Some Special Aspects of Liver Repair after Resection and Administration of Multipotent Stromal Cells in Experiment

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Preparation, Cultivation, and Characteristics of MMSCs
2.2. Liver Resection and Introduction of MMSCs
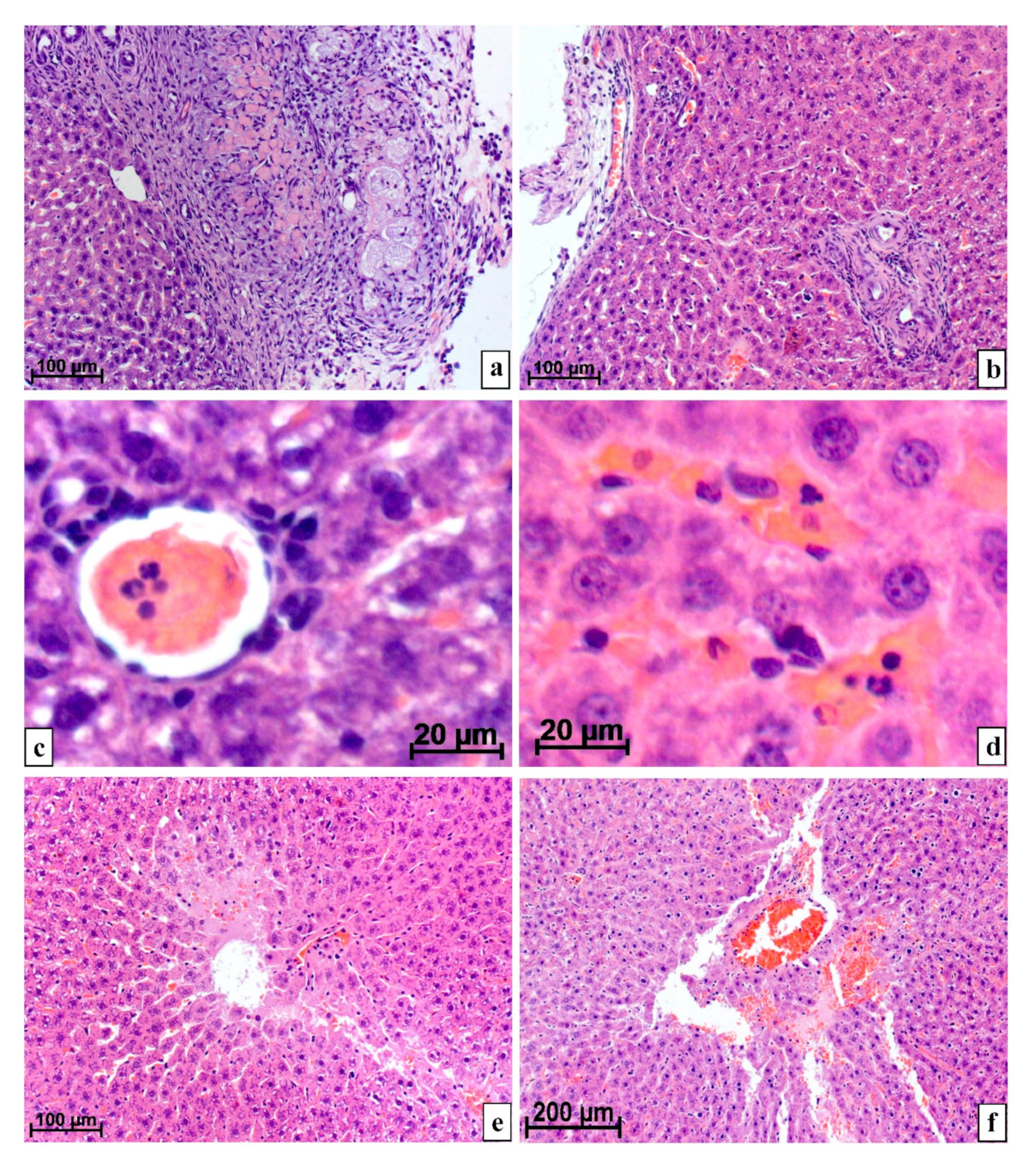
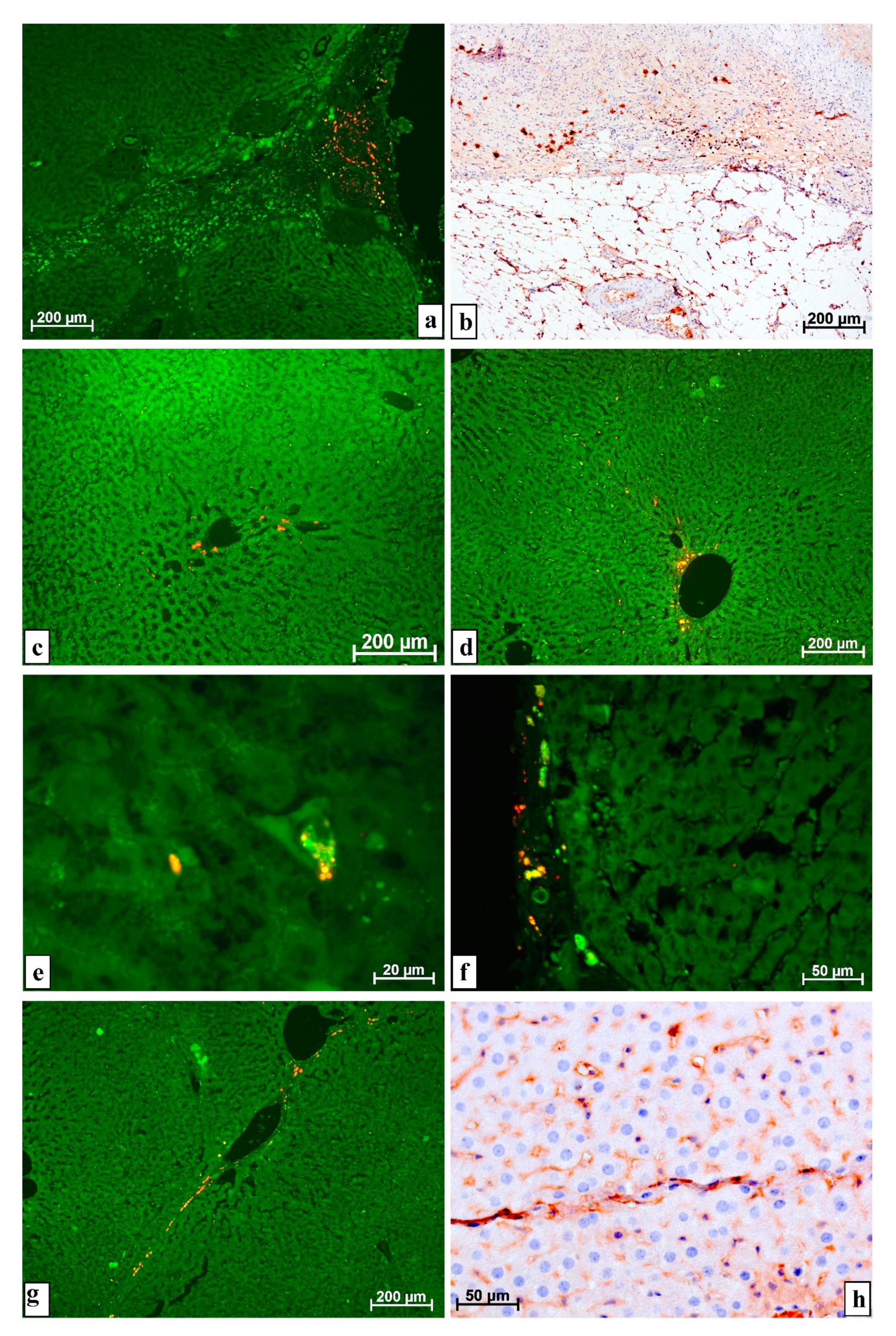
2.3. Morphological Research Methods
3. Research Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klink, T.; Simon, P.; Knopp, C.; Ittrich, H.; Fischer, L.; Adam, G.; Koops, A. Liver remnant regeneration in donors after living donor liver transplantation: Long-term follow-up using CT and MR imaging. RoFo 2014, 186, 598–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, K.H.; Kim, Y.W.; Kim, S.I.; Kim, K.S.; Lee, W.J.; Choi, J.S. Postoperative liver regeneration and complication in live liver donor after partial hepatectomy for living donor liver transplantation. Yonsei Med. J. 2003, 44, 1069–1077. [Google Scholar] [CrossRef]
- Jung, K.; Kim, Y.; Heo, Y.; Lee, J.C.; Youn, S.; Moon, J.; Kim, J.; Kim, T.Y.; Kim, B.; Wang, H. Management of severe blunt liver injuries by applying the damage control strategies with packing-oriented surgery: Experiences at a single institution in Korea. Hepatogastroenterology 2015, 62, 410–416. [Google Scholar] [PubMed]
- Uribe, C.H.M.; López, C.A.; Cote, J.C.; Franco, S.T.; Saldarriaga, M.F.; Mosquera, J.; Lanau, M.I.V. Tratamiento del traumatismo cerrado de higado; indicaciones de cirugia y desenlaces. Cir. Esp. 2014, 92, 23–29. [Google Scholar] [CrossRef]
- Beard, R.E.; Wang, Y.; Khan, S.; Marsh, J.W.; Tsung, A.; Geller, D.A. Laparoscopic liver resection for hepatocellular carcinoma in early and advanced cirrhosis. HPB 2018, 20, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Noda, T.; Eguchi, H.; Iwagami, Y.; Yamada, D.; Asaoka, T.; Gotoh, K.; Kawamoto, K.; Kobayashi, S.; Hashimoto, Y.; Takeda, Y.; et al. Minimally invasive liver resection for hepatocellular carcinoma of patients with liver damage B: A propensity score-based analysis. Hepatol. Res. 2018, 48, 539–548. [Google Scholar] [CrossRef]
- Machairas, N.; Prodromidou, A.; Molmenti, E.; Kostakis, I.D.; Sotiropoulos, G.C. Management of liver metastases from gastrointestinal stromal tumors: Where do we stand? J. Gastrointest. Oncol. 2017, 8, 1100–1108. [Google Scholar] [CrossRef] [Green Version]
