The Effect of Tobacco Smoking and Smoking Cessation on Urinal miRNAs in a Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection and Proceeding
2.3. miRNA Microarray Processing and qPCR
2.4. Data Analysis and Statistics
3. Results
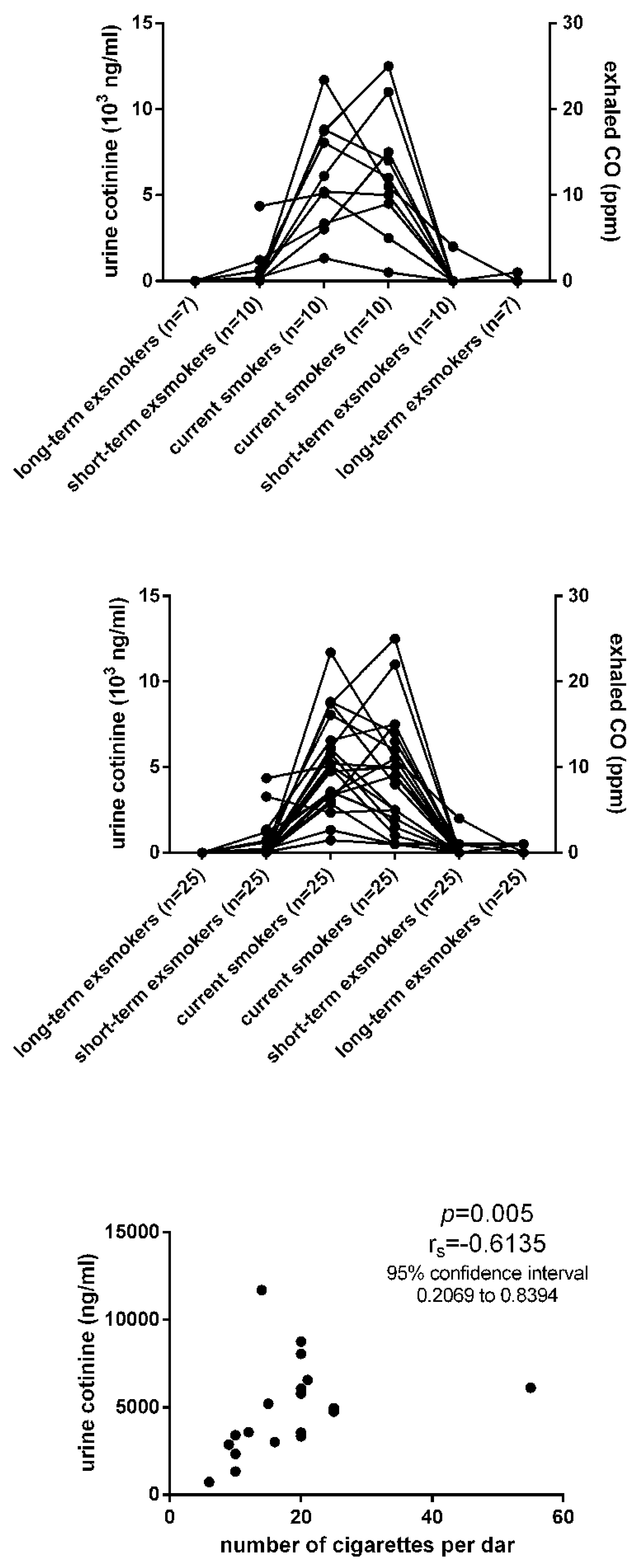
3.1. Urine Cotinine
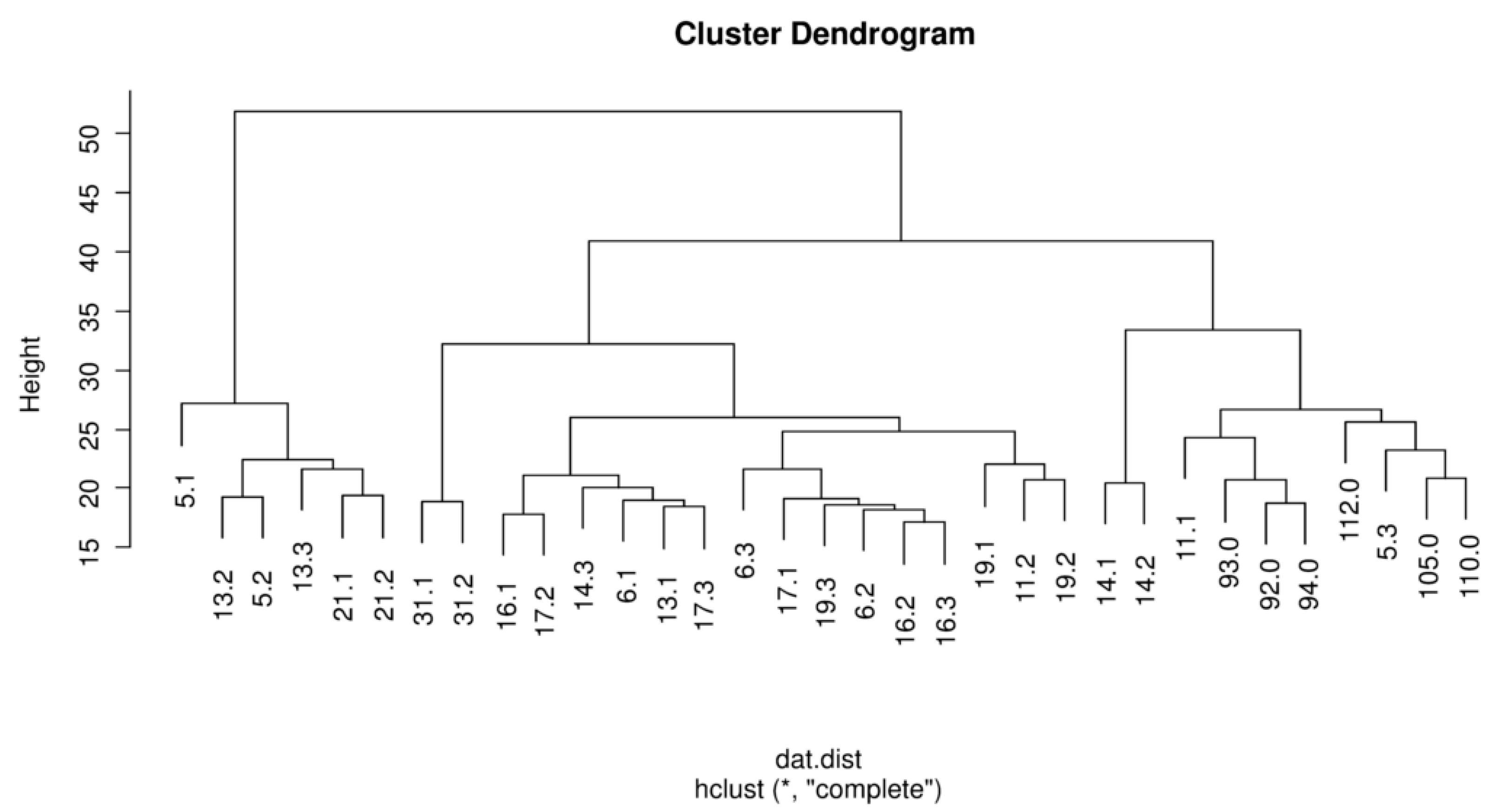
3.2. Urine miRNA Pattern
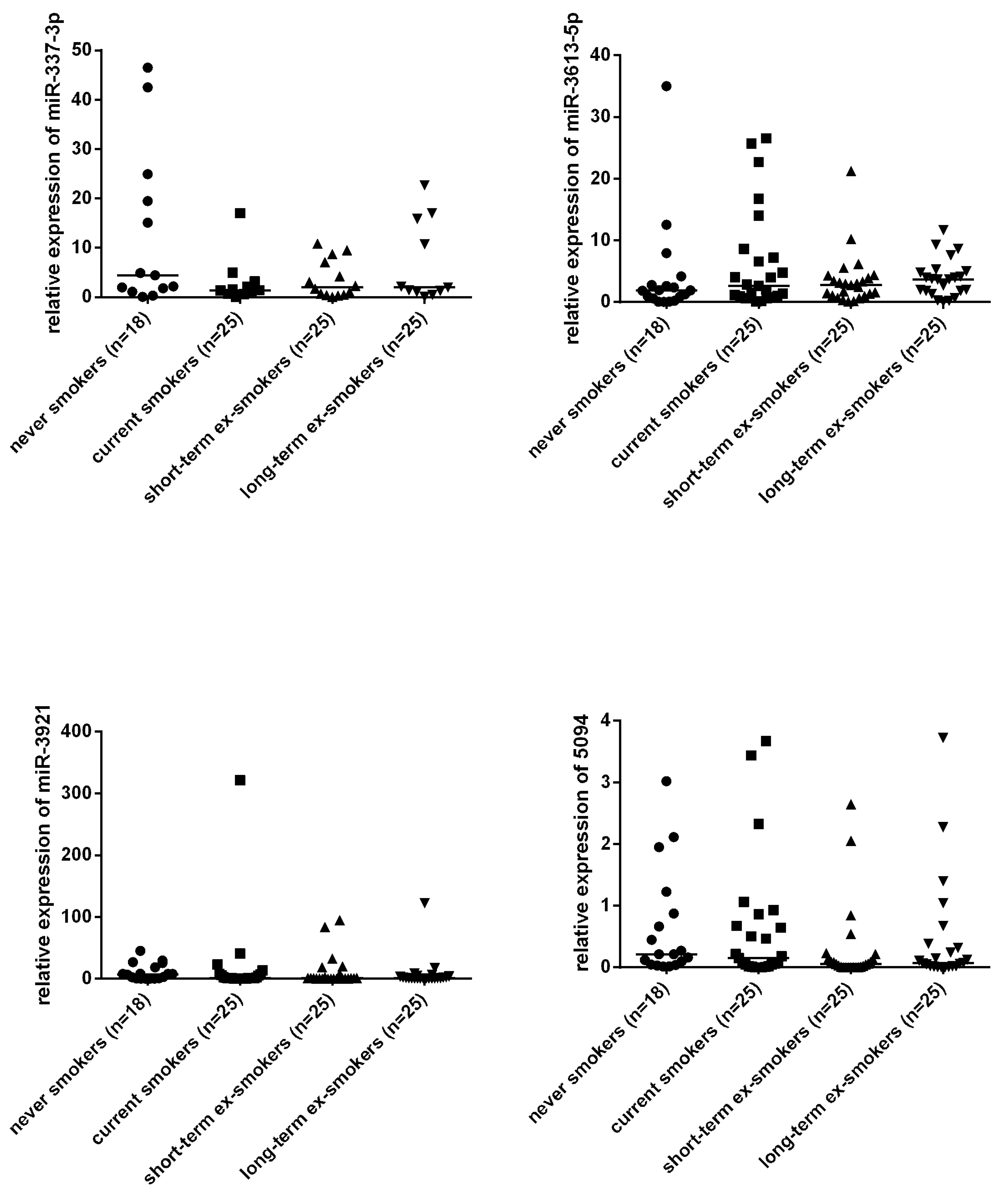
3.3. The Urine miRNA Profiles of Current/Ex-Smokers Versus Never Smokers in a Baseline Design Study
3.4. The Effect of Short-Term and Long-Term Abstinence in the Same Patient
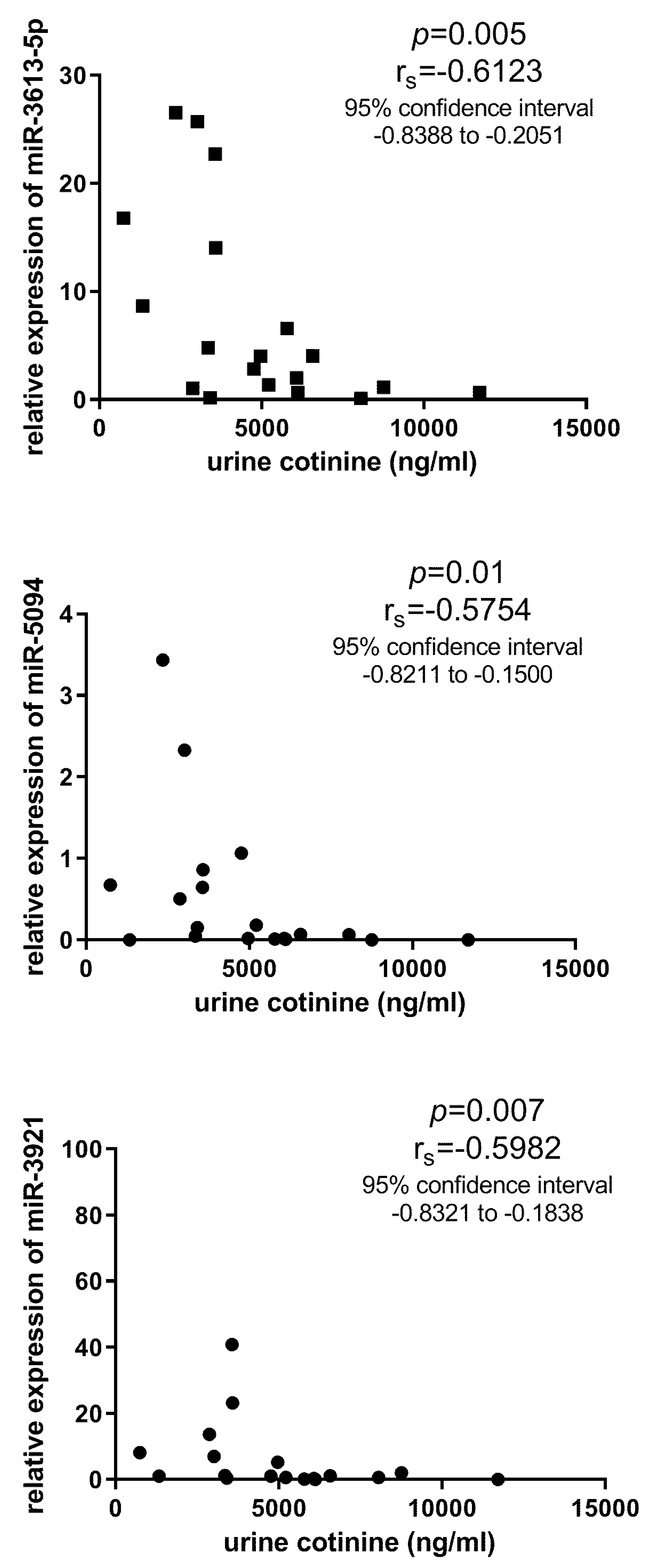
3.5. Validation with qPCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vestbo, J.; Hurd, S.S.; Agustí, A.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Cerveri, I.; Cazzoletti, L.; Corsico, A.; Marcon, A.; Niniano, R.; Grosso, A.; Ronzoni, V.; Accordini, S.; Janson, C.; Pin, I.; et al. The impact of cigarette smoking on asthma: A population-based international cohort study. Int. Arch. Allergy Immunol. 2012, 158, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Tonini, G.; D’Onofrio, L.; Dell’Aquila, E.; Pezzuto, A. New molecular insights in tobacco-induced lung cancer. Future Oncol. 2013, 9, 649–655. [Google Scholar] [CrossRef]
- Lee, P.N.; Forey, B.A.; Coombs, K.J. Systematic review with meta-analysis of the epidemiological evidence in the 1900s relating smoking to lung cancer. BMC Cancer 2012, 12, 385. [Google Scholar] [CrossRef] [Green Version]
- Cumberbatch, M.G.K.; Jubber, I.; Black, P.C.; Esperto, F.; Figueroa, J.D.; Kamat, A.M.; Kiemeney, L.; Lotan, Y.; Pang, K.; Silverman, D.T.; et al. Epidemiology of Bladder Cancer: A Systematic Review and Contemporary Update of Risk Factors in 2018. Eur. Urol. 2018, 74, 784–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Schlesinger, S.; Norat, T.; Riboli, E. Tobacco smoking and the risk of sudden cardiac death: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2018, 33, 509–521. [Google Scholar] [CrossRef] [Green Version]
