Amerindian Ancestry Influences Genetic Susceptibility to Chronic Obstructive Pulmonary Disease

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Genotyping, Imputation and Ancestry Estimation
2.3. Statistical Analyses
3. Results
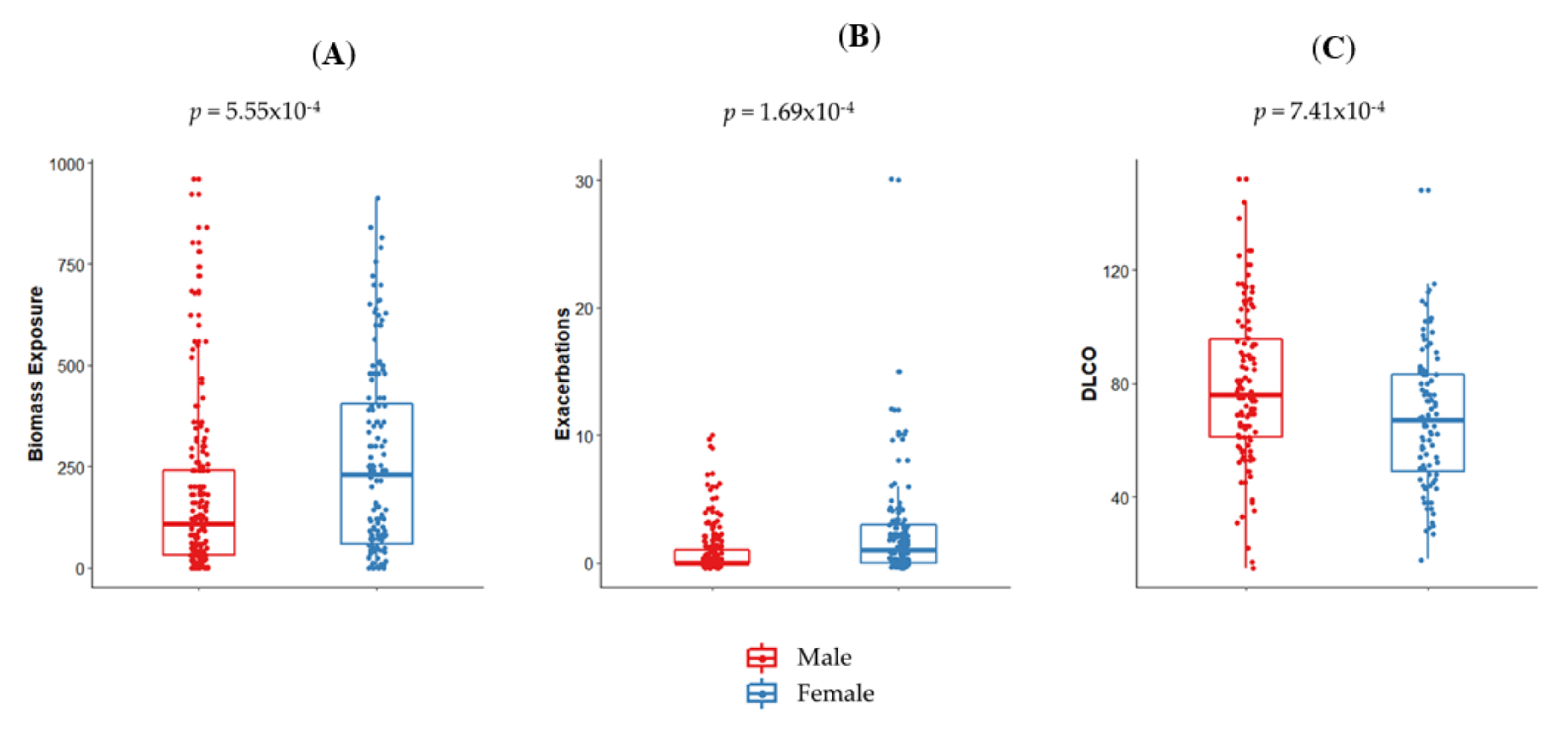
3.1. Demographic and Clinical Findings
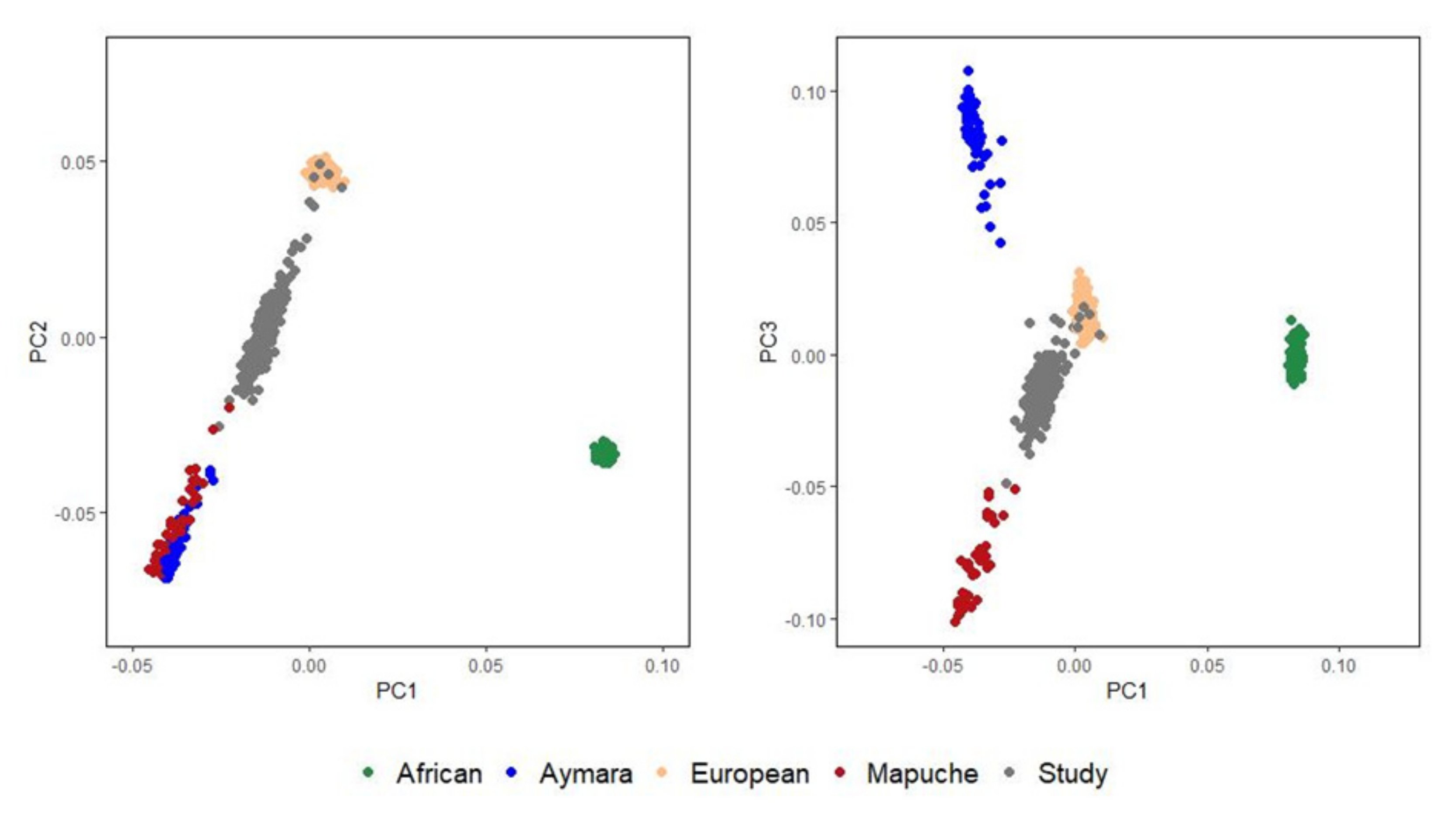
3.2. Analysis of Population Structure
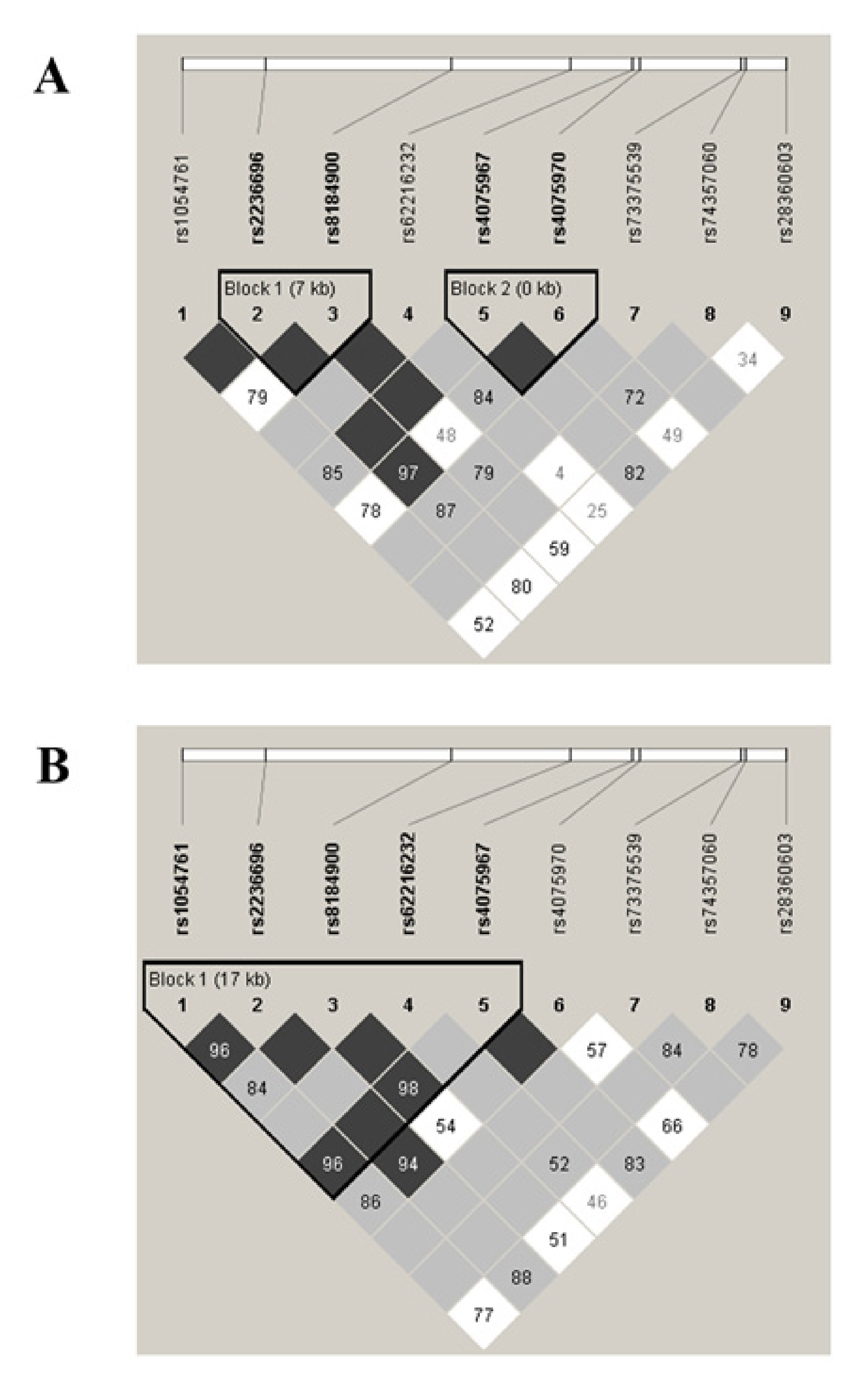
3.3. Influence of Genetic Ancestry on the Association of SNPs and COPD
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Diesease (GOLD). 2020 Global Strategy for Prevention, Diagnosis and Management of COPD; Global Initiative for Chronic Obstructive Lung Diesease (GOLD): Fontana, WI, USA, 2020. [Google Scholar]
- Silva, R.; Oyarzun, M.; Olloquequi, J. Pathogenic mechanisms in chronic obstructive pulmonary disease due to biomass smoke exposure. Arch. Bronconeumol. 2015, 51, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Han, M.K.; Hanania, N.A.; Martinez, F.J. Confronting the Challenge of COPD: What Is New in the Approaches to Diagnosis, Treatment, and Patient Outcomes. Chest 2018, 154, 984–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vestbo, J.; Hurd, S.S.; Agusti, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Ciapponi, A.; Alison, L.; Agustina, M.; Demian, G.; Silvana, C.; Edgardo, S. The epidemiology and burden of COPD in Latin America and the Caribbean: Systematic review and meta-analysis. COPD 2014, 11, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Menezes, A.M.; Perez-Padilla, R.; Jardim, J.R.; Muino, A.; Lopez, M.V.; Valdivia, G.; Montes de Oca, M.; Talamo, C.; Hallal, P.C.; Victora, C.G. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): A prevalence study. Lancet 2005, 366, 1875–1881. [Google Scholar] [CrossRef]
- Palloni, A.; Novak, B.; Pinto-Aguirre, G. The enduring effects of smoking in Latin America. Am. J. Public Health 2015, 105, 1246–1253. [Google Scholar] [CrossRef]
- Torres-Duque, C.; Maldonado, D.; Pérez-Padilla, R.; Ezzati, M.; Viegi, G. Biomass fuels and respiratory diseases: A review of the evidence. Proc. Am. Thorac. Soc. 2008, 5, 577–590. [Google Scholar] [CrossRef]
- SZOT M., J. Mortalidad por enfermedades respiratorias en Chile durante 1999. Rev. Chil. Enf. Respir. 2003, 19, 8–14. [Google Scholar] [CrossRef]
- Wade, P. Race and Ethnicity in Latin America; Pluto Press: London, UK, 2010. [Google Scholar]
- Klimentidis, Y.C.; Miller, G.F.; Shriver, M.D. Genetic admixture, self-reported ethnicity, self-estimated admixture, and skin pigmentation among Hispanics and Native Americans. Am. J. Phys. Anthropol. 2009, 138, 375–383. [Google Scholar] [CrossRef]
- Sans, M. Admixture studies in Latin America: From the 20th to the 21st century. Hum. Biol. 2000, 72, 155–177. [Google Scholar]