- Holka, P.S.; Eriksson, S.; Eberhard, J.; Bergenfeldt, M.; Lindell, G.; Sturesson, C. Significance of poor performance status after resection of colorectal liver metastases. World J. Surg. Oncol. 2018, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, D.H.; Hwang, S.; Hong, S.M.; Kim, K.H.; Ahn, C.S.; Moon, D.B.; Alshahrani, A.A.; Lee, S.G. Clinico-pathological correlation of hepatic angiomyolipoma: A series of 23 resection cases. ANZ J. Surg. 2018, 88, E60–E65. [Google Scholar] [CrossRef]
- Klompenhouwer, A.J.; Bröker, M.E.E.; Thomeer, M.G.J.; Gaspersz, M.P.; de Man, R.A.; IJzermans, J.N.M. Retrospective study on timing of resection of hepatocellular adenoma. Br. J. Surg. 2017, 104, 1695–1703. [Google Scholar] [CrossRef]
- Oz, G.; Eroglu, M.; Gunay, E.; Bal, A.; Kacar, E.; Eser, O.; Solak, O. Aggressive hydatid cysts: Characteristics of six cases. Surg. Today 2015, 45, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Patkowski, W.; Krasnodębski, M.; Grąt, M.; Masior, Ł.; Krawczyk, M. Surgical treatment of hepatic Echinococcus granulosus. Prz Gastroenterol. 2017, 12, 199–202. [Google Scholar] [CrossRef] [Green Version]
- Du, L.; Zhang, L.Q.; Hou, L.Z.; Ren, L.; Wang, H.J.; Guo, X.J.; Fan, H. Combined resection of the right liver lobe and retrohepatic inferior vena cava to treat hepatic alveolar echinococcosis: A case report. Medicine 2017, 96, e8097. [Google Scholar] [CrossRef]
- Patkowski, W.; Kotulski, M.; Remiszewski, P.; Grąt, M.; Zieniewicz, K.; Kobryń, K.; Najnigier, B.; Ziarkiewicz-Wróblewska, B.; Krawczyk, M. Alveococcosis of the liver-strategy of surgical treatment with special focus on liver transplantation. Transpl. Infect. Dis. 2016, 18, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Kholodenko, I.V.; Yarygin, K.N. Cellular mechanisms of liver regeneration and cell-based therapies of liver diseases. Biomed. Res. Int. 2017, 2017, 8910821. [Google Scholar] [CrossRef] [PubMed]
- Tuo, L.; Zeng, W.Z.; Xue, H.L.; Wu, X.L. Umbilical cord mesenchymal stem cells and their association with liver fibrosis. Zhonghua Gan Zang Bing Za Zhi. 2017, 25, 65–68. [Google Scholar] [CrossRef]
