
Calcium Phosphate Modified with Silicon vs. Bovine Hydroxyapatite for Alveolar Ridge Preservation: Densitometric Evaluation, Morphological Changes and Histomorphometric Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.1.1. Inclusion Criteria
- Patients aged over 18 years.
- Patients with uniradicular or biradicular teeth requiring bilateral extraction for various reasons (caries, trauma, crown fracture, root fracture, etc.).
2.1.2. Exclusion Criteria
- Smokers.
- Upper molars, lower molars, and lower incisors were excluded.
- Patients presenting cortical defects in the alveolus, whether pre-operative or as a result of dental extraction.
- Presence of acute or chronic alveolar infection.
- Patients with calcium disorders or immunodeprived patients.
- Patients in treatment by bisphosphonates (oral or injected), corticosteroids, immunosuppressants, radiotherapy, or drugs that would interfere with calcium metabolism.
2.2. Bone Graft Biomaterials Tested
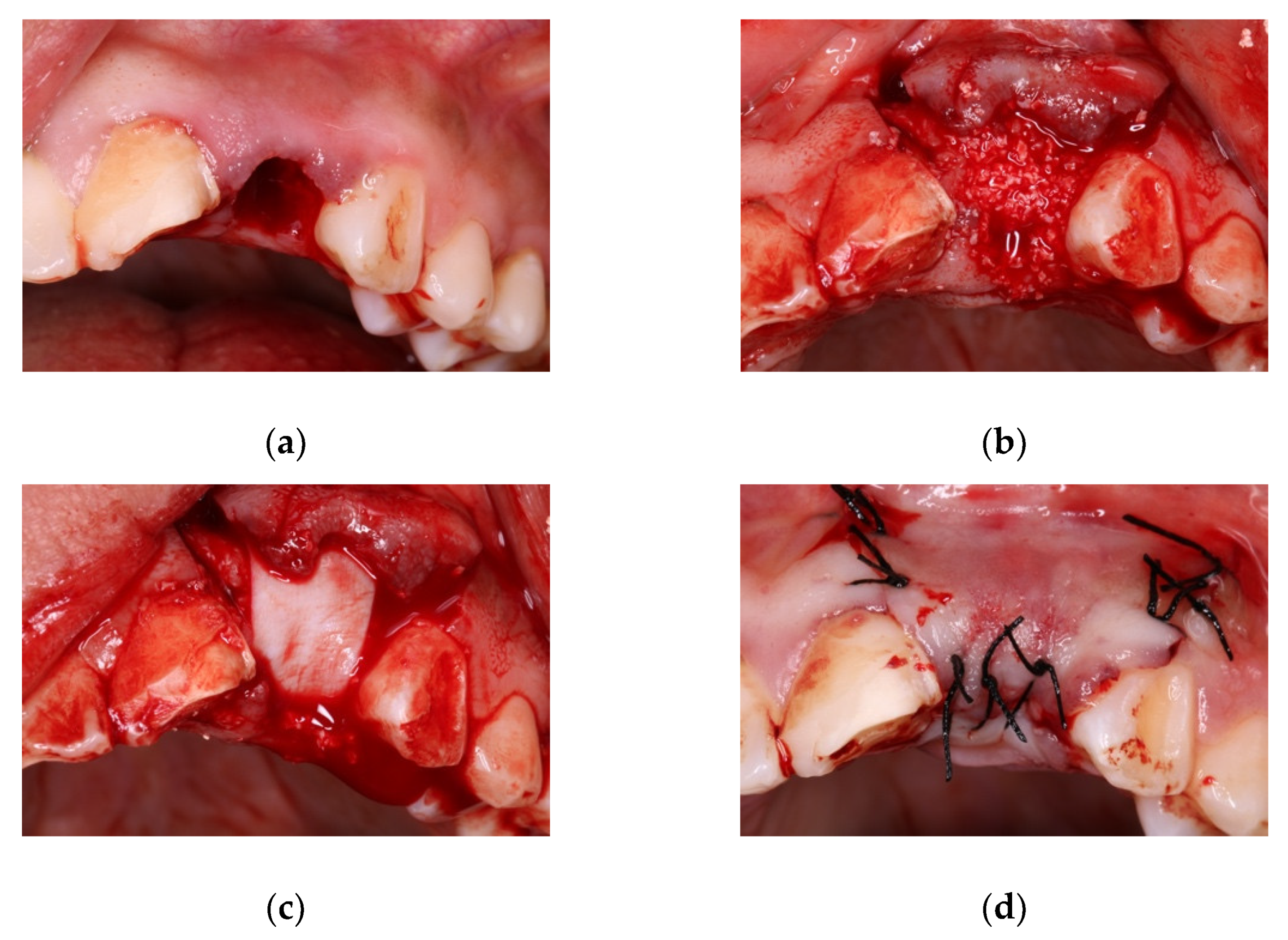
2.3. Alveolar Preservation Surgery
2.4. Evaluation of Outcomes
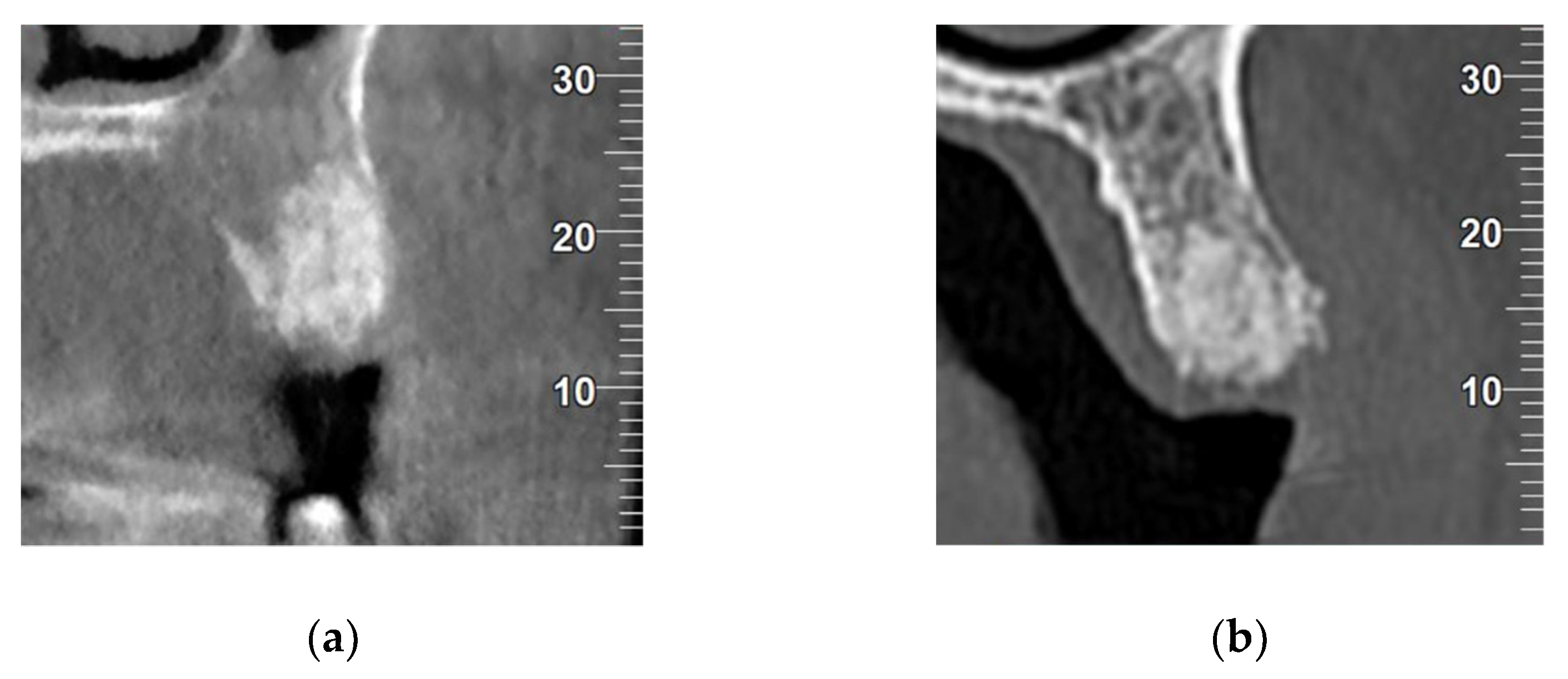
2.4.1. Densitometric Analysis
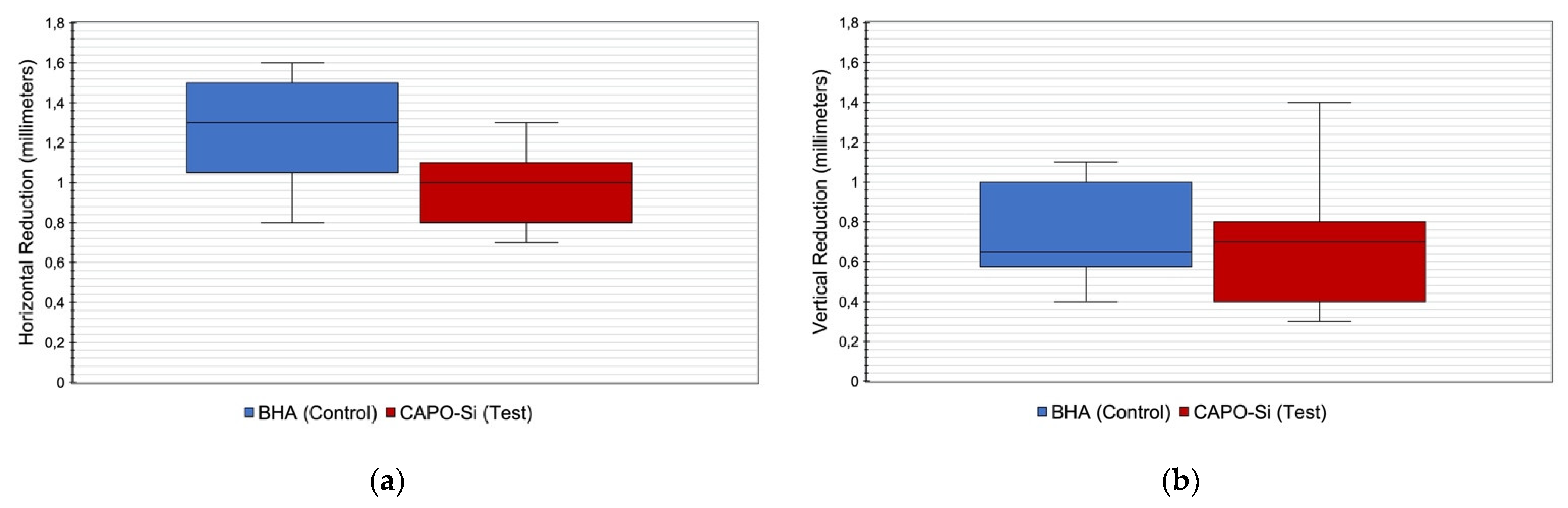
2.4.2. Analysis of Bone Loss
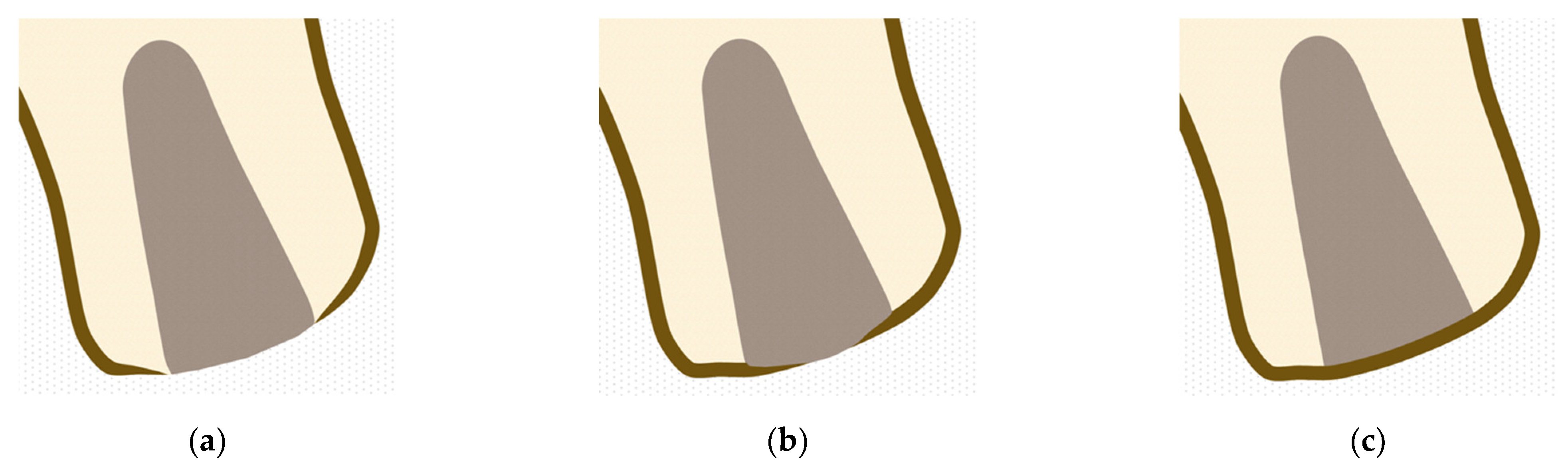
2.4.3. Evaluation of Degree of Alveolar Crest Corticalization
- Absent: When no union was observed between vestibular and palatine/lingual cortical at alveolar crestal level (Figure 3a).
