
Reliability of Tumor Testing Compared to Germline Testing for Detecting BRCA1 and BRCA2 Mutations in Patients with Epithelial Ovarian Cancer

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Pathogenic BRCA Mutations
2.2. Pathogenic BRCA Mutations Including BRCA Variants of Uncertain Significance (VUS)
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Germline Testing
4.3. Tumor Testing
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stratton, J.F.; Gayther, S.A.; Russell, P.; Dearden, J.; Gore, M.; Blake, P.; Easton, D.; Ponder, B.A.J. Contribution of BRCA1Mutations to Ovarian Cancer. N. Engl. J. Med. 1997, 336, 1125–1130. [Google Scholar] [CrossRef]
- Zhang, S.; Royer, R.; Li, S.; McLaughlin, J.R.; Rosen, B.; Risch, H.A.; Fan, I.; Bradley, L.; Shaw, P.A.; Narod, S.A. Frequencies of BRCA1 and BRCA2 mutations among 1342 unselected patients with invasive ovarian cancer. Gynecol. Oncol. 2011, 121, 353–357. [Google Scholar] [CrossRef]
- A Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Overall survival in patients with platinum-sensitive recurrent serous ovarian cancer receiving olaparib maintenance monotherapy: An updated analysis from a randomised, placebo-controlled, double-blind, phase 2 trial. Lancet Oncol. 2016, 17, 1579–1589. [Google Scholar] [CrossRef]
- Weren, R.D.; Mensenkamp, A.R.; Simons, M.; Eijkelenboom, A.; Sie, A.S.; Ouchene, H.; Van Asseldonk, M.; Gomez-Garcia, E.B.; Blok, M.J.; De Hullu, J.A.; et al. NovelBRCA1andBRCA2Tumor Test as Basis for Treatment Decisions and Referral for Genetic Counselling of Patients with Ovarian Carcinomas. Hum. Mutat. 2017, 38, 226–235. [Google Scholar] [CrossRef]
- Pennington, K.P.; Walsh, T.; Harrell, M.I.; Lee, M.K.; Pennil, C.C.; Rendi, M.H.; Thornton, A.; Norquist, B.M.; Casadei, S.; Nord, A.; et al. Germline and Somatic Mutations in Homologous Recombination Genes Predict Platinum Response and Survival in Ovarian, Fallopian Tube, and Peritoneal Carcinomas. Clin. Cancer Res. 2014, 20, 764–775. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef] [PubMed]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.L.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: A preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol. 2014, 15, 852–861. [Google Scholar] [CrossRef]
- Mafficini, A.; Simbolo, M.; Parisi, A.; Rusev, B.; Luchini, C.; Cataldo, I.; Piazzola, E.; Sperandio, N.; Turri, G.; Franchi, M.; et al. BRCA somatic and germline mutation detection in paraffin embedded ovarian cancers by next-generation sequencing. Oncotarget 2016, 7, 1076–1083. [Google Scholar] [CrossRef] [Green Version]
