
New Evidence of Potential Benefits of Dexamethasone and Added on Therapy of Fludrocortisone on Clinical Outcomes of Corticosteroid in Sepsis Patients: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
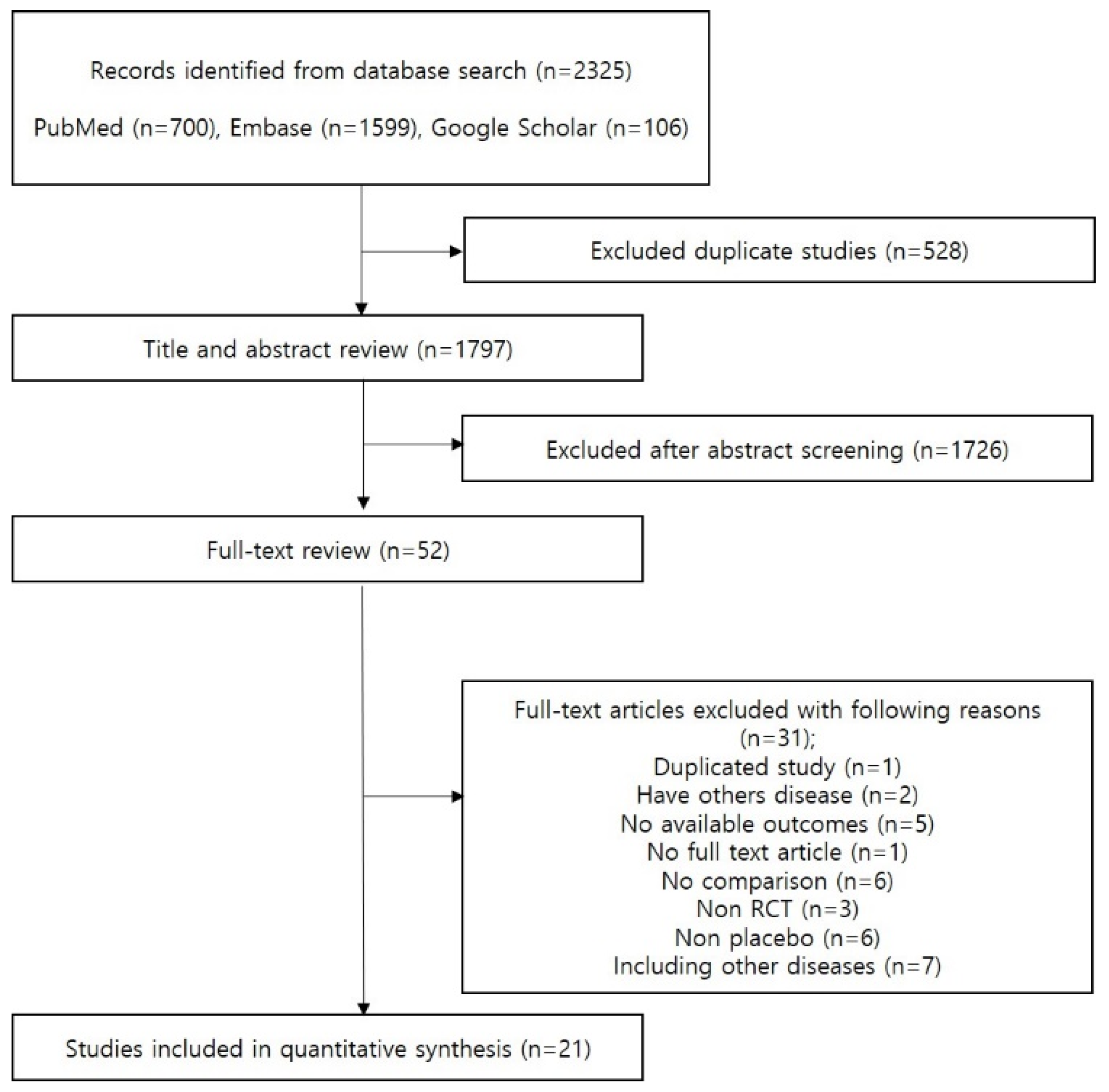
2.1. Search Strategy and Study Selection
2.2. Risk of Bias Assessment
2.3. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
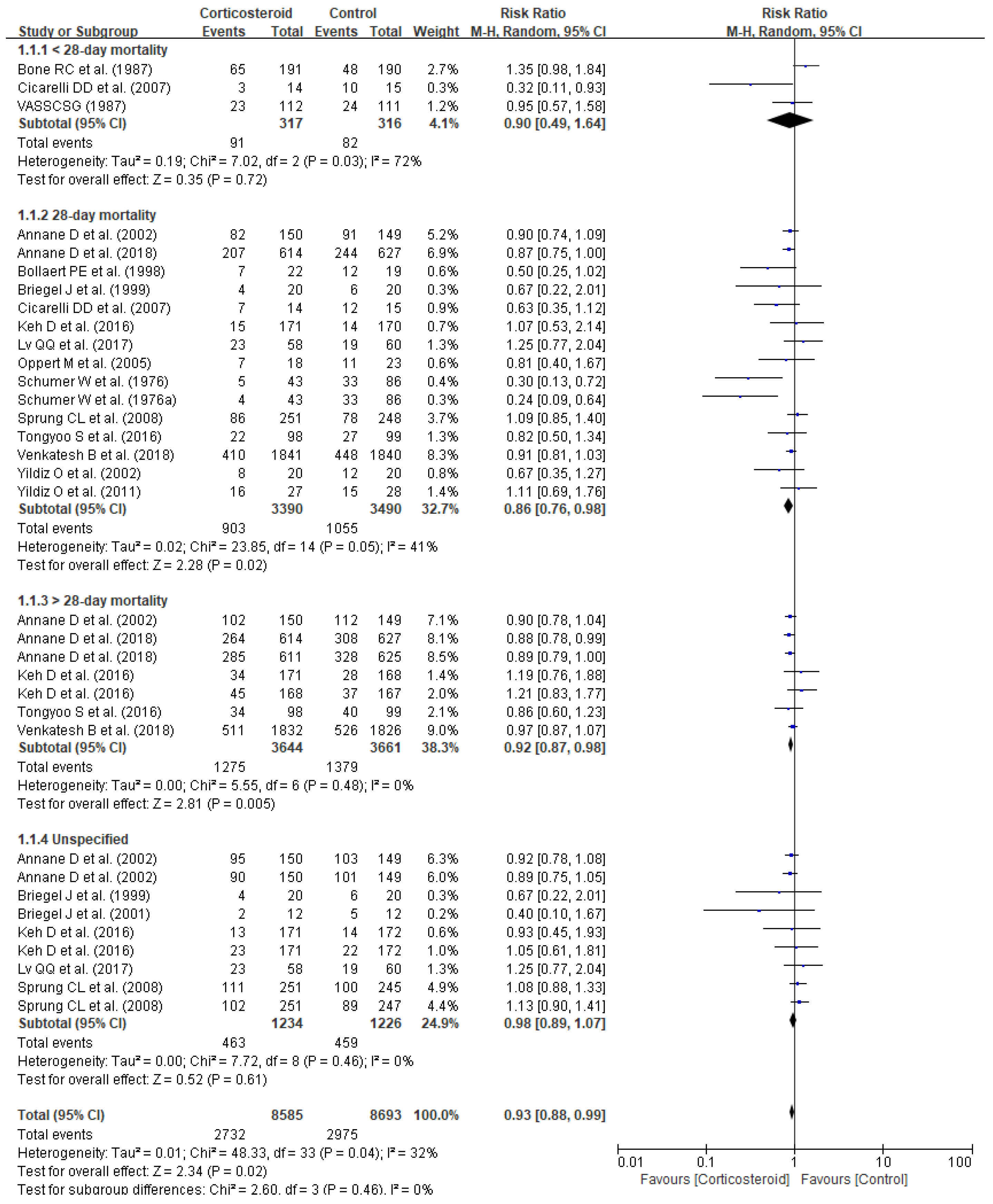
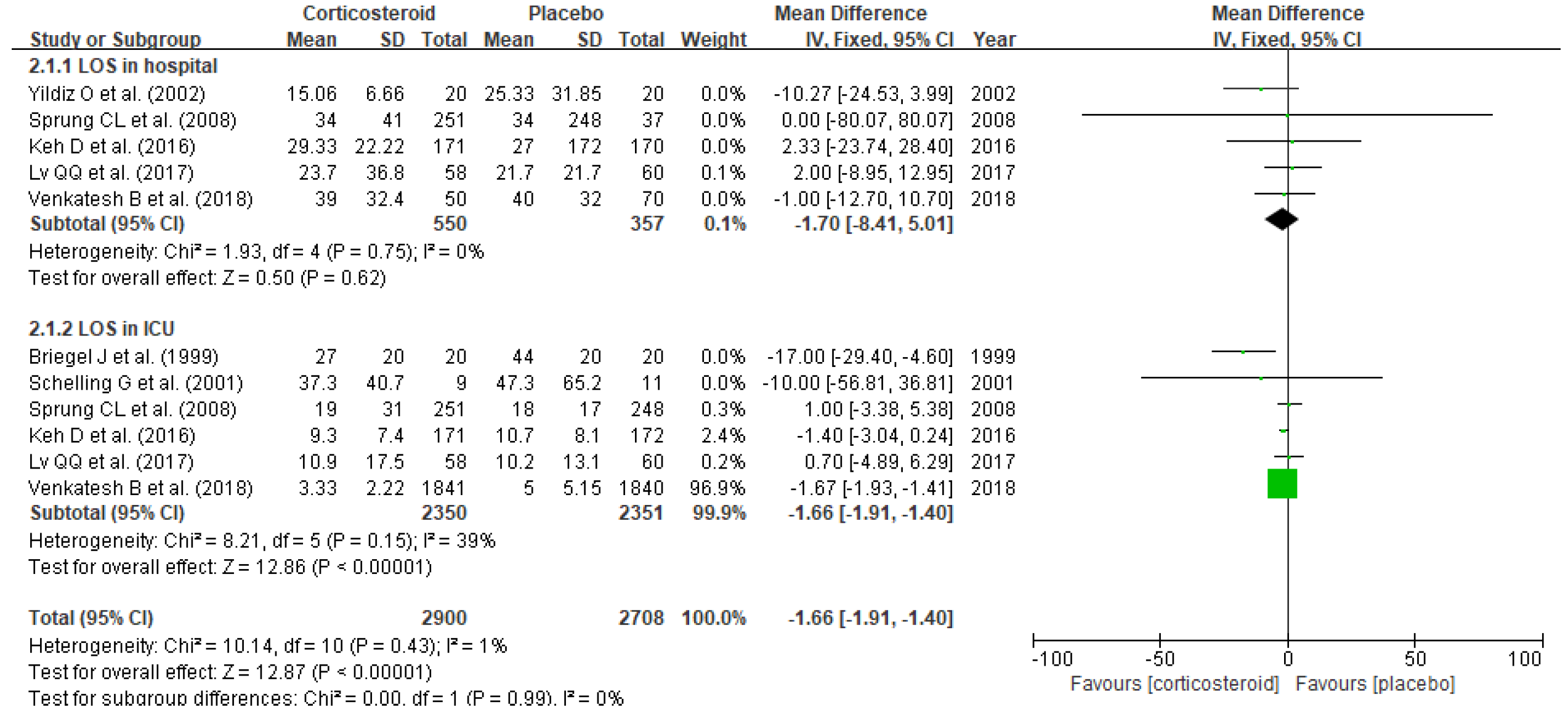
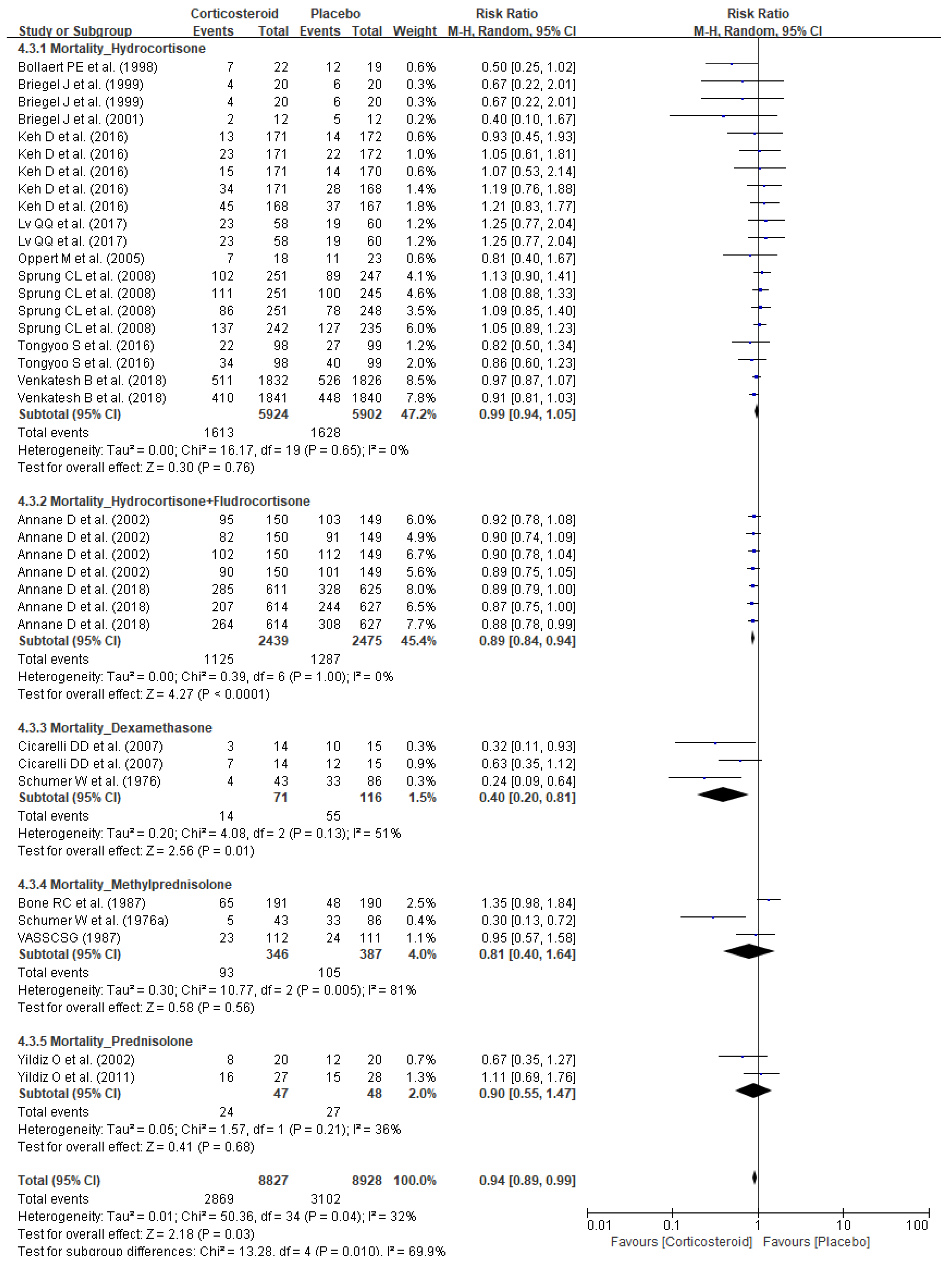
3.2. Clinical Outcomes
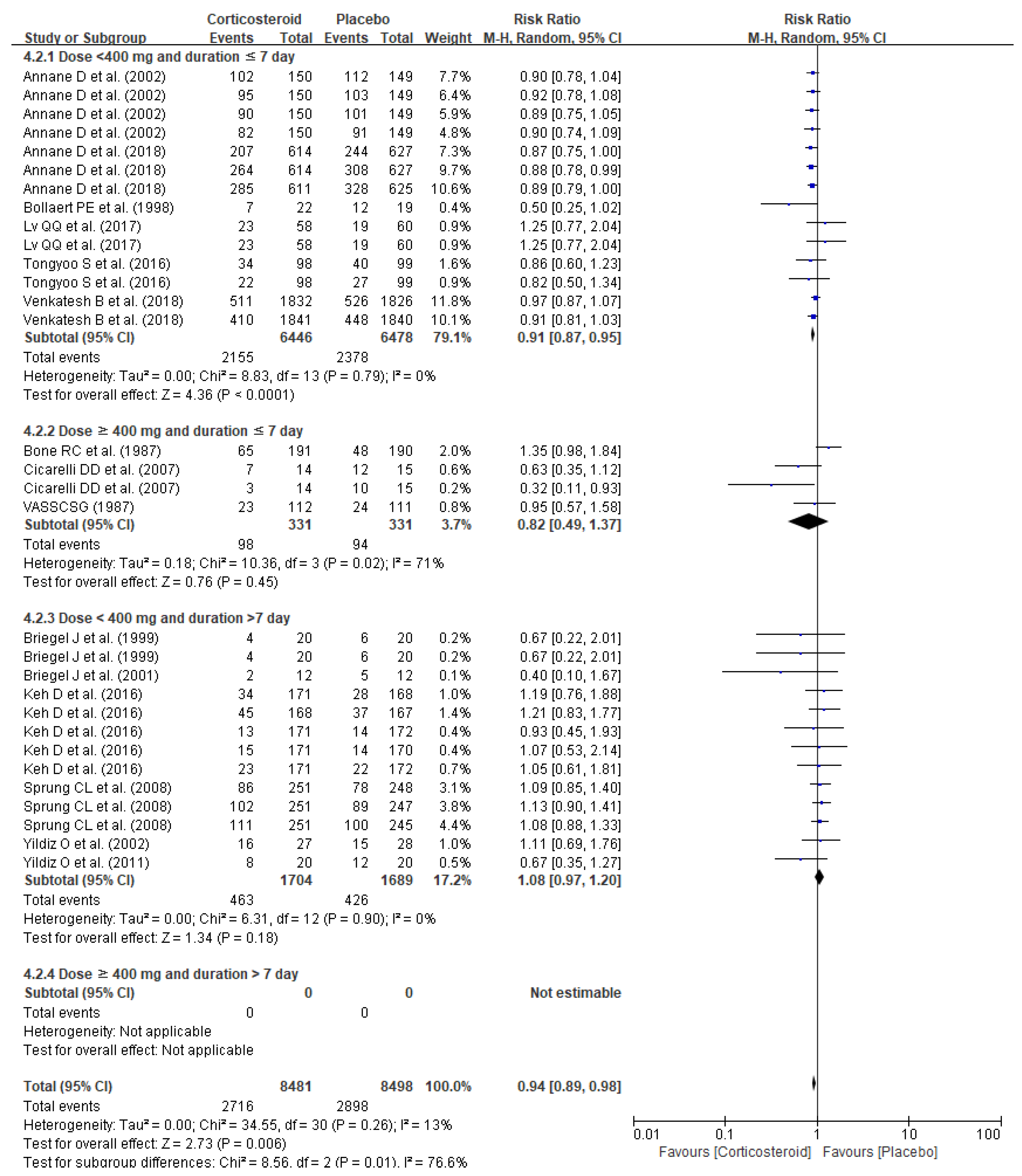
3.3. Subgroup Analyses
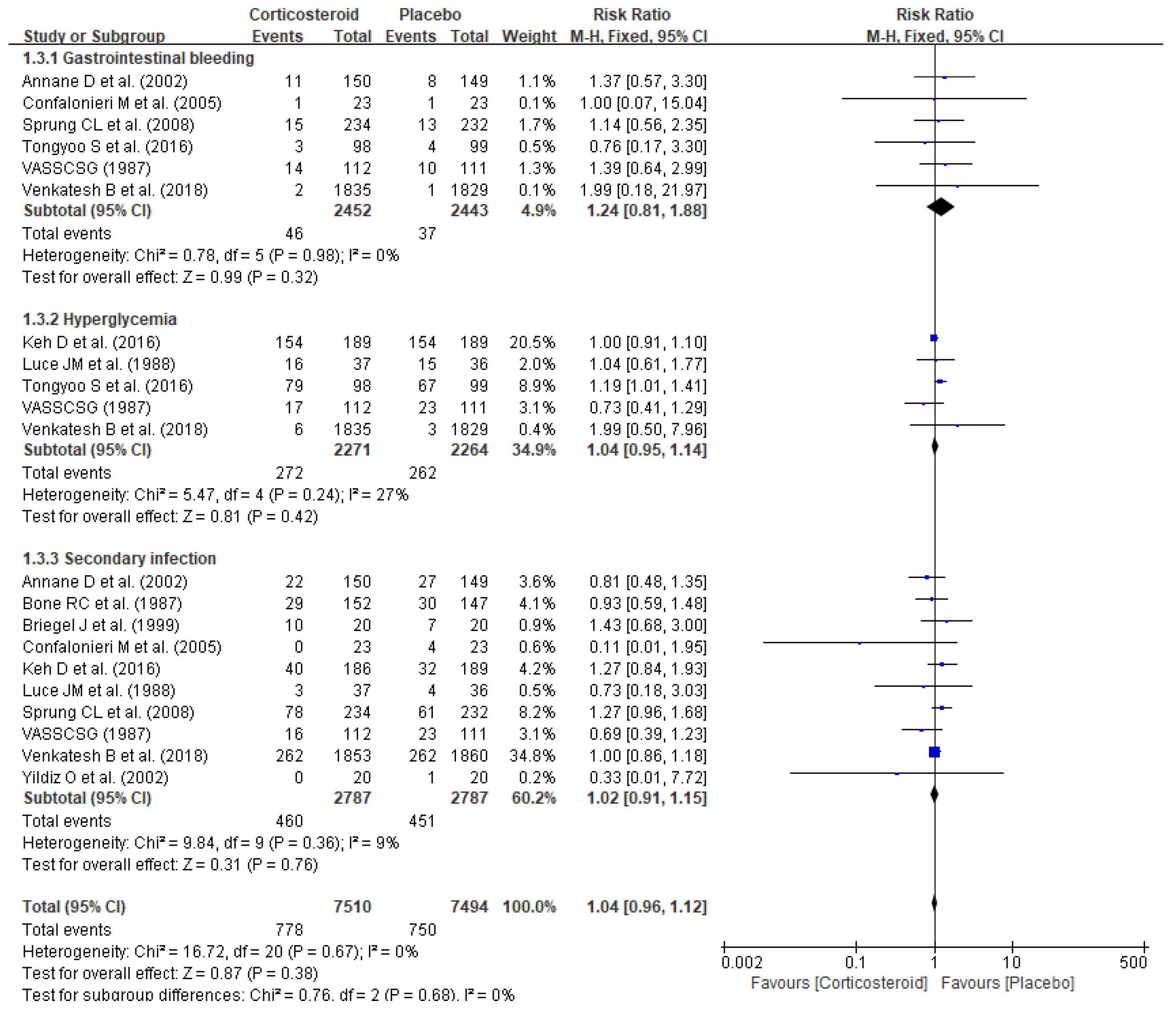
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hotchkiss, R.S.; Moldawer, L.L.; Opal, S.M.; Reinhart, K.; Turnbull, I.R.; Vincent, J.L. Sepsis and septic shock. Nat. Rev. Dis. Primers 2016, 2, 16045. [Google Scholar] [CrossRef]
- Ladha, E.; House-Kokan, M.; Gillespie, M. The ABCCs of sepsis: A framework for understanding the pathophysiology of sepsis. Can. J. Crit. Care Nurs. 2019, 30, 12–21. [Google Scholar]
- Rello, J.; Valenzuela-Sánchez, F.; Ruiz-Rodriguez, M.; Moyano, S. Sepsis: A Review of Advances in Management. Adv. Ther. 2017, 34, 2393–2411. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: With supraphysiologic doses of hydrocortisone. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef]
- Mok, K.; Christian, M.D.; Nelson, S.; Burry, L. Time to Administration of Antibiotics among Inpatients with Severe Sepsis or Septic Shock. Can. J. Hosp. Pharm. 2014, 67, 213–219. [Google Scholar] [CrossRef]
- Annane, D. The Role of ACTH and Corticosteroids for Sepsis and Septic Shock: An Update. Front. Endocrinol. 2016, 7, 70. [Google Scholar] [CrossRef] [PubMed]
- Annane, D.; Pastores, S.M.; Rochwerg, B.; Arlt, W.; Balk, R.A.; Beishuizen, A.; Briegel, J.; Carcillo, J.; Christ-Crain, M.; Cooper, M.S.; et al. Guidelines for the diagnosis and management of critical illness-related corticosteroid insufficiency (CIRCI) in critically ill patients (Part I): Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017. Intensive Care Med. 2017, 43, 1751–1763. [Google Scholar] [CrossRef]
