Primary Care Physician Experiences with Integrated Population-Scale Genetic Testing: A Mixed-Methods Assessment

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Qualitative Approach: Semi-Structured Interviews
2.2.1. Recruitment
2.2.2. Data Collection
2.2.3. Data Analysis
2.3. Quantitative Approach: Survey
2.3.1. Recruitment
2.3.2. Data Collection
2.3.3. Data Analysis
3. Results
3.1. Qualitative Results
3.1.1. Participant Characteristics
3.1.2. Semi-Structured Interviews: Major Themes
3.2. Quantitative Results
3.2.1. Participant Characteristics
3.2.2. Survey Findings
Benefits of Genetic Testing
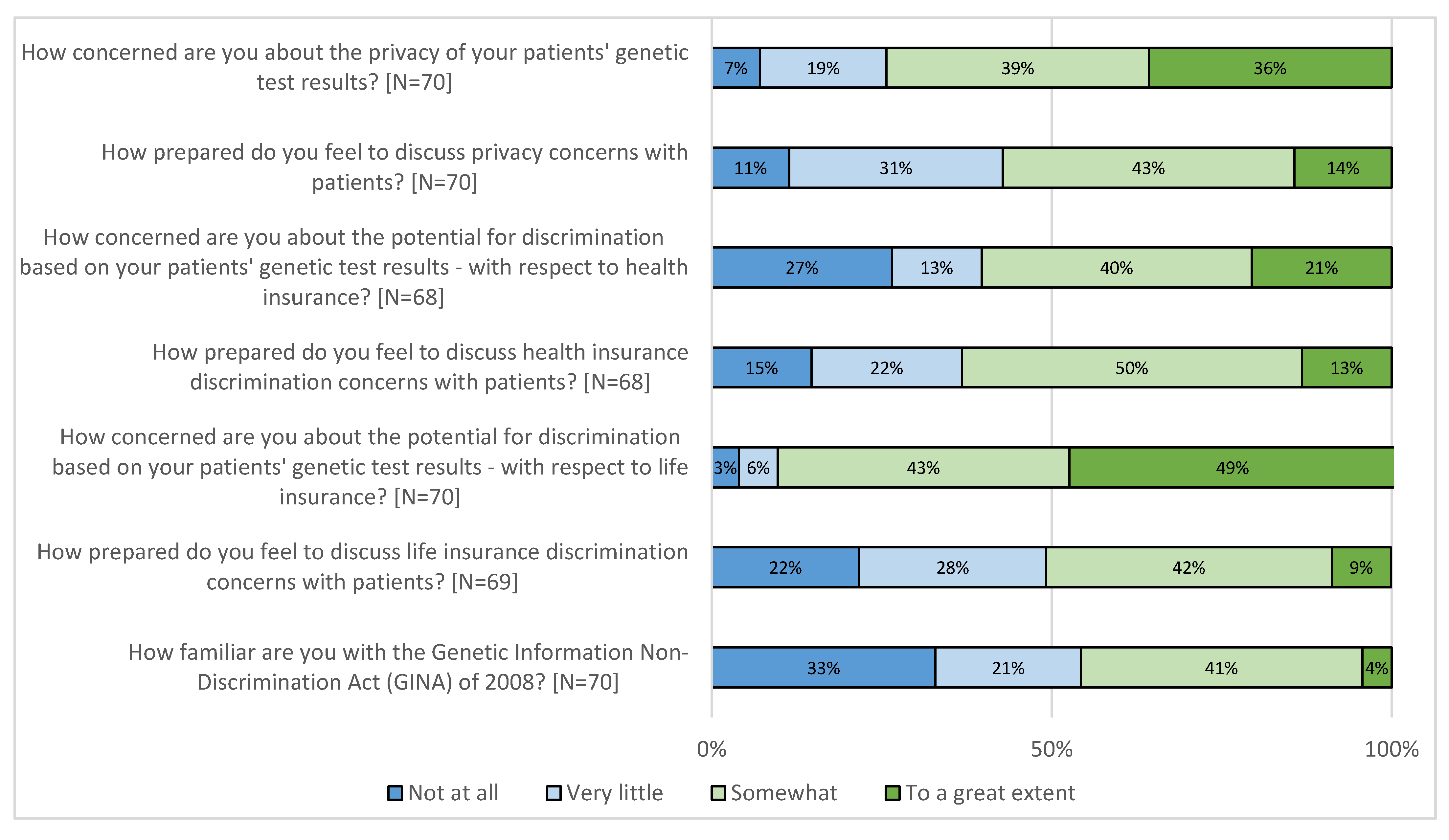
Challenges in Practice
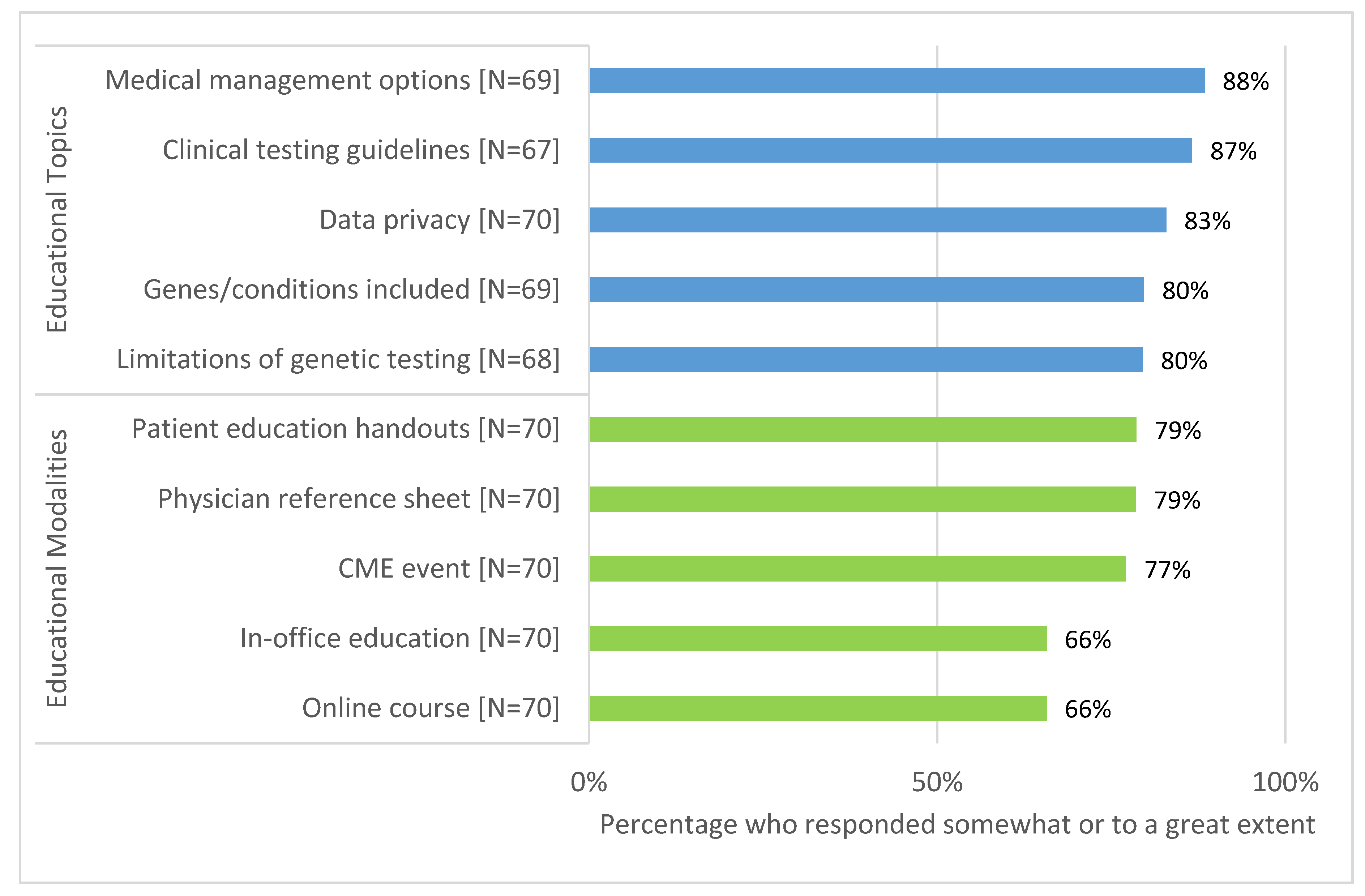
Recommendations for Additional Education
3.2.3. Exploration of Survey Results by Demographic Characteristics
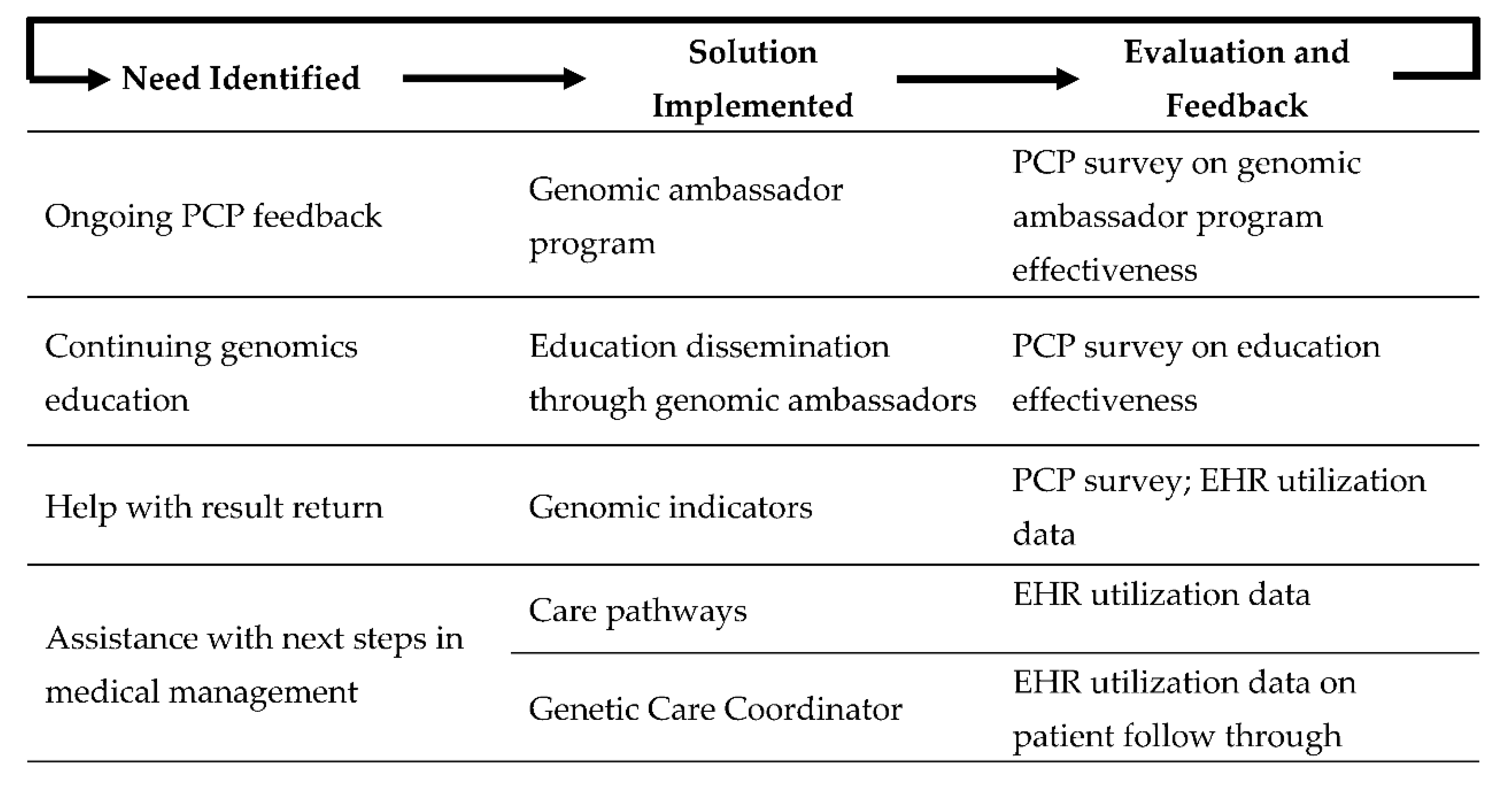
3.3. Post-Study Program Modifications
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abacan, M.; Alsubaie, L.; Barlow-Stewart, K.; Caanen, B.; Cordier, C.; Courtney, E.; Davoine, E.; Edwards, J.; Elackatt, N.J.; Gardiner, K.; et al. The Global State of the Genetic Counseling Profession. Eur. J. Hum. Genet. 2019, 27, 183–197. [Google Scholar] [CrossRef] [Green Version]