- Partial: When the union between vestibular and palatine/lingual cortical was interrupted at alveolar crestal level (Figure 3b).
- Complete: When union was observed between vestibular and palatine/lingual cortical bone at alveolar crestal level (Figure 3c).
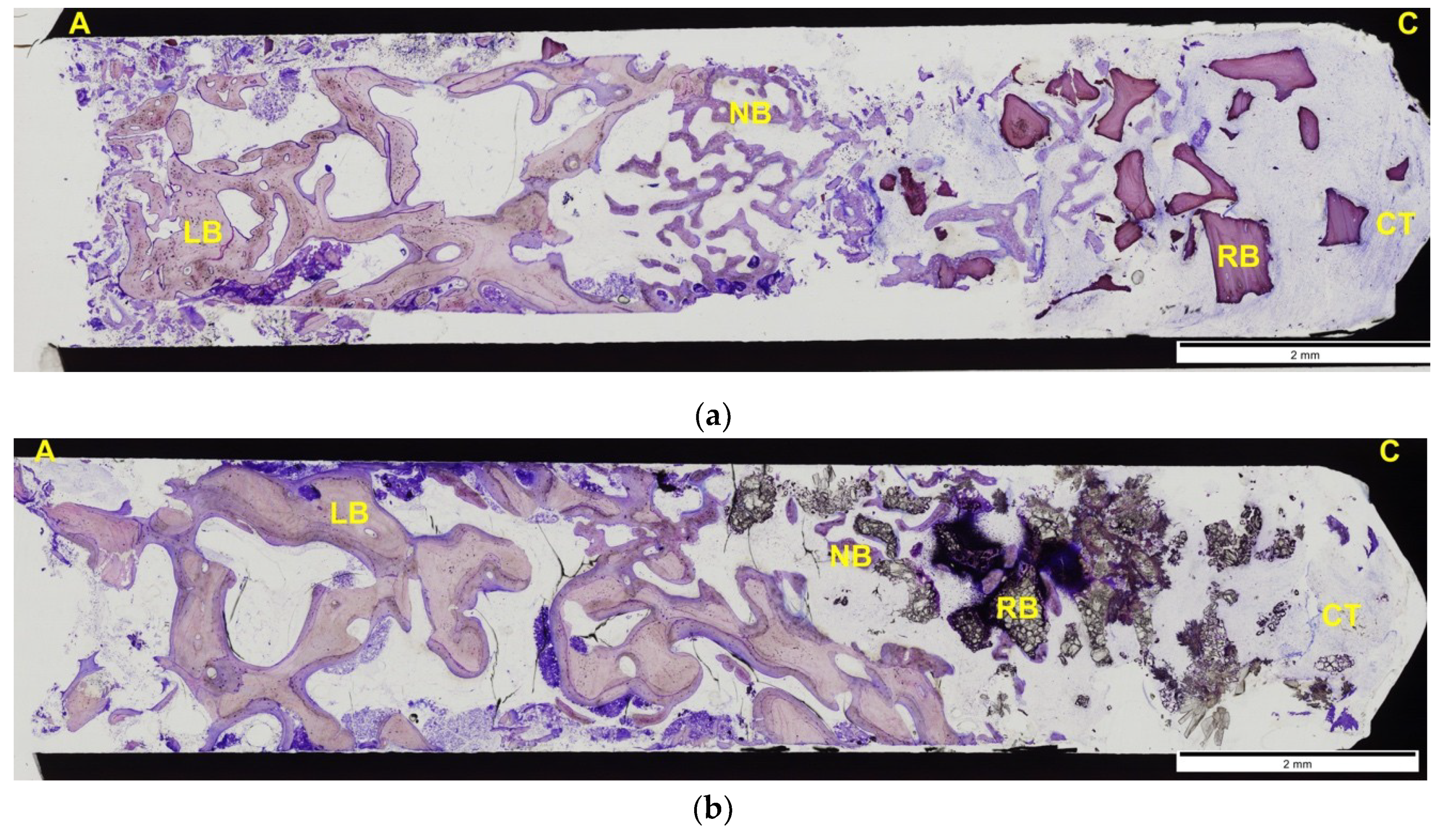
2.4.4. Histomorphometric Analyses
2.5. Statistical Analysis
3. Results
3.1. Densitometric Results
3.2. Bone Loss Results
3.3. Degree of Corticalization of Crestal Bone
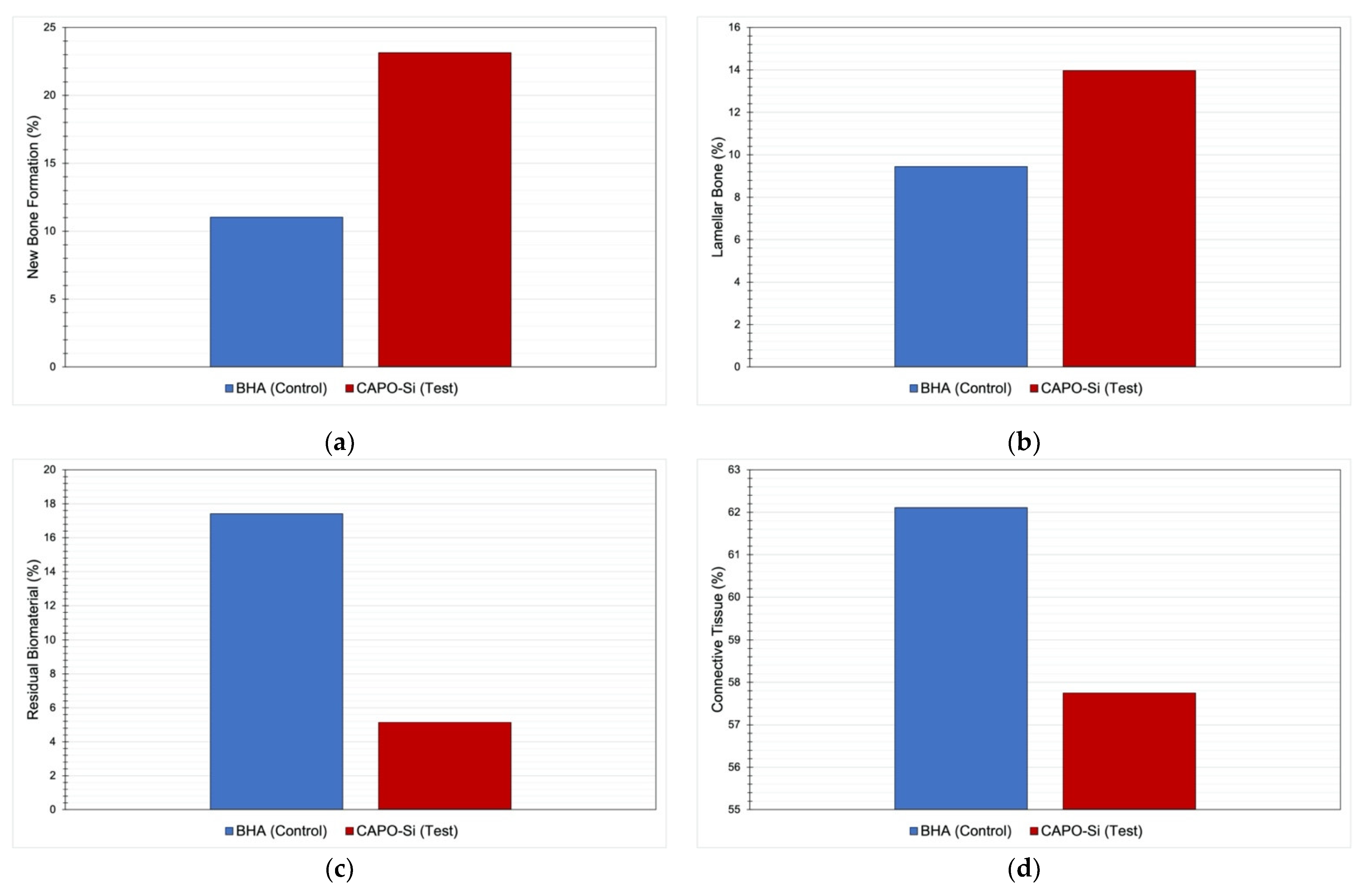
3.4. Histomorphometric Results
4. Discussion
- D1: Dense cortical bone: >1250 HU.
- D2: Dense to porous cortical bone and thick trabeculae: 850–1250 HU.
- D3: Thin porous cortical bone and fine trabeculae: 350–850 HU.
- D4: Fine trabeculae: 150–350 HU.
- D5: Bone with incomplete mineralization: <150 HU.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knabe, C.; Houshmand, A.; Berger, G.; Ducheyne, P.; Gildenhaar, R.; Kranz, I.; Stiller, M. Effect of rapidly resorbable bone substitute materials on the temporal expression of the osteoblastic phenotype in vitro. J. Biomed. Mater. Res. A 2008, 84, 856–868. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef]
- Vignoletti, F.; Matesanz, P.; Rodrigo, D.; Figuero, E.; Martin, C.; Sanz, M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin. Oral Impl. Res. 2012, 23, 22–38. [Google Scholar] [CrossRef]
