2.1. Sample Size Evaluation
The sample size of the present study was calculated setting the power of study at 80% and the level of significance at 0.05. The effect size eta-squared is 0.37, while assuming a standard deviation of 1 for each group, while considering 25 attachments for each group and a total of 75 attachments. This can be considered to be a large effect size, and it was chosen because the goal of the study is to assess clinically significant differences.
Study materials:
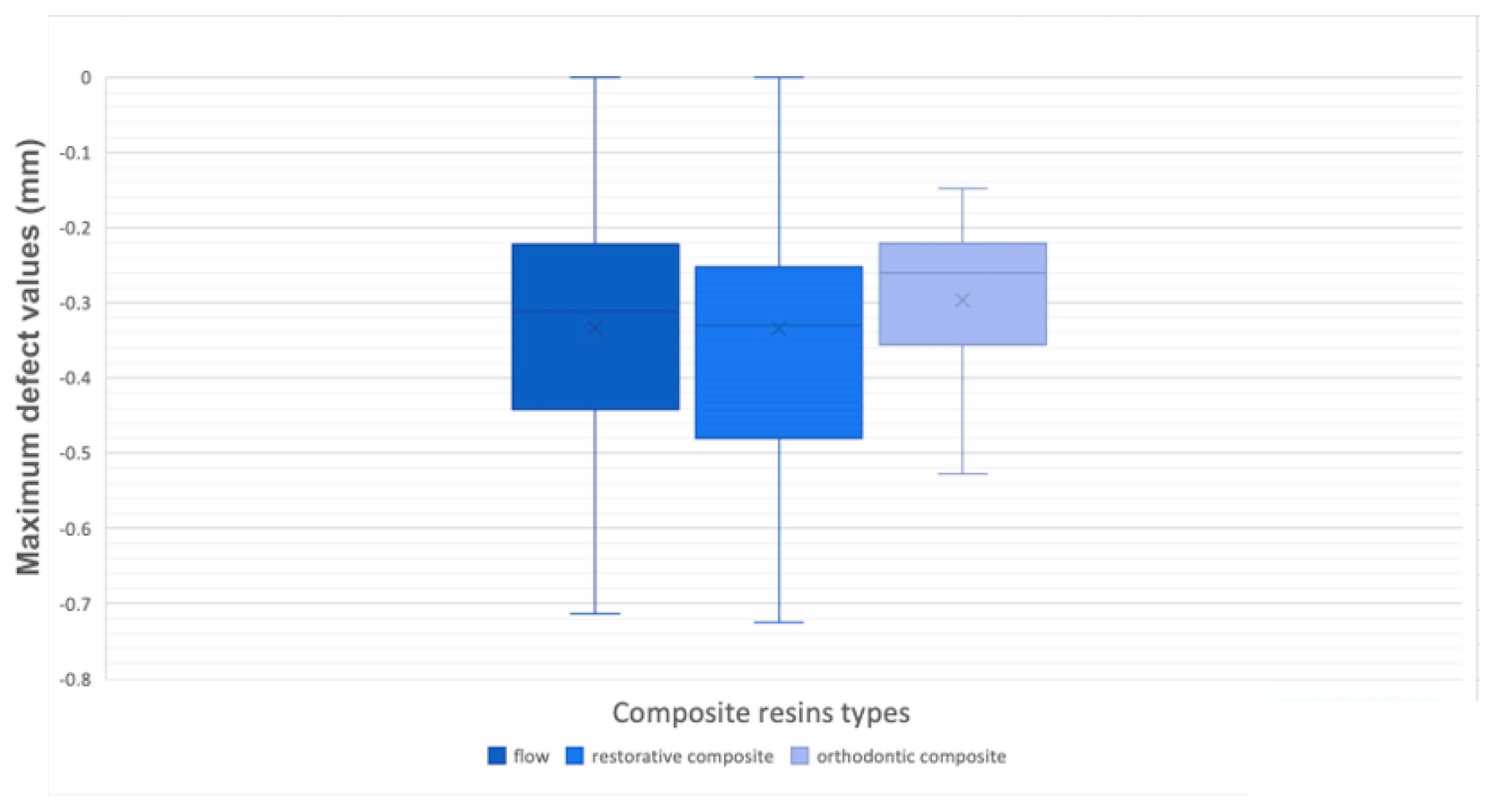
Three composite resins were selected based on three different degrees of viscosity: a low-viscosity flowable resin (ENAMEL plus HRi® Flow HF, GDF GmbH), a medium-viscosity orthodontic composite (Bracepaste® Medium Viscosity Adhesive, AO), and a high -viscosity dental restorative material (ENAMEL plus HRi® Enamel, GDF GmbH) (
Table 1).
