
Association between CYP3A5 Polymorphism and Statin-Induced Adverse Events: A Systemic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods and Materials
2.1. Literature Search Strategy and Inclusion Criteria
2.2. Data Extraction and Study Quality Assessment
2.3. Statistical Analysis
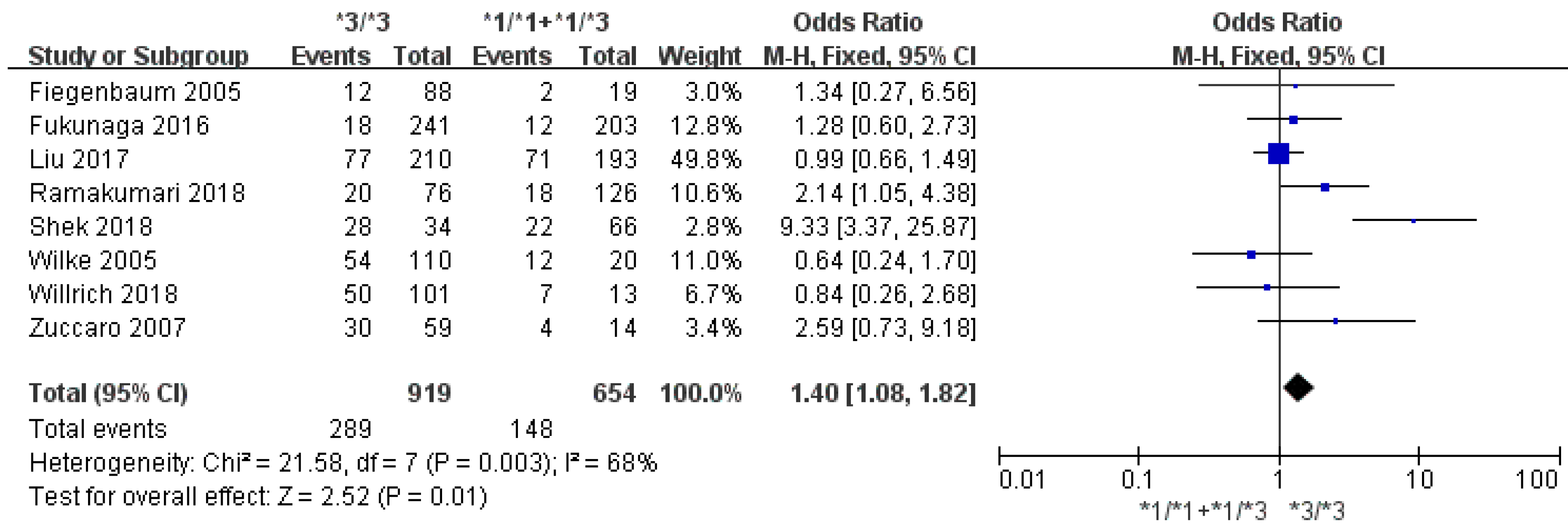
3. Results
Literature Search
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| CK | creatine kinase |
| CPIC | Clinical Pharmacogenetics Implementation Consortium |
| CYP | cytochrome P450 |
| GEOSTAT-1 | Ge-netic Effects On STATins |
| HMG-CoA | 3-hydroxy-3-methylglutaryl coenzyme A |
| NOS | Newcastle–Ottawa Scale |
| OR | odds ratio |
| PCR | polymerase chain reaction |
| RFLP | re-striction fragment length polymorphism |
| SLCO1B1 | solute carrier organic anion transporter family 1B1 |
| SNP | single-nucleotide polymorphism |
References
- Jellinger, P.S.; Smith, D.A.; Mehta, A.E.; Ganda, O.; Handelsman, Y.; Rodbard, H.W.; Shepherd, M.D.; Seibel, J.A. American Association of Clinical Endocrinologists’ Guidelines for Management of Dyslipidemia and Prevention of Atherosclerosis. Endocr. Pr. 2012, 18, 1–78. [Google Scholar] [CrossRef] [Green Version]
- Vaughan, C.J.; Gotto, A.M., Jr.; Basson, C.T. The evolving role of statins in the management of atherosclerosis. J. Am. Coll. Cardiol. 2000, 35, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, B.; Chan, P.; Lan, W. How well tolerated are lipid-lowering drugs? Drugs Aging 2001, 18, 665–683. [Google Scholar] [CrossRef] [PubMed]
- Mancini, G.B.; Baker, S.; Bergeron, J.; Fitchett, D.; Frohlich, J.; Genest, J.; Gupta, M.; Hegele, R.A.; Ng, D.; Pearson, G.J.; et al. Diagnosis, prevention, and management of statin adverse effects and intolerance: Canadian Consensus Working Group Update (2016). Can. J. Cardiol. 2016, 32, S35–S65. [Google Scholar] [CrossRef] [PubMed]
- Serban, M.-C.; Colantonio, L.; Manthripragada, A.D.; Monda, K.L.; Bittner, V.A.; Banach, M.; Chen, L.; Huang, L.; Dent, R.; Kent, S.T.; et al. Statin intolerance and risk of coronary heart events and all-cause mortality following myocardial infarction. J. Am. Coll. Cardiol. 2017, 69, 1386–1395. [Google Scholar] [CrossRef]
- Toth, P.P.; Patti, A.M.; Giglio, R.V.; Nikolic, D.; Castellino, G.; Rizzo, M.; Banach, M. Management of statin intolerance in 2018: Still more questions than answers. Am. J. Cardiovasc. Drugs 2018, 18, 157–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitchett, D.H.; Hegele, R.A.; Verma, S. Cardiology patient page. Statin intolerance. Circulation 2015, 131, e389–e391. [Google Scholar] [PubMed] [Green Version]
