Q-Switch Nd:YAG Laser-Assisted Elimination of Multi-Species Biofilm on Titanium Surfaces

 , ,
, ,  , ,
, ,  and
and 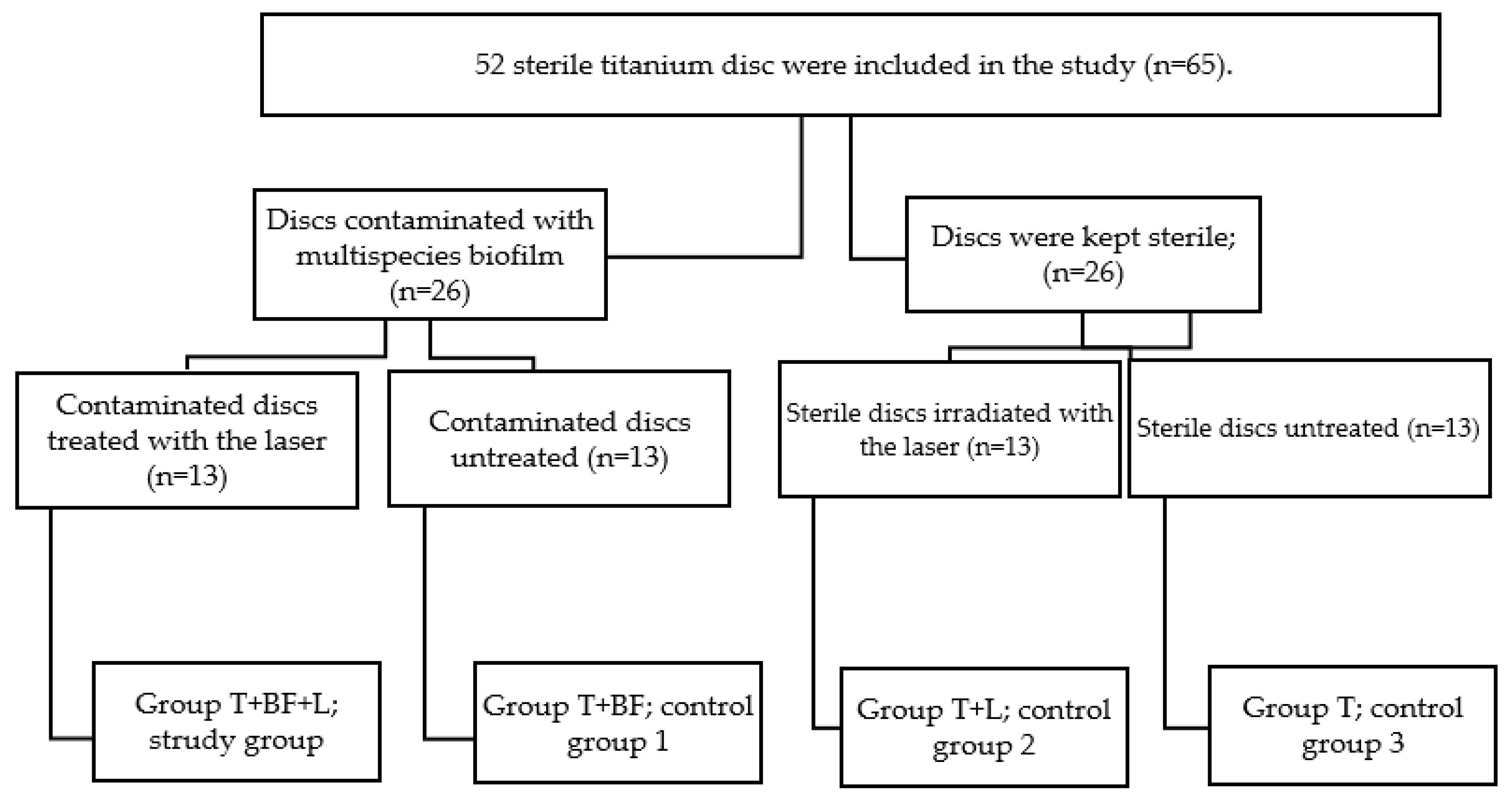{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Design of the Study
2.2. Bacterial Strains, Media, and Growth Conditions
Bioreactor-Derived Multi-Species Community and Multi-Species Biofilms
2.3. Treatment Protocol and Laser Irradiation
2.4. Biofilm Staining with Crystal Violet (CV)
2.5. Statistical and Data Analysis
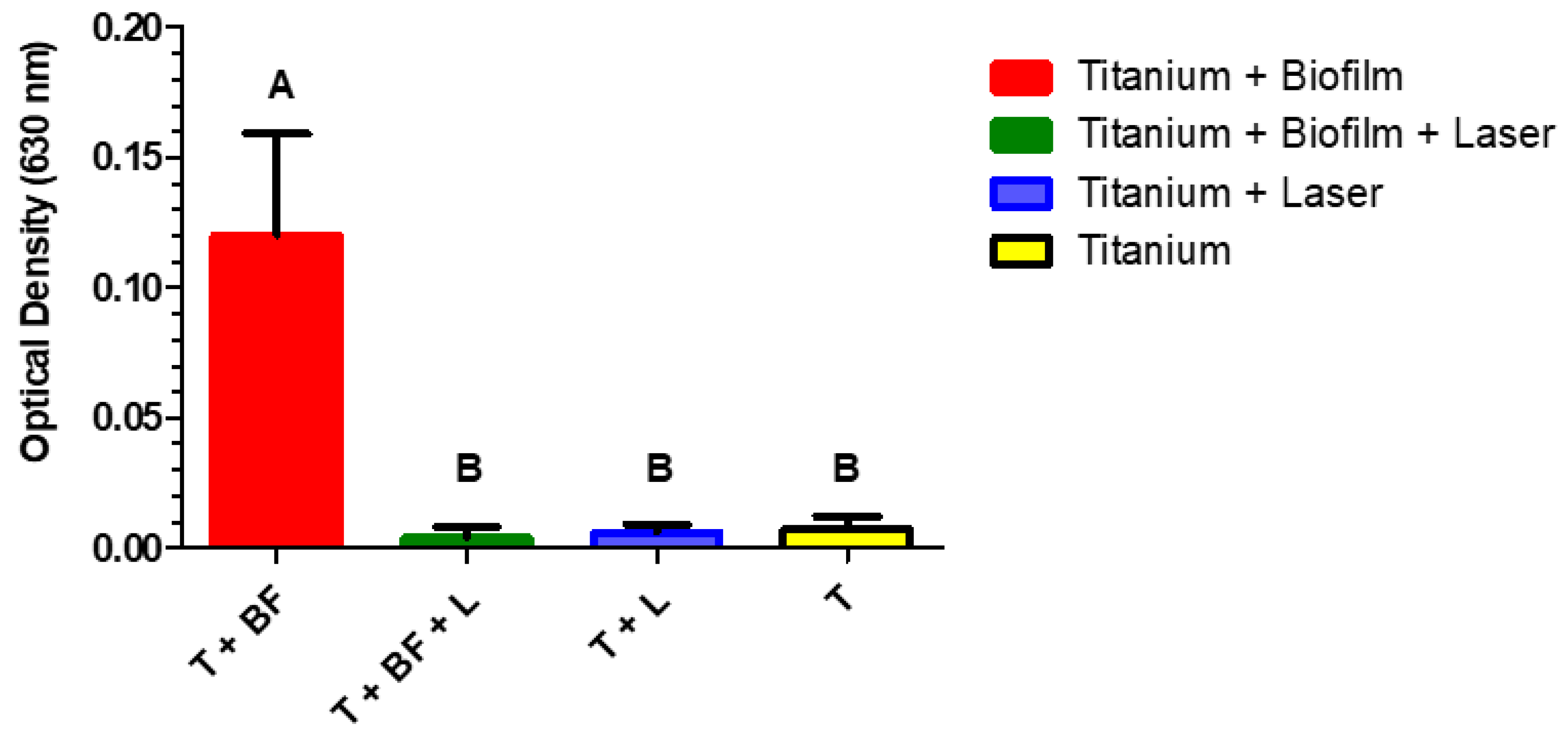
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Levin, L.; Laviv, A.; Schwartz-Arad, D. Long-term success of implants replacing a single molar. J. Periodontol. 2006, 77, 1528–1532. [Google Scholar] [CrossRef]
- Serino, G.; Turri, A.; Lang, N.P. Probing at implants with peri-implantitis and its relation to clinical peri-implant bone loss. Clin. Oral Implant. Res. 2013, 24, 91–95. [Google Scholar] [CrossRef]
- Lang, N.P.; Wilson, T.G.; Corbet, E.F. Biological complications with dental implants: Their prevention, diagnosis and treatment Note. Clin. Oral Implant. Res. Chapter 9 2000, 11, 146–155. [Google Scholar] [CrossRef]
- Schwarz, M.S. Mechanical complications of dental implants. Clin. Oral Implant. Res. Chapter 10 2000, 11, 156–158. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S313–S318. [Google Scholar] [CrossRef]
- Lindhe, J.; Meyle, J.; Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus report of the sixth European workshop on periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [Green Version]
- Renvert, S.; Polyzois, I. Treatment of pathologic peri-implant pockets. Periodontol. 2000 2018, 76, 180–190. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Layton, D.M.; Roccuzzo, A.; Heitz-Mayfield, L.J. Clinical outcomes of peri-implantitis treatment and supportive care: A systematic review. Clin. Oral Implant. Res. 2018, 29, 331–350. [Google Scholar] [CrossRef]
- Wong, R.L.; Hiyari, S.; Yaghsezian, A.; Davar, M.; Lin, Y.-L.; Galvan, M.; Tetradis, S.; Camargo, P.M.; Pirih, F.Q. Comparing the healing potential of late-stage periodontitis and Peri-Implantitis. J. Oral Implantol. 2017, 43, 437–445. [Google Scholar] [CrossRef]
- Varghese, S. Role of interleukin-1 in peri-implantitis. Drug Invent. Today 2018, 10, 3388–3390. [Google Scholar]