- Willenbacher, M.; Al-Nawas, B.; Berres, M.; Kämmerer, P.W.; Schiegnitz, E. The effects of alveolar ridge preservation: A meta-analysis. Clin. Implant Dent. Relat. Res. 2016, 18, 1248–1268. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Impl. Res. 2012, 23, 1–21. [Google Scholar] [CrossRef]
- Andrés-Veiga, M.; Barona-Dorado, C.; Martínez-González, M.J.; López-Quiles, J.; Martínez-González, J.M. Influence of the patient’s sex, type of dental prosthesis and antagonist on residual bone resorption at the level of the premaxila. Med. Oral Patol. Oral Cir. Bucal 2012, 1, 178–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardaropoli, G.; Araújo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef]
- Cawood, J.I.; Howell, R.A. Reconstructive preprosthetic surgery. I. Anatomical considerations. Int. J. Oral Maxillofac. Surg. 1991, 20, 75–82. [Google Scholar] [CrossRef]
- Horowitz, R.; Holtzclaw, D.; Rosen, P.S. A review on alveolar ridge preservation following tooth extraction. J. Evid. Based Dent. Pract. 2012, 12, 149–160. [Google Scholar] [CrossRef]
- Mardas, N.; Chadha, V.; Donos, N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: A randomized, controlled clinical trial. Clin. Oral Impl. Res. 2010, 21, 688–698. [Google Scholar] [CrossRef]
- Horváth, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.G.; Donos, N. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Canellas, J.V.; Ritto, F.; Figueredo, C.M.; Fischer, R.; de Oliveira, G.P.; Thole, A.A.; Medeiros, P. Histomorphometric Evaluation of Different Grafing Materials Used for Alveolar Ridge Preservation: A Systematic Review and Network Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2019, 49, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Alsabeeha, N.H.; Payne, A.G.; Duncan, W.; Faggion, C.M.; Esposito, M. Interventions for Replacing Missing Teeth: Alveolar Ridge Preservation Techniques for Dental Implant Site Development. Cochrane Database Syst. Rev. 2015, 5, CD010176. [Google Scholar] [CrossRef]
- Wallace, S.C. Guided bone regeneration for socket preservation in molar extraction sites: Histomorphometric and 3D computerized tomography analysis. J. Oral Implantol. 2013, 39, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Orsini, G.; Ricci, J.; Scarano, A.; Pecora, G.; Petrone, G.; Iezzi, G.; Piattelli, A. Bone-defect healing with calcium-sulfate particles and cement: An experimental study in rabbit. J. Biomed. Mater. Res. B Appl. Biomater. 2004, 68, 199–208. [Google Scholar] [CrossRef]
- Sakkas, A.; Wilde, F.; Heufelder, M.; Winter, K.; Schramm, A. Autogenous bone grafts in oral implantology-is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int. J. Implant Dent. 2017, 3, 23. [Google Scholar] [CrossRef]