- Kitzmiller, J.P.; Mikulik, E.B.; Dauki, A.; Mukherjee, C.; A Luzum, J. Pharmacogenomics of statins: Understanding susceptibility to adverse effects. Pharm. Pers. Med. 2016, ume 9, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, L.A.; Doney, A.S.; Tavendale, R.; Lang, C.C.; Pearson, E.R.; Colhoun, H.M.; McCarthy, M.I.; Hattersley, A.T.; Morris, A.D.; Palmer, C.N. Common nonsynonymous substitutions in SLCO1B1 predispose to statin intolerance in routinely treated individuals with type 2 diabetes: A go-DARTS study. Clin. Pharmacol. Ther. 2011, 89, 210–216. [Google Scholar] [CrossRef] [Green Version]
- Carr, D.; O’Meara, H.; Jorgensen, A.L.; Campbell, J.; Hobbs, M.; McCann, G.; van Staa, T.; Pirmohamed, M. SLCO1B1 genetic variant associated with statin-induced myopathy: A proof-of-concept study using the clinical practice research datalink. Clin. Pharmacol. Ther. 2013, 94, 695–701. [Google Scholar] [CrossRef]
- Xiang, Q.; Chen, S.-Q.; Ma, L.-Y.; Hu, K.; Zhang, Z.; Mu, G.-Y.; Xie, Q.-F.; Zhang, X.-D.; Cui, Y.-M. Association between SLCO1B1 T521C polymorphism and risk of statin-induced myopathy: A meta-analysis. Pharm. J. 2018, 18, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, L.B.; Johnson, S.G.; E Caudle, K.; E Haidar, C.; Voora, D.; A Wilke, R.; Maxwell, W.D.; McLeod, H.L.; Krauss, R.M.; Roden, D.M.; et al. The clinical pharmacogenetics implementation consortium guideline for SLCO1B1 and simvastatin-induced myopathy: 2014 update. Clin. Pharmacol. Ther. 2014, 96, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Prueksaritanont, T.; Ma, B.; Yu, N. The human hepatic metabolism of simvastatin hydroxy acid is mediated primarily by CYP3A, and not CYP2D6. Br. J. Clin. Pharmacol. 2003, 56, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Ward, L.D.; Kellis, M. HaploReg: A resource for exploring chromatin states, conservation, and regulatory motif alterations within sets of genetically linked variants. Nucleic Acids Res. 2012, 40, D930–D934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamba, J.K.; Lin, Y.S.; Schuetz, E.G.; E Thummel, K. Genetic contribution to variable human CYP3A-mediated metabolism. Adv. Drug Deliv. Rev. 2002, 54, 1271–1294. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 6, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Aromataris, E.; Munn, Z. Joanna Briggs Institute Reviewer’s Manual. The Joanna Briggs Institute. Available online: https://reviewersmanual.joannabriggs.org (accessed on 25 June 2021).