- Rochwerg, B.; Oczkowski, S.; Siemieniuk, R.A.; Menon, K.; Szczeklik, W.; English, S.; Agoritsas, T.; Belley-Cote, E.; D’Aragon, F.; Alhazzani, W.; et al. Corticosteroids in sepsis: An updated systematic review and meta-analysis (protocol). BMJ Open 2017, 7, e016847. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.; Zhang, Y.; Tang, J.; Lunsford, L.D.; Li, T.; Tang, R.; He, J.; Xu, P.; Faramand, A.; Xu, J.; et al. Association of corticosteroid treatment with outcomes in adult patients with sepsis: A systematic review and meta-analysis. JAMA Intern. Med. 2019, 179, 213–223. [Google Scholar] [CrossRef]
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell. Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Bollaert, P.-E.; Charpentier, C.; Levy, B.; Debouverie, M.; Audibert, G.; Larcan, A. Reversal of late septic shock with supraphysiologic doses of hydrocortisone. Crit. Care Med. 1998, 26, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Briegel, J.; Forst, H.; Haller, M.; Schelling, G.; Kilger, E.; Kuprat, G.; Hemmer, B.; Hummel, T.; Lenhart, A.; Heyduck, M.; et al. Stress doses of hydrocortisone reverse hyperdynamic septic shock: A prospective, randomized, double-blind, single-center study. Crit. Care Med. 1999, 27, 723–732. [Google Scholar] [CrossRef]
- Briegel, J.; Jochum, M.; Gippner-Steppert, C.; Thiel, M. Immunomodulation in septic shock: Hydrocortisone differentially regulates cytokine responses. J. Am. Soc. Nephrol. 2001, 12 (Suppl. 17), S70–S74. [Google Scholar] [CrossRef] [PubMed]
- Confalonieri, M.; Urbino, R.; Potena, A.; Piattella, M.; Parigi, P.; Puccio, G.; Della Porta, R.; Giorgio, C.; Blasi, F.; Umberger, R.; et al. Hydrocortisone infusion for severe community-acquired pneumonia: A preliminary randomized study. Am. J. Respir. Crit. Care Med. 2005, 171, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, I.; Briegel, J.; Schliephake, F.; Hoelzl, A.; Chouker, A.; Hummel, T.; Schelling, G.; Thiel, M. Stress doses of hydrocortisone in septic shock: Beneficial effects on