- Ruiz-Linares, A.; Adhikari, K.; Acuña-Alonzo, V.; Quinto-Sanchez, M.; Jaramillo, C.; Arias, W.; Fuentes, M.; Pizarro, M.; Everardo, P.; de Avila, F.; et al. Admixture in Latin America: Geographic Structure, Phenotypic Diversity and Self-Perception of Ancestry Based on 7,342 Individuals. PLoS Genet. 2014, 10, e1004572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Ray, N.; Rojas, W.; Parra, M.V.; Bedoya, G.; Gallo, C.; Poletti, G.; Mazzotti, G.; Hill, K.; Hurtado, A.M.; et al. Geographic Patterns of Genome Admixture in Latin American Mestizos. PLoS Genet. 2008, 4, e1000037. [Google Scholar] [CrossRef] [Green Version]
- Fuentes, M.; Pulgar, I.; Gallo, C.; Bortolini, M.-C.; Canizales-Quinteros, S.; Bedoya, G.; González-José, R.; Ruiz-Linares, A.; Rothhammer, F. Geografía génica de Chile: Distribución regional de los aportes genéticos americanos, europeos y africanos. Rev. Méd. de Chile 2014, 142, 281–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyheramendy, S.; Martinez, F.I.; Manevy, F.; Vial, C.; Repetto, G.M. Genetic structure characterization of Chileans reflects historical immigration patterns. Nat. Commun. 2015, 6, 6472. [Google Scholar] [CrossRef] [PubMed]
- Smolonska, J.; Wijmenga, C.; Postma, D.S.; Boezen, H.M. Meta-analyses on suspected chronic obstructive pulmonary disease genes: A summary of 20 years’ research. Am. J. Respir. Crit. Care Med. 2009, 180, 618–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wain, L.V.; Shrine, N.; Artigas, M.S.; Erzurumluoglu, A.M.; Noyvert, B.; Bossini-Castillo, L.; Obeidat, M.; Henry, P.A.; Portelli, M.A.; Hall, R.J.; et al. Genome-wide association analyses for lung function and chronic obstructive pulmonary disease identify new loci and potential druggable targets. Nat. Genet. 2017, 49, 416–425. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.; Tantisira, K. ¡HOLA! The Influence of Being Hispanic on Lung Ancestry. Am. J. Respir. Crit. Care Med. 2018, 198, 148–149. [Google Scholar] [CrossRef]
- Kheirallah, A.K.; Miller, S.; Hall, I.P.; Sayers, I. Translating Lung Function Genome-Wide Association Study (GWAS) Findings: New Insights for Lung Biology. Adv. Genet. 2016, 93, 57–145. [Google Scholar] [CrossRef]
- Lutz, S.M.; Cho, M.H.; Young, K.; Hersh, C.P.; Castaldi, P.J.; McDonald, M.L.; Regan, E.; Mattheisen, M.; DeMeo, D.L.; Parker, M.; et al. A genome-wide association study identifies risk loci for spirometric measures among smokers of European and African ancestry. BMC Genet. 2015, 16, 138. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Cho, M.H.; Zhou, X. What do polymorphisms tell us about the mechanisms of COPD? Clin. Sci. 2017, 131, 2847–2863. [Google Scholar] [CrossRef]