We applied the three different materials to three pairs of phantom dental arches to test their effectiveness when reproducing the attachments. Each pair received 25 attachments on the vestibular or lingual surface of the teeth, according to the sample size calculation. In this way, it was possible to test one type of composite for each pair of dental arch, thus reproducing the real operative procedures.
2.2. Operative Procedures
Three phantom models of patients’ dental arches were made while using extracted teeth.
Briefly, the teeth were chosen depending on the following inclusion criteria: well-preserved dental crown, extraction for orthodontic, periodontal, or prosthetic reasons. Exclusion criteria were: presence of carious lesions, prosthetic crowns, or even fillings of any material.
All of the teeth were stored in a physiological solution after extraction, and then divided into four morphological groups (incisors, canines, bicuspids, and molars) and used to create realistic upper and lower arches of the three phantom models. Once the models were created, dental impressions using polyvinyl siloxane material (Flextime Heavy Tray/Correct Flow, Kulzer GmbH, Wasserburg, Germany) were taken and sent to the manufacturer of the aligners (Airnivol S.r.l., Pisa, Italy) in efforts to fabricate the templates for attachment placement. Impression records and frontal, lateral occlusal photographs were also sent as usually required by aligner manufacturers.
Thereafter, the desired attachment shapes and positions were selected while using the AirCheck tool that was provided by the aligner manufacturers (
Figure 1).
Table 2 describes the description and details of the requested attachments.
For each phantom model, 13 attachments for the upper arch and 12 for the lower arch were requested. Once the templates, including the appropriate attachments’ hollows, were received, it was possible to proceed with the attachment placement while using three different composite resins on the phantom models, as previously described [
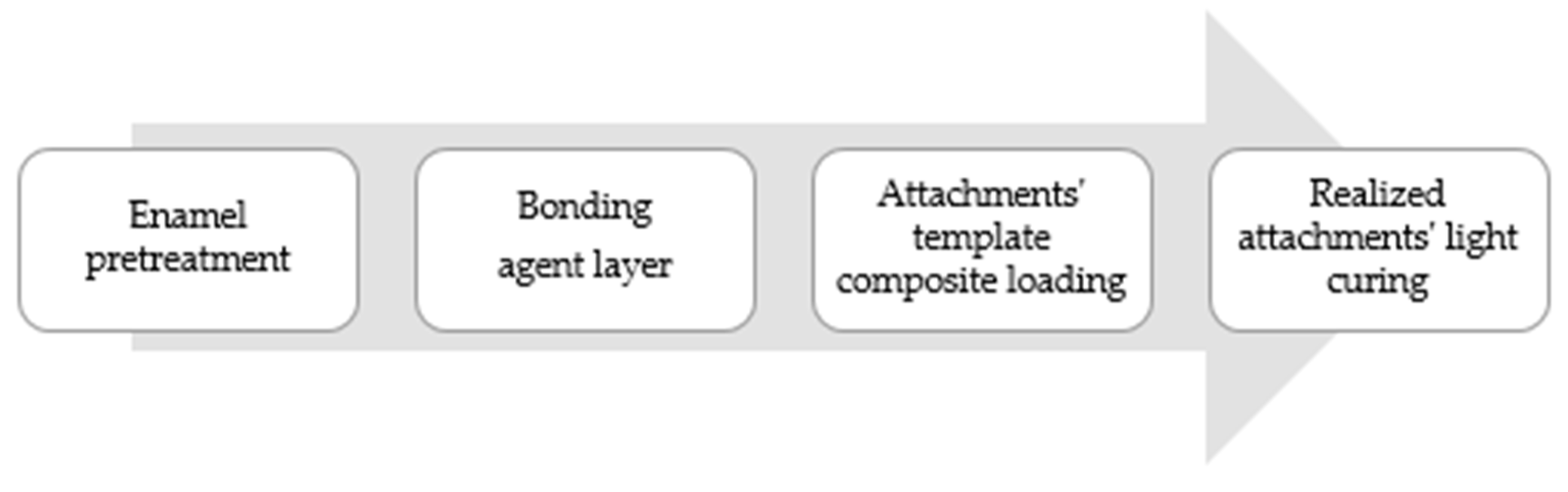
9]. Briefly, the workflow of attachments placing went as follows:
Step 1. Enamel pretreatment: To commence, the vestibular tooth surface, where the attachment needed to be placed, was etched while using a 37% orthophosphoric acid (Scientific Pharmaceuticals, Inc., Pomona, CA, USA) for 30 seconds, rinsed with plenty of water, and then dried with light air.