- Haga, H.; Yan, I.K.; Borrelli, D.A.; Matsuda, A.; Parasramka, M.; Shukla, N.; Lee, D.D.; Patel, T. Extracellular vesicles from bone marrow-derived mesenchymal stem cells protect against murine hepatic ischemia/reperfusion injury. Liver Transpl. 2017, 23, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cen, P.; Chen, J.; Fan, L.; Li, J.; Cao, H.; Li, L. Role of mesenchymal stem cells; their derived factors; and extracellular vesicles in liver failure. Stem Cell. Res. Ther. 2017, 8, 137. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, M.; Yates, C.C.; Nuschke, A.; Griffith, L.; Wells, A. The matrikine tenascin-C protects multipotential stromal cells/mesenchymal stem cells from death cytokines such as FasL. Tissue Eng. Part A 2013, 19, 1972–1983. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Jiang, L.; Li, H.; Shi, H.; Luo, H.; Zhang, Y.; Yu, C.; Jin, Y. Mesenchymal stem cells prevent hypertrophic scar formation via inflammatory regulation when undergoing apoptosis. J. Investig. Dermatol. 2014, 134, 2648–2657. [Google Scholar] [CrossRef] [Green Version]
- Maiborodin, I.V.; Morozov, V.V.; Anikeev, A.A.; Figurenko, N.F.; Maslov, R.V.; Matveeva, V.A.; Chastikin, G.A.; Maiborodina, V.I. Possibility of Aggravation of Tissue Sclerosis after Injection of Multipotent Mesenchymal Stromal Cells Near the Forming Cicatrix in the Experiment. Bull. Exp. Biol. Med. 2017, 163, 554–560. [Google Scholar] [CrossRef]
- Maiborodin, I.V.; Morozov, V.V.; Matveeva, V.A.; Anikeev, A.A.; Figurenko, N.F.; Maslov, R.V.; Chastikin, G.A.; Maiborodina, V.I. Results of Experimental Ligation of the Main Vein with the Use of Cell Technologies. Bull. Exp. Biol. Med. 2017, 164, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Babaei, A.; Katoonizadeh, A.; Ranjbar, A.; Naderi, M.; Ahmadbeigi, N. Directly injected native bone-marrow stem cells cannot incorporate into acetaminophen-induced liver injury. Biologicals 2018, 52, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Yates, C.C.; Nuschke, A.; Rodrigues, M.; Whaley, D.; Dechant, J.J.; Taylor, D.P.; Wells, A. Improved transplanted stem cell survival in a polymer gel supplemented with Tenascin C accelerates healing and reduces scarring of murine skin wounds. Cell Transplant. 2017, 26, 103–113. [Google Scholar] [CrossRef]