- Kim, D.K.; Cho, M.H.; Hersh, C.P.; Lomas, D.A.; Miller, B.E.; Kong, X.; Bakke, P.; Gulsvik, A.; Agustí, A.; Wouters, E.; et al. Genome-wide association analysis of blood biomarkers in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2012, 186, 1238–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manichaikul, A.; Hoffman, E.A.; Smolonska, J.; Gao, W.; Cho, M.H.; Baumhauer, H.; Budoff, M.; Austin, J.H.; Washko, G.R.; Carr, J.J.; et al. Genome-wide study of percent emphysema on computed tomography in the general population. The Multi-Ethnic Study of Atherosclerosis Lung/SNP Health Association Resource Study. Am. J. Respir. Crit. Care. Med. 2014, 189, 408–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Brehm, J.M.; Manichaikul, A.; Cho, M.H.; Boutaoui, N.; Yan, Q.; Burkart, K.M.; Enright, P.L.; Rotter, J.I.; Petersen, H.; et al. A genome-wide association study of chronic obstructive pulmonary disease in Hispanics. Ann. Am. Thorac. Soc. 2015, 12, 340–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkart, K.M.; Sofer, T.; London, S.J.; Manichaikul, A.; Hartwig, F.P.; Yan, Q.; Soler Artigas, M.; Avila, L.; Chen, W.; Davis Thomas, S.; et al. A Genome-Wide Association Study in Hispanics/Latinos Identifies Novel Signals for Lung Function. The Hispanic Community Health Study/Study of Latinos. Am. J. Respir. Crit. Care. Med. 2018, 198, 208–219. [Google Scholar] [CrossRef]
- Hosgood Iii, H.D.; Diaz-Pena, R.; Blansky, D.; Jaime, S.; Parra, V.; Boekstegers, F.; Bermejo, J.L.; Garcia-Valero, J.; Montes, J.F.; Valdivia, G.; et al. PRDM15 Is Associated with Risk of Chronic Obstructive Pulmonary Disease in a Rural Population in Chile. Respiration 2020, 99, 307–315. [Google Scholar] [CrossRef]
- Hindorff, L.A.; Bonham, V.L.; Brody, L.C.; Ginoza, M.E.C.; Hutter, C.M.; Manolio, T.A.; Green, E.D. Prioritizing diversity in human genomics research. Nat. Rev. Genet. 2018, 19, 175–185. [Google Scholar] [CrossRef]
- Díaz, A.A.; Celli, B.; Celedón, J.C. Chronic Obstructive Pulmonary Disease in Hispanics. A 9-Year Update. Am. J. Respir. Crit. Care. Med. 2018, 197, 15–21. [Google Scholar] [CrossRef]
- GOLD. 2019 Global Strategy for the Diagnosis, Management and Prevention of COPD; Global Initiative for Chronic Obstructive Lung Disease (GOLD): Fontana, WI, USA, 2019. [Google Scholar]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Olloquequi, J.; Jaime, S.; Parra, V.; Cornejo-Cordova, E.; Valdivia, G.; Agusti, A.; Silva, O.R. Comparative analysis of COPD associated with tobacco smoking, biomass smoke exposure or both. Respir. Res. 2018, 19, 13. [Google Scholar] [CrossRef]