- Momi, N.; Kaur, S.; Rachagani, S.; Ganti, A.K.; Batra, S.K.; Rachgani, S. Smoking and microRNA dysregulation: A cancerous combination. Trends Mol. Med. 2014, 20, 36–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, T.; Shimada, K.; Nakai, T.; Ohbayashi, C. MicroRNAs in Smoking-Related Carcinogenesis: Biomarkers, Functions, and Therapy. J. Clin. Med. 2018, 7, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroynowska-Czerwinska, A.; Fiszer, A.; Krzyzosiak, W.J. The panorama of miRNA-mediated mechanisms in mammalian cells. Cell. Mol. Life Sci. 2014, 71, 2253–2270. [Google Scholar] [CrossRef] [PubMed]
- Makarova, J.; Shkurnikov, M.; Wicklein, D.; Lange, T.; Samatov, T.R.; Turchinovich, A.A.; Tonevitsky, A. Intracellular and extracellular microRNA: An update on localization and biological role. Prog. Histochem. Cytochem. 2016, 51, 33–49. [Google Scholar] [CrossRef] [PubMed]
- Ezzie, M.E.; Crawford, M.; Cho, J.H.; Orellana, R.; Zhang, S.; Gelinas, R.; Batte, K.; Yu, L.; Nuovo, G.; Galas, D.; et al. Gene expression networks in COPD: MicroRNA and mRNA regulation. Thorax 2011, 67, 122–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, W.A.; Tsai, M.J.; Jian, S.F.; Sheu, C.C.; Kuo, P.L. Systematic analysis of transcriptomic profiles of COPD airway epithelium using next-generation sequencing and bioinformatics. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 2387–2398. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Nunez, R.T.; Rupani, H.; Platé, M.; Niranjan, M.; Chambers, R.C.; Howarth, P.H.; Sanchez-Elsner, T. Genome-Wide Posttranscriptional Dysregulation by MicroRNAs in Human Asthma as Revealed by Frac-seq. J. Immunol. 2018, 201, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo-Muñoz, J.M.; Rial, J.M.; Sastre, B.; Cañas, J.A.; Mahillo-Fernandez, I.; Quirce, S.; Sastre, J.; Cosio, B.G.; Del Pozo, V. Circulating miRNAs as diagnostic tool for discrimination of respiratory disease: Asthma, asthma-chronic obstructive pulmonary disease (COPD) overlap and COPD. Allergy 2019, 74, 2491–2494. [Google Scholar] [CrossRef] [PubMed]
