First Human Leucocyte Antigen (HLA) Response and Safety Evaluation of Fibrous Demineralized Bone Matrix in a Critical Size Femoral Defect Model of the Sprague-Dawley Rat

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
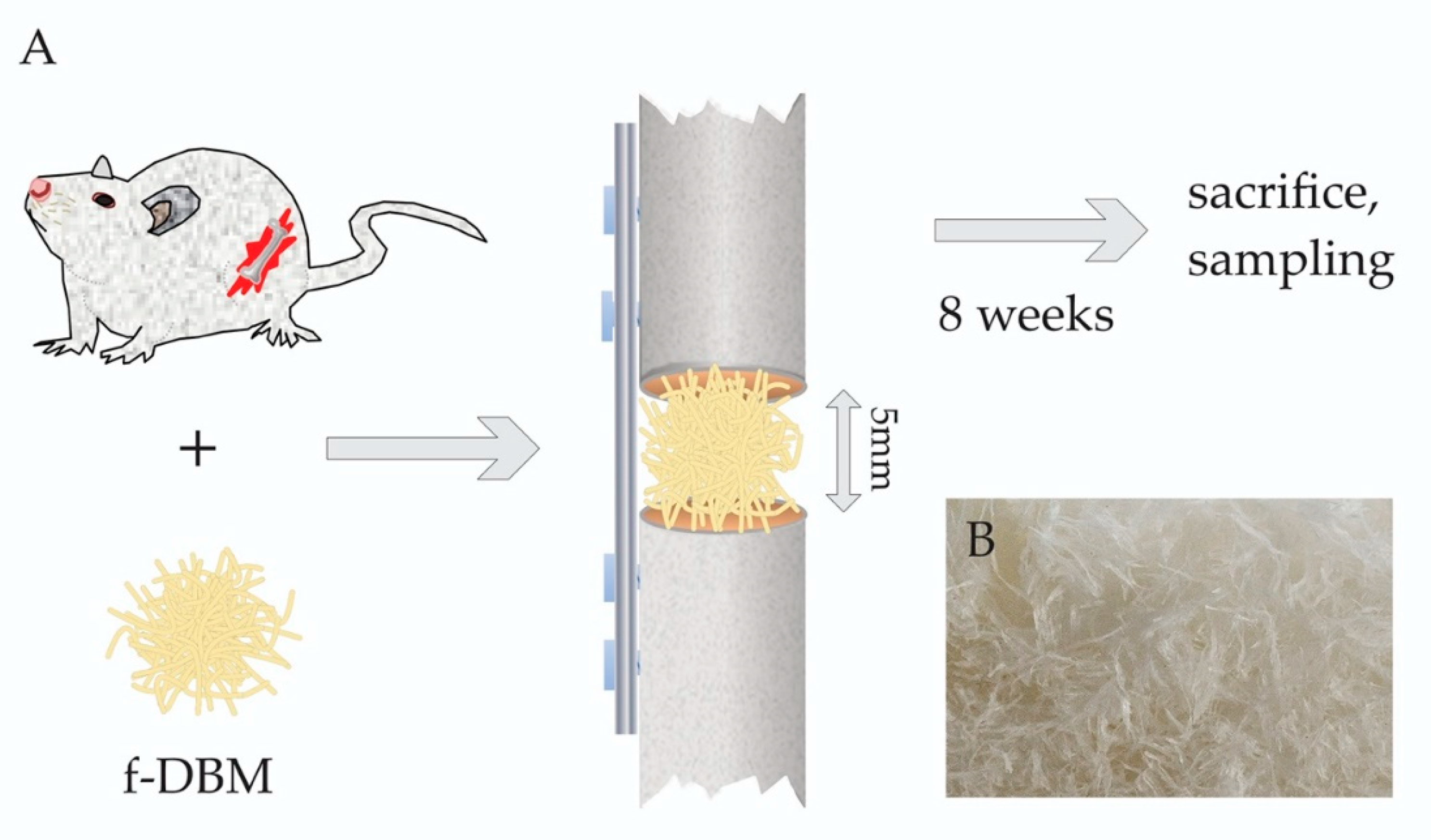
2.1. Preparation of Fibrous Scaffold
2.2. Ethics
2.3. Animal Care and Defect Surgery
2.4. Blood Sampling, Femur and Internal Organ Collection
2.5. Histology
2.6. Bone Healing Score
2.7. Haematological Analysis
2.8. Serum Biochemistry
2.9. HLA Diagnostics
2.10. Statistics
3. Results
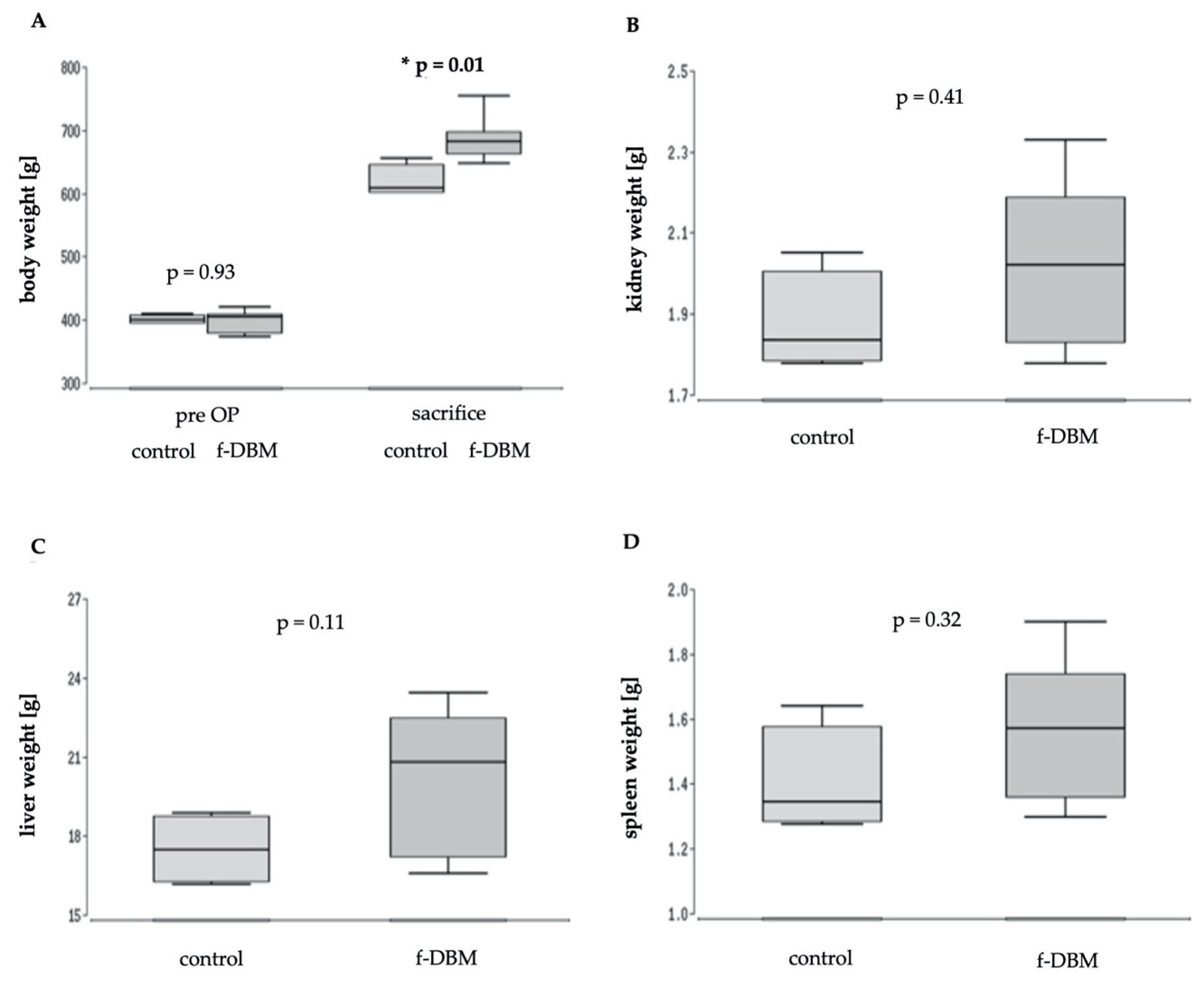
3.1. No Difference in Survival Weight and Organ Function
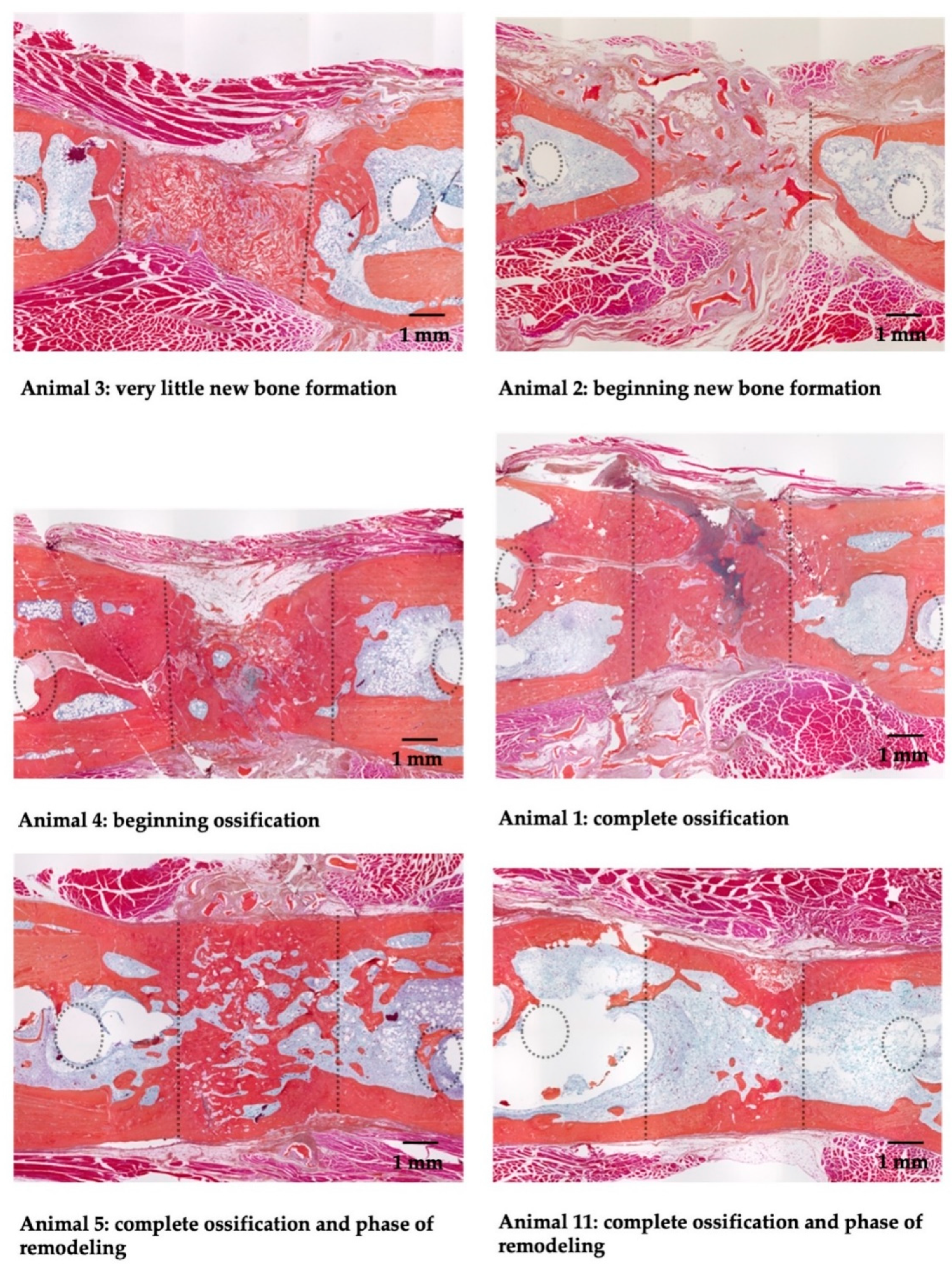
3.2. Histological Responses
Implantation Site
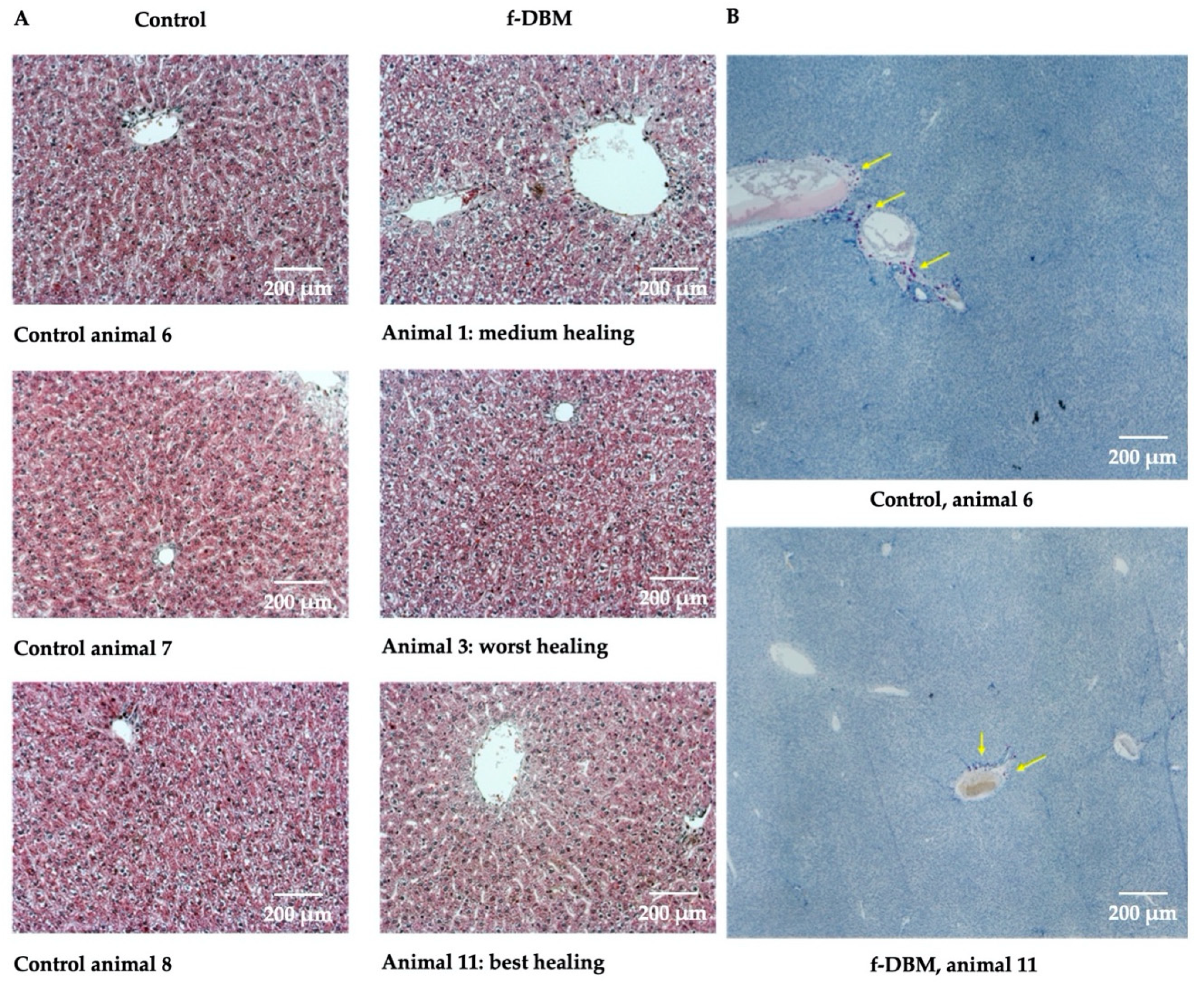
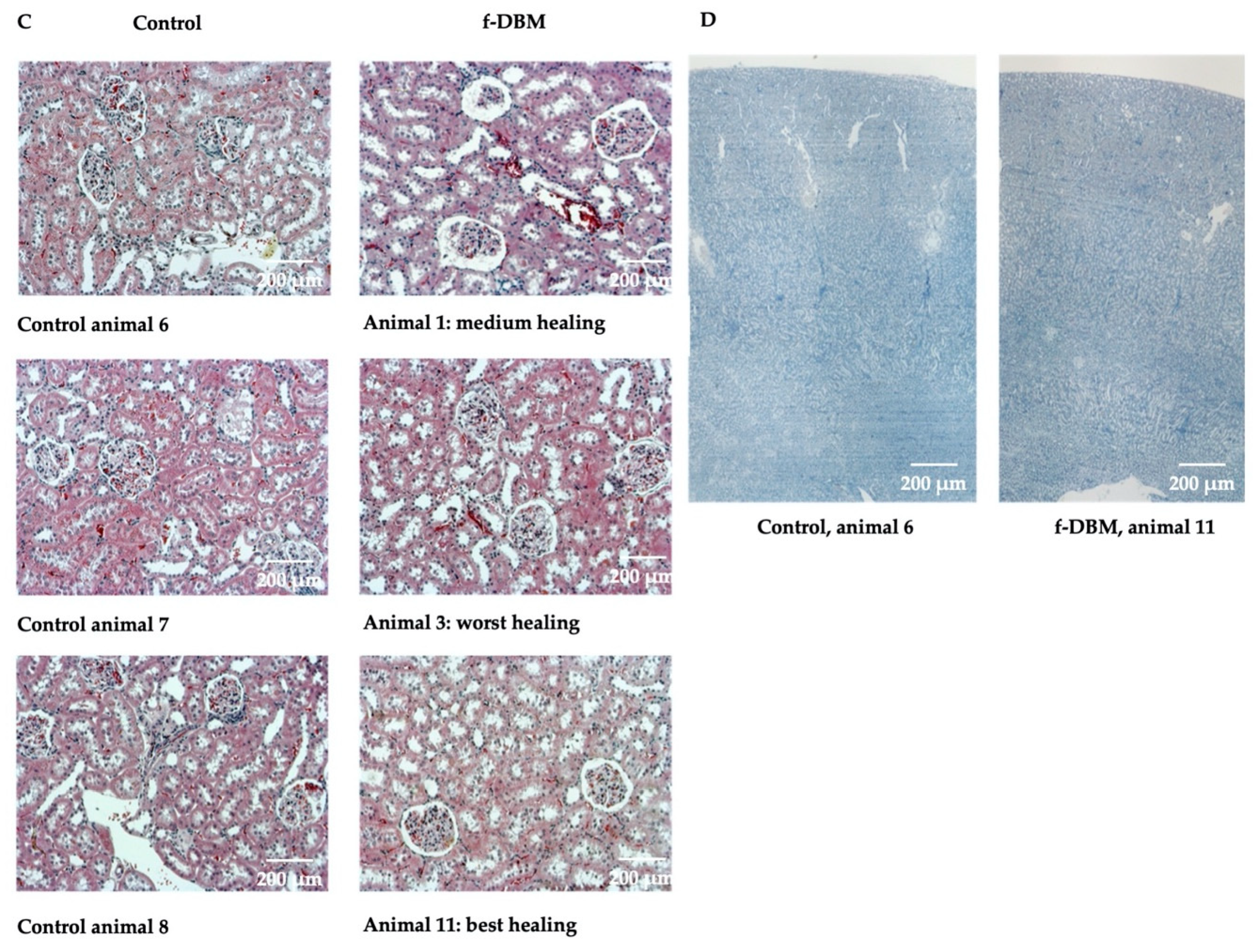
3.3. Liver, Spleen, Kidney
3.4. Hematology
3.5. Serum Biochemistry
3.6. Free Radical Markers
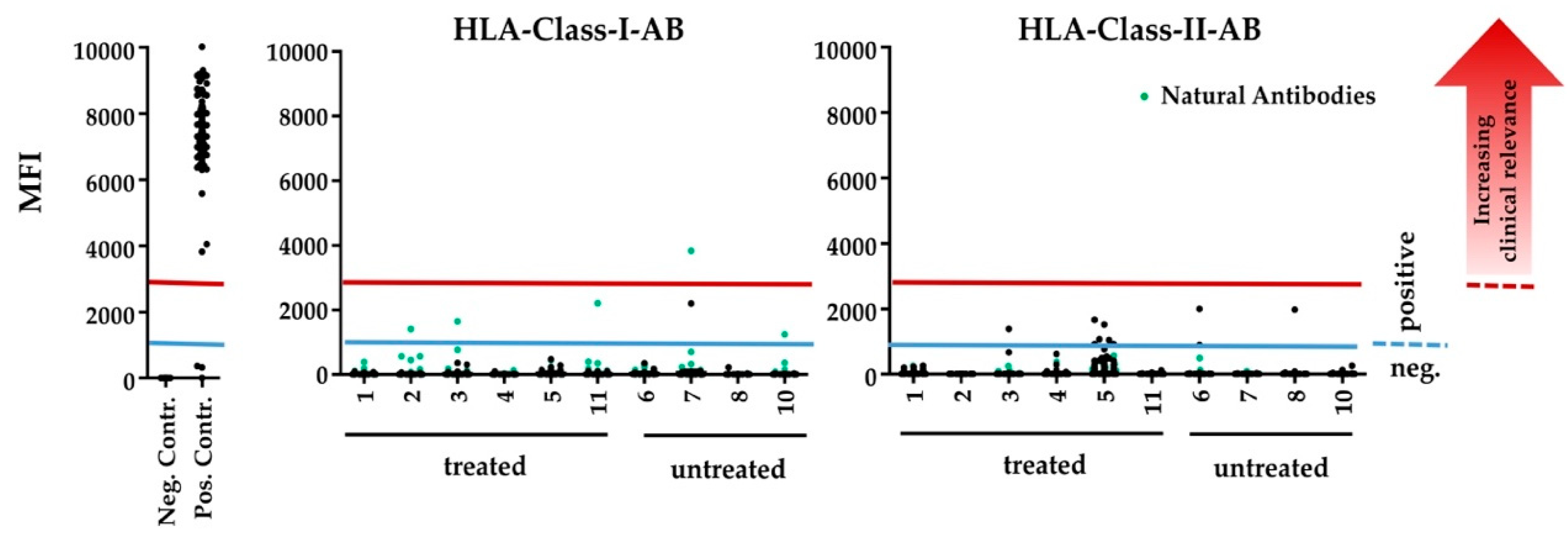
3.7. Human HLA-Antibody Detection
4. Discussion
4.1. Bone Growth
4.2. Biocompatibility, Tumorigenicity and Immunogenicity
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jakoi, A.M.; Iorio, J.A.; Cahill, P.J. Autologous bone graft harvesting: A review of grafts and surgical techniques. Musculoskelet. Surg. 2015, 99, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Goulet, J.A.; Senunas, L.E.; de Silva, G.L.; Greenfield, M.L.V. Autogenous Iliac Crest Bone Graft: Complications and Functional Assessment. Clin. Orthop. Relat. Res. 1997, 339, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Henrich, D.; Verboket, R.R.; Schaible, A.; Kontradowitz, K.; Oppermann, E.; Brune, J.C.; Nau, C.; Meier, S.; Bonig, H.; Marzi, I.; et al. Characterization of bone marrow mononuclear cells on biomaterials for bone tissue engineering in vitro. Biomed. Res. Int. 2015, 762407. [Google Scholar]
- Verboket, R.D.; Herrera-Vizcaíno, C.; Thorwart, K.; Booms, P.; Bellen, M.; Al-Maawi, S.; Sader, R.; Marzi, I.; Henrich, D.; Ghanaati, S. Influence of concentration and preparation of platelet rich fibrin on human bone marrow mononuclear cells (in vitro). Platelets 2018, 30, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Verboket, R.D.; Anbar, B.; Söhling, N.; Kontradowitz, K.; Marzi, I.; Ghanaati, S.; Henrich, D. Changes in platelet-rich fibrin composition after trauma and surgical intervention. Platelets 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Polo-Corrales, L.; Latorre-Esteves, M.; Ramirez-Vick, J.E. Scaffold design for bone regeneration. J. Nanosci. Nanotechnol. 2014, 14, 15–56. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Liu, X.; Yeung, K.W.; Liu, C.; Yang, X. Biomimetic porous scaffolds for bone tissue engineering. Mater. Sci. Eng. R Rep. 2014, 80, 1–36. [Google Scholar] [CrossRef]
