Biofunctionalization with a TGFβ-1 Inhibitor Peptide in the Osseointegration of Synthetic Bone Grafts: An In Vivo Study in Beagle Dogs

 , , ,
, , , 

Abstract
:1. Introduction
2. Results
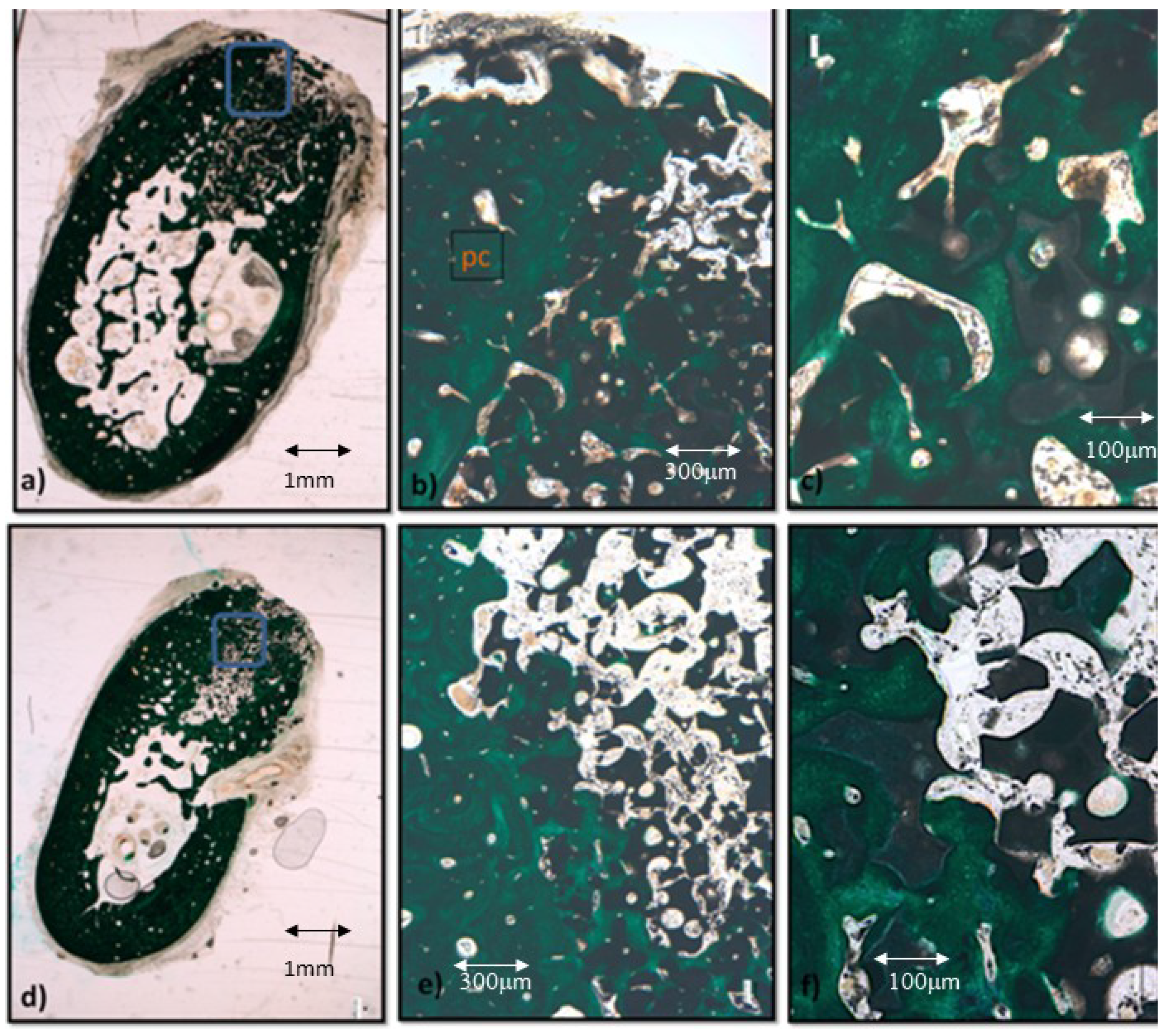
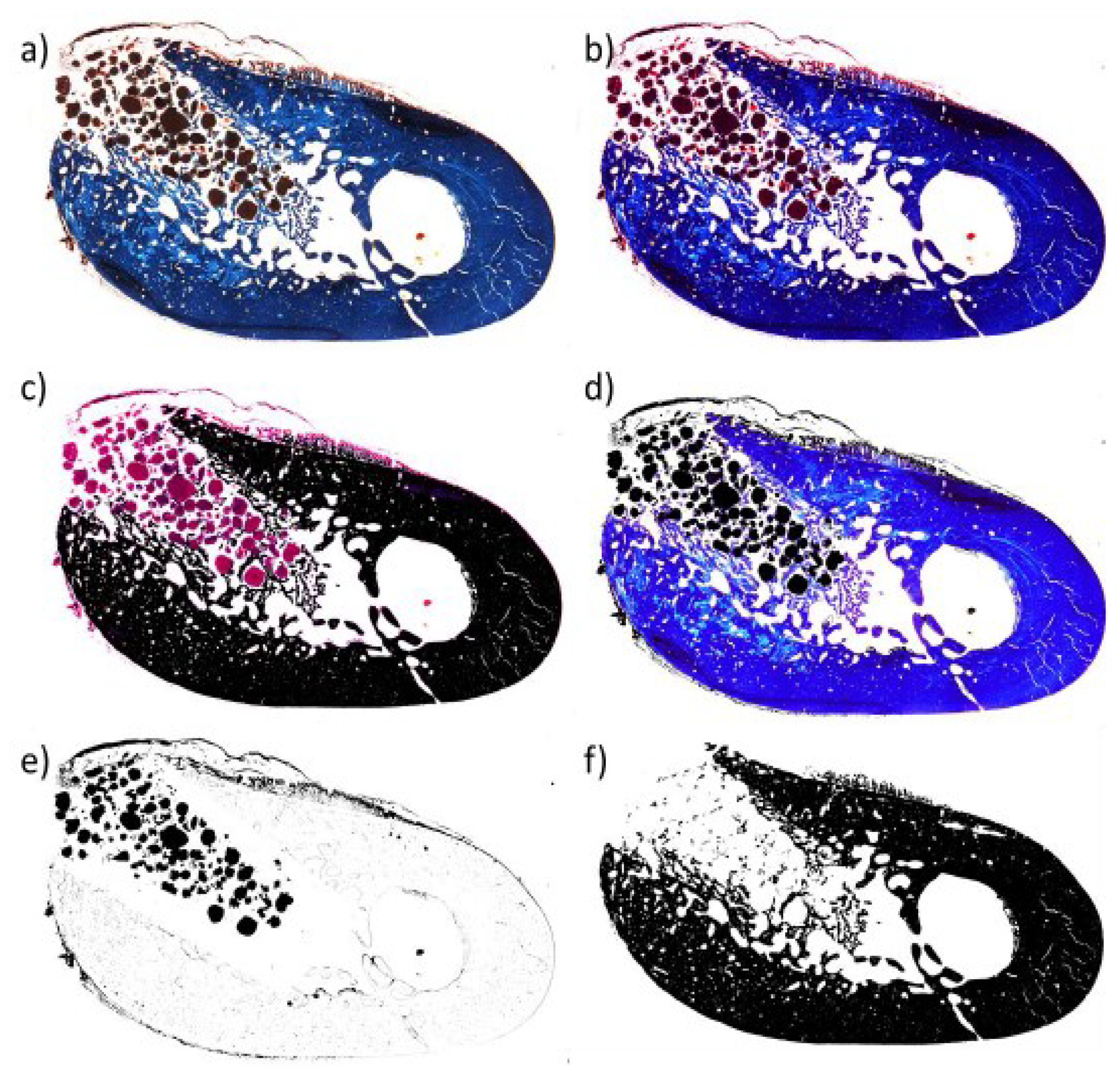
Histology and BS-SEM Analysis
3. Discussion
4. Materials and Methods
4.1. Description of Bone Grafts
4.2. Animal Model and Animal Selection Criteria
4.3. Surgical Procedures
4.4. Histology and Sample Preparation
4.5. Image Acquisition and Quantification
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burchardt, H. The Biology of Bone Graft Repair. Clin. Orthop. Relat. Res. 1983, 174, 28–42. [Google Scholar] [CrossRef]
- Jensen, O.T.; Sennerby, L. Histologic Analysis of Clinically Retrieved Titanium Microimplants Placed in Conjunction with Maxillary Sinus Floor Augmentation. Int. J. Oral Maxillofac. Implant. 1998, 13, 513–521. [Google Scholar]
- Tong, D.C.; Rioux, K.; Drangsholt, M.; Beirne, O.R. A Review of Survival Rates for Implants Placed in Grafted Maxillary Sinuses Using Meta-Analysis. Int. J. Oral Maxillofac. Implant. 1998, 13, 175–182. [Google Scholar]
- Bouwman, W.F.; Bravenboer, N.; Zijderveld, S.A.; Schulten, E.A.J.M.; Bruggenkate, C.M. The Use of Straumann Bone Ceramic in a Maxillary Sinus Floor Elevation Procedure: A Clinical, Radiological, Histological and Histomorphometric Evaluation with a 6-Month Healing Period. Clin. Oral Implant. Res. 2010, 21, 201–208. [Google Scholar] [CrossRef]
- Stein, J.M.; Fickl, S.; Yekta, S.S.; Hoischen, U.; Ocklenburg, C.; Smeets, R. Clinical Evaluation of a Biphasic Calcium Composite Grafting Material in the Treatment of Human Periodontal Randomized Controlled Clinical Trial. J. Periodontol. 2009, 80, 1774–1782. [Google Scholar] [CrossRef] [PubMed]
- Zirk, M.L.; Puhar, I. Monophasic SS-TCP vs. Biphasic HA/ß-TCP in Two-Stage Sinus Floor Augmentation Procedures-a Prospective Randomized Clinical Trial. Clin. Oral Implant. Res 2016, 1–9. [Google Scholar] [CrossRef]
- Reynolds, M.A.; Aichelmann-reidy, M.E.; Branch-mays, G.L.; Gunsolley, J.C. The Efficacy of Bone Replacement Grafts in the Treatment of Periodontal Osseous Defects. A Systematic Review. Ann. Peridodontol. 2003, 8, 227–265. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Lindhe, J. Dimensional Ridge Alterations Following Tooth Extraction. An Experimental Study in the Dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Chang, Y.-C.; Ho, K.-N.; Feng, S.-W.; Huang, H.-M.; Chang, C.-H.; Lin, C.-T.; Teng, N.-C.; Pan, Y.H.; Chang, W.-J. Fibronectin-Grafted Titanium Dental Implants: An in Vivo Study. Biomed Res. Int. 2016, 2016, 1–11. [Google Scholar] [CrossRef]