- Hardin, M.; Cho, M.H.; McDonald, M.L.; Wan, E.; Lomas, D.A.; Coxson, H.O.; MacNee, W.; Vestbo, J.; Yates, J.C.; Agusti, A.; et al. A genome-wide analysis of the response to inhaled beta2-agonists in chronic obstructive pulmonary disease. Pharmacogenomics J. 2016, 16, 326–335. [Google Scholar] [CrossRef] [Green Version]
- Hobbs, B.D.; de Jong, K.; Lamontagne, M.; Bosse, Y.; Shrine, N.; Artigas, M.S.; Wain, L.V.; Hall, I.P.; Jackson, V.E.; Wyss, A.B.; et al. Genetic loci associated with chronic obstructive pulmonary disease overlap with loci for lung function and pulmonary fibrosis. Nat. Genet. 2017, 49, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Obeidat, M.; Zhou, G.; Li, X.; Hansel, N.N.; Rafaels, N.; Mathias, R.; Ruczinski, I.; Beaty, T.H.; Barnes, K.C.; Pare, P.D.; et al. The genetics of smoking in individuals with chronic obstructive pulmonary disease. Respir. Res. 2018, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Howie, B.N.; Donnelly, P.; Marchini, J. A flexible and accurate genotype imputation method for the next generation of genome-wide association studies. PLoS Genet. 2009, 5, e1000529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auton, A.; Brooks, L.D.; Durbin, R.M.; Garrison, E.P.; Kang, H.M.; Korbel, J.O.; Marchini, J.L.; McCarthy, S.; McVean, G.A.; Abecasis, G.R. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, D.H.; Novembre, J.; Lange, K. Fast model-based estimation of ancestry in unrelated individuals. Genome Res. 2009, 19, 1655–1664. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo Bermejo, J.; Boekstegers, F.; Gonzalez Silos, R.; Marcelain, K.; Baez Benavides, P.; Barahona Ponce, C.; Muller, B.; Ferreccio, C.; Koshiol, J.; Fischer, C.; et al. Subtypes of Native American ancestry and leading causes of death: Mapuche ancestry-specific associations with gallbladder cancer risk in Chile. PLoS Genet. 2017, 13, e1006756. [Google Scholar] [CrossRef]
- Reich, D.; Patterson, N.; Campbell, D.; Tandon, A.; Mazieres, S.; Ray, N.; Parra, M.V.; Rojas, W.; Duque, C.; Mesa, N.; et al. Reconstructing Native American population history. Nature 2012, 488, 370–374. [Google Scholar] [CrossRef]
- Lindo, J.; Haas, R.; Hofman, C.; Apata, M.; Moraga, M.; Verdugo, R.A.; Watson, J.T.; Viviano Llave, C.; Witonsky, D.; Beall, C.; et al. The genetic prehistory of the Andean highlands 7000 years BP though European contact. Sci. Adv. 2018, 4, eaau4921. [Google Scholar] [CrossRef] [Green Version]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Gen. 2007, 81, 559–575. [Google Scholar] [CrossRef] [Green Version]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, J.R.; Armengol, L.; Sole, X.; Guino, E.; Mercader, J.M.; Estivill, X.; Moreno, V. SNPassoc: An R package to perform whole genome association studies. Bioinformatics 2007, 23, 644–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, A.L.; Patterson, N.J.; Plenge, R.M.; Weinblatt, M.E.; Shadick, N.A.; Reich, D. Principal