- Iwata, H.; Sakano, S.; Itoh, T.; Bauer, T.W. Demineralized Bone Matrix and Native Bone Morphogenetic Protein in Orthopaedic Surgery. Clin. Orthop. Relat. Res. 2002, 395, 99–109. [Google Scholar] [CrossRef]
- Zundler, M. Demineralisierte Knochenmatrix als Alternative zu Autologer Spongiosa bei der Dorsalen Fusion Traumatischer Thorakolumbaler Frakturen und bei Pseudarthrosen. Ph.D. Thesis, Universität Regensburg, Regensburg, Germany, 2015. [Google Scholar]
- McKee, M.D. Management of Segmental Bony Defects: The Role of Osteoconductive Orthobiologics. J. Am. Acad. Orthop. Surg. 2006, 14, S163–S167. [Google Scholar] [CrossRef]
- Glowacki, J. A review of osteoinductive testing methods and sterilization processes for demineralized bone. Cell Tissue Bank. 2005, 6, 3–12. [Google Scholar] [CrossRef]
- Afzali, B.; Lechler, R.; Hernandez-Fuentes, M.P. Allorecognition and the alloresponse: Clinical implications. Tissue Antigens 2007, 69, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Fretwurst, T.; Gad, L.M.; Steinberg, T.; Schmal, H.; Zeiser, R.; Amler, A.-K.; Nelson, K.; Altmann, B. Detection of major histocompatibility complex molecules in processed allogeneic bone blocks for use in alveolar ridge reconstruction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Strong, D.M.; Friedlaender, G.E.; Tomford, W.W.; Springfield, D.S.; Shives, T.C.; Burchardt, H.; Enneking, W.; Mankin, H. Immunologic Responses in Human Recipients of Osseous and Osteochondral Allografts. Clin. Orthop. Relat. Res. 1996, 326, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Gruskin, E.; Doll, B.A.; Futrell, F.W.; Schmitz, J.P.; Hollinger, J.O. Demineralized bone matrix in bone repair: History and use. Adv. Drug Deliv. Rev. 2012, 64, 1063–1077. [Google Scholar] [CrossRef] [PubMed]
- Wildemann, B.; Kadow-Romacker, A.; Haas, N.; Schmidmaier, G. Quantification of various growth factors in different demineralized bone matrix preparations. J. Biomed. Mater. Res. Part A 2007, 81, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Powers, R.M.; Wolfinbarger, L. Effect(s) of the Demineralization Process on the Osteoinductivity of Demineralized Bone Matrix. J. Periodontol. 1997, 68, 1085–1092. [Google Scholar] [CrossRef]