- Mahesh, L.; Venkataraman, N.; Shukla, S.; Prasad, H.; Kotsakis, G.A. Alveolar Ridge Preservation with the Socket-Plug Technique Utilizing an Alloplastic Putty Bone Substitute or a Particulate Xenograft: A Histological Pilot Study. J. Oral Implantol. 2015, 41, 178–183. [Google Scholar] [CrossRef]
- Ebrahimi, M.; Pripatnanont, P.; Monmaturapoj, N.; Suttapreyasri, S. Fabrication and Characterization of Novel Nano Hydroxyapatite/β-Tricalcium Phosphate Scaffolds in Three Different Composition Ratios. J. Biomed. Mater. Res. Part A 2012, 100, 2260–2268. [Google Scholar] [CrossRef]
- Das, S.; Jhingran, R.; Bains, V.; Madan, R.; Srivastava, R.; Rizvi, I. Socket Preservation by Beta-Tri-Calcium Phosphate with Collagen Compared to Platelet-Rich Fibrin: A Clinico-Radiographic Study. Eur. J. Dent. 2016, 10, 264. [Google Scholar] [CrossRef]
- Takahashi, Y.; Marukawa, E.; Omura, K. Application of a New Material (β-TCP/Collagen Composites) in Extraction Socket Preservation: An Experimental Study in Dogs. Int. J. Oral Maxillofac. Implant. 2013, 28, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Cuzmar, E.; Perez, R.A.; Manzanares, M.-C.; Ginebra, M.-P.; Franch, J. In Vivo Osteogenic Potential of Biomimetic Hydroxyapatite/Collagen Microspheres: Comparison with Injectable Cement Pastes. PLoS ONE 2015, 10, e0131188. [Google Scholar] [CrossRef] [PubMed]
- Guicheux, J.; Gauthier, O.; Aguado, E.; Heymann, D.; Pilet, P.; Couillaud, S.; Faivre, A.; Daculsi, G. Growth Hormone-Loaded Macroporous Calcium Phosphate Ceramic: In Vitro Biopharmaceutical Characterization and Preliminaryin Vivo Study. J. Biomed. Mater. Res. 1998, 40, 560–566. [Google Scholar] [CrossRef]
- Minier, K.; Touré, A.; Fusellier, M.; Fellah, B.; Bouvy, B.; Weiss, P.; Gauthier, O. BMP-2 Delivered from a Self-Cross-Linkable CaP/Hydrogel Construct Promotes Bone Regeneration in a Critical-Size Segmental Defect Model of Non-Union in Dogs. Vet. Comp. Orthop. Traumatol. 2014, 27, 411–421. [Google Scholar] [CrossRef]
- Abdullah, W.A. Micro CT Evaluation of Bone Regenerative Capacity in Rats Claverial Bone Defect Using Platelet Rich Fibrin with and without Beta Tri Calcium Phosphate Associate Professor, OMFS Department, Dental College, King Saud University, Saudi Arabia. Saudi Dent. J. 2015, 28, 109–117. [Google Scholar] [CrossRef]
- Ohgushi, H.; Caplan, A.I. Stem Cell Technology and Bioceramics: From Cell to Gene Engineering. J. Biomed. Mater. Res. 1999, 48, 913–927. [Google Scholar] [CrossRef]