components analysis corrects for stratification in genome-wide association studies. Nat. Genet 2006, 38, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Galesanu, R.G.; Bernard, S.; Marquis, K.; Lacasse, Y.; Poirier, P.; Bourbeau, J.; Maltais, F. Obesity in chronic obstructive pulmonary disease: Is fatter really better? Can. Respir. J. 2014, 21, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Montes de Oca, M.; Talamo, C.; Perez-Padilla, R.; Jardim, J.R.; Muino, A.; Lopez, M.V.; Valdivia, G.; Pertuze, J.; Moreno, D.; Halbert, R.J.; et al. Chronic obstructive pulmonary disease and body mass index in five Latin America cities: The PLATINO study. Respir. Med. 2008, 102, 642–650. [Google Scholar] [CrossRef] [Green Version]
- Perez-Padilla, R.; Schilmann, A.; Riojas-Rodriguez, H. Respiratory health effects of indoor air pollution. Int. J. Tuberc. Lung. Dis. 2010, 14, 1079–1086. [Google Scholar]
- Lisspers, K.; Larsson, K.; Janson, C.; Stallberg, B.; Tsiligianni, I.; Gutzwiller, F.S.; Mezzi, K.; Bjerregaard, B.K.; Jorgensen, L.; Johansson, G. Gender differences among Swedish COPD patients: Results from the ARCTIC, a real-world retrospective cohort study. NPJ Prim. Care Respir. Med. 2019, 29, 45. [Google Scholar] [CrossRef]
- Tsiligianni, I.; Rodriguez, M.R.; Lisspers, K.; LeeTan, T.; Infantino, A. Call to action: Improving primary care for women with COPD. NPJ Prim. Care Respir. Med. 2017, 27, 11. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, C.R.; Chapman, K.R.; Donohue, J.F.; Roche, N.; Tsiligianni, I.; Han, M.K. Improving the Management of COPD in Women. Chest 2017, 151, 686–696. [Google Scholar] [CrossRef] [Green Version]
- Hansel, N.N.; McCormack, M.C.; Belli, A.J.; Matsui, E.C.; Peng, R.D.; Aloe, C.; Paulin, L.; Williams, D.L.; Diette, G.B.; Breysse, P.N. In-home air pollution is linked to respiratory morbidity in former smokers with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 1085–1090. [Google Scholar] [CrossRef] [Green Version]
- Mzoughi, S.; Zhang, J.; Hequet, D.; Teo, S.X.; Fang, H.; Xing, Q.R.; Bezzi, M.; Seah, M.K.Y.; Ong, S.L.M.; Shin, E.M.; et al. PRDM15 safeguards naive pluripotency by transcriptionally regulating WNT and MAPK-ERK signaling. Nat. Genet. 2017, 49, 1354–1363. [Google Scholar] [CrossRef]
- Ito, M.; Nakano, T.; Erdodi, F.; Hartshorne, D.J. Myosin phosphatase: Structure, regulation and function. Mol. Cell Biochem. 2004, 259, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Freidin, M.B.; Polonikov, A.V. Validation of PPP1R12B as a candidate gene for childhood asthma in Russians. J. Genet. 2013, 92, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Agustí, A.; MacNee, W.; Donaldson, K.; Cosio, M. Hypothesis: Does COPD have an autoimmune component? Thorax 2003, 58, 832–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giallourakis, C.C.; Benita, Y.; Molinie, B.; Cao, Z.; Despo, O.; Pratt, H.E.; Zukerberg, L.R.; Daly, M.J.; Rioux, J.D.; Xavier, R.J. Genome-wide analysis of immune system genes by expressed sequence Tag profiling. J. Immunol. 2013, 190, 5578–5587. [Google Scholar] [CrossRef]