- Rakic, M.; Struillou, X.; Petkovic-Curcin, A.; Matic, S.; Canullo, L.; Sanz, M.; Vojvodic, D. Estimation of bone loss biomarkers as a diagnostic tool for peri-implantitis. J. Periodontol. 2014, 85, 1566–1574. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Muraglie, S.; Leonardi, R.; Lo Giudice, A. Assessment of Vitamin C and Antioxidant Profiles in Saliva and Serum in Patients with Periodontitis and Ischemic Heart Disease. Nutrients 2019, 11, 2956. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Zhu, Q.; Gong, J.; Xie, M.; Jiao, T. CyPA and Emmprin play a role in peri-implantitis. Clin. Implant Dent. Relat. Res. 2018, 20, 102–109. [Google Scholar] [CrossRef]
- Bordin, S.; Flemmig, T.F.; Habil, M.D.; Verardi, S. Role of fibroblast populations in peri-implantitis. Int. J. Oral Maxillofac. Implant. 2009, 24, 197–204. [Google Scholar]
- Poli, P.P.; Cicciu, M.; Beretta, M.; Maiorana, C. Peri-implant mucositis and peri-implantitis: A Current understanding of their diagnosis, clinical implications, and a report of treatment using a combined therapy approach. J. Oral Implantol. 2017, 43, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Mettraux, G.R.; Sculean, A.; Bürgin, W.B.; Salvi, G.E. Two-year clinical outcomes following non-surgical mechanical therapy of peri-implantitis with adjunctive diode laser application. Clin. Oral Implant. Res. 2016, 27, 845–849. [Google Scholar] [CrossRef]
- Lin, G.H.; Suárez López del Amo, F.; Wang, H.L. Laser therapy for treatment of peri-implant mucositis and peri-implantitis: An American Academy of Periodontology best evidence review. J. Periodontol. 2018, 89, 766–782. [Google Scholar]
- del Amo, F.S.-L.; Yu, S.-H.; Wang, H.-L. Non-surgical therapy for peri-implant diseases: A systematic review. J. Oral Maxillofac. Res. 2016, 7, e13. [Google Scholar]
- Namour, M.; El Mobadder, M.; Magnin, D.; Peremans, A.; Verspecht, T.; Teughels, W.; Lamard, L.; Nammour, S.; Rompen, E. Q-Switch Nd: YAG Laser-Assisted Decontamination of Implant Surface. Dent. J. 2019, 7, 99. [Google Scholar] [CrossRef] [Green Version]
- Nejem Wakim, R.; Namour, M.; Nguyen, H.V.; Peremans, A.; Zeinoun, T.; Vanheusden, A.; Rompen, E.; Nammour, S. Decontamination of Dental Implant Surfaces by the Er: YAG Laser Beam: A Comparative in Vitro Study of Various Protocols. Dent. J. 2018, 6, 66. [Google Scholar] [CrossRef] [Green Version]