opsonization-dependent neutrophil functions. Intensive Care Med. 2008, 34, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Keh, D.; Trips, E.; Marx, G.; Wirtz, S.P.; Abduljawwad, E.; Bercker, S.; Bogatsch, H.; Briegel, J.; Engel, C.; Gerlach, H.; et al. Effect of hydrocortisone on development of shock among patients with severe sepsis: The HYPRESS randomized clinical trial. JAMA 2016, 316, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Moreno, R.; Sprung, C.L.; Annane, D.; Chevret, S.; Briegel, J.; Keh, D.; Singer, M.; Weiss, Y.G.; Payen, D.; Cuthbertson, B.H.; et al. Time course of organ failure in patients with septic shock treated with hydrocortisone: Results of the Corticus study. Intensive Care Med. 2011, 37, 1765–1772. [Google Scholar] [CrossRef]
- Oppert, M.; Schindler, R.; Husung, C.; Offermann, K.; Gräf, K.-J.; Boenisch, O.; Barckow, D.; Frei, U.; Eckardt, K.-U. Low-dose hydrocortisone improves shock reversal and reduces cytokine levels in early hyperdynamic septic shock. Crit. Care Med. 2005, 33, 2457–2464. [Google Scholar] [CrossRef]
- Schelling, G.; Briegel, J.; Roozendaal, B.; Stoll, C.; Rothenhäusler, H.-B.; Kapfhammer, H.-P. The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder in survivors. Biol. Psychiatry 2001, 50, 978–985. [Google Scholar] [CrossRef]
- Sprung, C.L.; Annane, D.; Keh, D.; Moreno, R.; Singer, M.; Freivogel, K.; Weiss, Y.G.; Benbenishty, J.; Kalenka, A.; Forst, H.; et al. Hydrocortisone Therapy for Patients with Septic Shock. N. Engl. J. Med. 2008, 358, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Tongyoo, S.; Permpikul, C.; Mongkolpun, W.; Vattanavanit, V.; Udompanturak, S.; Kocak, M.; Meduri, G.U. Hydrocortisone treatment in early sepsis-associated acute respiratory distress syndrome: Results of a randomized controlled trial. Crit. Care 2016, 20, 329. [Google Scholar] [CrossRef]