- Legeros, R.Z. Properties of Osteoconductive Biomaterials: Calcium Phosphates. Clin. Orthop. Relat. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef]
- Bouler, J.M.; Pilet, P.; Gauthier, O.; Verron, E. Acta Biomaterialia Biphasic Calcium Phosphate Ceramics for Bone Reconstruction: A Review of Biological Response. Acta Biomater. 2017, 53, 1–12. [Google Scholar] [CrossRef]
- Cornelini, R.; Rubini, C.; Fioroni, M.; Favero, G.A.; Strocchi, R.; Piattelli, A. Transforming Growth Factor-Beta 1 Expression in the Peri-Implant Soft Tissues of Healthy and Failing Dental Implants. J. Periodontol. 2003, 74, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Sadowska, J.M.; Wei, F.; Guo, J.; Guillem-Marti, J.; Ginebra, M.-P.; Xiao, Y. Effect of Nano-Structural Properties of Biomimetic Hydroxyapatite on Osteoimmunomodulation. Biomaterials 2018, 181, 318–332. [Google Scholar] [CrossRef] [PubMed]
- Santiago, B.; Gutierrez-Cañas, I.; Dotor, J.; Palao, G.; Lasarte, J.J.; Ruiz, J.; Prieto, J.; Borrás-Cuesta, F.; Pablos, J.L. Topical Application of a Peptide Inhibitor of Transforming Growth Factor-Beta1 Ameliorates Bleomycin-Induced Skin Fibrosis. J. Investig. Dermatol. 2005, 125, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Branton, M.H.; Kopp, J.B. TGF-Beta and Fibrosis. Microbes Infect. 1999, 1, 1349–1365. [Google Scholar] [CrossRef]
- Janssens, K.; ten Dijke, P.; Janssens, S.; Van Hul, W. Transforming Growth Factor-Beta1 to the Bone. Endocr. Rev. 2005, 26, 743–774. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E.; Mendes, V.C.; Ko, J.C.H.; Ajami, E. Biomaterials Topographic Scale-Range Synergy at the Functional Bone/Implant Interface. Biomaterials 2014, 35, 25–35. [Google Scholar] [CrossRef]
- Ezquerro, I.-J.; Lasarte, J.-J.; Dotor, J.; Castilla-Cortázar, I.; Bustos, M.; Peñuelas, I.; Blanco, G.; Rodríguez, C.; Marıa del Carmen, G.L.; Greenwel, P.; et al. A Synthetic Peptide from Transforming Growth Factor Beta Type III Receptor Inhibits Liver Fibrogenesis in Rats with Carbon Tetrachloride Liver Injury. Cytokine 2003, 22, 12–20. [Google Scholar] [CrossRef]
- Vicent, S.; Luis-Ravelo, D.; Antón, I.; García-Tuñón, I.; Borrás-Cuesta, F.; Dotor, J.; De Las Rivas, J.; Lecanda, F. A Novel Lung Cancer Signature Mediates Metastatic Bone Colonization by a Dual Mechanism. Cancer Res. 2008, 68, 2275–2285. [Google Scholar] [CrossRef]
- Serratì, S.; Margheri, F.; Pucci, M.; Cantelmo, A.R.; Cammarota, R.; Dotor, J.; Borràs-Cuesta, F.; Fibbi, G.; Albini, A.; Del Rosso, M. TGFbeta1 Antagonistic Peptides Inhibit TGFbeta1-Dependent Angiogenesis. Biochem. Pharmacol. 2009, 77, 813–825. [Google Scholar] [CrossRef]