- Slomka, V.; Herrero, E.R.; Boon, N.; Bernaerts, K.; Trivedi, H.M.; Daep, C.; Quirynen, M.; Teughels, W. Oral prebiotics and the influence of environmental conditions in vitro. J. Periodontol. 2018, 89, 708–717. [Google Scholar] [CrossRef]
- Feoktistova, M.; Geserick, P.; Leverkus, M. Crystal violet assay for determining viability of cultured cells. Cold Spring Harb. Protoc. 2016, 2016, pdb. prot087379. [Google Scholar] [CrossRef]
- Olivi, G.; De Moor, R.; DiVito, E. Lasers in Endodontics: Scientific Background and Clinical Applications; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Schoop, U.; Kluger, W.; Dervisbegovic, S.; Goharkhay, K.; Wernisch, J.; Georgopoulos, A.; Sperr, W.; Moritz, A. Innovative wavelengths in endodontic treatment. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 2006, 38, 624–630. [Google Scholar] [CrossRef]
- Richter, L.J.; Buntin, S.A.; King, D.S.; Cavanagh, R.R. State-resolved studies of the laser-induced desorption of NO from Si (111) 7 × 7: Low coverage results. J. Chem. Phys. 1992, 96, 2324–2338. [Google Scholar] [CrossRef]
- Fukutani, K.; Peremans, A.; Mase, K.; Murata, Y. Photo-stimulated desorption of NO from a Pt (001) surface. Surf. Sci. 1993, 283, 158–168. [Google Scholar] [CrossRef]
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37. [Google Scholar] [CrossRef]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-implantitis–onset and pattern of progression. J. Clin. Periodontol. 2016, 43, 383–388. [Google Scholar] [CrossRef]
- Dreyer, H.; Grischke, J.; Tiede, C.; Eberhard, J.; Schweitzer, A.; Toikkanen, S.; Glöckner, S.; Krause, G.; Stiesch, M. Epidemiology and risk factors of peri-implantitis: A systematic review. J. Periodontal Res. 2018, 53, 657–681. [Google Scholar] [CrossRef]
- Stacchi, C.; Berton, F.; Perinetti, G.; Frassetto, A.; Lombardi, T.; Khoury, A.; Andolsek, F.; Di Lenarda, R. Risk factors for peri-implantitis: Effect of history of periodontal disease and smoking habits. A systematic review and meta-analysis. J. Oral Maxillofac. Res. 2016, 7, e3. [Google Scholar] [CrossRef]