- Venkatesh, B.; Finfer, S.; Cohen, J.; Rajbhandari, D.; Arabi, Y.; Bellomo, R.; Billot, L.; Correa, M.; Glass, P.; Harward, M.; et al. Adjunctive glucocorticoid therapy in patients with septic shock. N. Engl. J. Med. 2018, 378, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Lv, Q.-Q.; Gu, X.-H.; Chen, Q.-H.; Yu, J.-Q.; Zheng, R.-Q. Early initiation of low-dose hydrocortisone treatment for septic shock in adults: A randomized clinical trial. Am. J. Emerg. Med. 2017, 35, 1810–1814. [Google Scholar] [CrossRef]
- Annane, D.; Renault, A.; Brun-Buisson, C.; Megarbane, B.; Quenot, J.-P.; Siami, S.; Cariou, A.; Forceville, X.; Schwebel, C.; Martin, C.; et al. Hydrocortisone plus Fludrocortisone for Adults with Septic Shock. N. Engl. J. Med. 2018, 378, 809–818. [Google Scholar] [CrossRef]
- Annane, D.; Sébille, V.; Charpentier, C.; Bollaert, P.-E.; François, B.; Korach, J.-M.; Capellier, G.; Cohen, Y.; Azoulay, E.; Troché, G.; et al. Effect of Treatment with Low Doses of Hydrocortisone and Fludrocortisone on Mortality in Patients with Septic Shock. JAMA 2002, 288, 862–871. [Google Scholar] [CrossRef]
- Cicarelli, D.D.; Vieira, J.E.; Benseñor, F.E.M. Early dexamethasone treatment for septic shock patients: A prospective randomized clinical trial. Sao Paulo Med. J. 2007, 125, 237–241. [Google Scholar] [CrossRef]
- Schumer, W. Steroids in the treatment of clinical septic shock. Ann. Surg. 1976, 184, 333–341. [Google Scholar] [CrossRef]
- Bone, R.C.; Fisher, C.J.; Clemmer, T.P.; Slotman, G.J.; Metz, C.A.; Balk, R.A.; The Methylprednisolone Severe Sepsis Study Group. A Controlled Clinical Trial of High-Dose Methylprednisolone in the Treatment of Severe Sepsis and Septic Shock. N. Engl. J. Med. 1987, 317, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Luce, J.M.; Montgomery, A.B.; Marks, J.D.; Turner, J.; Metz, C.A.; Murray, J.F. Ineffectiveness of High-dose Methylprednisolone in Preventing Parenchymal Lung Injury and Improving Mortality in Patients with Septic Shock. Am. Rev. Respir. Dis. 1988, 138, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Veterans Administration Systemic Sepsis Cooperative Study Group. Effect of high-dose glucocorticoid therapy on mortality in patients with clinical signs of systemic sepsis. N. Engl. J. Med. 1987, 317, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, O.; Doganay, M.; Aygen, B.; Güven, M.; Klelestimur, F.; Tutuş, A. Physiological-dose steroid therapy in sepsis [ISRCTN36253388]. Crit. Care 2002, 6, 251–259. [Google Scholar] [CrossRef]