- Sevilla, P.; Cirera, A.; Dotor, J.; Gil, F.J.; Galindo-Moreno, P.; Aparicio, C. In Vitro Cell Response on CP-Ti Surfaces Functionalized with TGF-Β1 Inhibitory Peptides. J. Mater. Sci. Mater. Med. 2018, 29, 73. [Google Scholar] [CrossRef]
- Sevilla, P.; Gil, J.; Aparicio, C. Relevant Properties for Immobilizing Short Peptides on Biosurfaces. IRBM 2017, 38, 256–265. [Google Scholar] [CrossRef]
- Filvaroff, E.; Erlebacher, A.; Ye, J.; Gitelman, S.E.; Lotz, J.; Heillman, M.; Derynck, R. Inhibition of TGF-Beta Receptor Signaling in Osteoblasts Leads to Decreased Bone Remodeling and Increased Trabecular Bone Mass. Development 1999, 126, 4267–4279. [Google Scholar]
- Shen, Z.-J.; Kim, S.K.; Jun, D.Y.; Park, W.; Kim, Y.H.; Malter, J.S.; Moon, B.J. Antisense Targeting of TGF-Beta1 Augments BMP-Induced Upregulation of Osteopontin, Type I Collagen and Cbfa1 in Human Saos-2 Cells. Exp. Cell Res. 2007, 313, 1415–1425. [Google Scholar] [CrossRef]
- Weber, F.E. Reconsidering Osteoconduction in the Era of Additive Manufacturing. Tissue Eng. Part B 2019. [Google Scholar] [CrossRef]
- Barba, A.; Diez-Escudero, A.; Maazouz, Y.; Rappe, K.; Espanol, M.; Montufar, E.B.; Bonany, M.; Sadowska, J.M.; Guillem-Marti, J.; Öhman-Mägi, C.; et al. Osteoinduction by Foamed and 3D-Printed Calcium Phosphate Scaffolds: Effect of Nanostructure and Pore Architecture. ACS Appl. Mater. Interfaces 2017, 9, 41722–41736. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, M.; Botelho, M.G.; Dorozhkin, S.V. Biphasic Calcium Phosphates Bioceramics (HA/TCP): Concept, Physicochemical Properties and the Impact of Standardization of Study Protocols in Biomaterials Research. Mater. Sci. Eng. 2017, 71, 1293–1312. [Google Scholar] [CrossRef]
- Owen, G.R.; Dard, M.; Larjava, H. Review Article Hydoxyapatite/Beta-Tricalcium Phosphate Biphasic Ceramics as Regenerative Material for the Repair of Complex Bone Defects. J. Biomed. Mater. Res. Part B: Appl. Biomater. 2017, 1–20. [Google Scholar] [CrossRef]
- Daculsi, G.; Laboux, O.; Malard, O.; Weiss, P. Current State of the Art of Biphasic Calcium Phosphate Bioceramics. J. Mater. Sci. Mater. Med. 2003, 14, 195–200. [Google Scholar] [CrossRef]
- Aspenberg, P.; Jeppsson, C.; Wang, J.S.; Boström, M. Transforming Growth Factor Beta and Bone Morphogenetic Protein 2 for Bone Ingrowth: A Comparison Using Bone Chambers in Rats. Bone 1996, 19, 499–503. [Google Scholar] [CrossRef]
- Tieline, L.; Puolakkainen, P.; Pohjonen, T.; Rautavuori, J.; Törmälä, P.; Rokkanen, P. The Effect of Transforming Growth Factor-Beta1, Released from a Bioabsorbable Self-Reinforced Polylactide Pin, on a Bone Defect. Biomaterials 2002, 23, 3817–3823. [Google Scholar] [CrossRef]