- Kim, S.-H.; Park, S.H.; Chang, B.-S.; Lee, S.Y.; Lee, J.-K.; Um, H.-S. Antimicrobial effect of photodynamic therapy using methylene blue and red color diode laser on biofilm attached to sandblasted and acid-etched surface of titanium. Lasers Dent. Sci. 2017, 1, 83–90. [Google Scholar] [CrossRef]
- De Meyer, S.; Meire, M.; Coenye, T.; De Moor, R. Effect of laser-activated irrigation on biofilms in artificial root canals. Int. Endod. J. 2017, 50, 472–479. [Google Scholar] [CrossRef]
- Pommer, B.; Haas, R.; Mailath-Pokorny, G.; Fürhauser, R.; Watzek, G.; Busenlechner, D.; Müller-Kern, M.; Kloodt, C. Periimplantitis treatment: Long-term comparison of laser decontamination and implantoplasty surgery. Implant Dent. 2016, 25, 646–649. [Google Scholar] [CrossRef]
- Parker, S.P. Laser–tissue interaction. In Lasers in Dentistry—Current Concepts; Springer: Berlin/Heidelberg, Germany, 2017; pp. 29–55. [Google Scholar]
- El Mobadder, M.; Namour, A.; Namour, M.; Dib, W.; El Mobadder, W.; Maalouf, E.; Geerts, S.; Zeinoun, T.; Nammour, S. Dentinal Hypersensitivity Treatment Using Diode Laser 980 nm: In Vivo Study. Dent. J. 2019, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Strauss, R.A. Lasers in oral and maxillofacial surgery. Dent. Clin. North Am. 2000, 44, 851–873. [Google Scholar] [CrossRef]
- Grzech-Leśniak, K.; Sculean, A.; Gašpirc, B. Laser reduction of specific microorganisms in the periodontal pocket using Er: YAG and Nd: YAG lasers: A randomized controlled clinical study. Lasers Med Sci. 2018, 33, 1461–1470. [Google Scholar] [CrossRef]
- Salvi, G.E.; Stähli, A.; Schmidt, J.C.; Ramseier, C.A.; Sculean, A.; Walter, C. Adjunctive laser or antimicrobial photodynamic therapy to non-surgical mechanical instrumentation in patients with untreated periodontitis. A systematic review and meta-analysis. J. Clin. Periodontol. 2019. [Google Scholar] [CrossRef]
- Annaji, S.; Sarkar, I.; Rajan, P.; Pai, J.; Malagi, S.; Bharmappa, R.; Kamath, V. Efficacy of photodynamic therapy and lasers as an adjunct to scaling and root planing in the treatment of aggressive periodontitis–A clinical and microbiologic short term study. J. Clin. Diagn. Res. Jcdr 2016, 10, ZC08. [Google Scholar] [CrossRef]