- Yildiz, O.; Tanriverdi, F.; Simsek, S.; Aygen, B.; Kelestimur, F. The effects of moderate-dose steroid therapy in sepsis: A placebo-controlled, randomized study. J. Res. Med. Sci. 2011, 16, 1410–1421. [Google Scholar]
- Minneci, P.; Deans, K.; Eichacker, P.; Natanson, C. The effects of steroids during sepsis depend on dose and severity of illness: An updated meta-analysis. Clin. Microbiol. Infect. 2009, 15, 308–318. [Google Scholar] [CrossRef]
- Ahmed, M.H.; Hassan, A. Dexamethasone for the Treatment of Coronavirus Disease (COVID-19): A Review. SN Compr. Clin. Med. 2020, 2, 2637–2646. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in hospitalized patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Treatment (N) | Control (N) | Inclusion Criteria | Dose | Hydrocortisone Equivalent (mg/Day) | Duration (Day) | Outcomes |
|---|---|---|---|---|---|---|---|
| Bollaert PE et al., (1998) [14] | Hydrocortisone (N = 22) | Placebo (N = 19) | Septic shock requiring catecholamine for >48 h | 300 mg IV/day | 300 | <5 | Mortality |
| Briegel J et al., (1999) [15] | Hydrocortisone (N = 20) | Placebo (N = 20) | Adult patients who met ACCP/SCCM criteria for septic shock | 100 mg (loading dose within 30 min) followed by a continuous infusion of 0.18 mg/kg/h (sepsis) or 0.08 mg/kg/h (septic shock) for 6 days | 359.2 | 4–8 | Mortality Secondary infection Mechanical ventilation LOS in ICU |
| Confalonieri M et al., (2005) [17] | Hydrocortisone (N = 23) | Placebo (N = 23) | Adult patients diagnosed with sepsis | 200 mg (IV bolus) followed by 10 mg/h for 7 days | 440 | 7 | Mortality LOS in ICU LOS in hospital Mechanical ventilation ARDS Secondary infection Respiratory failure Organ failure Gastrointestinal bleeding |
| Briegel J et al., (2001) [16] | Hydrocortisone (N = 12) | Placebo (N = 12) | Patients with septic shock | Infusion of 100 mg of hydrocortisone, followed by 0.18 mg/kg/h (continuous infusion) | 359.2 | <6 | Mortality |
