1. Introduction
Low back pain (LBP) has become the leading cause of disabilities and absenteeism worldwide [
1,
2]. A study in 2018 showed that more than 500 million people globally suffer from this symptom and are affected by concurrent comorbidities such as depression, diabetes, and other musculoskeletal disorders [
3,
4]. These problems, when chronic, put heavy economic and psychological burdens on patients. For example, in the US, approximately
$784 million was spent on surgery and
$1.8 billion on conservative treatments in 12-month care in 2018–2019 [
5,
6,
7].
Intradiscal pressure (IDP) is the hydrostatic pressure measured in the nucleus pulposus of the intervertebral disc (IVD). As the innervated structure of the IVD [
8,
9], it is recognized as one of the potential causes of LBP. Studies have discovered that an increased IDP may accelerate the process of disc degeneration [
10,
11,
12]. In the degenerated disc, the amount of incompressible fluid decreases, and the nucleus pulposus cannot maintain even pressure on the adjacent annulus fibrosus and endplates, which could be a mechanical cause of LBP [
13]. Thus, understanding the factors that could affect the IDP could help clinicians and scientists to develop and modify the strategy for managing LBP.
Many studies have investigated the relationships between lumbar IDP and postures. Although finite models have calculated IDP in recent years, in vivo measurements tend to show more accurate data. A previous study suggests that a finite model is never “valid” for all situations and applications; instead, validation is tied to a specific topic of interest [
14]. Moreover, a number of these validation studies may fail in providing complete modelling methodologies and validation data [
15]. In the 1960s, Nachemson et al. implanted a pressure transducer into the IVD to measure the IDP directly [
16]. In earlier studies, they reported that sitting increases the IDP by 40% more than standing [
17]. In 1975, Andersson et al. performed a similar experiment using a subminiature pressure transducer and found that the IDP in standing is about 35% of that in relaxed sitting without back support [
18]. Since then, sitting has been considered a risk factor that induces high lumbar IDP.
With the continuous advancement in transducer design, results of the in vivo IDP measures do not coincide with those of previous studies [
19]. More recently, new methods such as internal spinal fixators and vertebral body replacement (VBR) have been seen as alternatives to obtaining in vivo IDP measurements. Similarly, results from current IDP studies are not consistent with earlier results and do not support the hypothesis that sitting increases the load on the lumbar spine. For example, a study that estimated IDP by measuring disc heights inferred that standing could impose higher loads on the lumbar spine than sitting [
20]. Based on more recent studies, the strategy of reducing sitting time to prevent LBP may not be valid. A systematic review in 2008 [
21] evaluated the effect of posture on IDP data and concluded that sitting and standing have a similar level of IDP. In addition, a review in 2015 conducted several comparisons of different postures in vivo and vitro measurement, and their conclusion supports the similar IDP as well [
22]. The limitation in measurement technology could be a confounding factor that affects the accuracy of the IDP measure. For example, the insertion of a needle transducer will result in abnormal muscle contraction when changing postures [
23]. To date, no study has evaluated the effect of sitting and standing on IDP using a meta-analysis. Therefore, this study aims to estimate the effect size of lumbar IDP in vivo measurement in sitting compared to standing posture. This study will also compare the effect size estimate between (1) dated and more recent studies and (2) healthy and degenerated IVDs.