- Ranade, A.R.; Cherba, D.; Sridhar, S.; Richardson, P.; Webb, C.; Paripati, A.; Bowles, B.; Weiss, G.J. MicroRNA 92a-2*: A Biomarker Predictive for Chemoresistance and Prognostic for Survival in Patients with Small Cell Lung Cancer. J. Thorac. Oncol. 2010, 5, 1273–1278. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Todd, N.W.; Liu, Z.; Zhan, M.; Fang, H.; Peng, H.; Alattar, M.; Deepak, J.; Stass, S.A.; Jiang, F. Altered miRNA expression in sputum for diagnosis of non-small cell lung cancer. Lung Cancer 2010, 67, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.G.; Chang, T.H.; Liu, Y.N.; Shih, J.Y. MicroRNA in Lung Cancer Metastasis. Cancers 2019, 11, 265. [Google Scholar] [CrossRef] [Green Version]
- Vu, T.; Yang, S.; Datta, P.K. MiR-216b/Smad3/BCL-2 Axis Is Involved in Smoking-Mediated Drug Resistance in Non-Small Cell Lung Cancer. Cancers 2020, 12, 1879. [Google Scholar] [CrossRef]
- Orth, S.R.; Hallan, S.I. Smoking: A Risk Factor for Progression of Chronic Kidney Disease and for Cardiovascular Morbidity and Mortality in Renal Patients—Absence of Evidence or Evidence of Absence? Clin. J. Am. Soc. Nephrol. 2007, 3, 226–236. [Google Scholar] [CrossRef] [Green Version]
- Nandakumar, P.; Tin, A.; Grove, M.L.; Ma, J.; Boerwinkle, E.; Coresh, J.; Chakravarti, A. MicroRNAs in the miR-17 and miR-15 families are downregulated in chronic kidney disease with hypertension. PLoS ONE 2017, 12, e0176734. [Google Scholar] [CrossRef] [Green Version]
- Lv, L.L.; Cao, Y.H.; Ni, H.F.; Xu, M.; Liu, D.; Liu, H.; Chen, P.S.; Liu, B.C. MicroRNA-29c in urinary exosome/microvesicle as a biomarker of renal fibrosis. Am. J. Physiol. Physiol. 2013, 305, F1220–F1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conserva, F.; Barozzino, M.; Pesce, F.; Divella, C.; Oranger, A.; Papale, M.; Sallustio, F.; Simone, S.; Laviola, L.; Giorgino, F.; et al. Urinary miRNA-27b-3p and miRNA-1228-3p correlate with the progression of Kidney Fibrosis in Diabetic Nephropathy. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Urquidi, V.; Netherton, M.; Gomes-Giacoia, E.; Serie, D.J.; Eckel-Passow, J.; Rosser, C.J.; Goodison, S. A microRNA biomarker panel for the non-invasive detection of bladder cancer. Oncotarget 2016, 7, 86290–86299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudziec, E.; Miah, S.; Choudhry, H.; Owen, H.C.; Blizard, S.; Glover, M.; Hamdy, F.C.; Catto, J. Hypermethylation of CpG Islands and Shores around Specific MicroRNAs and Mirtrons Is Associated with the Phenotype and Presence of Bladder Cancer. Clin. Cancer Res. 2010, 17, 1287–1296. [Google Scholar] [CrossRef] [Green Version]