| Kaufmann I et al., (2008) [18] | Hydrocortisone (N = 15) | Placebo (N = 15) | Patients admitted to ICU and met criteria for septic shock | 100 mg (IV bolus), followed by 10 mg/h (continuous infusion) | 340 | 1 | Organ failure Respiratory failure |
| Keh D et al.,/HYPRESS study (2016) [19] | Hydrocortisone (N = 171) | Placebo (N = 172) | Sepsis patients >18 years | 200 mg/day (continuous infusion) for 5 days, 100 mg (day 6 and 7), 50 mg (day 8 and 9), on days 8 and 9, and 25 mg (day 10 and 11) | 200 | 5–11 | Mortality LOS in ICU LOS in hospital Mechanical ventilation Secondary infection Respiratory failure Organ failure |
| Lv QQ et al., (2017) [26] | Hydrocortisone (N = 58) | Placebo (N = 60) | Age 18 years old or older, onset of septic shock within 6 h | 200 mg/day | 200 | 6 | Mortality LOS in ICU LOS in hospital Reversal of shock |
| Moreno R et al.,/CROTICUS (2011) [20] | Hydrocortisone (N = 251) | Placebo (N = 248) | Patients >18 years diagnosed with sepsis or septic shock | 50 mg (IV bolus every 6 h for 5 days), 50 mg (IV every 12 h for days 6–8), 50 mg (IV every 24 h for days 9–11) | 200 | 11 | Organ failure Respiratory failure |
| Oppert M et al., (2005) [21] | Hydrocortisone (N = 18) | Placebo (N = 23) | Adult patients met criteria for sepsis | 50 mg (IV bolus) followed by 0.18 mg/kg body of weight/h (continuous infusion) | 309.2 | No record | Mortality |
| Schelling G et al., (2001) [22] | Hydrocortisone (N = 9) | Placebo (N = 11) | Adult patients with hyperdynamic septic shock | 100 mg IV, 0.18 mg/kg/h | 359.2 | 6 | LOS in ICU Respiratory failure |
| Sprung CL et al., (2008) [23] | Hydrocortisone (N = 251) | Placebo (N = 248) | Adults septic shock patients | 50 mg of IV every 6 h for 5 days; dose-tapering for 6 days | 200 | 11 | Mortality LOS in ICU LOS in hospital Secondary infection Respiratory failure Reversal of shock Gastrointestinal bleeding Organ failure |