2. Methods
2.1. Identification and Selection of Studies
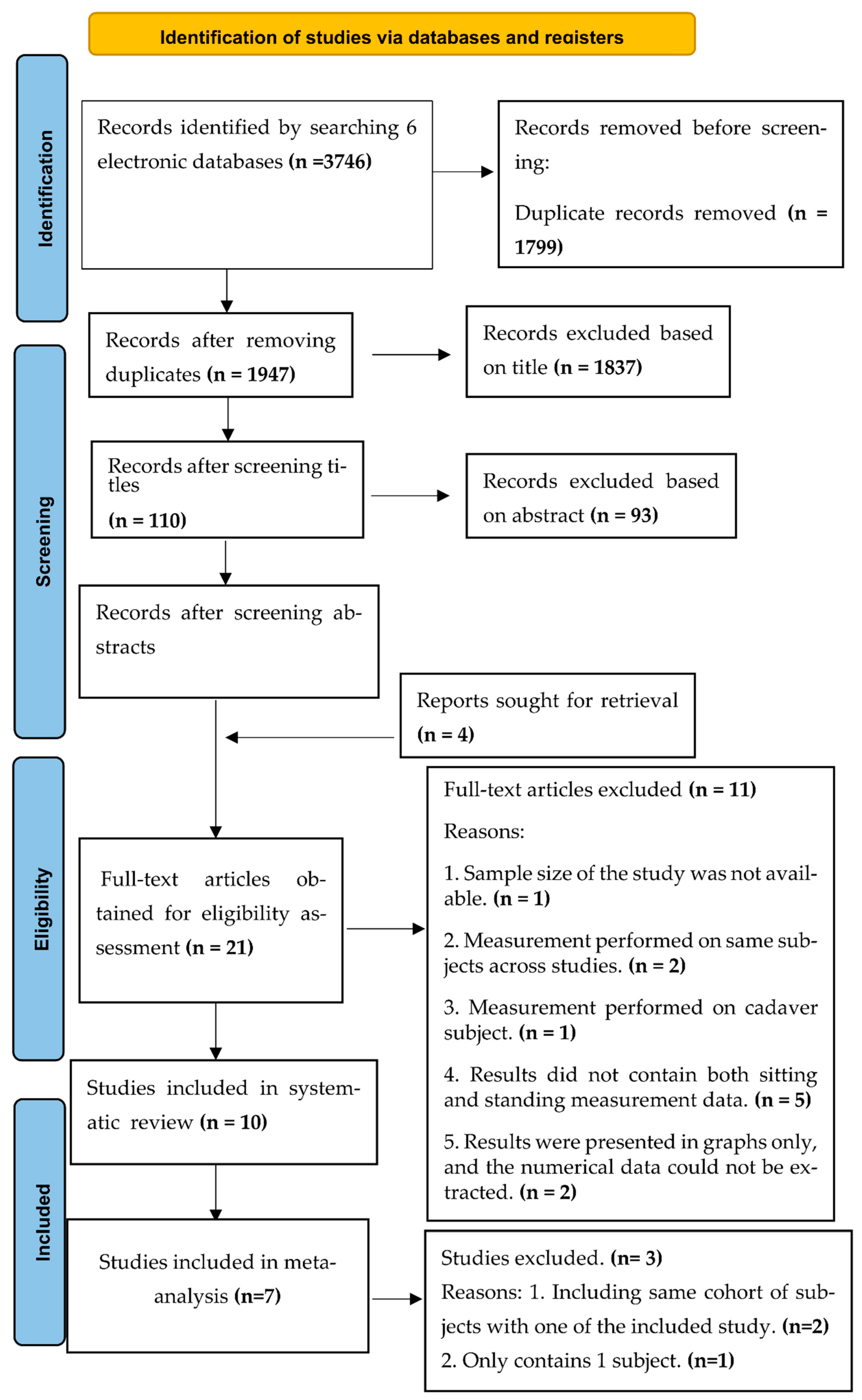
A systematic search was performed by two reviewers (Li J and Chan M) for articles published before November 2021, and there was no restriction on the earliest publication date. Six electronic databases, namely, Google Scholar, Scopus, PubMed, Web of Science, EMBASE, and Cochrane Library, were used to search for the related articles. The detailed searching strategy is presented in
Appendix A. The keywords used in the literature search included healthy adults, sitting posture, standing posture, in vivo spinal loads, and in vivo IDP. Hand searching was also performed to obtain additional information by Li J and Chan M. The reference lists of the included studies were reviewed (backward tracking), and literature citing the included studies were tracked (forward tracking) to identify additional studies. For each paper, the ‘similar articles’ option in the PubMed database was used to further expand the search. Two reviewers (Li J and Chan M) screened for potentially eligible studies.
Figure 1 illustrates the searching process. Disagreements regarding the eligibility of studies were resolved by discussion with a third reviewer (Kwong PWH).
Studies were included in the review if they (1) involved in vivo IDP measurement in both sitting and standing postures, (2) involved measurements with intervertebral body replacement, and (3) included spinal loading data of healthy adults. Studies were excluded if they (1) investigated in vitro measurement of IDP, (2) did not report the central tendency and/or variability of the outcome of interest, and (3) were letters to the editor, case studies, case series or review articles. For the relevant papers that did not provide sufficient data, we contacted the corresponding author to acquire the data. The article written in Japanese was reviewed by a researcher who is a native Japanese speaker ( Kawabata M).
2.2. Quality Assessment
Because all included studies were cross-sectional studies and no standard assessment tools were used to assess their quality, we referenced an approach developed by Friedemann et al. [
24] that mainly considers five elements: (1) blinding of outcome assessment, (2) incomplete outcome data, (3) selective reporting, (4) precision of measurement methods, and (5) representative samples. Each of these outcomes is given a mark, resulting in a maximum of 5 marks for a cross-sectional study. We classified a paper as having moderate quality if it scored 3 or more marks. Studies with a quality score below 3 were considered low quality and were not included in the meta-analysis.
2.3. Data Extraction
Full-text reviews were performed on the selected articles after the title and abstract screening. Two reviewers (Li J and Chan M) extracted the data from articles independently. A standardized data extraction form was used to extract the data from the included studies. The extracted information included the sample size, characteristics of participants (age, gender, and disc condition), and outcomes (type of outcome measures and means and standard deviations (SDs) of the outcomes). For one study that measured the IDP at two spinal levels [
25], we extracted the value of the L4-5 level only to ensure that individual data were not repeatedly included in the meta-analysis.
2.4. Data Synthesis and Analysis
The primary outcome measures were direct measures of the participants’ IDP or force at the lumbar level (containing the internal fixators with several segments, including adjacent thoracic vertebrae). Mean values and the SDs of the IDP were used to estimate the effect size. The mean value and SD were either directly extracted from the study or calculated manually according to the respective data of each subject provided in the article.