- Mukhopadhyay, M.; Kundu, P.K. Laser assisted conditioning of aluminium oxide grinding wheel using Nd: YAG laser: A review. In Proceedings of the National Conference on Advanced Functional Materials Processing and Manufacturing, CMERI, Durgapur, India, 2–3 February 2017; pp. 63–66. [Google Scholar]
- Al-Hashedi, A.A.; Laurenti, M.; Benhamou, V.; Tamimi, F. Decontamination of titanium implants using physical methods. Clin. Oral Implant. Res. 2017, 28, 1013–1021. [Google Scholar] [CrossRef]
- Wheelis, S.E.; Gindri, I.M.; Valderrama, P.; Wilson, T.G., Jr.; Huang, J.; Rodrigues, D.C. Effects of decontamination solutions on the surface of titanium: Investigation of surface morphology, composition, and roughness. Clin. Oral Implant. Res. 2016, 27, 329–340. [Google Scholar] [CrossRef]
- Wiedmer, D.; Petersen, F.C.; Lönn-Stensrud, J.; Tiainen, H. Antibacterial effect of hydrogen peroxide-titanium dioxide suspensions in the decontamination of rough titanium surfaces. Biofouling 2017, 33, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Htet, M.; Madi, M.; Zakaria, O.; Miyahara, T.; Xin, W.; Lin, Z.; Aoki, K.; Kasugai, S. Decontamination of anodized implant surface with different modalities for peri-implantitis treatment: Lasers and mechanical debridement with citric acid. J. Periodontol. 2016, 87, 953–961. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Alibrandi, A.; Indelicato, F.; Ferlito, S. Analysis of Endothelin-1 concentrations in individuals with periodontitis. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Namour, M.; Verspecht, T.; El Mobadder, M.; Teughels, W.; Peremans, A.; Nammour, S.; Rompen, E. Q-Switch Nd:YAG Laser-Assisted Elimination of Multi-Species Biofilm on Titanium Surfaces. Materials 2020, 13, 1573. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13071573
Namour M, Verspecht T, El Mobadder M, Teughels W, Peremans A, Nammour S, Rompen E. Q-Switch Nd:YAG Laser-Assisted Elimination of Multi-Species Biofilm on Titanium Surfaces. Materials. 2020; 13(7):1573. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13071573
Chicago/Turabian StyleNamour, Melanie, Tim Verspecht, Marwan El Mobadder, Wim Teughels, Andre Peremans, Samir Nammour, and Eric Rompen. 2020. "Q-Switch Nd:YAG Laser-Assisted Elimination of Multi-Species Biofilm on Titanium Surfaces" Materials 13, no. 7: 1573. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13071573