the Scientific Panel on contaminants in the food chain [CONTAM] related heptachlor as an undesirable substance in animal feed. EFSA J. 2007, 478, 1–48. [Google Scholar] [CrossRef]
- WHO. Pesticide Residues in Food—2000: Toxicological Evaluations. World Health Organization, Geneva, Switzerland. 2001. Available online: https://iris.who.int/bitstream/handle/10665/42411/WHO_PCS_01.3.pdf;jsessionid=8E32A276D1E50688E733E22DA958A8D0?sequence=1 (accessed on 23 July 2023).
- EFSA. Risk assessment of chlorinated paraffins in feed and food. EFSA J. 2019, 18, e05991. [Google Scholar] [CrossRef]
- Health Canada. Non-Carcinogen Tolerable Daily Intake (TDI) Values from Health Canada. 2007. Available online: http://www.popstoolkit.com/tools/HHRA/TDI_HealthCanada.aspx (accessed on 23 July 2023).



{kind=link}
{kind=link}
| Individual Breast Milk Samples | WHO/UNEP Pooled Sample | |||
|---|---|---|---|---|
| Sampling Period | 2013 | 2014–2016 | 2014–2016 | |
| Substance groups (number of substances analysed) | PBDE (20) | PFAS (14) | PFAS (25) | POPs |
| Number of samples | 18 | 21 | 40 | 1 pooled sample (from n = 34) |
| Age of the mother in years (mean ± SD) | 22–40 (30 ± 6) | 22–40 (31 ± 5) | 21–36 (29 ± 4) | 21–36 (28 ± 4) |
| Body weight after delivery in kg (mean ± SD) | 51–96 (68 ± 12) | 51–96 (68 ± 11) | - | - |
| Birth weight newborn in g (mean ± SD) | 2800–4150 (3595 ± 361) | 2800–4150 (3571 ± 360) | - | - |
| PBDE Congener Concentrations in Breast Milk from Austrian Women from 2013 (Pilot Study) | WHO Pooled Sample from 2014–2016 1 | Daily Intake via Breast Milk Consumption [ng/kg bw/d] 2 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [ng/g lipid] | [ng/g breast milk] | [ng/g lipid] | Average intake (present study) | EFSA 3 Average intake | High intake (present study) | EFSA High intake | |||||||
| Substance | n | n < LOD | range | median | range | median | range | median (mean) | range | median (mean) | range | ||
| BDE-15 | - | - | - | - | - | - | 0.02 | - | - | - | - | - | - |
| BDE-17 | - | - | - | - | - | - | 0.0017 | - | - | - | - | - | - |
| BDE-28 | 18 | 5 | n.d.–0.38 | 0.048 | n.d.–0.012 | <LOQ | 0.0256 | 0.0–1.57 | 0.17 (0.60) | <0.05–1.38 | 0.0–2.36 | 0.26 (0.90) | <0.07–2.06 |
| BDE-47 | 18 | 6 | n.d.–6.0 | 0.32 | n.d.–0.20 | <LOQ | 0.412 | 0.0–26.2 | 1.84 (6.11) | 0.64–13.77 | 0.0–39.3 | 2.75 (9.17) | 0.96–20.64 |
| BDE-49 | 18 | 11 | n.d.–0.67 | n.d. | n.d.–0.021 | n.d. | 0.01 | 0.0–2.75 | 0.0 (0.32) | - | 0.0–4.13 | 0.0 (0.48) | - |
| BDE-66 | 18 | 11 | n.d.–0.48 | n.d. | n.d.–0.015 | n.d. | <LOQ | 0.0–1.97 | 0.0 (0.25) | - | 0.0–2.95 | 0.0 (0.37) | - |
| BDE-75 | - | - | - | - | - | - | <LOQ | - | - | - | - | - | - |
| BDE-77 | 18 | 12 | n.d.–0.38 | n.d. | n.d.–0.012 | n.d. | <LOQ | 0.0–1.57 | 0.0 (0.17) | - | 0.0–2.36 | 0.0 (0.25) | - |
| BDE-85 | 18 | 18 | n.d. | n.d. | n.d. | n.d. | - | 0.0 | 0.0 (0.0) | - | 0.0 | 0.0 (0.0) | - |