- Tölle, A.; Jung, M.; Rabenhorst, S.; Kilic, E.; Jung, K.; Weikert, S. Identification of microRNAs in blood and urine as tumour markers for the detection of urinary bladder cancer. Oncol. Rep. 2013, 30, 1949–1956. [Google Scholar] [CrossRef]
- Snowdon, J.; Boag, S.; Feilotter, H.; Izard, J.; Siemens, D.R. A pilot study of urinary microRNA as a biomarker for urothelial cancer. Can. Urol. Assoc. J. 2013, 7, 28–32. [Google Scholar] [CrossRef]
- Hanke, M.; Hoefig, K.; Merz, H.; Feller, A.C.; Kausch, I.; Jocham, D.; Warnecke, J.M.; Sczakiel, G. A robust methodology to study urine microRNA as tumor marker: MicroRNA-126 and microRNA-182 are related to urinary bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2010, 28, 655–661. [Google Scholar] [CrossRef]
- Tsivian, M.; Moreira, D.M.; Caso, J.R.; Mouraviev, V.; Polascik, T.J. Cigarette smoking is associated with advanced renal cell carcinoma. J. Clin. Oncol. 2011, 29, 2027–2031. [Google Scholar] [CrossRef]
- Du, L.; Jiang, X.; Duan, W.; Wang, R.; Wang, L.; Zheng, G.; Yan, K.; Wang, L.; Li, J.; Zhang, X.; et al. Cell-free microRNA expression signatures in urine serve as novel noninvasive biomarkers for diagnosis and recurrence prediction of bladder cancer. Oncotarget 2017, 8, 40832–40842. [Google Scholar] [CrossRef]
- Pospisilova, S.; Pazourková, E.; Horinek, A.; Brisuda, A.; Svobodová, I.; Soukup, V.; Hrbacek, J.; Čapoun, O.; Hanuš, T.; Mares, J.; et al. MicroRNAs in urine supernatant as potential non-invasive markers for bladder cancer detection. Neoplasma 2016, 63, 799–808. [Google Scholar] [CrossRef] [Green Version]
- Fedorko, M.; Juracek, J.; Stanik, M.; Svoboda, M.; Poprach, A.; Buchler, T.; Pacik, D.; Dolezel, J.; Slaby, O. Detection of let-7 miRNAs in urine supernatant as potential diagnostic approach in non-metastatic clear-cell renal cell carcinoma. Biochem. Med. 2017, 27, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pezzuto, A.; Carico, E. Effectiveness of smoking cessation in smokers with COPD and nocturnal oxygen desaturation: Functional analysis. Clin. Respir. J. 2019, 14, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, B.D.S.; Irizarry, R.A. A framework for oligonucleotide microarray preprocessing. Bioinformatics 2010, 26, 2363–2367. [Google Scholar] [CrossRef] [PubMed]