- Maiese, D.R.; Keehn, A.; Lyon, M.; Flannery, D.; Watson, M. Current conditions in medical genetics practice. Genet. Med. Off. J. Am. Coll. Med. Genet. 2019, 21, 1874–1877. [Google Scholar] [CrossRef] [Green Version]
- Dekanek, E.W.; Thull, D.L.; Massart, M.; Grubs, R.E.; Rajkovic, A.; Mai, P.L. Knowledge and opinions regarding BRCA1 and BRCA2 genetic testing among primary care physicians. J. Genet. Couns. 2020, 29, 122–130. [Google Scholar] [CrossRef]
- Owusu, O.A.; Fei, K.; Levy, K.D.; Elsey, A.R.; Pollin, T.I.; Ramirez, A.H.; Weitzel, K.W.; Horowitz, C.R. Physician-Reported Benefits and Barriers to Clinical Implementation of Genomic Medicine: A Multi-Site IGNITE-Network Survey. J. Pers. Med. 2018, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Heck, P.R.; Meyer, M.N. Population Whole Exome Screening: Primary Care Provider Attitudes About Preparedness, Information Avoidance, and Nudging. Med. Clin. N. Am. 2019, 103, 1077–1092. [Google Scholar] [CrossRef]
- Hauser, D.; Obeng, A.O.; Fei, K.; Ramos, M.A.; Horowitz, C.R. Views of Primary Care Providers on Testing Patients for Genetic Risks for Common Chronic Diseases. Health Aff. 2018, 37, 793–800. [Google Scholar] [CrossRef]
- Carroll, J.C.; Allanson, J.; Morrison, S.; Miller, F.A.; Wilson, B.J.; Permaul, J.A.; Telner, D. Informing Integration of Genomic Medicine Into Primary Care: An Assessment of Current Practice, Attitudes, and Desired Resources. Front. Genet. 2019, 10, 1189. [Google Scholar] [CrossRef] [Green Version]
- Carroll, J.C.; Makuwaza, T.; Manca, D.P.; Sopcak, N.; Permaul, J.A.; O’Brien, M.A.; Heisey, R.; Eisenhauer, E.A.; Easley, J.; Krzyzanowska, M.K.; et al. Primary care providers’ experiences with and perceptions of personalized genomic medicine. Can. Fam. Physician 2016, 62, e626–e635. [Google Scholar] [PubMed]
- Harding, B.; Webber, C.; Ruhland, L.; Dalgarno, N.; Armour, C.M.; Birtwhistle, R.; Brown, G.; Carroll, J.C.; Flavin, M.; Phillips, S.; et al. Primary care providers’ lived experiences of genetics in practice. J. Community Genet. 2019, 10, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Mikat-Stevens, N.A.; Larson, I.A.; Tarini, B.A. Primary-care providers’ perceived barriers to integration of genetics services: A systematic review of the literature. Genet. Med. Off. J. Am. Coll. Med. Genet. 