| BDE-99 | 18 | 6 | n.d.–2.4 | 0.153 | n.d.–0.11 | <LOQ | 0.128 | 0.0–14.43 | 0.79 (3.05) | <0.14–5.05 | 0.0–21.64 | 1.18 (4.57) | <0.14–7.57 |
| BDE-100 | 18 | 4 | n.d.–1.1 | 0.16 | n.d.–0.034 | 0.0065 | 0.126 | 0.0–4.46 | 0.85 (1.23) | 0.18–4.59 | 0.0–6.69 | 1.28 (1.85) | 0.28–6.88 |
| BDE-118 | 18 | 12 | n.d.–0.38 | n.d. | n.d.–0.012 | n.d. | - | 0.0–1.57 | 0.0 (0.18) | - | 0.0–2.36 | 0.0 (0.27) | - |
| BDE-119 | - | - | - | - | - | - | 0.01 | - | - | - | - | - | - |
| BDE-126 | 18 | 17 | n.d.–0.024 | n.d. | n.d.–0.0011 | n.d. | - | 0.0–0.14 | 0.0 (0.01) | - | 0.0–0.22 | 0.0 (0.01) | - |
| BDE-138 | - | - | - | - | - | - | 0.0042 | - | - | - | - | - | - |
| BDE-139 | 18 | 14 | n.d.–0.25 | n.d. | n.d.–0.0079 | n.d. | - | 0.0–1.04 | 0.0 (0.10) | - | 0.0–1.55 | 0.0 (0.15) | - |
| BDE-153 | 18 | 2 | n.d.–0.86 | 0.23 | n.d.–0.028 | 0.011 | 0.548 | 0.0–5.51 | 1.44 (1.54) | 0.46–11.02 | 0.0–5.51 | 2.16 (2.31) | 0.69–16.51 |
| BDE-154 | 18 | 12 | n.d.–1.3 | n.d. | n.d.–0.041 | n.d. | 0.0124 | 0.0–5.38 | 0.0 (0.57) | <0.05–2.30 | 0.0–8.07 | 0.0 (0.85) | <0.07–3.44 |
| BDE-181 | 18 | 18 | n.d. | n.d. | n.d. | n.d. | - | 0.0 | 0.0 (0.0) | - | 0.0 | 0.0 (0.0) | - |
| BDE-183 | 18 | 3 | n.d.–0.37 | 0.054 | n.d.–0.012 | <LOQ | 0.05 | 0.0–1.57 | 0.25 (0.52) | 0.23–1.38 | 0.0–2.36 | 0.37 (0.78) | 0.34–2.06 |
| BDE-190 | - | - | - | - | - | - | <LOQ | - | - | - | - | - | - |
| BDE-196 | 18 | 13 | n.d.–0.21 | n.d. | n.d.–0.011 | n.d. | - | 0.0–1.44 | 0.0 (0.19) | - | 0.0–2.16 | 0.0 (0.29) | - |
| BDE-197 | 18 | 1 | n.d.–0.39 | 0.095 | n.d.–0.020 | <LOQ | - | 0.0–2.62 | 0.70 (0.75) | - | 0.0–3.93 | 1.04 (1.13) | - |
| BDE-203 | 18 | 13 | n.d.–0.35 | n.d. | n.d.–0.018 | n.d. | 1.35 | 0.0–2.36 | 0.0 (0.30) | - | 0.0–3.54 | 0.0 (0.45) | - |
| BDE-206 | - | - | - | - | - | - | 1.35 | - | - | - | - | - | - |
| BDE-207 | 18 | 9 | n.d.–2.5 | 0.035 | n.d.–0.13 | <LOQ | 0.24 | 0.0–17.1 | 1.93 (3.51) | - | 0.0–25.6 | 2.90 (5.27) | - |
| BDE-208 | - | - | - | - | - | - | 0.1 | - | - | - | - | - | - |
| BDE-209 | 18 | 8 | n.d.–43 | 9.5 | n.d.–2.2 | <LOQ | - | 0.0–289 | 57.1 (70.4) | 0.96–13.31 | 0.0–433 | 85.6 (106) | 1.44–19.95 |
| Sum 8 BDE 4 | 18 | 1 | n.d.–12.5 | 1.06 | n.d.–0.39 | 0.056 | - | 0.0–51.5 | 7.32 (13.34) | - | 0.0–77.3 | 10.98 (20.02) | - |
| Sum PBDE | 18 | 0 | 0.055–52 | 11 | 0.002–2.53 | 0.47 | 4.38 5 | 0.28–332 | 61.90 (89.78) | - | 0.41–497 | 92.84 (135) | - |
| Technical mixtures | |||||||||||||
| TetraBDE 6 | 18 | 6 | n.d.–0.238 | 0.0169 | n.d.–7.53 | 0.423 | - | - | - | - | - | - | - |
| PentaBDE 7 | 18 | 3 | n.d.–0.134 | 0.0135 | n.d.–3.88 | - | - | - | - | - | - | - | - |
| HexaBDE 8 | 18 | 2 | n.d.–0.0759 | 0.0125 | n.d.–2.41 | - | - | - | - | - | - | - | - |
| HeptaBDE 9 | 18 | 3 | n.d.–0.012 | 0.0019 | n.d.–0.37 | - | - | - | - | - | - | - | - |
| OctaBDE 10 | 18 | 1 | n.d.–0.044 | 0.0063 | n.d.–0.85 | - | - | - | - | - | - | - | - |