- Park, H.Y.; Lee, S.-B.; Yoo, H.-Y.; Kim, S.-J.; Kim, W.-S.; Kim, J.-I.; Ko, Y.-H. Whole-exome and transcriptome sequencing of refractory diffuse large B-cell lymphoma. Oncotarget 2016, 7, 86433–86445. [Google Scholar] [CrossRef] [Green Version]
- Polverino, F.; Seys, L.J.M.; Bracke, K.R.; Owen, C.A. B cells in chronic obstructive pulmonary disease: Moving to center stage. Am. J. Physiol. Lung Cell. Mol. Physiol. 2016, 311, L687–L695. [Google Scholar] [CrossRef]
- Östensson, M.; Montén, C.; Bacelis, J.; Gudjonsdottir, A.H.; Adamovic, S.; Ek, J.; Ascher, H.; Pollak, E.; Arnell, H.; Browaldh, L.; et al. A possible mechanism behind autoimmune disorders discovered by genome-wide linkage and association analysis in celiac disease. PLoS ONE 2013, 8, e70174. [Google Scholar] [CrossRef]
- Lynch, M.; Ackerman, M.S.; Gout, J.F.; Long, H.; Sung, W.; Thomas, W.K.; Foster, P.L. Genetic drift, selection and the evolution of the mutation rate. Nat. Rev. Genet. 2016, 17, 704–714. [Google Scholar] [CrossRef]
- Gurdasani, D.; Barroso, I.; Zeggini, E.; Sandhu, M.S. Genomics of disease risk in globally diverse populations. Nat. Rev. Genet. 2019, 20, 520–535. [Google Scholar] [CrossRef]
- Baran, Y.; Pasaniuc, B.; Sankararaman, S.; Torgerson, D.G.; Gignoux, C.; Eng, C.; Rodriguez-Cintron, W.; Chapela, R.; Ford, J.G.; Avila, P.C.; et al. Fast and accurate inference of local ancestry in Latino populations. Bioinformatics 2012, 28, 1359–1367. [Google Scholar] [CrossRef] [Green Version]
- Martin, A.R.; Kanai, M.; Kamatani, Y.; Okada, Y.; Neale, B.M.; Daly, M.J. Clinical use of current polygenic risk scores may exacerbate health disparities. Nat. Genet. 2019, 51, 584–591. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| - | Control Subjects n = 193 | COPD Patients n = 214 |
|---|---|---|
| Sex, Male/Female | 60/133 | 121/93 |
| Age, years | 68.66 ± 3.25 | 70.97 ± 4.69 |
| Smoking history, pack-years | 7.75 ± 3.25 | 30.47 ± 14.82 * |
| Current Smoker | 31 (16.06%) | 33 (15.42%) |
| Former smoker | 71 (36.79%) | 145 (67.76%) |
| Never smoker | 91 (47.15%) | 36 (16.82%) |
| Biomass exposure, hour-years | 96.87 ± 32.57 | 225.62 ± 54.28 * |
| Scholarship, years | 14.33 ± 2.57 | 7.21 ± 3.98 * |
| BMI, kg/m2 | 29.45 ± 5.02 | 26.96 ± 5.02 * |
| Exacerbations in the previous year | –– | 1.37 ± 1.50 |
| FEV1, % predicted | 108.84 ± 18.40 | 61.47 ± 24.56 * |