- Nikolidakis, D.; Meijer, G.J.; Oortgiesen, D.AW.; Walboomers, X.F.; Jansen, J.A. The Effect of a Low Dose of Transforming Growth Factor Beta1 (TGF-Beta1) on the Early Bone-Healing around Oral Implants Inserted in Trabecular Bone. Biomaterials 2009, 30, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, K.; Abe, M.; Hiasa, M.; Oda, A.; Amou, H.; Kido, S.; Harada, T.; Tanaka, O.; Miki, H.; Nakamura, S.; et al. TGF- β Inhibition Restores Terminal Osteoblast Differentiation to Suppress Myeloma Growth. PLoS ONE 2010, 5, e9870. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Ortega, E.; Alfonso-Rodríguez, C.A.; Monsalve-Guil, L.; España-López, A.; Jiménez-Guerra, A.; Garzón, I.; Alaminos, M.; Gil, F.J. Relevant aspects in the surface properties in titanium dental implants for the cellular viability. Mater. Sci. Eng. C 2016, 64, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pegueroles, M.; Tonda-Turo, C.; Planell, J.A.; Gil, F.J.; Aparicio, C. Adsorption of fibronectin, fibrinongen, and albumin on TiO2: Time-Resolved Kinetics, Structural Changes, and Competition Study. Biointerphases 2012, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Hermida, N.; López, B.; González, A.; Dotor, J.; Lasarte, J.J.; Sarobe, P.; Borrás-Cuesta, F.; Díez, J. A synthetic peptide from transforming growth factor-β1 type III receptor prevents myocardial fibrosis in spontaneously hypertensive rats. Cardiovasc. Res. 2009, 81, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Arisan, V.; Anil, A.; Wolke, J.G.; Özer, K. The Effect of Injectable Calcium Phosphate Cement on Bone Anchorage of Titanium Implants: An Experimental Feasibility Study in Dogs. Int. J. Oral Maxillofac. Surg. 2010, 39, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.M.; Koepple, M.; Moest, T.; Neumann, K.; Weisel, T.; Schlegel, K.A. In Vivo Evaluation of Biofunctionalized Implant Surfaces with a Synthetic Peptide (P-15) and Its Impact on Osseointegration. A Preclinical Animal Study. Clin. Oral Implant. Res. 2016, 27, 1339–1348. [Google Scholar] [CrossRef]
- Aparicio, C.; Padrós, A.; Gil, F.J. In Vivo Evaluation of Micro-Rough and Bioactive Titanium Dental Implants Using Histometry and Pull-out Tests. J. Mech. Behav. Biomed. Mater. 2011, 4, 1672–1682. [Google Scholar] [CrossRef] [PubMed]