The statistical analyses were performed using the R language and the Meta package [
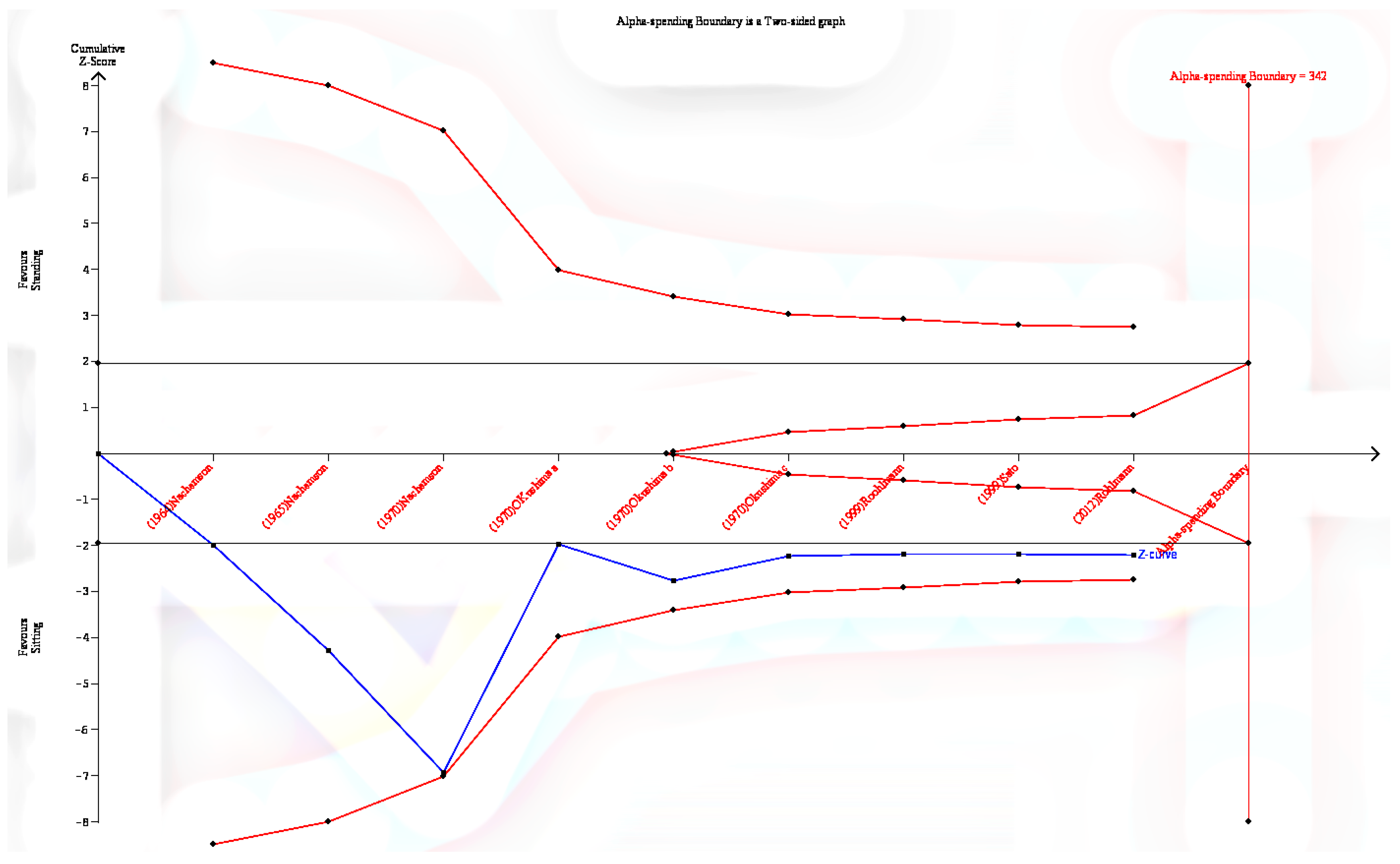
26]. In addition, a trial sequential analysis was conducted to determine the required information size and adjust thresholds for significance [
27]. The trial sequential analysis was conducted using the Trial Sequential Analysis software (The Copenhagen Trial Unit, Denmark). Where studies recruited the same batch of subjects, the most recent study was included in the meta-analysis. The study with only one subject was excluded from the analysis. As the relevant studies used different units of measurement, the standardized mean difference (SMD) was used to estimate the effect size.
2.5. Measuring Heterogeneity and Publication Bias
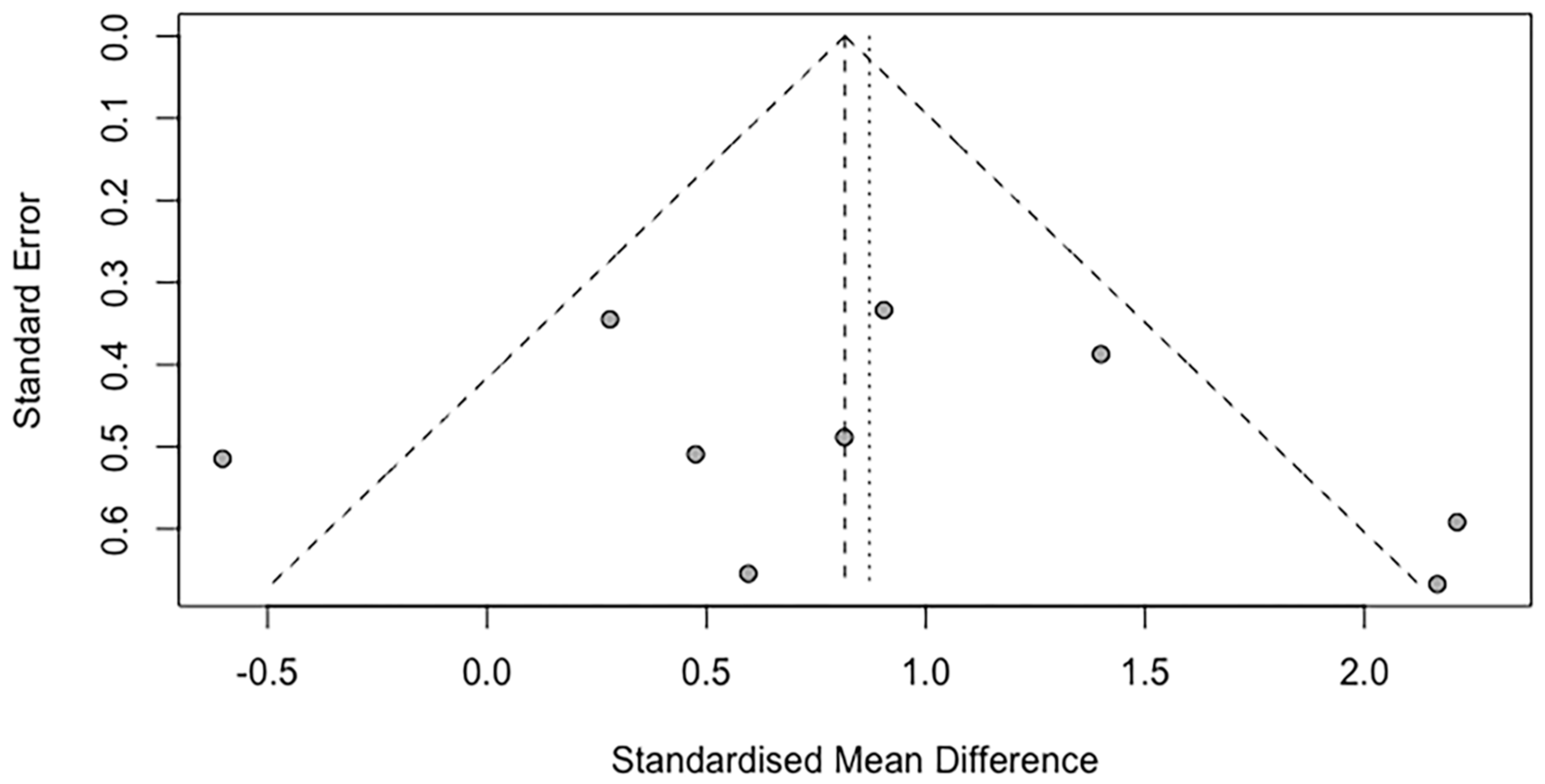
The I2 statistic was used to quantify statistical heterogeneity. A random-effects model would be used for each meta-analysis if the I2 statistic result were significant (p < 0.05) or if the I2 value were more than 50%, indicating significant heterogeneity. If the I2 statistic was non-significant, a fixed-effects model would be used, and a funnel plot was added to visualize the publication bias.