2015, 17, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, J.G.; Abdiwahab, E.; Edwards, H.M.; Fang, M.L.; Jdayani, A.; Breslau, E.S. Primary care providers’ cancer genetic testing-related knowledge, attitudes, and communication behaviors: A systematic review and research agenda. J. Gen. Intern. Med. 2017, 32, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Jonas, M.C.; Suwannarat, P.; Burnett-Hartman, A.; Carroll, N.; Turner, M.; Janes, K.; Truong, C.; Blum-Barnett, E.; Aziz, N.; McGlynn, E.A. Physician Experience with Direct-To-Consumer Genetic Testing in Kaiser Permanente. J. Pers. Med. 2019, 9, 47. [Google Scholar] [CrossRef] [Green Version]
- Arora, N.S.; Davis, J.K.; Kirby, C.; McGuire, A.A.L.; Green, R.C.; Blumenthal-Barby, J.S.; Ubel, P.A. Communication challenges for nongeneticist physicians relaying clinical genomic results. Pers. Med. 2016, 14, 423–431. [Google Scholar] [CrossRef]
- Puryear, L.; Downs, N.; Nevedal, A.; Lewis, E.T.; Ormond, K.E.; Bregendahl, M.; Suarez, C.J.; David, S.P.; Charlap, S.; Chu, I.; et al. Patient and provider perspectives on the development of personalized medicine: A mixed-methods approach. J. Community Genet. 2018, 9, 283–291. [Google Scholar] [CrossRef]
- Lerner, B.; Marshall, N.; Oishi, S.; Lanto, A.; Lee, M.; Hamilton, A.B.; Yano, E.M.; Scheuner, M.T. The value of genetic testing: Beyond clinical utility. Genet. Med. Off. J. Am. Coll. Med. Genet. 2017, 19, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Vassy, J.L.; Christensen, K.D.; Schonman, E.F.; Blout, C.L.; Robinson, J.O.; Krier, J.B.; Diamond, P.M.; Lebo, M.; Machini, K.; Azzariti, D.R.; et al. The Impact of Whole-Genome Sequencing on the Primary Care and Outcomes of Healthy Adult Patients: A Pilot Randomized Trial. Ann. Intern. Med. 2017, 167, 159–169. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 2nd ed.; Sage Publications: Los Angeles, CA, USA, 2011. [Google Scholar]
- Willis, G.B. Cognitive Interviewing. A Tool for Improving Questionnaire Design; Sage Publishing: New York, NY, USA, 2004. [Google Scholar]
- Atlasti Qualitative Data Analysis. Available online: https://atlasti.com/ (accessed on 25 August 2020).