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1099. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiegenbaum, M.; da Silveira, F.R.; Van der Sand, C.R.; Van der Sand, L.C.; Ferreira, M.E.; Pires, R.C.; Hutz, M.H. The role of common variants of ABCB1, CYP3A4, and CYP3A5 genes in lipid-lowering efficacy and safety of simvastatin treatment. Clin. Pharmacol. Ther. 2005, 78, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Fukunaga, K.; Nakagawa, H.; Ishikawa, T.; Kubo, M.; Mushiroda, T. ABCB1 polymorphism is associated with atorvastatin-induced liver injury in Japanese population. BMC Genet. 2016, 17, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.-E.; Liu, X.-Y.; Chen, S.; Zhang, Y.; Cai, L.-Y.; Yan, Z.; Lai, W.-H.; Ren, B.; Zhong, S.-L. SLCO1B1 521T > C polymorphism associated with rosuvastatin-induced myotoxicity in Chinese coronary artery disease patients: A nested case-control study. Eur. J. Clin. Pharmacol. 2017, 73, 1409–1416. [Google Scholar] [CrossRef]
- V Willrich, M.A.; Kaleta, E.J.; Bryant, S.C.; Spears, G.M.; Train, L.J.; Peterson, S.E.; Lennon, V.A.; Kopecky, S.L.; Baudhuin, L.M. Genetic variation in statin intolerance and a possible protective role for UGT1A1. Pharmacogenomics 2018, 19, 83–94. [Google Scholar] [CrossRef]
- Ramakumari, N.; Indumathi, B.; Katkam, S.K.; Kutala, V.K. Impact of pharmacogenetics on statin-induced myopathy in South-Indian subjects. Indian Heart J. 2018, 70, S120–S125. [Google Scholar] [CrossRef]
- Shek, A.B.; Kurbanov, R.D.; Alieva, R.B.; Abdullaeva, G.J.; Nagay, A.V.; Abdullaev, A.; Hoshimov, S.U.; Nizamov, U.I. Personalized rosuvastatin therapy in problem patients with partial statin intolerance. Arch. Med Sci. Atheroscler. Dis. 2018, 3, e83–e89. [Google Scholar] [CrossRef] [Green Version]
- Wilke, R.A.; Moore, J.H.; Burmester, J.K. Relative impact of CYP3A genotype and concomitant medication on the severity of atorvastatin-induced muscle damage. Pharm. Genom. 2005, 15, 415–421. [Google Scholar] [CrossRef]
- Zuccaro, P.; Mombelli, G.; Calabresi, L.; Baldassarre, D.; Palmi, I.; Sirtori, C.R. Tolerability of statins is not linked to CYP450 polymorphisms, but reduced CYP2D6 metabolism improves cholesteraemic response to simvastatin and fluvastatin. Pharmacol. Res. 2007, 55, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Kiortsis, D.N.; Filippatos, T.D.; Mikhailidis, D.P.; Elisaf, M.S.; Liberopoulos, E.N. Statin-associated adverse effects beyond muscle and liver toxicity. Atherosclerosis 2007, 195, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Golomb, B.A.; Evans, M.A. Statin adverse effects: A review of the literature and evidence for a mitochondrial mechanism. Am. J. Cardiovasc. Drugs 2008, 8, 373–418. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.M.; Pirmohamed, M. Statin-related myotoxicity: A comprehensive review of pharmacokinetic, pharmacogenomic and muscle Components. J. Clin. Med. 2019, 9, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatzizisis, Y.S.; Koskinas, K.C.; Misirli, G.; Vaklavas, C.; Hatzitolios, A.; Giannoglou, G.D. Risk factors and drug interactions predisposing to statin-induced myopathy: Implications for risk assessment, prevention and treatment. Drug Saf. 2010, 33, 171–187. [Google Scholar] [CrossRef] [PubMed]
- Dreier, J.P.; Endres, M. Statin-associated rhabdomyolysis triggered by grapefruit consumption. Neurology 2004, 62, 670. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, P.M.; Zhang, J.; Lin, Y.; Lamba, J.K.; Assem, M.; Schuetz, J.D.; Watkins, P.B.; Daly, A.; Wrighton, S.A.; Hall, S.D.; et al. Sequence diversity in CYP3A promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nat. Genet. 2001, 27, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Rojas, L.; Neumann, I.; Herrero, M.J.; Boso, V.; Reig, J.; Poveda, J.L.; Megías, J.; Bea, S.; Aliño, S.F. Effect of CYP3A5*3 on kidney transplant recipients treated with tacrolimus: A systematic review and meta-analysis of observational studies. Pharm. J. 2015, 15, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.J.; Yuan, S.H.; Fang, Y.; Sun, X.Z.; Kong, H.; Ge, W.H. The effect of CYP3A5 polymorphism on dose-adjusted cyclosporine concentration in renal transplant recipients: A meta-analysis. Pharm. J. 2010, 11, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.A.; Park, P.W.; Lee, O.J.; Kang, D.K.; Park, J.Y. Effect of polymorphic CYP3A5 genotype on the single-dose simvastatin pharmacokinetics in healthy subjects. J. Clin. Pharmacol. 2007, 47, 87–93. [Google Scholar] [CrossRef]