The degree of publication bias was determined using a funnel plot and Egger’s regression test. In the funnel plot, the Hedges’ g of each study was plotted against its standard error. Egger’s regression test determines whether the intercept of the precision (inverse of the standard error) regression line of each study against the weighted effect size deviates significantly from 0. The funnel plot is skewed, according to a statistically significant Egger’s regression test. For Egger’s regression test, a statistical significance threshold of p < 0.1 was used.
2.6. Subgroup Meta-Analyses
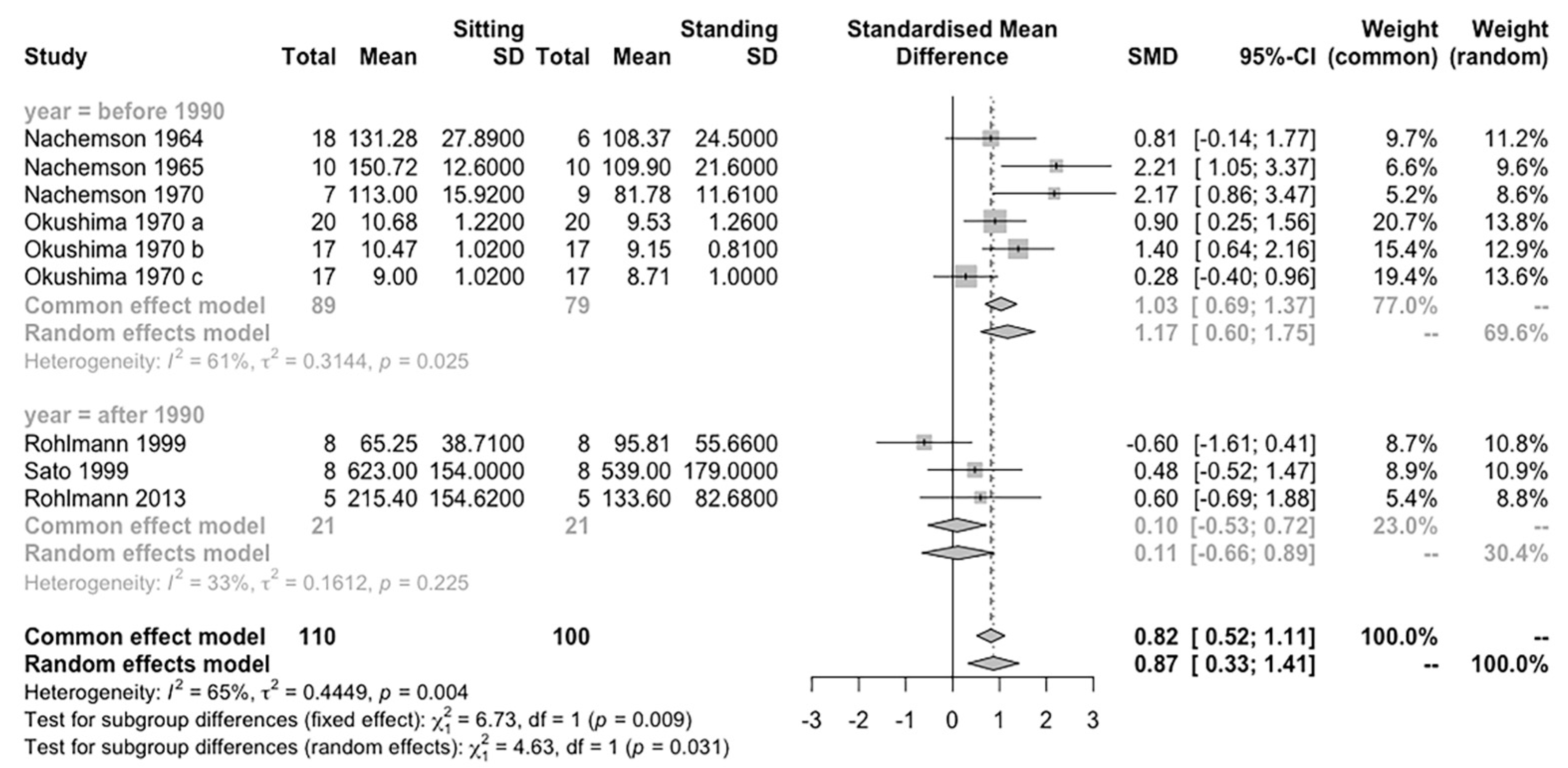