- Kloss, F.R.; Offermanns, V.; Kloss-Brandstätter, A. Comparison of allogeneic and autogenous bone grafts for augmentation of alveolar ridge defects-A 12-month retrospective radiographic evaluation. Clin. Oral Implants Res. 2018, 29, 1163–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taschieri, S.; Del Fabbro, M.; Panda, S.; Goker, F.; Babina, K.S.; Tampieri, A.; Mortellaro, C. Prospective Clinical and Histologic Evaluation of Alveolar Socket Healing Following Ridge Preservation Using a Combination of Hydroxyapatite and Collagen Biomimetic Xenograft Versus Demineralized Bovine Bone. J. Craniofac. Surg. 2019, 30, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Min, S.; Freire, M.; Bakshallian, N.; Wu, I.; Zadeh, H.H. A Histologic and Histomorphometric Retrospective Analysis of the Outcomes of Ridge Preservation Using Anorganic Bovine Bone Minerals and a Nonresorbable Membrane. Int. J. Periodontics Restorative Dent. 2018, 38, 637–644. [Google Scholar] [CrossRef]
- Fischer, K.R.; Mühlemann, S.; Jung, R.E.; Friedmann, A.; Fickl, S. Dimensional Evaluation of Different Ridge Preservation Techniques with a Bovine Xenograft: A Randomized Controlled Clinical Trial. Int. J. Periodontics Restorative Dent. 2018, 38, 549–556. [Google Scholar] [CrossRef]
- Flichy-Fernández, A.J.; Blaya-Tárraga, J.A.; O’Valle, F.; Padial-Molina, M.; Peñarrocha-Diago, M.; Galindo-Moreno, P. Sinus Floor Elevation Using Particulate PLGA-coated Biphasic Calcium Phosphate Bone Graft Substitutes: A Prospective Histological and Radiological Study. Clin. Implant Dent. Relat. Res. 2019, 21, 895–902. [Google Scholar] [CrossRef]