| FEV1/FVC, % | 83.00 ± 6.27 | 58.25 ± 10.48 * |
| DLCO, % predicted | 87.43 ± 24.48 | 72.33 ± 25.13 * |
| Oxygen Saturation, % | 96.14 ± 2.34 | 92.36 ± 4.76 * |
| 6MW, meters | 462.95 ± 87.82 | 351.50 ± 155.61 * |
| mMRC | –– | 2.28 ± 1.39 |
| CAT | –– | 14.94 ± 8.46 |
| BODE | –– | 3.18 ± 2.74 |
| European ancestry, % | 55.93 ± 6.89 | 56.32 ± 10.27 |
| African ancestry, % | 1.73 ± 1.00 | 1.73 ± 1.12 |
| Mapuche ancestry, % | 35.39 ± 6.71 | 35.11 ± 8.54 |
| Aymara ancestry, % | 6.96 ±.45 | 6.73 ± 3.52 |
| CAUCASIAN | CHILEAN | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SNP | SNP Risk Allele | Risk Allele Frequency | OR | A1 | MAF Controls | MAF COPD Cases | OR1 | p | *OR2 | 95% CI | p |
| rs626750 | T | 0.17 | 0.74 | T | 0.15 | 0.09 | 0.57 | 0.01 | 0.50 | 0.28–0.90 | 0.02 |
| rs8034191 | C | 0.33 | 1.40 | C | 0.21 | 0.27 | 1.44 | 0.03 | 1.33 | 0.86–2.07 | 0.20 |
| rs7181486 | C | 0.39 | 1.32 | T | 0.21 | 0.27 | 1.40 | 0.04 | 1.39 | 0.90–2.15 | 0.14 |
| rs9599114 | C | 0.42 | 0.11 | C | 0.47 | 0.40 | 0.75 | 0.05 | 0.77 | 0.53–1.13 | 0.18 |
| Low PMA | |||||||
| SNP | A1 | OR1 | 95%CI | p | *OR2 | 95%CI | p |
| rs1054761 | T | 0.31 | 0.18–0.51 | 7.24 × 10–7 | 0.23 | 0.09–0.89 | 0.02 |
| rs2236696 | T | 2.45 | 1.5–3.99 | 1.89 × 10–4 | 10.41 | 1.99–54.59 | 1.00 × 10−3 |
| rs8184900 | G | 0.4 | 0.26–0.62 | 9.99 × 10–6 | 0.40 | 0.11–1.49 | 0.16 |
| rs4075967 | A | 0.27 | 0.16–0.46 | 9.46 × 10–8 | 0.22 | 0.04–1.12 | 0.05 |
| rs4075970 | A | 2.43 | 1.57–3.78 | 3.32 × 10–5 | 6.76 | 1.84–24.84 | 8.25 × 10−4 |
| rs28360603 | A | 2.26 | 1.46–3.48 | 1.24 × 10–4 | 7.55 | 2–28.54 | 5.41 × 10−4 |
| rs7275618 | C | 1.79 | 1.18–2.71 | 4.75 × 10–3 | 2.04 | 0.57–7.30 | 0.25 |
| rs35109371 | C | 1.87 | 1.24–2.82 | 2.16 × 10–3 | 2.02 | 0.56–7.26 | 0.27 |
| High PMA | |||||||
| SNP | A1 | OR1 | 95%CI | p | *OR2 | 95%CI | p |
| rs1054761 | T | 0.63 | 0.41–0.96 | 0.03 | 0.41 | 0.13–1.25 | 0.10 |
| rs2236696 | T | 1.02 | 0.7–1.5 | 0.92 | 2.34 | 0.80–6.92 | 0.11 |
| rs8184900 | G | 0.73 | 0.5–1.08 | 0.12 | 0.58 | 0.29–1.16 | 0.12 |
| rs4075967 | A | 0.73 | 0.47–1.13 | 0.15 | 0.45 | 0.15–1.40 | 0.15 |
| rs4075970 | A | 0.98 | 0.68–1.43 | 0.93 | 2.08 | 0.77–5.64 | 0.13 |
| rs28360603 | A | 1.22 | 0.82–1.79 | 0.32 | 1.04 | 0.34–3.17 | 0.94 |
| rs7275618 | C | 1.18 | 0.77–1.83 | 0.44 | 0.81 | 0.22–3.01 | 0.75 |
| rs35109371 | C | 1.32 | 0.88–1.96 | 0.17 | 1.08 | 0.31–3.71 | 0.90 |
| SNP Markers | p-Value |
|---|---|
| rs4075967|rs4075970 | 1.01 × 10−7 |
| rs1054761|rs2236696|rs8184900 | 9.53 × 10−7 |
| rs2236696|rs8184900|rs62216232 | 3.77 × 10−8 |
| rs62216232|rs4075967|rs4075970 | 1.43 × 10−7 |
| rs2236696|rs8184900|rs62216232|rs4075967 | 1.01 × 10−7 |
| rs8184900|rs62216232|rs4075967|rs4075970 | 1.16 × 10−7 |