| Tongyoo S et al., (2016) [24] | Hydrocortisone (N = 98) | Placebo (N = 99) | Age ≥18 years meeting the criteria for severe sepsis or septic shock | 50 mg per 6 h (200 mg/day) | 200 | 7 | Mortality Mechanical ventilation Mechanical ventilation-free time Secondary infection Hyperglycemia Gastrointestinal bleeding |
| Venkatesh B et al., (2018) [25] | Hydrocortisone (N = 1853) | Placebo (N = 1860) | Sepsis adult patients (>18 years) | 200 mg/day | 200 | ≤7 | Mortality Resolution of shock Reversal of shock LOS in ICU LOS in hospital Mechanical ventilation-free time Secondary infection Gastrointestinal bleeding |
| Annane D et al., (2002) [28] | Hydrocortisone and Fludrocortisone (N = 150) | Placebo (N = 149) | Adults (18 years or older) and hospitalized in ICU with sepsis/septic shock | Hydrocortisone (50 mg IV bolus every 6 h) and fludrocortisone (50 µg tablet once daily) | 200.5 | 7 | Mortality Secondary infection Gastrointestinal bleeding |
| Annane D et al., (2018) [27] | Hydrocortisone and Fludrocortisone (N = 614) | Placebo (N = 627) | Indisputable or probable septic shock patients | Hydrocortisone 50 mg IV every 6 h, fludrocortisone 50 μg tablet/day for 7 days | 200.5 | 7 | Mortality Mechanical ventilation |
| Cicarelli DD et al., (2007) [29] | Dexamethasone (N = 15) | Placebo (N = 15) | Septic shock patients aged ≥18 years and admitted to ICU | 0.2 mg/kg IV at intervals of 36 h (total 3 doses) | 640 | 4.5 | Mortality Mechanical ventilation |
| Schumer W et al., (1976) [30] | Dexamethasone (N = 43) | Placebo (N = 86) | Septic shock | 3 mg/kg | 480 | No record | Mortality |
| Methylprednisolone (N = 43) | Placebo (N = 86) | Septic shock | 30 mg/kg | 900 | No record | Mortality | |
| Bone RC et al., (1987) [31] | Methylprednisolone (N = 191) | Placebo (N = 190) | Adult patients with infection plus the presence of fever or hypothermia, organ dysfunction | 30 mg/kg × 4 doses | 36,000 | 1 | Mortality Reversal of shock Secondary infection |
| Luce JM et al., (1988) [32] | Methylprednisolone (N = 38) | Placebo (N = 37) | Patients with septic shock and ARDS | 30 mg/kg, 1800 mg/60 kg × 4 doses | 36,000 | 1 | ARDS Total mortality Hyperglycemia Secondary infection |