- Katz, J.M.; Nataraj, C.; Jaw, R.; Deigl, E.; Bursac, P. Demineralized bone matrix as an osteoinductive biomaterial and in vitro predictors of its biological potential. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 89, 127–134. [Google Scholar] [CrossRef]
- Weber, F.E. Reconsidering Osteoconduction in the Era of Additive Manufacturing. Tissue Eng. Part B Rev. 2019, 25, 375–386. [Google Scholar] [CrossRef]
- Khan, S.N.; Cammisa, F.P.; Sandhu, H.S.; Diwan, A.; Girardi, F.P.; Lane, J.M. The Biology of Bone Grafting. J. Am. Acad. Orthop. Surg. 2005, 13, 77–86. [Google Scholar] [CrossRef]
- Urist, M.R.; Dawson, E. Intertransverse Process Fusion with the Aid of Chemosterilized Autolyzed Antigen-Extracted Allogeneic (AAA) Bone. Clin. Orthop. Relat. Res. 1981, 154, 97113. [Google Scholar] [CrossRef]
- Guizzardi, S.; di Silvestre, M.; Scandroglio, R.; Ruggeri, A.; Savini, R. Implants of Heterologous Demineralized Bone Matrix for Induction of Posterior Spinal Fusion in Rats. Spine 1992, 17, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Frenkel, S.R.; Moskovich, R.; Spivak, J.; Zhang, Z.H.; Prewett, A.B. Demineralized bone matrix. Enhancement of spinal fusion. Spine 1993, 18, 1634–1639. [Google Scholar] [CrossRef]
- Albert, A.; Leemrijse, T.; Druez, V.; Delloye, C.; Cornu, O. Are bone autografts still necessary in 2006? A three-year retrospective study of bone grafting. Acta Orthop. Belg. 2006, 72, 734–740. [Google Scholar] [PubMed]
- Stumbras, A.; Kuliesius, P.; Januzis, G.; Juodzbalys, G. Alveolar Ridge Preservation after Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet Concentrates: A Systematic Review. J. Oral Maxillofac. Res. 2019, 10, e2. [Google Scholar] [CrossRef] [PubMed]
- Baumann, F.; Krutsch, W.; Pfeifer, C.; Neumann, C.; Nerlich, M.; Loibl, M. Posterolateral fusion in acute traumatic thoracolumbar fractures: A comparison of demineralized bone matrix and autologous bone graft. Acta Chir. Orthop. Traumatol. 2015, 82, 119–125. [Google Scholar]
- Zadegan, S.A.; Abedi, A.; Jazayeri, S.B.; Vaccaro, A.R.; Rahimi-Movaghar, V. Demineralized bone matrix in anterior cervical discectomy and fusion: A systematic review. Eur. Spine J. 2016, 26, 958–974. [Google Scholar] [CrossRef]