- Hennessy, B.T.; Timms, K.M.; Carey, M.S.; Gutin, A.; Meyer, L.A.; Flake, D.D.; Abkevich, V.; Potter, J.; Pruss, D.; Glenn, P.; et al. Somatic Mutations in BRCA1 and BRCA2 Could Expand the Number of Patients that Benefit from Poly (ADP Ribose) Polymerase Inhibitors in Ovarian Cancer. J. Clin. Oncol. 2010, 28, 3570–3576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capoluongo, E.D.; Ellison, G.; López-Guerrero, J.A.; Penault-Llorca, F.; Ligtenberg, M.J.; Banerjee, S.; Singer, C.; Friedman, E.; Markiefka, B.; Schirmacher, P.; et al. Guidance Statement on BRCA1/2 Tumor Testing in Ovarian Cancer Patients. Semin. Oncol. 2017, 44, 187–197. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Norquist, B.; Lacchetti, C.; Armstrong, D.; Grisham, R.N.; Goodfellow, P.J.; Kohn, E.C.; Levine, D.A.; Liu, J.F.; Lu, K.H.; et al. Germline and Somatic Tumor Testing in Epithelial Ovarian Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 1222–1245. [Google Scholar] [CrossRef]
- Tavtigian, S.V.; Greenblatt, M.S.; Goldgar, D.E.; Boffetta, P.; The IARC Unclassified Genetic Variants Working Group. Assessing pathogenicity: Overview of results from the IARC Unclassified Genetic Variants Working Group. Hum. Mutat. 2008, 29, 1261–1264. [Google Scholar] [CrossRef]
- Kwon, J.; Tinker, A.; Karsan, A.; Schrader, K.; Sun, S. Costs and benefits of tumor testing for mutations in high-grade serous ovarian cancer as a triage for confirmatory genetic testing. Gynecol. Oncol. 2019, 154, 5. [Google Scholar] [CrossRef]
- Ellison, G.; Ahdesmäki, M.; Luke, S.; Waring, P.M.; Wallace, A.; Wright, R.; Röthlisberger, B.; Ludin, K.; Merkelbach-Bruse, S.; Heydt, C.; et al. An evaluation of the challenges to developing tumor BRCA1 and BRCA2 testing methodologies for clinical practice. Hum. Mutat. 2018, 39, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, C.; Tomao, F.; Betella, I.; Rappa, A.; Calvello, M.; Bonanni, B.; Bernard, L.; Peccatori, F.; Colombo, N.; Viale, G.; et al. Tumor BRCA Test for Patients with Epithelial Ovarian Cancer: The Role of Molecular Pathology in the Era of PARP Inhibitor Therapy. Cancers 2019, 11, 1641. [Google Scholar] [CrossRef] [Green Version]
- Care, M.; McCuaig, J.; Clarke, B.; Grenier, S.; Kim, R.H.; Rouzbahman, M.; Stickle, N.; Bernardini, M.Q.; Stockley, T.L. Tumor and germline next generation sequencing in high grade serous cancer: Experience from a large population-based testing program. Mol. Oncol. 2021, 15, 80–90. [Google Scholar] [CrossRef]
- Lindor, N.M.; Goldgar, D.E.; Tavtigian, S.V.; Plon, S.E.; Couch, F.J. BRCA1/2 Sequence Variants of Uncertain Significance: A Primer for Providers to Assist in Discussions and in Medical Management. Oncologist 2013, 18, 518–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, T.S.; Deffenbaugh, A.M.; Reid, J.E.; Hulick, M.; Ward, B.E.; Lingenfelter, B.; Gumpper, K.L.; Scholl, T.; Tavtigian, S.V.; Pruss, D.R.; et al. Clinical Characteristics of Individuals with Germline Mutations in BRCA1 and BRCA2: Analysis of 10,000 Individuals. J. Clin. Oncol. 2002, 20, 1480–1490. [Google Scholar] [CrossRef]