- Glaser, B.G.; Strauss, A.A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Dillman, D.A.; Smyth, J.D.; Christian, L.M. Internet, Phone, Mail, and Mixed-Mode Surveys, 4th ed.; Wiley: Hoboken, NJ, USA, 2014. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- SAS Institute Inc. Base SAS® 9.3 Procedures Guide; SAS Institute Inc.: Cary, NC, USA, 2011. [Google Scholar]
- Starks, H.; Trinidad, S.B. Choose your method: A comparison of phenomenology, discourse analysis, and grounded theory. Qual. Health Res. 2007, 17, 1372–1380. [Google Scholar] [CrossRef]
- Kurnat-Thoma, E. Educational and Ethical Considerations for Genetic Test Implementation within Health Care Systems. Netw. Syst. Med. 2020, 3, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Klitzman, R.; Chung, W.; Marder, K.; Shanmugham, A.; Chin, L.J.; Stark, M.; Leu, C.S.; Appelbaum, P.S. Attitudes and practices among internists concerning genetic testing. J. Genet. Couns. 2013, 22, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Lowstuter, K.J.; Sand, S.; Blazer, K.R.; MacDonald, D.J.; Banks, K.C.; Lee, C.A.; Schwerin, B.U.; Juarez, M.; Uman, G.C.; Weitzel, J.N. Influence of genetic discrimination perceptions and knowledge on cancer genetics referral practice among clinicians. Genet. Med. Off. J. Am. Coll. Med. Genet. 2008, 10, 691–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemke, A.; Amendola, L.M.; Thompson, J.; Dunnenberger, H.M.; Kuchta, K.; Wang, C.; Dilzell-Yu, K.; Hulick, P.J. Patient-reported outcomes and experiences with population genetic testing offered through a primary care network. 2020; in preparation. [Google Scholar]
- Haga, S.B. Overview of Policy, Ethical, and Social Considerations in Genomic and Personalized Medicine. In Genomic and Precision Medicine: Primary Care, 3rd ed.; David, S.P., Ed.; Academic Press: Cambridge, MA, USA, 2017; pp. 19–43. [Google Scholar]
- McClaren, B.J.; Crellin, E.; Janinski, M.; Nisselle, A.E.; Ng, L.; Metcalfe, S.A.; Gaff, C.L. Preparing Medical Specialists for Genomic Medicine: Continuing Education Should Include Opportunities for Experiential Learning. Front. Genet. 2020, 11, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linzer, M.; Manwell, L.B.; Williams, E.S.; Bobula, J.A.; Brown, R.L.; Varkey, A.B.; Man, B.; McMurray, J.E.; Maguire, A.; Horner-Ibler, B.; et al. Working conditions in primary care: Physician reactions and care quality. Ann. Intern. Med. 2009, 151, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.R.; Barton, A.J. The emergence of a learning healthcare system. Clin. Nurse Spec. 2013, 27, 7–9. [Google Scholar] [CrossRef]
- Lemke, A.A.; Thompson, J.; Hulick, P.J.; Sereika, A.W.; Johnson, C.; Oshman, L.; Dunnenberger, H.M. Primary care physician experiences utilizing a family health history tool with electronic health record-integrated clinical decision support: An implementation process assessment. J. Community Genet. 2020, 11, 339–350. [Google Scholar] [CrossRef]
- Lemke, A.A.; Selkirk, C.G.H.; Glaser, N.S.; Sereika, A.W.; Wake, D.T.; Hulick, P.J.; Dunnenberger, H.M. Primary care physician experiences with integrated pharmacogenomic testing in a community health system. Pers. Med. 2017, 14, 389–400. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Themes and Sub-Themes | Illustrative Interview Quotes |
|---|---|
| Benefits to clinical care provision | |
| Detect/prevent disease | “The benefits are that we discover something on genetic testing that sheds light on increased risk or something we are not screening for; might trigger additional screening.” (P5) |
| Increase access to genetic services | “For some reason it was really hard to get people to genetics, even when they had compelling family histories; …there’s a lower barrier with integrated testing.” (P9) |
| Identify patients at risk with no family history of disease | “I have had some patients, adopted and those not knowing their family histories, and one came back as Lynch positive. So changed everything I counseled and recommended.” (P10) |
| Improve medication management based on pharmacogenomics results | “I have had a number of patients who are on a lot of antidepressants and we’ve been able to fine tune their medication regimes as a result of testing.” (P7) |