- Team, R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 10 September 2020).
- Smyth, G.K. LIMMA: Linear Models for Microarray Data. In Bioinformatics and Computational Biology Solutions using R and Bioconductor; Gentleman, R., Carey, V.J., Huber, W., Irizarry, R.A., Dudoit, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2005; pp. 397–420. [Google Scholar]
- Schembri, F.; Sridhar, S.; Perdomo, C.; Gustafson, A.M.; Zhang, X.; Ergun, A.; Lu, J.; Liu, G.; Bowers, J.; Vaziri, C.; et al. MicroRNAs as modulators of smoking-induced gene expression changes in human airway epithelium. Proc. Natl. Acad. Sci. USA 2009, 106, 2319–2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, M.W.; Yu, S.L.; Lin, W.C.; Tsai, C.H.; Chen, P.H.; Lee, Y.L. Smoking-related microRNAs and mRNAs in human peripheral blood mononuclear cells. Toxicol. Appl. Pharmacol. 2016, 305, 169–175. [Google Scholar] [CrossRef]
- Suzuki, K.; Yamada, H.; Nagura, A.; Ohashi, K.; Ishikawa, H.; Yamazaki, M.; Ando, Y.; Ichino, N.; Osakabe, K.; Sugimoto, K.; et al. Association of cigarette smoking with serum microRNA expression among middle-aged Japanese adults. Fujita Med. J. 2016, 2, 1–5. [Google Scholar]
- Wang, G.; Wang, R.; Strulovici-Barel, Y.; Salit, J.; Staudt, M.R.; Ahmed, J.; Tilley, A.E.; Yee-Levin, J.; Hollmann, C.; Harvey, B.G.; et al. Persistence of Smoking-Induced Dysregulation of MiRNA Expression in the Small Airway Epithelium Despite Smoking Cessation. PLoS ONE 2015, 10, e0120824. [Google Scholar] [CrossRef]
- Willinger, C.M.; Rong, J.; Tanriverdi, K.; Courchesne, P.L.; Huan, T.; Wasserman, G.A.; Lin, H.; Dupuis, J.; Joehanes, R.; Jones, M.R.; et al. MicroRNA Signature of Cigarette Smoking and Evidence for a Putative Causal Role of MicroRNAs in Smoking-Related Inflammation and Target Organ Damage. Circ. Cardiovasc. Genet. 2017, 10, e001678. [Google Scholar] [CrossRef]