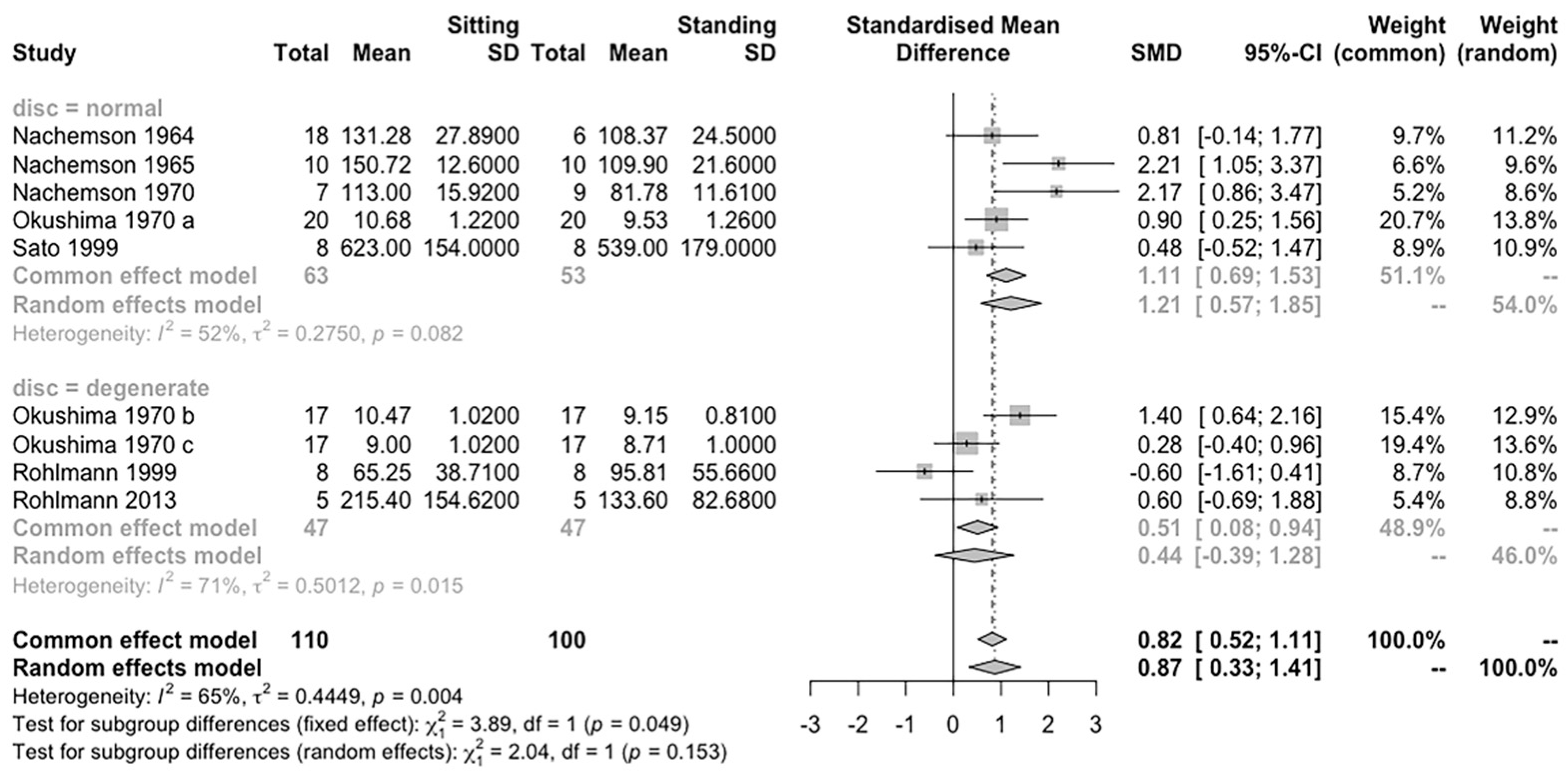
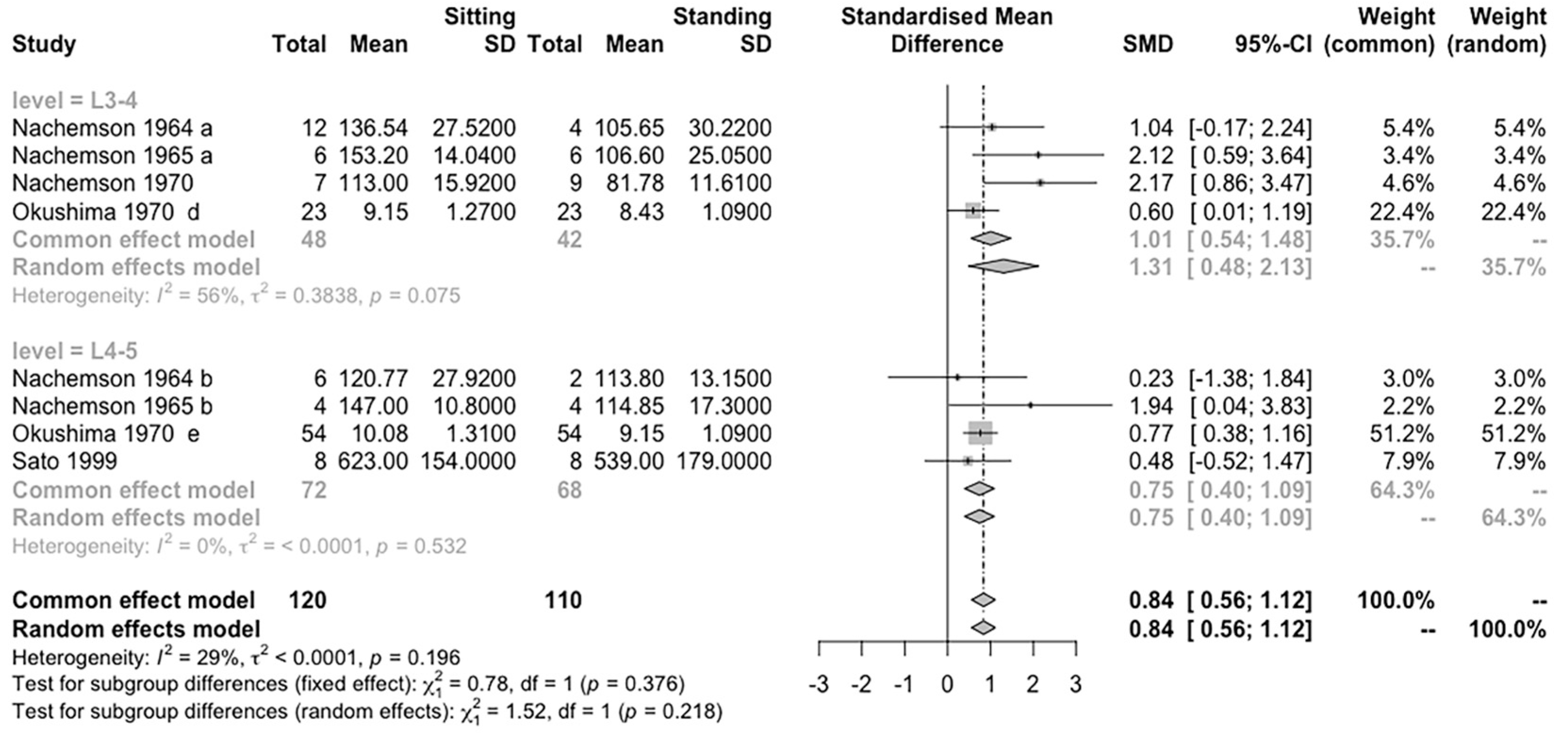
Three subgroup analyses were conducted to determine whether the effect size estimate is affected by other factors. (1) An analysis of the differences between studies published before and after 1990. This cut-off point was selected since more advanced methods to measure the spine load was developed. (2) An analysis of the differences between normal and degenerated discs, and (3) an analysis of the differences in loading between L3-4 and L4-5 discs. All the statistical tests were two-tailed, and we set α = 0.05.