Step 2. Bonding: a thin bonding agent layer (iBOND Total Etch, Heraeus Kulzer, Hanau, Germany) was then applied and light-cured for 20 seconds while using a high power lamp (DB685 Super Dual, COXO Dental, Foshang, China).
Step 3. Composite loading: The resin composite was loaded into each hollows of the attachment template by using a thin tip syringe for low and medium viscosity materials. Otherwise, high viscosity resin was loaded with a metallic spatula. Once the composite was loaded, it was fully situated onto the teeth and gentle pressure around each attachment was then applied with tweezers.
Step 4. Light curing: The composite resin was light-cured according to the composite instructions, selecting the most effective wavelength (400–500 nm). No polishing or finishing procedure was done once the attachment template was removed (
Figure 2).
For this study, three materials were selected with three different levels of viscosity in order to test composites with different viscosities and consistencies: a low-viscosity flowable resin (ENAMEL plus HRi® Flow HF, GDF GmbH), a medium-viscosity orthodontic composite (Bracepaste® Medium Viscosity Adhesive, AO), and a high -viscosity dental restorative material (ENAMEL plus HRi® Enamel, GDF GmbH) (
Table 1). Each step was repeated for each composite resin selected by using one phantom model per time.
2.3. 3D Analysis
Once the attachments were placed, the upper and lower arches of the phantom models were scanned while using a laser light three-dimensional (3D) scanner (D800, 3Shape, Copenaghen, Denmark), with a declared accuracy of 10 μm, and converted in a 3D mesh model (stl). The obtained 3D files of the phantom models were analyzed while using a reverse engineering analysis software (Geomagic Control, 3DS Systems, Rock Hill, South Carolina, USA) by following the previously described protocols to compare the shape between the realized and programmed attachments [