- Horváthy, D.B.; Vácz, G.; Toró, I.; Szabó, T.; May, Z.; Duarte, M.; Hornyák, I.; Szabó, B.T.; Dobó-Nagy, C.; Doros, A.; et al. Remineralization of demineralized bone matrix in critical size cranial defects in rats: A 6-month follow-up study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2015, 104, 1336–1342. [Google Scholar] [CrossRef]
- Janko, M.; Sahm, J.; Schaible, A.; Brune, J.C.; Bellen, M.; Schröder, K.; Seebach, C.; Marzi, I.; Henrich, D. Comparison of three different types of scaffolds preseeded with human bone marrow mononuclear cells on the bone healing in a femoral critical size defect model of the athymic rat. J. Tissue Eng. Regen. Med. 2017, 12, 653–666. [Google Scholar] [CrossRef]
- Pruß, A.; Göbel, U.B.; Pauli, G.; Kao, M.; Seibold, M.; Mönig, H.-J.; Hansen, A.; von Versen, R. Peracetic acid-ethanol treatment of allogeneic avital bone tissue transplants a reliable sterilization method. Ann. Transplant. 2003, 8, 34–42. [Google Scholar]
- Drosse, I.; Volkmer, E.; Seitz, S.; Seitz, H.; Penzkofer, R.; Zahn, K.; Matis, U.; Mutschler, W.; Augat, P.; Schieker, M. Validation of a Femoral Critical Size Defect Model for Orthotopic Evaluation of Bone Healing: A Biomechanical, Veterinary and Trauma Surgical Perspective. Tissue Eng. Part C Methods 2008, 14, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Nowalk, J.R.; Flick, L.M. Visualization of different tissues involved in endochondral ossification with alcian blue hematoxylin and orange G/eosin counterstain. J. Histotechnol. 2008, 31, 19–21. [Google Scholar] [CrossRef]
- Han, Z.; Bhavsar, M.; Leppik, L.P.; Oliveira, K.M.C.; Barker, J.H. Histological Scoring Method to Assess Bone Healing in Critical Size Bone Defect Models. Tissue Eng. Part C Methods 2018, 24, 272–279. [Google Scholar] [CrossRef]
- Delwatta, S.L.; Gunatilake, M.; Baumans, V.; Seneviratne, M.D.; Dissanayaka, M.L.B.; Batagoda, S.S.; Udagedara, A.H.; Walpola, P.B. Reference values for selected hematological, biochemical and physiological parameters of Sprague-Dawley rats at the Animal House, Faculty of Medicine, University of Colombo, Sri Lanka. Anim. Model. Exp. Med. 2018, 1, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Morales-Buenrostro, L.E.; Terasaki, P.I.; Marino-Vázquez, L.A.; Lee, J.-H.; El-Awar, N.; Alberú, J. “Natural” Human Leukocyte Antigen Antibodies Found in Nonalloimmunized Healthy Males. Transplantation 2008, 86, 1111–1115. [Google Scholar] [CrossRef]