- Vivan Cardoso, M.; Vandamme, K.; Chaudhari, A.; De Rycker, J.; Van Meerbeek, B.; Naert, I.; Duyck, J. Dental Implant Macro-Design Features Can Impact the Dynamics of Osseointegration. Clin. Implant. Dent. Relat. Res. 2013, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.V.; Chaudhari, A.; Yoshida, Y.; Van Meerbeek, B.; Naert, I.; Duyck, J. Bone Tissue Response to Implant Surfaces Functionalized with Phosphate-Containing Polymers. Clin. Oral Implant. Res. 2014, 25, 91–100. [Google Scholar] [CrossRef]
- Manresa, C.; Bosch, M.; Manzanares, M.C.; Carvalho, P.; Echeverra, J.J. A New Standardized-Automatic Method for Bone-to-Implant Contact Histomorphometric Analysis Based on Backscattered Scanning Electron Microscopy Images. Clin. Oral Implant. Res. 2014, 25, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Alt, V.; Cheung, W.H.; Chow, S.K.H.; Thormann, U.; Cheung, E.N.M.; Lips, K.S.; Schnettler, R.; Leung, K.S. Bone Formation and Degradation Behavior of Nanocrystalline Hydroxyapatite with or without Collagen-Type 1 in Osteoporotic Bone Defects—An Experimental Study in Osteoporotic Goats. Injury 2016, 47, S58–S65. [Google Scholar] [CrossRef]
- Ding, M.; Henriksen, S.S.; Theilgaard, N.; Overgaard, S. Assessment of Activated Porous Granules on Implant Fixation and Early Bone Formation in Sheep. J. Orthop. Transl. 2016, 5, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Bakhshalian, N.; Abdelhamid, A.; Park, Y.J.; Zadeh, H.H. Histological and Histomorphometric Response to SocketKAPTM and SocketKAGETM Used for Ridge Preservation and Repair: Results from a Randomized Controlled Clinical Trial. J. Oral Maxillofac. Surg. 2018, 76, 1884–1892. [Google Scholar] [CrossRef] [PubMed]
- Blouin, S.; Moreau, M.F.; Weiss, P.; Daculsi, G.; Baslé, M.F.; Chappard, D. Evaluation of an Injectable Bone Substitute (BetaTCP/Hydroxyapatite/Hydroxy- Propyl-Methyl-Cellulose) in Severely Osteopenic and Aged Rats. J. Biomed. Mater. Res. A 2006, 78, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Parfitt, A.M. Trabecular Bone Architecture in the Pathogenesis and Prevention of Fracture. Am. J. Med. 1987, 82, 68–72. [Google Scholar] [CrossRef]
- Parfitt, A.M.; Drezner, M.K.; Glorieux, F.H.; Kanis, J.A.; Malluche, H.; Meunier, P.J.; Ott, S.M.; Recker, R.R. Bone Histomorphometry: Standardization of Nomenclature, Symbols, and Units: Report of the Asbmr Histomorphometry Nomenclature Committee. J. Bone Miner. Res. 2009, 2, 595–610. [Google Scholar] [CrossRef] [PubMed]
- Dempster, D.W.; Compston, J.E.; Drezner, M.K.; Glorieux, F.H.; Kanis, J.A.; Malluche, H.; Meunier, P.J.; Ott, S.M.; Recker, R.R.; Parfitt, A.M. Standardized Nomenclature, Symbols, and Units for Bone Histomorphometry: A 2012 Update of the Report of the ASBMR Histomorphometry Nomenclature Committee. J. Bone Miner. Res. 2013, 28, 2–17. [Google Scholar] [CrossRef]