- Alizadeh, A.; Aranda, V.; Bardelli, A.; Blanpain, C.; Bock, C.; Borowski, C.; Caldas, C.; Califano, A.; Doherty, M.; Elsner, M.; et al. Toward understanding and exploiting tumor heterogeneity. Nat. Med. 2015, 21, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Patch, A.-M.; The Australian Ovarian Cancer Study Group; Christie, E.; Etemadmoghadam, D.; Garsed, D.W.; George, J.; Fereday, S.; Nones, K.; Cowin, P.; Alsop, K.; et al. Whole–genome characterization of chemoresistant ovarian cancer. Nature 2015, 521, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Norquist, B.; Wurz, K.A.; Pennil, C.C.; Garcia, R.; Gross, J.; Sakai, W.; Karlan, B.Y.; Taniguchi, T.; Swisher, E.M. Secondary Somatic Mutations Restoring BRCA1/2 Predict Chemotherapy Resistance in Hereditary Ovarian Carcinomas. J. Clin. Oncol. 2011, 29, 3008–3015. [Google Scholar] [CrossRef] [Green Version]
- Swisher, E.M.; Sakai, W.; Karlan, B.Y.; Wurz, K.; Urban, N.; Taniguchi, T. Secondary BRCA1 Mutations in BRCA1-Mutated Ovarian Carcinomas with Platinum Resistance. Cancer Res. 2008, 68, 2581–2586. [Google Scholar] [CrossRef] [Green Version]
- Incorvaia, L.; Fanale, D.; Bono, M.; Calò, V.; Fiorino, A.; Brando, C.; Corsini, L.R.; Cutaia, S.; Cancelliere, D.; Pivetti, A.; et al. BRCA1/2 pathogenic variants in triple-negative versus luminal-like breast cancers: Genotype–phenotype correlation in a cohort of 531 patients. Ther. Adv. Med. Oncol. 2020, 12, 1758835920975326. [Google Scholar] [CrossRef]
- Przybytkowski, E.; Davis, T.; Hosny, A.; Eismann, J.; Matulonis, U.A.; Wulf, G.M.; Nabavi, S. An immune-centric exploration of BRCA1 and BRCA2 germline mutation related breast and ovarian cancers. BMC Cancer 2020, 20, 197. [Google Scholar] [CrossRef] [PubMed]
- Safra, T.; Lai, W.C.; Borgato, L.; Nicoletto, M.O.; Berman, T.; Reich, E.; Alvear, M.; Haviv, I.; Muggia, F.M. BRCA mutations and outcome in epithelial ovarian cancer (EOC): Experience in ethnically diverse groups. Ann. Oncol. 2013, 24, viii63–viii68. [Google Scholar] [CrossRef]
- Gallardo, M.; Silva, A.; Rubio, L.; Alvarez, C.; Torrealba, C.; Salinas, M.A.; Tapia, T.; Faundez, P.; Palma, L.; Riccio, M.E.; et al. Incidence of BRCA1 and BRCA2 mutations in 54 Chilean families with breast/ovarian cancer, genotype-phenotype correlations. Breast Cancer Res. Treat. 2005, 95, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Incorvaia, L.; Fanale, D.; Badalamenti, G.; Bono, M.; Calò, V.; Cancelliere, D.; Castiglia, M.; Fiorino, A.; Pivetti, A.; Barraco, N.; et al. Hereditary Breast and Ovarian Cancer in Families from Southern Italy (Sicily)—Prevalence and Geographic Distribution of Pathogenic Variants in BRCA1/2 Genes. Cancers 2020, 12, 1158. [Google Scholar] [CrossRef]