15,
16]. Briefly, the obtained 3D models were superimposed with the ones that were derived from the virtual plan, using a surface-based superimposition. The landmark areas that were selected to achieve the superimposition process were the palatal area and the occlusal teeth surfaces.
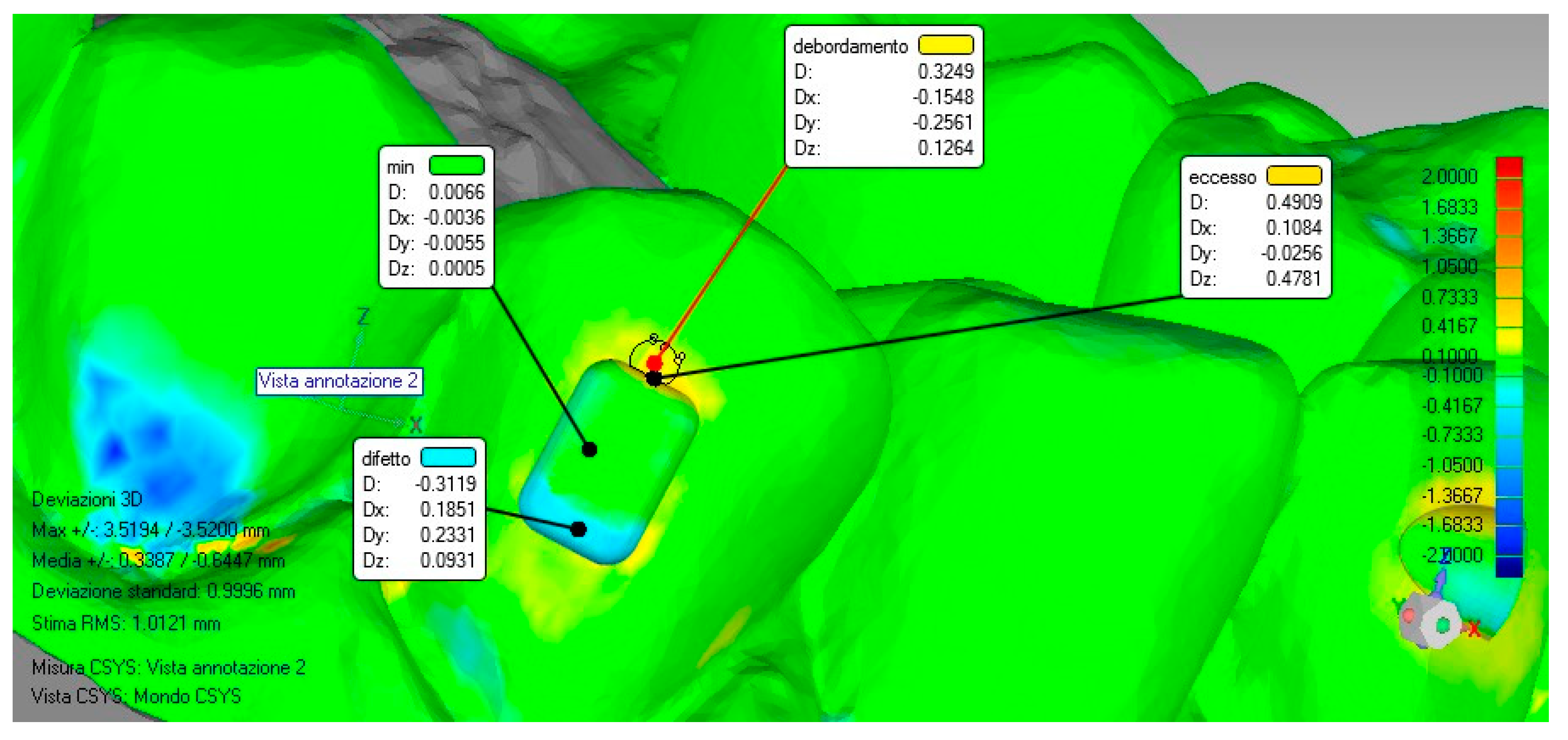
Once the models were superimposed, the virtual planning model was used as a reference and a surface deviation analysis was carried out. The software automatically calculated the linear distances (Euclidean distances) between 100% of the surface of the two superimposed models and then provided a color map that