| PFAS Concentrations in Breast Milk [ng/L] | Weekly Intake via Breast Milk Consumption [ng/kg bw/Week] a | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Average intake | High intake | ||||||||
| Substance | n | n < LOD | range | median | P95 | range | median (mean) | range | median (mean) |
| Pilot study (2013) | |||||||||
| PFOA | 21 | 11 | n.d.–83 | n.d. | 81 | 0.0–76 | 0.0 (13) | 0.0–114 | 0.0 (20) |
| PFOS | 21 | 0 | 58–310 | 110 | 300 | 53–285 | 101 (116) | 80–427 | 151 (174) |
| Sum 4 PFAS b | 21 | 0 | 69–310 | 120 | 308 | 63–285 | 110 (129) | 95–427 | 165 (194) |
| Follow-up study (2014–2016) | |||||||||
| PFBA | 40 | 36 | n.d.–<LOQ | n.d. | <LOQ | ||||
| PFBS | 40 | 39 | n.d.–8.1 | n.d. | n.d. | ||||
| PFPeS | 40 | 36 | n.d.–18 | n.d. | <LOQ | ||||
| PFHxA | 40 | 27 | n.d.–28 | n.d. | 16 | ||||
| PFHxS | 40 | 0 | <LOQ–9.7 | <LOQ | 6.0 | 1.9–8.9 | 1.9 (2.5) | 2.8–13 | 2.8 (3.7) |
| PFHpA | 40 | 30 | n.d.–<LOQ | n.d. | <LOQ | ||||
| PFOA | 40 | 0 | <LOQ–91 | 25 | 75 | 4.1–84 | 22 (28) | 6.3–125 | 34 (41) |
| PFOS | 40 | 1 | n.d.–55 | 12 | 39 | 0.0–50 | 11 (14) | 0.0–76 | 17 (20) |
| PFNA | 40 | 6 | n.d.–15 | <LOQ | 8.0 | 0.0–14 | 2.1 (3.0) | 0.0–21 | 3.2 (4.5) |
| PFDA | 40 | 22 | n.d.–8.7 | n.d. | 4.6 | ||||
| PFDS | 40 | 39 | n.d.–<LOQ | n.d. | n.d. | ||||
| PFUnDA | 39 | 36 | n.d.–<LOQ | n.d. | <LOQ | ||||
| PFDoDA | 39 | 37 | n.d.–<LOQ | n.d. | <LOQ | ||||
| PFTrDA | 40 | 39 | n.d.–<LOQ | n.d. | n.d. | ||||
| PFTeDA | 39 | 37 | n.d.–<LOQ | n.d. | <LOQ | ||||
| 6:2-FTS | 40 | 31 | n.d.–<LOQ | n.d. | <LOQ | ||||
| DONA | 40 | 31 | n.d.–9.6 | n.d. | <LOQ | ||||
| 6:2 Cl-PFESA | 40 | 39 | n.d.–5.5 | n.d. | n.d. | ||||
| GenX | 40 | 39 | n.d.–14 | n.d. | n.d. | ||||
| Sum 4 PFAS b | 40 | 0 | 14–124 | 44 | 119 | 13–114 | 40 (47) | 20–170 | 61 (70) |
| WHO/UNEP monitoring programme (in ng/g) | |||||||||
| PFOS | 1 | 1 | 0.025 c | ||||||
| PFOA | 1 | 1 | 0.045 c | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartmann, C.; Kaiser, A.-M.; Moche, W.; Weiss, S.; Raffesberg, W.; Scharf, S.; Graf-Rohrmeister, K.; Thanhaeuser, M.; Haiden, N.; Uhl, M. Persistent Organic Pollutants in Austrian Human Breast Milk Collected between 2013 and 2016. J. Xenobiot. 2024, 14, 247-266. https://0-doi-org.brum.beds.ac.uk/10.3390/jox14010015
Hartmann C, Kaiser A-M, Moche W, Weiss S, Raffesberg W, Scharf S, Graf-Rohrmeister K, Thanhaeuser M, Haiden N, Uhl M. Persistent Organic Pollutants in Austrian Human Breast Milk Collected between 2013 and 2016. Journal of Xenobiotics. 2024; 14(1):247-266. https://0-doi-org.brum.beds.ac.uk/10.3390/jox14010015
Chicago/Turabian StyleHartmann, Christina, Andreas-Marius Kaiser, Wolfgang Moche, Stefan Weiss, Wolfgang Raffesberg, Sigrid Scharf, Klaudia Graf-Rohrmeister, Margarita Thanhaeuser, Nadja Haiden, and Maria Uhl. 2024. "Persistent Organic Pollutants in Austrian Human Breast Milk Collected between 2013 and 2016" Journal of Xenobiotics 14, no. 1: 247-266. https://0-doi-org.brum.beds.ac.uk/10.3390/jox14010015