- Karami, F.; Mehdipour, P. A Comprehensive Focus on Global Spectrum ofBRCA1andBRCA2Mutations in Breast Cancer. BioMed Res. Int. 2013, 2013, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meisel, C.; Sadowski, C.E.; Kohlstedt, D.; Keller, K.; Stäritz, F.; Grübling, N.; Becker, K.; Mackenroth, L.; Rump, A.; Schröck, E.; et al. Spectrum of genetic variants of BRCA1 and BRCA2 in a German single center study. Arch. Gynecol. Obstet. 2017, 295, 1227–1238. [Google Scholar] [CrossRef] [PubMed]
- Jorge, S.; McFaddin, A.S.; Doll, K.M.; Pennington, K.P.; Norquist, B.M.; Bennett, R.L.; Pritchard, C.C.; Swisher, E.M. Simultaneous germline and somatic sequencing in ovarian carcinoma: Mutation rate and impact on clinical decision-making. Gynecol. Oncol. 2020, 156, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Norquist, B.M.; Harrell, M.I.; Brady, M.F.; Walsh, T.; Lee, M.K.; Gulsuner, S.; Bernards, S.S.; Casadei, S.; Yi, Q.; Burger, R.A.; et al. Inherited Mutations in Women with Ovarian Carcinoma. JAMA Oncol. 2016, 2, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Singer, C.; Tea, M.; Pristauz, G.; Hubalek, M.; Rappaport, C.; Riedl, C.; Helbich, T. Clinical Practice Guideline for the prevention and early detection of breast and ovarian cancer in women from HBOC (hereditary breast and ovarian cancer) families. Wien. Klin. Wochenschr. 2015, 127, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Landrum, M.J.; Lee, J.M.; Benson, M.; Brown, G.R.; Chao, C.; Chitipiralla, S.; Gu, B.; Hart, J.; Hoffman, D.; Jang, W.; et al. ClinVar: Improving access to variant interpretations and supporting evidence. Nucleic Acids Res. 2018, 46, D1062–D1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plon, S.E.; Eccles, D.M.; Easton, D.; Foulkes, W.D.; Genuardi, M.; Greenblatt, M.S.; Hogervorst, F.B.; Hoogerbrugge, N.; Spurdle, A.B.; Tavtigian, S.V.; et al. Sequence variant classification and reporting: Recommendations for improving the interpretation of cancer susceptibility genetic test results. Hum. Mutat. 2008, 29, 1282–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| gBRCA mt (n = 47) | gBRCA VUS (n = 8) | gBRCA wt (n = 85) | p-Value | |
|---|---|---|---|---|
| Age (years), mean (SD) | 54.23 (9.67) | 56.75 (11.71) | 56.19 (13.34) | 0.650 a |
| Ethnicity | ||||
| Caucasians | 47 (100%) | 8 (100%) | 85 (100%) | |
| FIGO Stage, number (%) | 0.339 b | |||
| I | 2 (4.3%) | 1 (12.5%) | 2 (2.4%) | |
| II | 3 (6.4%) | 0 | 1 (1.2%) | |
| III | 34 (72.3%) | 6 (75.0%) | 66 (77.6%) | |
| IV | 8 (17.0%) | 1 (12.5%) | 11 (12.9%) | |
| missing | 0 | 0 | 5 (5.9%) | |