- Izzotti, A.; Longobardi, M.; La Maestra, S.; Micale, R.T.; Pulliero, A.; Camoirano, A.; Geretto, M.; D’Agostini, F.; Balansky, R.; Miller, M.S.; et al. Release of MicroRNAs into Body Fluids from Ten Organs of Mice Exposed to Cigarette Smoke. Theranostics 2018, 8, 2147–2160. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, Q.; Zhang, M.; Su, W.; Wang, Z.; Li, Y.; Zhang, J.; Beer, D.G.; Yang, S.; Chen, G. Serum microRNA Signature is Capable of Early Diagnosis for Non-Small Cell Lung Cancer. Int. J. Biol. Sci. 2019, 15, 1712–1722. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Huang, Q.; Cheng, S.; Wu, S.; Sang, H.; Hou, J. Circ_ZNF124 promotes non-small cell lung cancer progression by abolishing miR-337-3p mediated downregulation of JAK2/STAT3 signaling pathway. Cancer Cell Int. 2019, 19, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, L.; Subauste, M.C.; DeSevo, C.; Zhao, Z.; Baker, M.; Borkowski, R.; Schageman, J.J.; Greer, R.; Yang, C.R.; Suraokar, M.; et al. miR-337-3p and Its Targets STAT3 and RAP1A Modulate Taxane Sensitivity in Non-Small Cell Lung Cancers. PLoS ONE 2012, 7, e39167. [Google Scholar] [CrossRef] [PubMed]
- Bradicich, M.; Schuurmans, M.M. Smoking status and second-hand smoke biomarkers in COPD, asthma and healthy controls. ERJ Open Res. 2020, 6, 00192–02019. [Google Scholar] [CrossRef]
- Rounge, T.B.; Umu, S.U.; Keller, A.; Meese, E.; Ursin, G.; Tretli, S.; Lyle, R.; Langseth, H. Circulating small non-coding RNAs associated with age, sex, smoking, body mass and physical activity. Sci. Rep. 2018, 8, 17650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, J.; Woldhuis, R.R.; Boudewijn, I.M.; Berg, A.V.D.; Kluiver, J.; Kok, K.; Terpstra, M.M.; Guryev, V.; de Vries, M.; Vermeulen, C.J.; et al. Age-related gene and miRNA expression changes in airways of healthy individuals. Sci. Rep. 2019, 9, 3765. [Google Scholar] [CrossRef] [Green Version]
- Hooten, N.N.; Abdelmohsen, K.; Gorospe, M.; Ejiogu, N.; Zonderman, A.B.; Evans, M.K. microRNA Expression Patterns Reveal Differential Expression of Target Genes with Age. PLoS ONE 2010, 5, e10724. [Google Scholar] [CrossRef] [Green Version]