| VASSCSG (1987) [33] | Methylprednisolone (N = 112) | Placebo (N = 111) | Systemic sepsis patients | 30 mg/kg followed by infusion of 5 mg/kg | 22,500 | 1 | Mortality |
| Yildiz O et al., (2002) [34] | Prednisolone (N = 20) | Placebo (N = 20) | >17 years old and sepsis | 5 mg IV at 06:00 am and 2.5 mg IV at 18:00 for 10 days | 30 | 10 | LOS in hospital Secondary infection Mortality |
| Yildiz O et al., (2011) [35] | Prednisolone (N = 27) | Placebo (N = 28) | Patients >17 years and diagnosed with sepsis | 20 mg/day | 80 | 10 | Mortality |
| Outcome | Statistical Method | Studies | Participants | I2 (%) | Effect Estimate | p | |
|---|---|---|---|---|---|---|---|
| Organ failure | Organ failure | Risk Ratio (M-H, Fixed, 95% Cl) | 1 | 466 | N/A | 1.02 (0.66, 1.59) | 0.93 |
| Respiratory failure | Risk Ratio (M-H, Fixed, 96% Cl) | 5 | 1381 | 0 | 1.01 (0.89, 1.14) | 0.88 | |
| Mechanical ventilation | Mean Difference (IV, Fixed, 95% Cl) | 2 | 69 | 0 | −0.58 (−2.64, 1.47) | 0.58 | |
| Reversal of shock | Risk Ratio (M-H, Random, 95% Cl) | 2 | 362 | 0 | 0.91 (0.79, 1.05) | 0.18 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, J.-y.; Shin, S.; Choi, Y.J. New Evidence of Potential Benefits of Dexamethasone and Added on Therapy of Fludrocortisone on Clinical Outcomes of Corticosteroid in Sepsis Patients: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 544. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11060544
Son J-y, Shin S, Choi YJ. New Evidence of Potential Benefits of Dexamethasone and Added on Therapy of Fludrocortisone on Clinical Outcomes of Corticosteroid in Sepsis Patients: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(6):544. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11060544
Chicago/Turabian StyleSon, Ji-young, Sooyoung Shin, and Yeo Jin Choi. 2021. "New Evidence of Potential Benefits of Dexamethasone and Added on Therapy of Fludrocortisone on Clinical Outcomes of Corticosteroid in Sepsis Patients: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 6: 544. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11060544