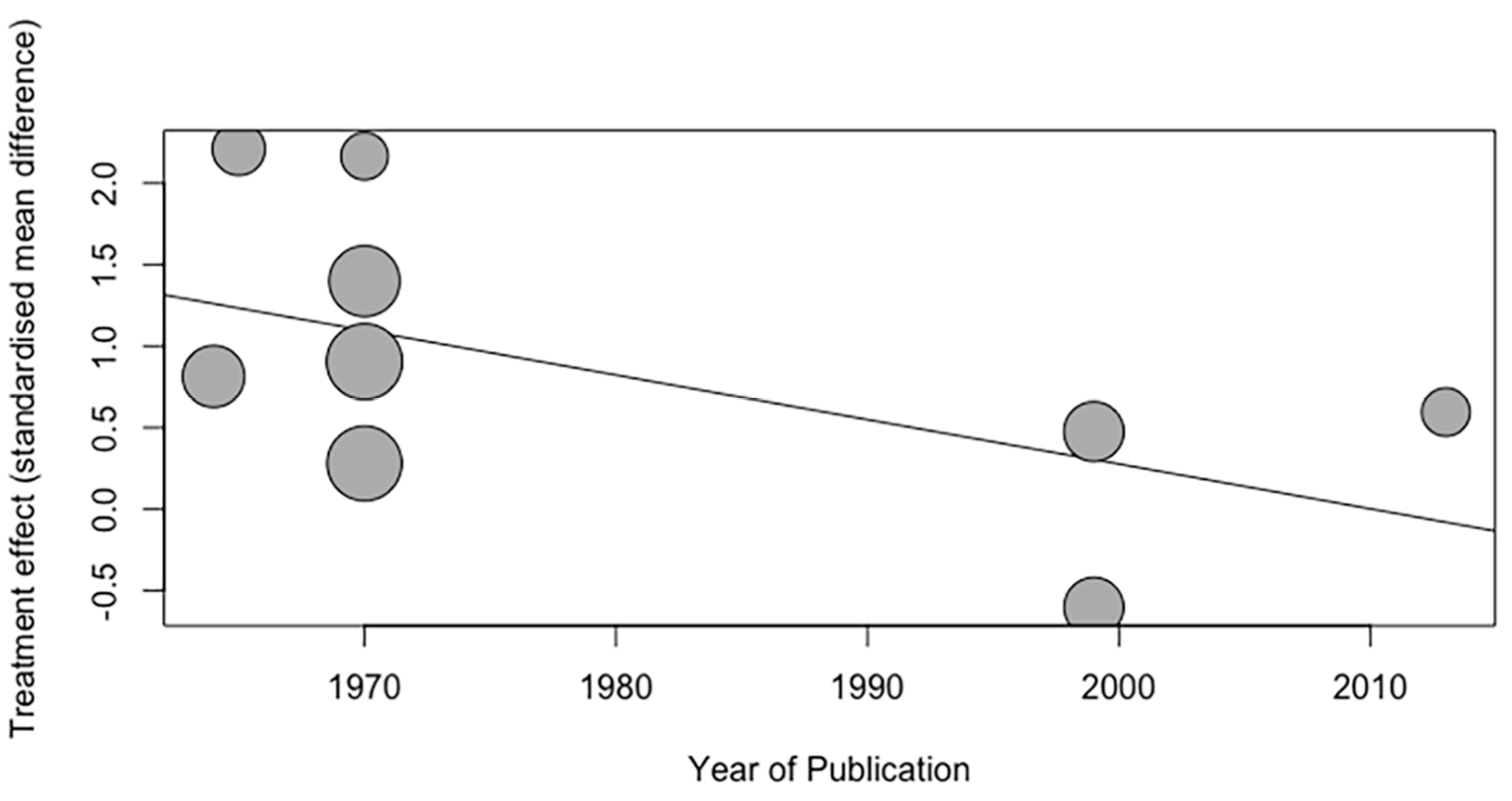
2.7. Meta-Regression
A meta-regression is used to quantify the relationship between the effect size of posture and the year of publication and total sample size of each study [
28].