- Stancoven, B.W.; Lee, J.; Dixon, D.R.; McPherson, J.; Bisch, F.C.; Wikesjö, U.M.E.; Susin, C. Effect of bone morphogenetic protein-2, demineralized bone matrix and systemic parathyroid hormone (1-34) on local bone formation in a rat calvaria critical-size defect model. J. Periodont. Res. 2012, 48, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Aghdasi, B.; Montgomery, S.; Daubs, M.; Wang, J. A review of demineralized bone matrices for spinal fusion: The evidence for efficacy. Surgeon 2013, 11, 39–48. [Google Scholar] [CrossRef]
- Huber, E.; Pobloth, A.-M.; Bormann, N.; Kolarczik, N.; Schmidt-Bleek, K.; Schell, H.; Schwabe, P.; Duda, G.N.; Wildemann, B. Demineralized Bone Matrix as a Carrier for Bone Morphogenetic Protein-2: Burst Release Combined with Long-Term Binding and Osteoinductive Activity Evaluated In Vitro and In Vivo. Tissue Eng. Part A 2017, 23, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Loi, F.; Córdova, L.A.; Pajarinen, J.; Lin, T.; Yao, Z.; Goodman, S.B. Inflammation, fracture and bone repair. Bone 2016, 86, 119–130. [Google Scholar] [CrossRef] [Green Version]
- Kong, Z.; Li, J.; Zhao, Q.; Zhou, Z.; Yuan, X.; Yang, D.; Chen, X. Dynamic compression promotes proliferation and neovascular networks of endothelial progenitor cells in demineralized bone matrix scaffold seed. J. Appl. Physiol. 2012, 113, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Verboket, R.D.; Leiblein, M.; Seebach, C.; Nau, C.; Janko, M.; Bellen, M.; Bonig, H.; Henrich, D.; Marzi, I. Autologous cell-based therapy for treatment of large bone defects: From bench to bedside. Eur. J. Trauma Emerg. Surg. 2018, 44, 649–665. [Google Scholar] [CrossRef] [Green Version]
- Verboket, R.D.; Leiblein, M.; Janko, M.; Schaible, A.; Brune, J.C.; Schröder, K.; Heilani, M.; Fremdling, C.; Busche, Y.; Irrle, T.; et al. From two stages to one: Acceleration of the induced membrane (Masquelet) technique using human acellular dermis for the treatment of non-infectious large bone defects. Eur. J. Trauma Emerg. Surg. 2020, 46, 317–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janko, M.; Pöllinger, S.; Schaible, A.; Bellen, M.; Schröder, K.; Heilani, M.; Fremdling, C.; Marzi, I.; Nau, C.; Henrich, D.; et al. Determination of the effective dose of bone marrow mononuclear cell therapy for bone healing in vivo. Eur. J. Trauma Emerg. Surg. 2020, 46, 265–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Lv, Y. Reconstructing Bone with Natural Bone Graft: A Review of In Vivo Studies in Bone Defect Animal Model. Nanomaterials 2018, 8, 999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Grado, G.F.