- Maiborodin, I.V.; Morozov, V.V.; Anikeev, A.A.; Figurenko, N.F.; Maslov, R.V.; Chastikin, G.A.; Matveeva, V.A.; Maiborodina, V.I. Macrophage reaction to multipotent mesenchymal stromal cells introduction into surgical trauma site in rats. Novosti Khirurgii 2017, 25, 233–241. (In Russian) [Google Scholar] [CrossRef] [Green Version]
- Maiborodin, I.V.; Maslov, R.V.; Mikheeva, T.V.; Elovskiy, A.A.; Figurenko, N.F.; Maiborodina, V.I.; Shevela, A.I.; Anishchenko, V.V. The possibility of the angiogenesis in tissues remote from the place of the multipotent mesenchymal stromal cell injection. Mol. Meditsina 2018, 16, 22–26. (In Russian) [Google Scholar] [CrossRef]
- Shima, W.N.; Ali, A.M.; Subramani, T.; Mohamed Alitheen, N.B.; Hamid, M.; Samsudin, A.R.; Yeap, S.K. Rapid growth and osteogenic differentiation of mesenchymal stem cells isolated from human bone marrow. Exp. Ther. Med. 2015, 9, 2202–2206. [Google Scholar] [CrossRef] [Green Version]
- Qiu, K.; Chen, B.; Nie, W.; Zhou, X.; Feng, W.; Wang, W.; Chen, L.; Mo, X.; Wei, Y.; He, C. Electrophoretic deposition of dexamethasone-loaded mesoporous silica nanoparticles onto Poly(L-Lactic Acid)/Poly(ε-Caprolactone) composite scaffold for bone tissue engineering. ACS Appl. Mater. Interfaces 2016, 8, 4137–4148. [Google Scholar] [CrossRef]
- Chen, Y.; Kawazoe, N.; Chen, G. Preparation of dexamethasone-loaded biphasic calcium phosphate nanoparticles/collagen porous composite scaffolds for bone tissue engineering. Acta Biomater. 2018, 67, 341–353. [Google Scholar] [CrossRef]
- Lee, C.H.; Shah, B.; Moioli, E.K.; Mao, J.J. CTGF directs fibroblast differentiation from human mesenchymal stem/stromal cells and defines connective tissue healing in a rodent injury model. J. Clin. Investig. 2015, 125, 3992. [Google Scholar] [CrossRef] [Green Version]
- Rosenzweig, M.; Connole, M.; Glickman, R.; Yue, S.P.; Noren, B.; DeMaria, M.; Johnson, R.P. Induction of cytotoxic T lymphocyte and antibody responses to enhanced green fluorescent protein following transplantation of transduced CD34 (+) hematopoietic cells. Blood 2001, 97, 1951–1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolotova, N.M.; Maiborodin, I.V.; Fursov, S.A.; Lushnikova, E.L.; Zarubenkov, O.A.; Maiborodina, V.I. Morphology of pararectal lymph nodes in rectal cancer after neoadjuvant therapy. Bull Exp. Biol. Med. 2010, 149, 250–254. [Google Scholar] [CrossRef] [PubMed]