| Grade, number (%) | 0.255 b | |||
| Low-grade | 0 | 0 | 4 (4.7%) | |
| High-grade | 47 (100%) | 8 (100%) | 79 (92.9%) | |
| Missing | 0 | 0 | 2 (2.4%) | |
| Histology, number (%) | 0.064 b | |||
| Serous | 47 (100%) | 8 (100%) | 77 (90.6%) | |
| others | 0 | 0 | 8 (9.4%) | |
| Primary vs. recurrent disease for tumor testing, number (%) | 0.940 b | |||
| Primary disease | 40 (85.1%) | 7 (87.5%) | 71 (83.5%) | |
| Recurrent disease | 7 (14.9%) | 1 (12.5%) | 14 (16.5%) | |
| Family history, number (%) | <0.001 b | |||
| Positive | 16 (34.0%) | 1 (12.5%) | 3 (3.5%) | |
| Negative | 4 (8.5%) | 5 (62.5%) | 30 (35.3%) | |
| Unknown | 27 (57.4%) | 2 (25.0%) | 52 (61.2%) | |
| PFS (months), mean (SD) | 30.06 (25.86) | 30.13 (16.82) | 32.82 (28.42) | 0.843 a |
| OS (months), mean (SD) | 49.17 (44.92) | 41.25 (19.85) | 55.14 (44.82) | 0.579 a |
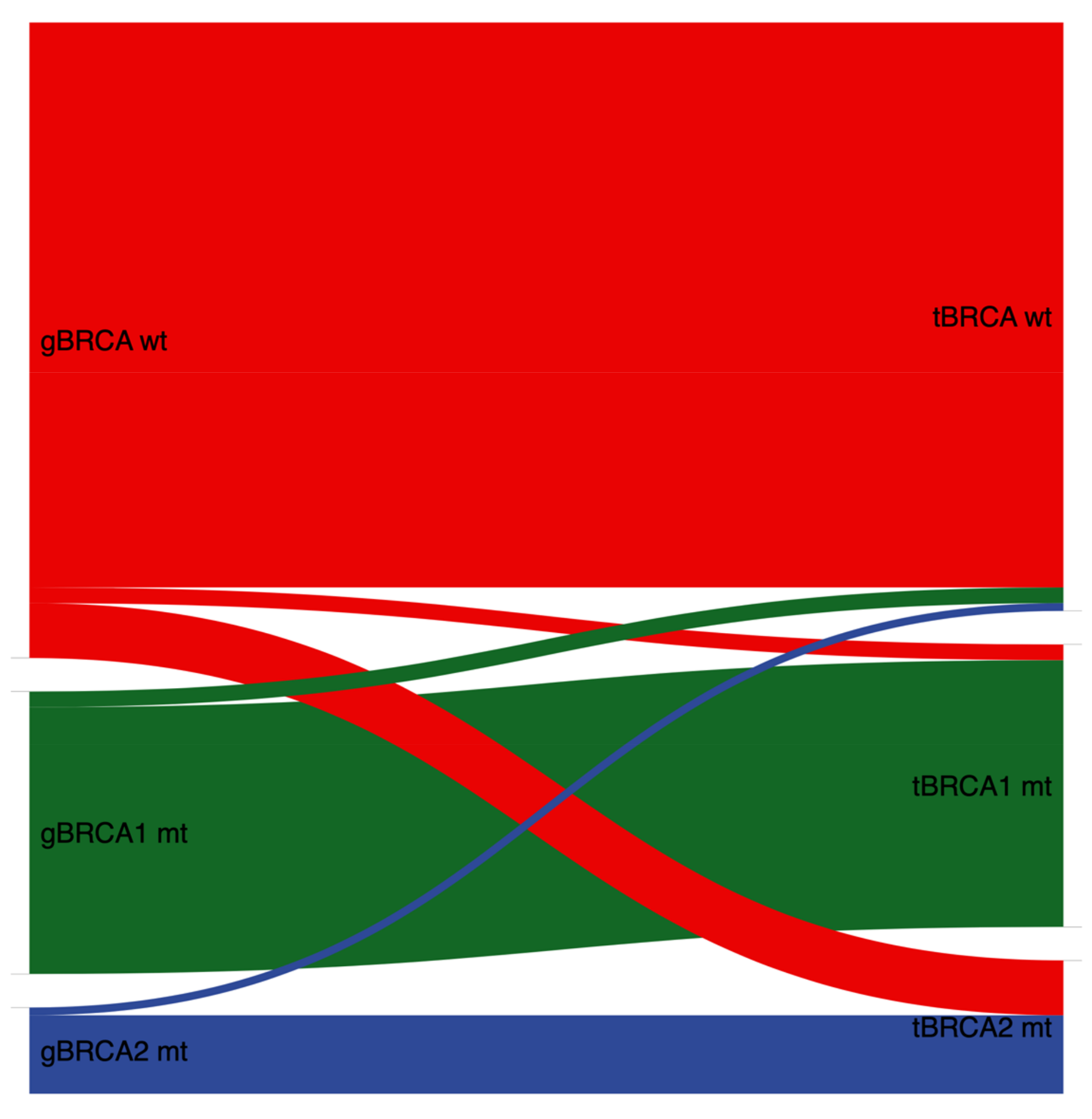
| Germline | ||||
|---|---|---|---|---|
| Wildtype (n = 81) | BRCA1 mt (n = 36) | BRCA2 mt (n = 11) | ||
| Tumor | wildtype | 72 (88.9%) | 2 (5.6%) | 1 (9.1%) |
| BRCA1 mt | 2 (2.4%) | 34 (94.4%) | 0 | |
| BRCA2 mt | 7 (8.6%) | 0 | 10 (90.9%) | |
| Germline | ||||||
|---|---|---|---|---|---|---|
| Wildtype (n = 85) | BRCA1 mt (n = 36) | BRCA1 VUS (n = 2) | BRCA2 mt (n = 11) | BRCA2 VUS (n = 6) | ||
| Tumor | wildtype | 72 (84.7%) | 2 (5.6%) | 1 (50.0%) | 1 (9.1%) | 1 (16.7%) |
| BRCA1 mt | 2 (2.4%) | 34 (94.4%) | 1 (50.0%) | 0 | 0 | |
| BRCA1 VUS | 2 (2.4%) | 0 | 0 | 0 | 0 | |
| BRCA2 mt | 7 (8.2%) | 0 | 0 | 10 (90.9%) | 3 (50.0%) | |
| BRCA2 VUS | 2 (2.4%) | 0 | 0 | 0 | 2 (33.3%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bekos, C.; Grimm, C.; Kranawetter, M.; Polterauer, S.; Oberndorfer, F.; Tan, Y.; Müllauer, L.; Singer, C.F. Reliability of Tumor Testing Compared to Germline Testing for Detecting BRCA1 and BRCA2 Mutations in Patients with Epithelial Ovarian Cancer. J. Pers. Med. 2021, 11, 593. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070593
Bekos C, Grimm C, Kranawetter M, Polterauer S, Oberndorfer F, Tan Y, Müllauer L, Singer CF. Reliability of Tumor Testing Compared to Germline Testing for Detecting BRCA1 and BRCA2 Mutations in Patients with Epithelial Ovarian Cancer. Journal of Personalized Medicine. 2021; 11(7):593. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070593
Chicago/Turabian StyleBekos, Christine, Christoph Grimm, Marlene Kranawetter, Stephan Polterauer, Felicitas Oberndorfer, Yen Tan, Leonhard Müllauer, and Christian F. Singer. 2021. "Reliability of Tumor Testing Compared to Germline Testing for Detecting BRCA1 and BRCA2 Mutations in Patients with Epithelial Ovarian Cancer" Journal of Personalized Medicine 11, no. 7: 593. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070593