| Family implications | “Then also to know for children, so that you know if kids need to be screened for anything as well.” (P3) |
| Challenges in practice | |
| Privacy and insurance concerns | “There are some people out there who really worry about the idea of their DNA being tested…is somebody going to use it against them, like for health/life insurance.” (P9) |
| Time constraints and competing priorities | “There’s such a big list of things that we need to review and talk about and recommend to patients, that it becomes a challenge for time having yet another thing to talk about.” (P5) |
| Interpreting and discussing results | “Having potentially to field questions from patients, where I don’t have the skillset to tell them. A negative result is pretty easy, but for positive results I don’t have the full skillset.” (P15) |
| Unclear about next steps for medical management | “Sometimes there are results we are unfamiliar with or unprepared to deal with, and not sure about where to direct patients to go and what surveillance is appropriate.” (P7) |
| Role in results disclosure workflow unclear | “I can’t tell like, did somebody call the patient, am I supposed to be doing something? I can’t see anything in the chart to know if someone got a hold of the patient with results.” (P14) |
| Recommended Improvements | |
| Patient education resources | “I think brochures are key because the patient can actually hold onto it and take a look as opposed to just on electronic format.” (P12) |
| Physician education | “I think there are still physicians who don’t buy in because they feel like this is not part of their primary care field. And they don’t understand the genes being tested. We need to provide easy access to CME.” (P6) |
| Additional resources | “Some sort of reference, even if it was just literally a PDF that people could download on their own.” (P2) |
| N (%) | |
|---|---|
| Total Respondents | 70 |
| Age group: [N = 69] | |
| 20–29 | 0 (0.0) |
| 30–39 | 17 (24.6) |
| 40–49 | 23 (33.3) |
| 50–59 | 18 (26.1) |
| 60–69 | 8 (11.6) |
| 70 or older | 3 (4.4) |
| Gender: [N = 69] | |
| Male | 34 (49.3) |
| Female | 35 (50.7) |
| Non-binary | 0 (0.0) |
| Other | 0 (0.0) |
| Race/Ethnicity: [N = 65] | |
| American Indian or Alaska Native | 0 (0.0) |
| Asian | 12 (18.5) |
| Black or African American | 0 (0.0) |
| Hispanic or Latino | 0 (0.0) |
| Native Hawaiian or Other Pacific Islander | 1 (1.5) |
| White | 52 (80.0) |
| Primary area of practice: [N = 70] | |
| Internal Medicine | 41 (58.6) |
| Family Medicine | 18 (25.7) |
| Obstetrics/Gynecology | 11 (15.7) |
| Other | 0 (0.0) |
| How many years have you been in clinical practice? [N = 70] | |
| 0–5 | 10 (14.3) |
| 6–10 | 10 (14.3) |
| 11–15 | 8 (11.4) |
| 16–20 | 18 (25.7) |
| 21 or more | 24 (34.3) |
| Percentage of time is in patient care-related activities: [N = 69] | |
| 0–30 | 0 (0.0) |
| 31–40 | 2 (2.9) |
| 41–50 | 1 (1.4) |
| 51 or more | 67 (95.7) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemke, A.A.; Amendola, L.M.; Kuchta, K.; Dunnenberger, H.M.; Thompson, J.; Johnson, C.; Ilbawi, N.; Oshman, L.; Hulick, P.J. Primary Care Physician Experiences with Integrated Population-Scale Genetic Testing: A Mixed-Methods Assessment. J. Pers. Med. 2020, 10, 165. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10040165
Lemke AA, Amendola LM, Kuchta K, Dunnenberger HM, Thompson J, Johnson C, Ilbawi N, Oshman L, Hulick PJ. Primary Care Physician Experiences with Integrated Population-Scale Genetic Testing: A Mixed-Methods Assessment. Journal of Personalized Medicine. 2020; 10(4):165. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10040165
Chicago/Turabian StyleLemke, Amy A., Laura M. Amendola, Kristine Kuchta, Henry M. Dunnenberger, Jennifer Thompson, Christian Johnson, Nadim Ilbawi, Lauren Oshman, and Peter J. Hulick. 2020. "Primary Care Physician Experiences with Integrated Population-Scale Genetic Testing: A Mixed-Methods Assessment" Journal of Personalized Medicine 10, no. 4: 165. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10040165