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.-M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone substitutes: A review of their characteristics, clinical use, and perspectives for large bone defects management. J. Tissue Eng. 2018, 9, 9. [Google Scholar] [CrossRef] [Green Version]
- Faßbender, M.; Minkwitz, S.; Thiele, M.; Wildemann, B. Efficacy of two different demineralised bone matrix grafts to promote bone healing in a critical-size-defect: A radiological, histological and histomorphometric study in rat femurs. Int. Orthop. 2014, 38, 1963–1969. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; McBride, S.; Dean, D.D.; Sylvia, V.L.; Doll, B.A.; O Hollinger, J. In vivo performance of combinations of autograft, demineralized bone matrix, and tricalcium phosphate in a rabbit femoral defect model. Biomed. Mater. 2014, 9, 35010. [Google Scholar] [CrossRef]
- Schmidt-Bleek, K.; Schell, H.; Schulz, N.; Hoff, P.; Perka, C.; Buttgereit, F.; Volk, H.-D.; Lienau, J.; Duda, G.N. Inflammatory phase of bone healing initiates the regenerative healing cascade. Cell Tiss. Res. 2011, 347, 567–573. [Google Scholar] [CrossRef]
- Schmidt-Bleek, K.; Schell, H.; Lienau, J.; Schulz, N.; Hoff, P.; Pfaff, M.; Schmidt, G.; Martin, C.; Perka, C.; Buttgereit, F.; et al. Initial immune reaction and angiogenesis in bone healing. J. Tiss. Eng. Regen. Med. 2012, 8, 120–130. [Google Scholar] [CrossRef]
- Schouten, C.C.; Hartman, E.H.M.; Spauwen, P.H.M.; Jansen, J.A. DBM induced ectopic bone formation in the rat: The importance of surface area. J. Mater. Sci. Mater. Electron. 2005, 16, 149–152. [Google Scholar] [CrossRef]
- Li, G.; Li, P.; Chen, Q.; Thu, H.E.; Hussain, Z. Current Updates on Bone Grafting Biomaterials and Recombinant Human Growth Factors Implanted Biotherapy for Spinal Fusion: A Review of Human Clinical Studies. Curr. Drug Deliv. 2018, 16, 94–110. [Google Scholar] [CrossRef]
- Gazdag, A.R.; Lane, J.M.; Glaser, D.; Forster, R.A. Alternatives to Autogenous Bone Graft: Efficacy and Indications. J. Am. Acad. Orthop. Surg. 1995, 3, 1–8. [Google Scholar] [CrossRef]
- Jirkof, P. Side effects of pain and analgesia in animal experimentation. Lab Anim. 2017, 46, 123–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, A.K.; Hannah, E.; Honeywell, A.C.S.; Pedersen, S. The composition of normal rat blood. J. Biol. Chem. 1930, 86, 157–160. [Google Scholar]