- De Witte, S.F.H.; Merino, A.M.; Franquesa, M.; Strini, T.; van Zoggel, J.A.A.; Korevaar, S.S. Cytokine treatment optimises the immunotherapeutic effects of umbilical cord-derived MSC for treatment of inflammatory liver disease. Stem Cell. Res. Ther. 2017, 8, 140. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Gleason, J.; Fik-Rymarkiewicz, E.; DiFiglia, A.; Bharathan, M.; Morschauser, A.; Djuretic, I.; Xu, Y.; Krakovsky, M.; Jankovic, V.; et al. Human placenta-derived mesenchymal stromal-like cells enhance angiogenesis via T cell-dependent reprogramming of macrophage differentiation. Stem Cells 2017, 35, 1603–1613. [Google Scholar] [CrossRef] [Green Version]
- Yin, Y.; Wu, R.X.; He, X.T.; Xu, X.Y.; Wang, J.; Chen, F.M. Influences of age-related changes in mesenchymal stem cells on macrophages during in-vitro culture. Stem Cell. Res. Ther. 2017, 8, 153. [Google Scholar] [CrossRef] [Green Version]
- Amouzegar, A.; Mittal, S.K.; Sahu, A.; Sahu, S.K.; Chauhan, S.K. Mesenchymal stem cells modulate differentiation of myeloid progenitor cells during inflammation. Stem Cells 2017, 35, 1532–1541. [Google Scholar] [CrossRef] [Green Version]
- Munir, H.; Ward, L.S.; Sheriff, L.; Kemble, S.; Nayar, S.; Barone, F.; Nash, G.B.; McGettrick, H.M. Adipogenic differentiation of mesenchymal stem cells alters their immunomodulatory properties in a tissue-specific manner. Stem Cells 2017, 35, 1636–1646. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maiborodin, I.; Lushnikova, E.; Klinnikova, M.; Klochkova, S. Some Special Aspects of Liver Repair after Resection and Administration of Multipotent Stromal Cells in Experiment. Life 2021, 11, 66. https://0-doi-org.brum.beds.ac.uk/10.3390/life11010066
Maiborodin I, Lushnikova E, Klinnikova M, Klochkova S. Some Special Aspects of Liver Repair after Resection and Administration of Multipotent Stromal Cells in Experiment. Life. 2021; 11(1):66. https://0-doi-org.brum.beds.ac.uk/10.3390/life11010066
Chicago/Turabian StyleMaiborodin, Igor, Elena Lushnikova, Marina Klinnikova, and Swetlana Klochkova. 2021. "Some Special Aspects of Liver Repair after Resection and Administration of Multipotent Stromal Cells in Experiment" Life 11, no. 1: 66. https://0-doi-org.brum.beds.ac.uk/10.3390/life11010066