highlighted the lack (blue color) and the excess (red/orange color) areas inside and outside the perimeter of the attachment shape.
For this study, the maximum deviation evaluated was set to ±2 mm and the tolerance range (green color) within the deviation values considered acceptable was set to ±0.1 mm.
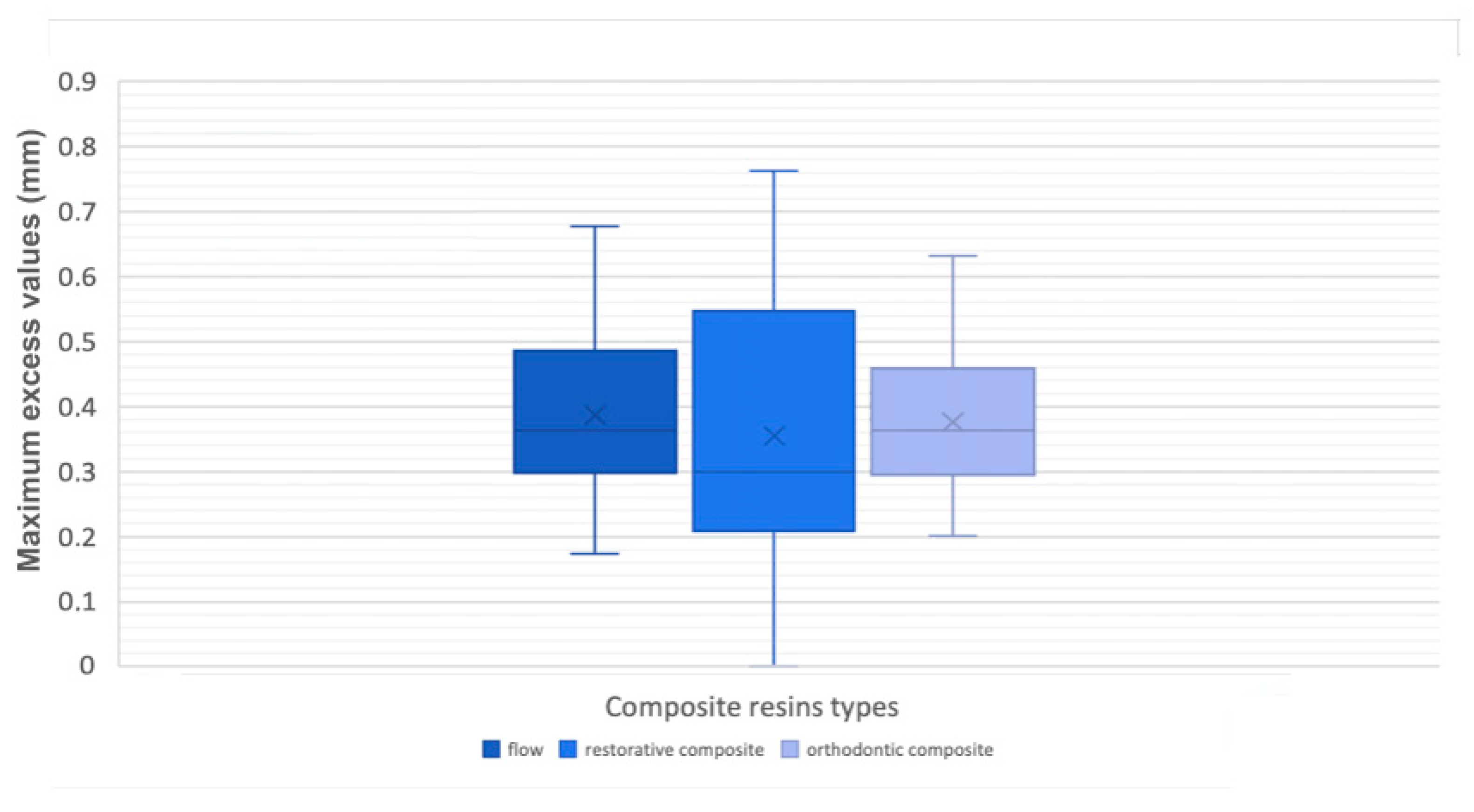
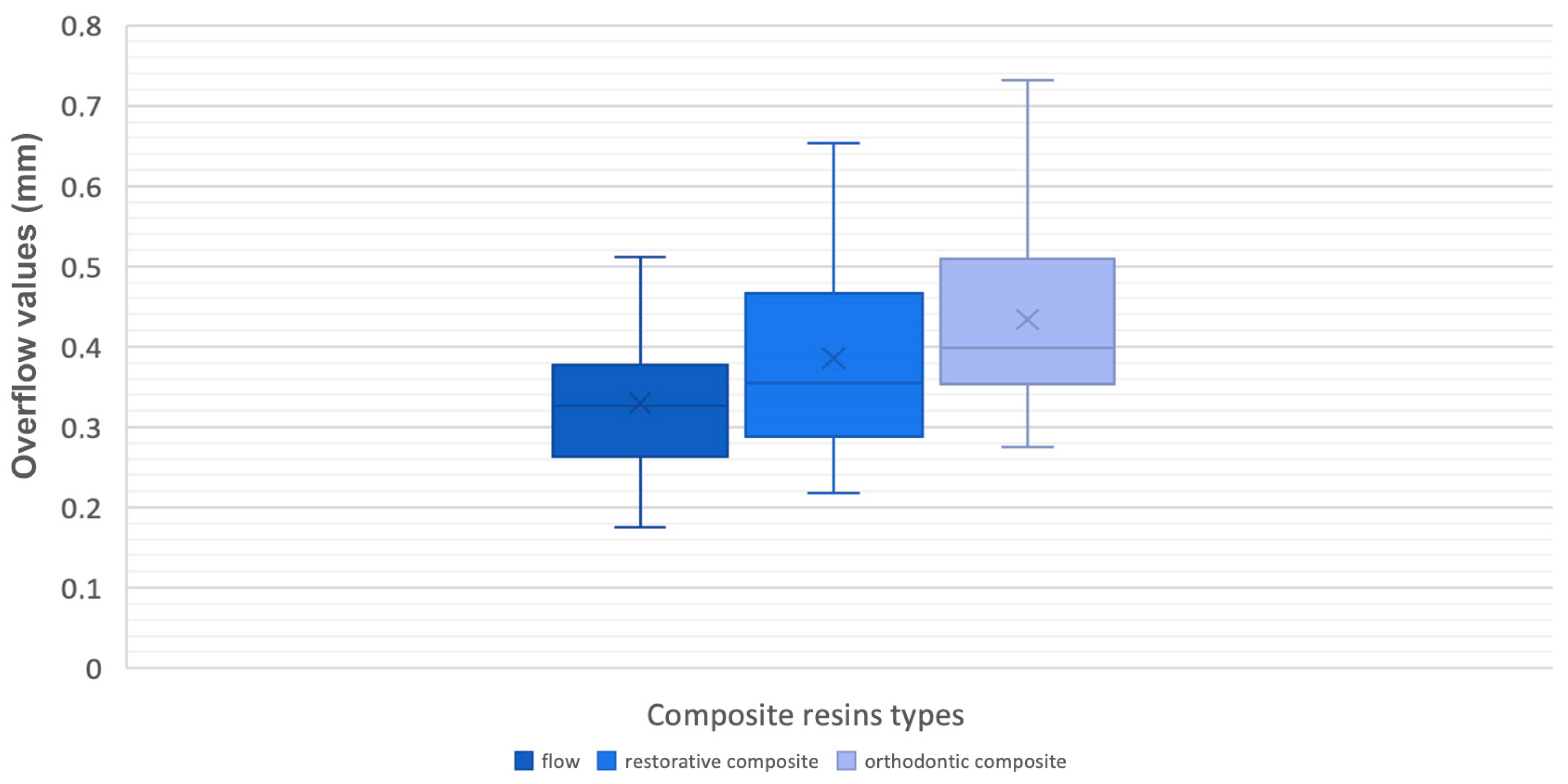
Measurements were carried out at the level of the attachment’s surface to distinguish the maximum value in defect and in excess, inside the perimeter of the attachment shape, and the overflow value outside that perimeter, once this procedure was done for