4. Discussion
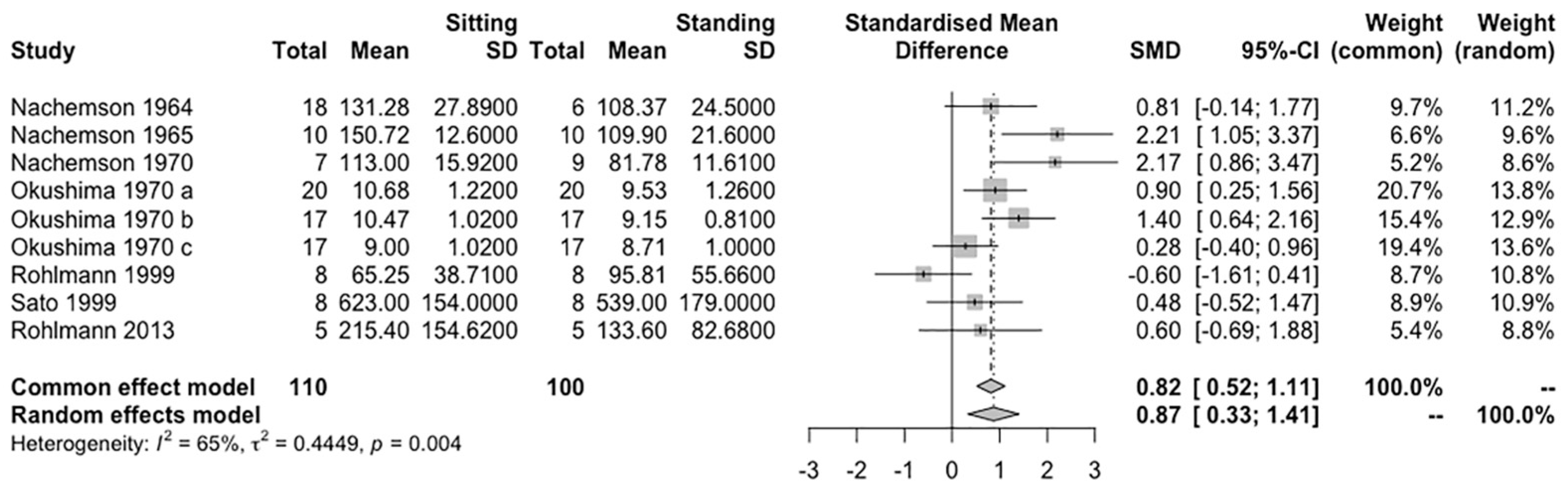
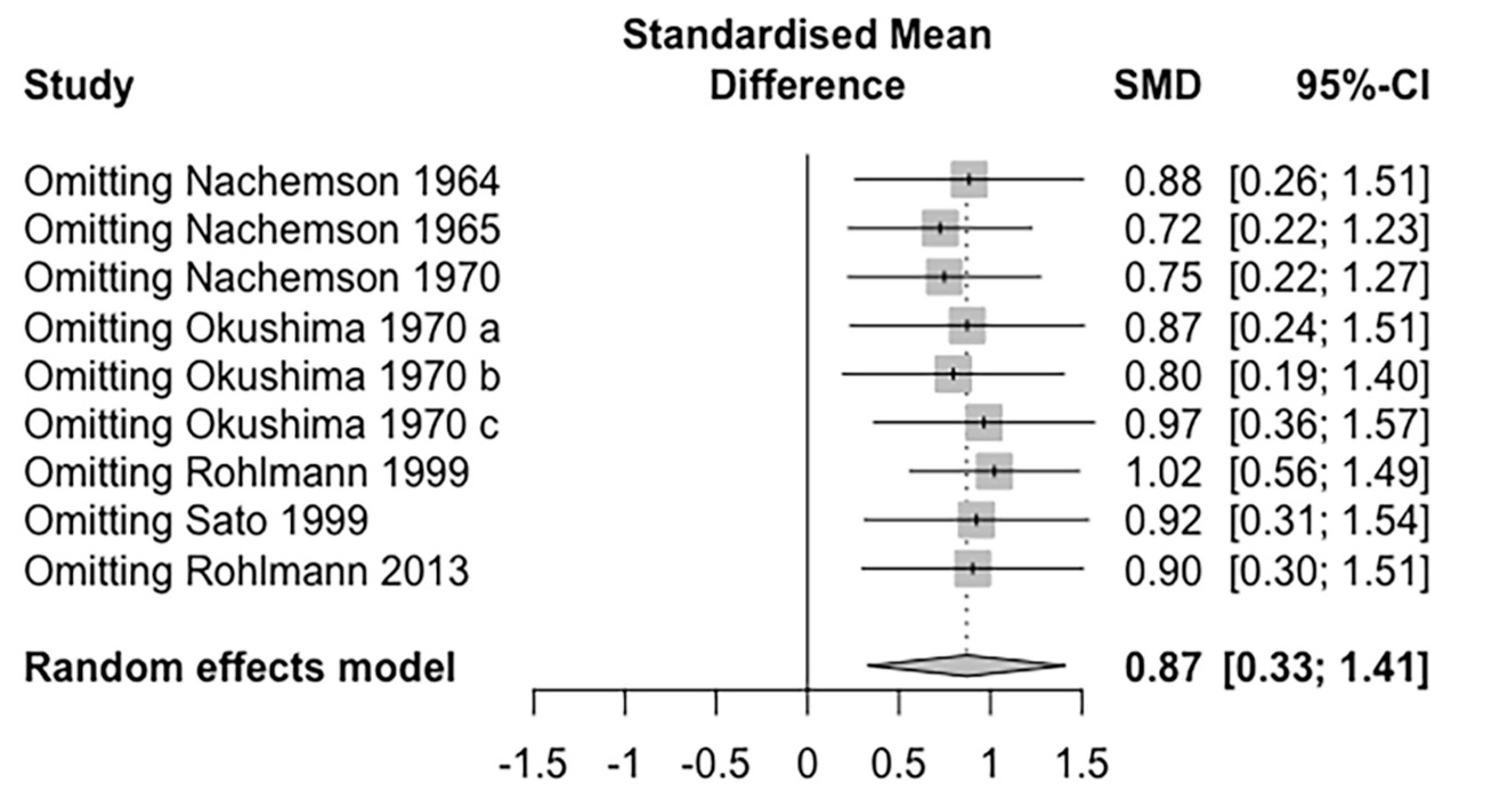
The overarching goal of this review is to contrast the in vivo lumbar spine IDP measures between sitting and standing. The results of this review highlighted that sitting induces higher loads on the lumbar spine than standing in general. However, a meta-analysis of the more recent studies showed no significant difference between sitting and standing, which is consistent with the conclusion of the two reviews [
21,
22]. Besides, the trial sequential analysis showed that the overall effect size still falls within the adjusted monitoring boundary, indicating that more study is required. In addition, the degenerated discs showed no difference in IDP in both postures.