- Kivistö, K.T.; Niemi, M.; Schaeffeler, E.; Pitkälä, K.; Tilvis, R.; Fromm, M.F.; Schwab, M.; Eichelbaum, M.; Strandberg, T. Lipid-lowering response to statins is affected by CYP3A5 polymorphism. Pharmacogenetics 2004, 14, 523–525. [Google Scholar] [CrossRef]
- Bailey, K.M.; Romaine, S.P.; Jackson, B.M.; Farrin, A.J.; Efthymiou, M.; Barth, J.H.; Copeland, J.; McCormack, T.; Whitehead, A.; Flather, M.D.; et al. Hepatic metabolism and transporter gene variants enhance response to rosuvastatin in patients with acute myocardial infarction: The GEOSTAT-1 Study. Circ. Cardiovasc. Genet. 2010, 3, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Zanger, U.M.; Schwab, M. Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef]
- Klomp, S.D.; Manson, M.L.; Guchelaar, H.J.; Swen, J.J. Phenoconversion of cytochrome P450 metabolism: A systematic review. J. Clin. Med. 2020, 9, 2890. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.R.; Smith, R.L. Addressing phenoconversion: The Achilles’ heel of personalized medicine. Br. J. Clin. Pharmacol. 2015, 79, 222–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Design | Case/Control Number | Mean Age of Case/Control | Male % of Case/Control | Case Definition | Statins Included in the Analysis | Genotyping Method | NOS |
|---|---|---|---|---|---|---|---|---|---|
| Fiegenbaum et al. (2005) | Brazil | Prospective cohort study | 15/99 | 63.0/59.2 | 18.8/25.3 | Myopathy | Simvastatin | PCR-RFLP | 9 |
| Fukunaga et al. (2016) | Japan | Case-control study | 30/414 | 61.0/66.0 a | 60.0/53.9 | Liver injury | Atorvastatin | Invader Assay | 6 |
| Liu et al. (2017) | China | Case-control study | 148/255 | 60.6/63.3 | 82.4/82.7 | Myopathy | Atorvastatin, fluvastatin, pravastatin, rosuvastatin, simvastatin | TaqMan | 9 |
| Ramakumari et al. (2018) | India | Retrospective cohort study | 38/164 | 63.0 b | 64.9 b | Myopathy symptoms with elevated CK level | Atorvastatin, rosuvastatin | PCR | 7 |
| Shek et al. (2017) | Uzbekistan | Case-control study | 50/50 | 59.3/61.7 | 42.0/56.0 | Elevated transaminase or CK level | Simvastatin | PCR-RFLP | 6 |
| Wilke et al. (2005) | USA | Case-control study | 68/69 | 58.1/63.1 | 79.4/50.7 | Myopathy symptoms with elevated CK level | Atorvastatin | Invader Assay | 6 |
| Willrich et al. (2018) | USA | Case-control study | 57/57 | 65.5/65.7 | 56.6/56.6 | Statin intolerance | Atorvastatin, lovastatin, simvastatin | TaqMan | 9 |
| Zuccaro et al. (2007) | Italy | Retrospective cohort study | 50/50 | 61.4/61.1 | 44.0/46.0 | Myopathy | Atorvastatin, simvastatin. | PCR-RFLP | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yee, J.; Kim, H.; Heo, Y.; Yoon, H.-Y.; Song, G.; Gwak, H.-S. Association between CYP3A5 Polymorphism and Statin-Induced Adverse Events: A Systemic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 677. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070677
Yee J, Kim H, Heo Y, Yoon H-Y, Song G, Gwak H-S. Association between CYP3A5 Polymorphism and Statin-Induced Adverse Events: A Systemic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(7):677. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070677
Chicago/Turabian StyleYee, Jeong, Hamin Kim, Yunhee Heo, Ha-Young Yoon, Gonjin Song, and Hye-Sun Gwak. 2021. "Association between CYP3A5 Polymorphism and Statin-Induced Adverse Events: A Systemic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 7: 677. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11070677