each model; moreover, a minimum value was detected as a control mechanism to consider the accuracy of the alignment between the files (
Figure 3).
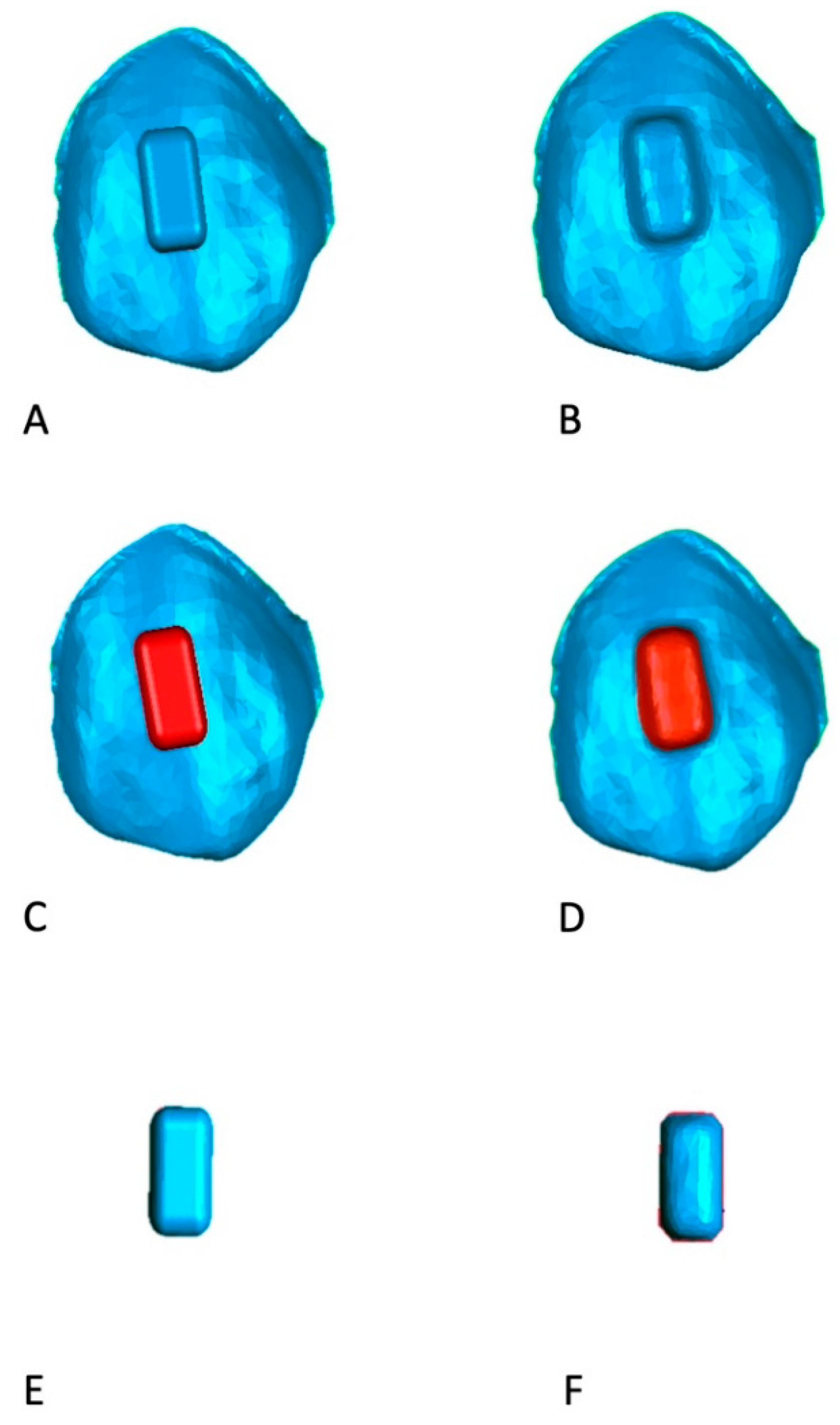
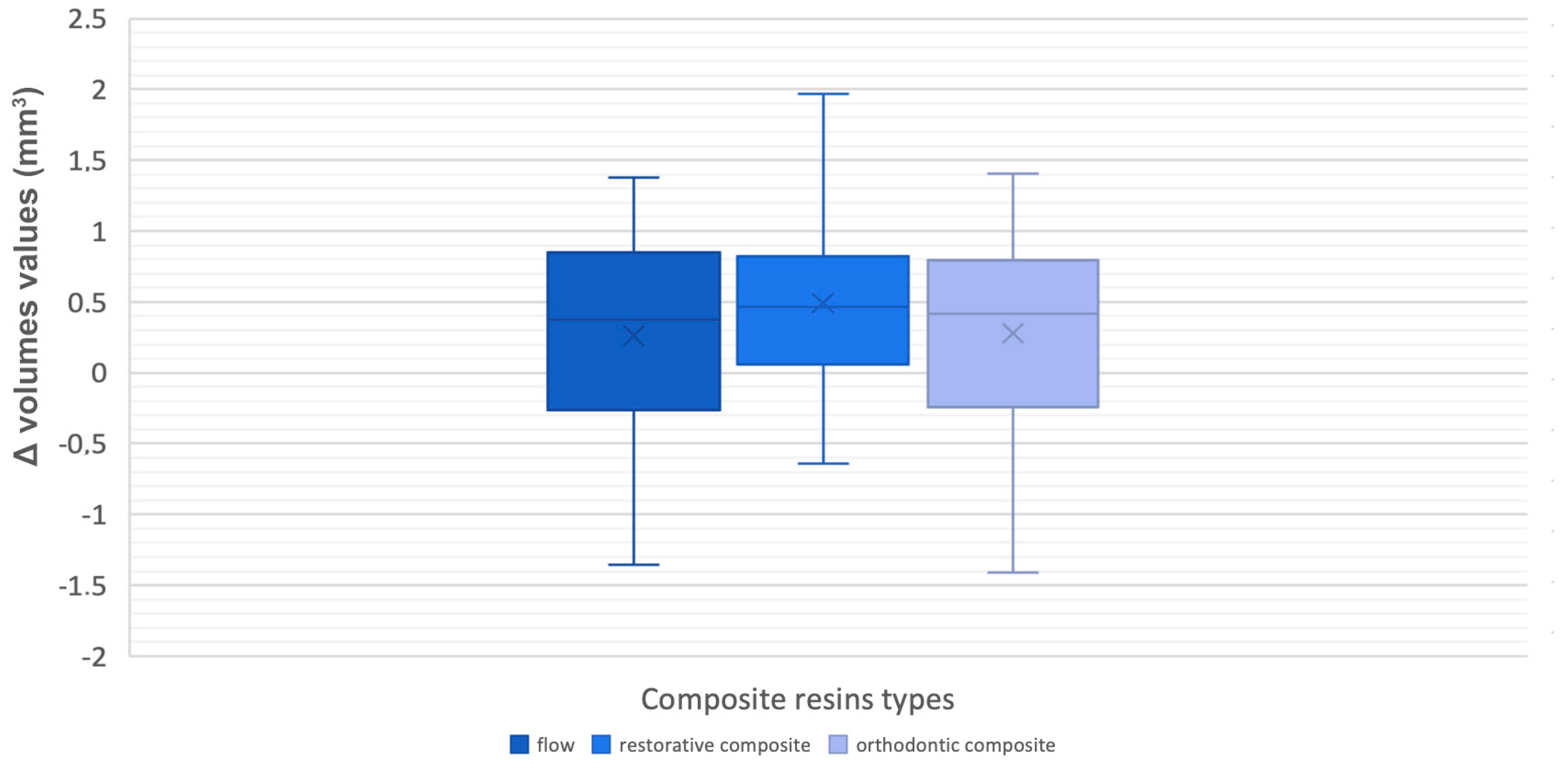
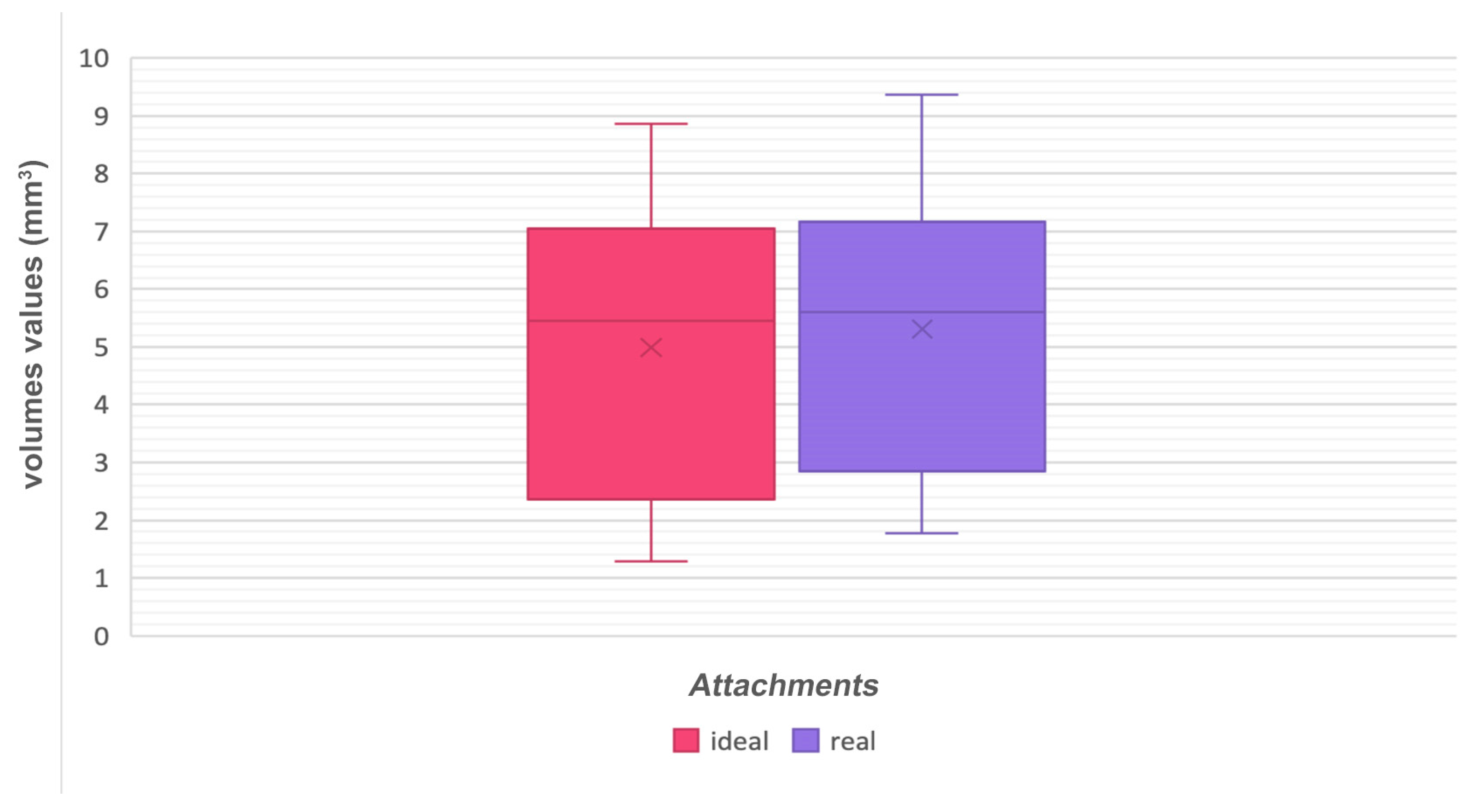
Furthermore, volumetric measurements of auxiliary elements were carried out through Geomagic software (
Figure 4) by segmenting the real and ideal attachments and while using a specific tool of the software in order to assess whether any differences in volumes were present between programmed and realized attachments.

 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}