- Turco, A.E.; Lam, W.; Rule, A.D.; Denic, A.; Lieske, J.C.; Miller, V.M.; Larson, J.J.; Kremers, W.K.; Jayachandran, M. Specific renal parenchymal-derived urinary extracellular vesicles identify age-associated structural changes in living donor kidneys. J. Extracell. Vesicles 2016, 5, 57. [Google Scholar] [CrossRef]
- Ranghino, A.; DiMuccio, V.; Papadimitriou, E.; Bussolati, B. Extracellular vesicles in the urine: Markers and mediators of tissue damage and regeneration. Clin. Kidney J. 2014, 8, 23–30. [Google Scholar] [CrossRef]
- Fang, D.Y.; King, H.W.; Li, J.Y.; Gleadle, J. Exosomes and the kidney: Blaming the messenger. Nephrology 2012, 18, 1–10. [Google Scholar] [CrossRef]
- Pezzuto, A.; Stumbo, L.; Russano, M.; Crucitti, P.; Scarlata, S.; Caricato, M.; Tonini, G. “Impact of Smoking Cessation Treatment” on Lung Function and Response Rate in EGFR Mutated Patients: A Short-Term Cohort Study. Recent Pat. Anticancer Drug Discov. 2015, 10, 342–351. [Google Scholar] [CrossRef]
- Pezzuto, A.; D’Ascanio, M.; Grieco, A.; Ricci, A. Functional benefit of smoking cessation in severe COPD patients undergoing bronchial valve implantation. Eur. J. Intern. Med. 2019, 68, 55–59. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analysed Group (Total Number of Samples, n) | Age (Years) Mean (Min.-Max.) | Sex (F:M) | Pack-Year Mean * (Min.-Max.) | Urine Cotinine (ng/mL) Mean (SD, Min.-Max.) | Exhaled CO (ppm) Mean (SD, Min.-Max.) | Urine Creatinine (mmol/l) (SD, Min.-Max.] |
| Never smokers (6) | 54 (39–83) | 3:3 | 0 | <10 | 0 | 10.81 (4.88, 2.34–15.66) |
| Current smokers (10) | 48 (27–73) | 2:8 | 29 (7–83) | 6140 (3184, 1325–11,712) | 12.4 (7.183, 1.000–25.000) | 12.86 (7.50, 2.69–29.89) |
| Short-term successful ex-smokers (10) | 48 (27–73) | 2:8 | 29 (7–83) | 684 (1346, 10–4359) | 0.400 (1.265, 0.000–4.000) | 11.96 (7.99, 2.22–25.53) |
| Long-term successful ex-smokers (7) | 46 (27–67) | 2:5 | 33 (7–83) | 20 (16, 10–54) | 0.286 (0.488, 0.000–1.000) | 12.88 (5.11, 3.48–18.65) |
| Analysed Group (Total Number of Samples, n) | Age (Years) Mean (Min.-Max.) | Sex (F:M) | Pack-Year * Mean (Min.-Max.) | Urine Cotinine (ng/mL) Mean (SD, Min.-Max.) | Exhaled CO (ppm) Mean (SD, Min.-Max.) | Urine Creatinine (mmol/l) (SD, Min.-Max.) |
| Never smokers (18) | 50 (38–83) | 9:9 | 0 | <10 | 0 | 10.81 (4.88, 2.34–15.66) |