| rs62216232|rs4075967|rs4075970|rs73375539 | 1.44 × 10−7 |
| rs4075967|rs4075970|rs73375539|rs74357060 | 1.42 × 10−7 |
| rs2236696|rs8184900|rs62216232|rs4075967|rs4075970 | 9.48 × 10−8 |
| rs8184900|rs62216232|rs4075967|rs4075970|rs73375539 | 8.36 × 10−8 |
| rs62216232|rs4075967|rs4075970|rs73375539|rs74357060 | 1.09 × 10−7 |
| rs4075967|rs4075970|rs73375539|rs74357060|rs28360603 | 4.38 × 10−7 |
| rs2236696|rs8184900|rs62216232|rs4075967|rs4075970|rs73375539 | 9.52 × 10−8 |
| rs8184900|rs62216232|rs4075967|rs4075970|rs73375539|rs74357060 | 5.81 × 10−8 |
| rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603 | 5.80 × 10−7 |
| rs2236696|rs8184900|rs62216232|rs4075967|rs4075970|rs73375539|rs74357060 | 1.61 × 10−7 |
| rs8184900|rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603 | 4.78 × 10−7 |
| rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603|rs28708536 | 4.29 × 10−7 |
| rs2236696|rs8184900|rs62216232|rs4075967|rs4075970|rs73375539|rs74357060| rs28360603 | 6.39 × 10−7 |
| rs8184900|rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603| rs28708536 | 3.76 × 10−7 |
| rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603|rs28708536| rs76291974 | 2.28 × 10−7 |
| rs8184900|rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603| rs28708536|rs76291974 | 1.79 × 10−7 |
| rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603|rs28708536| rs76291974|rs62214694 | 2.86 × 10−7 |
| rs8184900|rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603| rs28708536|rs76291974|rs62214694 | 2.17 × 10−7 |
| rs62216232|rs4075967|rs4075970|rs73375539|rs74357060|rs28360603|rs28708536| rs76291974|rs62214694|rs17766525 | 2.66 × 10−7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Peña, R.; Boekstegers, F.; Silva, R.S.; Jaime, S.; Hosgood, H.D., III; Miravitlles, M.; Agustí, À.; Lorenzo Bermejo, J.; Olloquequi, J. Amerindian Ancestry Influences Genetic Susceptibility to Chronic Obstructive Pulmonary Disease. J. Pers. Med. 2020, 10, 93. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10030093
Díaz-Peña R, Boekstegers F, Silva RS, Jaime S, Hosgood HD III, Miravitlles M, Agustí À, Lorenzo Bermejo J, Olloquequi J. Amerindian Ancestry Influences Genetic Susceptibility to Chronic Obstructive Pulmonary Disease. Journal of Personalized Medicine. 2020; 10(3):93. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10030093
Chicago/Turabian StyleDíaz-Peña, Roberto, Felix Boekstegers, Rafael S. Silva, Sergio Jaime, H. Dean Hosgood, III, Marc Miravitlles, Àlvar Agustí, Justo Lorenzo Bermejo, and Jordi Olloquequi. 2020. "Amerindian Ancestry Influences Genetic Susceptibility to Chronic Obstructive Pulmonary Disease" Journal of Personalized Medicine 10, no. 3: 93. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10030093