4.1. Effect of Posture Variety in IDP Measurement
The meta-analysis of eligible studies showed that sitting induces a higher load on the lumbar spine than standing, which is consistent with earlier recommendations to avoid long sitting times in daily life [
39]. However, most results were based on data from more than 30 years ago. In 2001, Wilke et al. [
35] found that sitting and standing have similar effects on the lumbar spine IDP. They used a new implant transducer, a smaller apparatus, and their findings highly agreed with anthropometric data in many finite models. This improved equipment could stay securely in the IVD, thus ensuring that the measure is highly accurate and reliable. Rohlmann et al. [
36] used internal spinal fixators and reported similar results in 1999. The implant of the vertebral body could restore normal load-bearing in the spine and collect the three degree-of-freedom force and moment data. Their results revealed that there is a higher load on the lumbar spine in standing because the upright position increases axial loads. The increase in lumbar lordosis in standing also raises the concave-sided compression force. These findings indicated that the improvement in measurement technique may lead to a dramatic difference in the observed in vivo IDP.
The subgroup analysis that separated studies before and after the 1990s showed that there is no difference between the sitting and standing postures in more recent studies, which agrees with our hypothesis. However, only three studies [
30,
34,
36] conducted in vivo IDP measurements after the 1990s and only 21 participants were involved. Therefore, these results should be interpreted with caution.
4.2. Effect of Disc Conditions and Levels on IDP Measurement
Because the measurements are of the pressure of the nucleus pulposus [
40], according to previous studies, degenerative changes may affect the measure outcomes [
41,
42]. The bulging lamellae are squeezed by compressive load, and a disrupted disc partially loses the function of weight-bearing, thus showing higher stress in the annulus while reducing the nucleus pressure [
43]. Considering the potential effects of pathological conditions in the disc, we performed a subgroup meta-analysis of the normal and the degenerated discs. Possibly, there is no difference of IDP between sitting and standing, and the degenerative changes do not change the comparison result, as both demonstrated the decreased measured value in general. Referring to the differences between disc levels, the results show no significant change in the effect size estimation, and indicated that the effect of posture could be similar on the two spinal segments.
4.3. Large Variation in Outcomes
The variability of the IDP measure is high, even in similar disc conditions and in the same study, possibly because of the various types of transducers used. The earliest measurement [
32] used a polyethylene-tipped liquid-filled transducer and obtained data nearly twice that of later measurements [
19,
34], 11 atmospheres compared with 5~6 atmospheres. Measurements using a piezoresistive needle and implanted transducers obtained similar outcomes, although confounding factors such as muscle activation and ligament responses still existed. Another possible source of error is the measurement process. The sequence of sitting and standing changes the body height, and prolonged standing reduces the disc height, thus lowering the spine loads [
20] and eventually impacting the results.
Moreover, considering individual factors, people with a higher weight will put more upper limb pressure on the same disc. Females with small nucleus pulposus areas along the spine will possibly have relatively lower IDPs. Thus, the variability of the IDP can be high if the participants have diverse body builds.
There is also some variation in the VBR measurement [
29,
30,
31,
36]. The location of each patient’s surgery level is varied, resulting in different outcomes. Moreover, in the early stages after surgery, patients may suffer from pain and psychological factors that restrict motion; therefore, the outcome difference may appear on the left and right sides and existing regional variations sometimes. Considering the implants in different spine levels and surgery setups within patients, sintered cancellous bone and bridged intact disc induce relatively high loads, while slight compression for implant mounting shows relatively lower loads [
44].
4.4. Clinical Implication
Management of LBP includes several aspects. In addition to medicine, surgery, and psychological counselling to relieve pain [
45,
46], posture control is essential and preventative. Since Nachemson [
33] reported that sitting led to a more significant loading on lumbar discs than standing, it was widely accepted that sitting poses more risks to intervertebral discs. The current review reveals that the previous viewpoint may not be correct, given the inconsistent findings of the more recent studies. Knowledge regarding the lumbar spinal loads in daily life is essential in LBP management [
47]. Well recognized factors such as flexion and lifting weights result in a high spinal load [
21,
30,
48]. The ‘postural perturbations’ strategy proposed recently can induce a high IDP, which interacts with the degenerated disc [
49]. Existing conclusions are still controversial regarding the effect of the sitting and standing postures on IDP. Regardless of which posture induces a higher IDP, any prolonged posture is not recommended [
50].
4.5. Limitation
This review has some limitations. First, the studies that undertook in vivo measurements are relatively few, and some of them were published decades ago and thus cannot provide the most recent data in this field and should be interpreted cautiously. Second, it is possible that there are duplicate subjects in some articles published by the same authors.
5. Conclusions
In conclusion, sitting induces higher loads on the lumbar spine than standing. However, this finding should be interpreted cautiously, as more recent studies indicate similar values or contradictory conclusions in both postures, even if they are in small quantities. The trial sequential analysis also indicates that the current number of studies may not provide sufficient statistical power. Furthermore, degenerated discs have a smaller IDP, and they show no difference in IDP in the sitting and standing postures may possibly result from the evenly distributed structures being ruptured. Furthermore, to maintain the well-functioning of the lumbar spine and manage LBP symptoms, any prolonged posture should be prohibited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