- Helder, M.N.; van Esterik, F.; Kwehandjaja, M.D.; ten Bruggenkate, C.M.; Klein-Nulend, J.; Schulten, E. Evaluation of a New Biphasic Calcium Phosphate for Maxillary Sinus Floor Elevation: Micro-CT and Histomorphometrical Analyses. Clin. Oral Implants Res. 2018, 29, 488–498. [Google Scholar] [CrossRef]
- Friedmann, A.; Gissel, K.; Konermann, A.; Götz, W. Tissue Reactions After Simultaneous Alveolar Ridge Augmentation with Biphasic Calcium Phosphate and Implant Insertion-Histological and Immunohistochemical Evaluation in Humans. Clin. Oral Investig. 2015, 19, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Machtei, E.E.; Mayer, Y.; Horwitz, J.; Zigdon-Giladi, H. Prospective Randomized Controlled Clinical Trial to Compare Hard Tissue Changes Following Socket Preservation Using Alloplasts, Xenografts vs No Grafting: Clinical and Histological Findings. Clin. Implant Dent. Relat. Res. 2019, 21, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Canullo, L.; Tronchi, M.; Kawakami, S.; Iida, T.; Signorini, L.; Mordini, L. Horizontal Bone Augmentation in the Anterior Esthetic Area of the Maxilla Using a Flap Design Adapted from Mucogingival Surgery in Association with PLA Membrane and β-TCP. Int. J. Perodontics Restorative Dent. 2019, 39, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Knabe, C.; Adel-Khattab, D.; Hübner, W.D.; Peters, F.; Knauf, T.; Peleska, B.; Barnewitz, D.; Genzel, A.; Kusserow, R.; Sterzik, F.; et al. Effect of silicon-doped calcium phosphate bone grafting materials on bone regeneration and osteogenic marker expression after implantation in the ovine scapula. J. Biomed. Mater. Res. B Appl. Biomater. 