- López-López, J.; Chimenos-Küstner, E.; Manzanares-Cespedes, C.; Muñoz-Sánchez, J.; Castañeda-Vega, P.; Jané-Salas, E.; Alvarez-López, J.-M.; Gimeno-Sanding, A. Histomorphological Study of the Bone Regeneration Capacity of Platelet-Rich Plasma, Bone Marrow and Tricalcium Phosphate: Experimental Study on Pigs. Medicina Oral Patología Oral y Cirugia Bucal 2009, 14, e620–e627. [Google Scholar] [CrossRef]
- Manzano, M.; Arcos, D.; Rodríguez-Delgado, M.; Ruiz, E.; Gil, F.J.; Vallet-Regí, M. Bioactive Star Gels. Chem. Mater. 2006, 18, 5696–5703. [Google Scholar] [CrossRef]
- Salinas, A.J.; Merino, J.M.; Babonneau, F.; Gil, F.J.; Vallet-Regí, M. Microstructure and Macroscopic Properties of Bioactive CaO-SiO2-PDMS Hybrids. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 81, 274–282. [Google Scholar] [CrossRef]
- Vallet-Regí, M.; San Román, J.; Padilla, S.; Doadrio, J.C.; Gil, F.J. Bioactivity and mechanical properties of SiO2-CaO-P2O5 glass-ceramics. J. Mater. Chem. 2005, 15, 1353–1359. [Google Scholar] [CrossRef]
- Fernández, E.; Gil, F.J.; Best, S.; Ginebra, M.P.; Driessens, F.C.M.; Planell, J.A. The cement setting reaction in the CaHPO4-αCa3(PO4)2 system: An X-Ray Diffraction study. J. Biomed. Mater. Res. 1998, 42, 403–406. [Google Scholar] [CrossRef]
- Lafuente, P.; Franch, J.; Durall, I.; Manzanares, C. Experimental Study of Bone Lengthening in Dogs by Means of Backscattered Scanning Electron Microscopy. Vet. Surg. 2009, 38, 388–397. [Google Scholar] [CrossRef]
- Goret-Nicaise, M. Identification of Collagen Type I and Type II in Chondroid Tissue. Calcif. Tissue Int. 1984, 36, 682–689. [Google Scholar] [CrossRef]
- Goret-Nicaise, M.; Dhem, A. The Mandibular Body of the Human Fetus. Histologic Analysis of the Basilar Part. Anat. Embryol. (Berl) 1984, 169, 231–236. [Google Scholar] [CrossRef]
- Zagba-Mongalima, G.; Goret-Nicaise, M.; Dhem, A. Age Changes in Human Bone: A Microradiographic and Histological Study of Subperiosteal and Periosteal Calcifications. Gerontology 1988, 34, 264–276. [Google Scholar] [CrossRef]
- Manzanares, M.C.; Goret-Nicaise, M.; Dhem, A. Metopic Sutural Closure in the Human Skull. J. Anat. 1988, 161, 203–215. [Google Scholar] [PubMed]
- Nery, E.B.; Lee, K.K.; Czajkowski, S.J.J.; Sullivan, O.M.R.T. Study of Biphasic Calcium Phosphate Ceramic in Periodontal Osseous Defects. J. Periodontal. 1990, 61, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Pilipili, C.M.; Nyssen-Behets, C.; Dhem, A. Microradiography and Fluorescence Microscopy of Bone Remodeling on the Basal Crypt of Permanent Mandibular Premolars in Dogs during Eruption. Connect. Tissue Res. 1995, 32, 171–181. [Google Scholar] [CrossRef]