- Eldesoqi, K.; Henrich, D.; El-Kady, A.M.; Arbid, M.; el Hady, B.A.; Marzi, I.; Seebach, C. Safety Evaluation of a Bioglass–Polylactic Acid Composite Scaffold Seeded with Progenitor Cells in a Rat Skull Critical-Size Bone Defect. PLoS ONE 2014, 9, e87642. [Google Scholar] [CrossRef]
- Lee, Y.-P.; Jo, M.; Luna, M.; Chien, B.; Lieberman, J.R.; Wang, J.C. The Efficacy of Different Commercially Available Demineralized Bone Matrix Substances in an Athymic Rat Model. J. Spinal Disord. Tech. 2005, 18, 439–444. [Google Scholar] [CrossRef]
- Drosos, G.I.; Kazakos, K.I.; Kouzoumpasis, P.; Verettas, D.-A. Safety and efficacy of commercially available demineralised bone matrix preparations: A critical review of clinical studies. Injury 2007, 38, S13–S21. [Google Scholar] [CrossRef]
- Sampath, T.K.; Reddi, A.H. Homology of bone-inductive proteins from human, monkey, bovine, and rat extracellular matrix. Proc. Natl. Acad. Sci. USA 1983, 80, 6591–6595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Xu, Z.; Yu, R.; Wang, J.; Wang, Z.; Harrell, C.R. The Use of Type I and Type III Injectable Human Collagen for Dermal Fill: 10 Years of Clinical Experience in China. Semin. Plast. Surg. 2005, 19, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Süsal, C.; Seidl, C.; Schönemann, C.; Heinemann, F.M.; Kauke, T.; Gombos, P.; Kelsch, R.; Arns, W.; Bauerfeind, U.; Hallensleben, M.; et al. Determination of unacceptable HLA antigen mismatches in kidney transplant recipients: Recommendations of the German Society for Immunogenetics. Tiss. Antigens 2015, 86, 317–323. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Bone Healing Score |
|---|---|
| 1 | 28 |
| 2 | 14 |
| 3 | 12 |
| 4 | 20 |
| 5 | 37 |
| 11 | 33 |
| Haematological Marker | Control (Median) | f-DBM (Median) | Statistics | Standard Range |
|---|---|---|---|---|
| Erythrocytes [cells/pL] | 6.4 | 6.3 | p = 0.26 | 3.8–6.7 |
| Hemoglobin [g/dL] | 15.6 | 15.8 | p = 0.9 | 10.4–16.5 |
| White blood cells [cells/nL] | 13.35 | 12.85 | p = 0.71 | 4.4–14.8 |
| Lymphocytes [%] | 85.5 | 81.3 | p = 0.03 | 61–86 |
| Neutrophiles [%] | 13.4 | 16.6 | p = 0.03 | 13–36 |
| Monocytes [%] | 0.94 | 0.98 | p = 0.71 | 0–1 |
| Blood Serum Marker | Control (Median) | f-DBM (Median) | Statistics | Standard Range |
|---|---|---|---|---|