| Current smokers (25) | 47 (25–69) | 10:15 | 35 (5–170) | 4851 (2689, 736–11,712) | 8.857 (6.139, 1.000–25.000) | 10.71 (7.95, 2.05–29.89) |
| Short-term successful ex-smokers (25) | 47 (25–69) | 10:15 | 35 (5–170) | 546 (875, 12–3285) | 0.286 (0.810, 0.000–4.000) | 9.69 (5.74, 2.22–22.54) |
| Long-term successful ex-smokers (25) | 47 (25–69) | 10:15 | 35 (5–170) | 24 (15, 14–54) | 0.107 (0.315, 0.000–1.000) | 12.87 (4.36, 3.48– 8.65) |
| Vs. Never Smokers | Mature miRNA | logFC | p Value | adj. P. Val |
|---|---|---|---|---|
| current smokers | hsa-miR-3613-5p | −4.86 | 3.30e-10 | 8.51e-07 |
| hsa-miR-3921 | −4.14 | 5.43e-07 | 6.99e-04 | |
| hsa-miR-5094 | −1.09 | 1.12e-06 | 9.65e-04 | |
| hsa-miR-337-3p | −2.38 | 2.84e-06 | 1.83e-03 | |
| hsa-miR-3620-5p | 1.64 | 7.19e-05 | 3.71e-02 | |
| short-term ex-smokers | hsa-miR-3613-5p | −5.77 | 5.58e-12 | 1.44e-08 |
| hsa-miR-337-3p | −2.70 | 3.11e-07 | 3.04e-04 | |
| hsa-miR-3921 | −4.24 | 3.54e-07 | 3.04e-04 | |
| hsa-miR-5094 | −1.13 | 6.26e-07 | 4.04e-04 | |
| hsa-miR-7159-5p | −0.44 | 1.37e-05 | 7.05e-03 | |
| hsa-miR-1298-3p | −1.70 | 6.77e-05 | 2.91e-02 | |
| hsa-miR-5004-5p | −0.55 | 1.37e-04 | 0.05 | |
| hsa-miR-6501-3p | −0.40 | 1.64e-04 | 0.05 | |
| hsa-miR-3620-5p | 1.51 | 2.05e-04 | 0.06 | |
| long-term ex-smokers | hsa-miR-3613-5p | −5.33 | 2.23e-10 | 5.75e-07 |
| hsa-miR-5094 | −0.90 | 6.45e-05 | 0.08 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navratilova, Z.; Losse, S.; Petrova, P.; Sikorova, K.; Chabronova, A.; Petrek, M. The Effect of Tobacco Smoking and Smoking Cessation on Urinal miRNAs in a Pilot Study. Life 2020, 10, 191. https://0-doi-org.brum.beds.ac.uk/10.3390/life10090191
Navratilova Z, Losse S, Petrova P, Sikorova K, Chabronova A, Petrek M. The Effect of Tobacco Smoking and Smoking Cessation on Urinal miRNAs in a Pilot Study. Life. 2020; 10(9):191. https://0-doi-org.brum.beds.ac.uk/10.3390/life10090191
Chicago/Turabian StyleNavratilova, Zdenka, Stanislav Losse, Pavla Petrova, Katerina Sikorova, Alzbeta Chabronova, and Martin Petrek. 2020. "The Effect of Tobacco Smoking and Smoking Cessation on Urinal miRNAs in a Pilot Study" Life 10, no. 9: 191. https://0-doi-org.brum.beds.ac.uk/10.3390/life10090191