- Pilipili, C.M.; Goret-Nicaise, M.; Dhem, A. Microradiographic Aspects of the Growing Mandibular Body during Permanent Premolar Eruption in the Dog. Eur. J. Oral Sci. 1998, 106 (Suppl. 1), 429–436. [Google Scholar] [CrossRef]
- Martino, M.M.; Briquez, P.S.; Maruyama, K.; Hubbell, J.A. Extracellular Matrix-Inspired Growth Factor Delivery Systems for Bone Regeneration. Adv. Drug Deliv. Rev. 2015, 94, 41–52. [Google Scholar] [CrossRef]
- Biguetti, C.C.; Cavalla, F.; Silveira, E.M.; Fonseca, A.C.; Vieira, A.E.; Tabanez, A.P.; Rodrigues, D.C.; Trombone, A.P.F.; Garlet, G.P.; Biguetti, C.C.; et al. Oral Implant Osseointegration Model in C57Bl/6 Mice: Microtomographic, Histological, Histomorphometric and Molecular Characterization. J. Appl. Oral Sci. 2018, 26. [Google Scholar] [CrossRef]
- Sevilla, P.; Vining, K.V.; Dotor, J.; Rodriguez, D.; Gil, F.J.; Aparicio, C. Surface Immobilization and Bioactivity of TGF-Β1 Inhibitor Peptides for Bone Implant Applications. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 385–394. [Google Scholar] [CrossRef]
- Gil, F.J.; Manzanares, N.; Badet, A.; Aparicio, C.; Ginebra, M.P. Biomimetic treatment on dental implants for short-term bone regeneration. Clin. Oral Investig. 2014, 18, 59–66. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomaterial | 2 weeks | 4 weeks | 8 weeks |
|---|---|---|---|
| BCP | 20% (8) | 33% (8) | 65% (9) |
| BCP-P-144 | 30% (6) | 40% (7) | 77% (8) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirera, A.; Manzanares, M.C.; Sevilla, P.; Ortiz-Hernandez, M.; Galindo-Moreno, P.; Gil, J. Biofunctionalization with a TGFβ-1 Inhibitor Peptide in the Osseointegration of Synthetic Bone Grafts: An In Vivo Study in Beagle Dogs. Materials 2019, 12, 3168. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12193168
Cirera A, Manzanares MC, Sevilla P, Ortiz-Hernandez M, Galindo-Moreno P, Gil J. Biofunctionalization with a TGFβ-1 Inhibitor Peptide in the Osseointegration of Synthetic Bone Grafts: An In Vivo Study in Beagle Dogs. Materials. 2019; 12(19):3168. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12193168
Chicago/Turabian StyleCirera, Andrea, Maria Cristina Manzanares, Pablo Sevilla, Monica Ortiz-Hernandez, Pablo Galindo-Moreno, and Javier Gil. 2019. "Biofunctionalization with a TGFβ-1 Inhibitor Peptide in the Osseointegration of Synthetic Bone Grafts: An In Vivo Study in Beagle Dogs" Materials 12, no. 19: 3168. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12193168