| Creatine [mg/dL] | 0.37 | 0.46 | p = 0.47 | 0.2–0.8 |
| Urea [mg/dL] | 39 | 36.5 | p = 0.48 | 32–53 |
| Protein [g/dL] | 5.4 | 6.5 | p = 0.04 | 5.6–7.6 |
| Glucose [mg/dL] | 294 | 245 | p = 0.07 | 62–202 * |
| GOT/AST [U/L] | 155 | 192 | p = 0.35 | 0.2–838 |
| GPT/ALT [U/L] | 39 | 38 | p = 0.26 | 1–223 |
| ALP [U/L] | 156 | 148 | p = 0.91 | 160–838 |
| Free Radical Marker | Control (Median) | f-DBM (Median) | Statistics |
|---|---|---|---|
| SOD [U/mL] | 0.29 | 0.27 | p = 0.47 |
| MDA [µmol/L] | 10.59 | 10.1 | p = 0.48 |
| GSH [µmol/L] | 12.62 | 19.56 | p = 0.25 |
| Nitrate/Nitrite [µmol/L] | 22.6 | 34.61 | p = 0.26 |
| ID | Treatment | Anti HLA Class I [MFI] | Anti HLA Class II [MFI] |
|---|---|---|---|
| 6 | control | neg | DQ5 (DQB1*05:01) [1993] |
| 7 | control | A80 [3831]; Cw12 [2196] | neg |
| 8 | control | neg | DQA1*03:03 [1973] |
| 10 | control | A11 (A*11:02) [1239] | neg |
| 1 | f-DBM | neg | neg |
| 2 | f-DBM | A23 [1414] | neg |
| 3 | f-DBM | A30 (A*30:01) [1643] | DP13 [1387] |
| 4 | f-DBM | neg | neg |
| 5 | f-DBM | neg | DR4 (DRB1*04:05) [1662]; DR14 (DRB1*14:01 *14:54) [1516]; DQ2 [1066] |
| 11 | f-DBM | A43 [2209] | neg |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Söhling, N.; Leiblein, M.; Schaible, A.; Janko, M.; Schwäble, J.; Seidl, C.; Brune, J.C.; Nau, C.; Marzi, I.; Henrich, D.; et al. First Human Leucocyte Antigen (HLA) Response and Safety Evaluation of Fibrous Demineralized Bone Matrix in a Critical Size Femoral Defect Model of the Sprague-Dawley Rat. Materials 2020, 13, 3120. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13143120
Söhling N, Leiblein M, Schaible A, Janko M, Schwäble J, Seidl C, Brune JC, Nau C, Marzi I, Henrich D, et al. First Human Leucocyte Antigen (HLA) Response and Safety Evaluation of Fibrous Demineralized Bone Matrix in a Critical Size Femoral Defect Model of the Sprague-Dawley Rat. Materials. 2020; 13(14):3120. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13143120
Chicago/Turabian StyleSöhling, Nicolas, Maximilian Leiblein, Alexander Schaible, Maren Janko, Joachim Schwäble, Christian Seidl, Jan C. Brune, Christoph Nau, Ingo Marzi, Dirk Henrich, and et al. 2020. "First Human Leucocyte Antigen (HLA) Response and Safety Evaluation of Fibrous Demineralized Bone Matrix in a Critical Size Femoral Defect Model of the Sprague-Dawley Rat" Materials 13, no. 14: 3120. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13143120