2019, 107, 594–614. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E. Dental implants placed in extraction sites grafted with different bone substitutes: Radiographic evaluation at 24 months. J. Periodontol. 2009, 80, 1616–1621. [Google Scholar] [CrossRef]
- Bernhardt, A.; Lode, A.; Peters, F.; Gelinsky, M. Comparative evaluation of different calcium phosphate-based bone graft granules—An in vitro study with osteoblast-like cells. Clin. Oral Impl. Res. 2013, 24, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Liu, H.; Zhou, N.; Li, Q.; Yang, G.; Chen, L.; Mou, Y. Surface Modified Techniques and Emerging Functional Coating of Dental Implants. Coatings 2020, 10, 1012. [Google Scholar] [CrossRef]
- Capparè, P.; Tetè, G.; Sberna, M.T.; Panina-Bordignon, P. The Emerging Role of Stem Cells in Regenerative Dentistry. Curr. Gene Ther. 2020, 20, 259–268. [Google Scholar] [CrossRef]
- Limongi, T.; Susa, F.; Allione, M.; di Fabrizio, E. Drug Delivery Applications of Three-Dimensional Printed (3DP) Mesoporous Scafolds. Pharmaceutics 2020, 12, 851. [Google Scholar] [CrossRef] [PubMed]
- Fielding, G.; Bose, S. SiO2 and ZnO dopants in three-dimensionally printed tricalcium phosphate bone tissue engineering scaffolds enhance osteogenesis and angiogenesis in vivo. Acta Biomater. 2013, 9, 9137–9148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohner, M. Silicon-substituted calcium phosphates—A critical view. Biomaterials 2009, 30, 6403–6406. [Google Scholar] [CrossRef] [PubMed]
- Al-Sabbagh, M.; Burt, J.; Barakat, A.; Kutkut, A.; El-Ghannam, A. Alveolar ridge preservation using resorbable bioactive ceramic composite: A histological study. J. Int. Acad. Periodontol. 2013, 15, 91–98. [Google Scholar]
- Pietak, A.M.; Reid, J.W.; Stott, M.J.; Sayer, M. Silicon substitution in the calcium phosphate bioceramics. Biomaterials 2007, 28, 4023–4032. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Best, S.M.; Bonfield, W.; Gibson, I.R.; Hing, K.A.; Damien, E.; Revell, P.A. A comparative study on the in vivo behavior of hydroxyapatite and silicon substituted hydroxyapatite granules. J. Mater. Sci. Mater. Med. 2002, 13, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Shakibaie-M, B. Comparison of the effectiveness of two different bone substitute materials for socket preservation after tooth extraction: A controlled clinical study. Int. J. Periodontics Restorative Dent. 2013, 33, 223–228. [Google Scholar] [CrossRef]
- Lorenz, J.; Korzinskas, T.; Chia, P.; Maawi, S.A.; Eichler, K.; Sader, R.A.; Ghanaati, S. Do Clinical and Radiological Assessments Contribute to the Understanding of Biomaterials? Results From a Prospective Randomized Sinus Augmentation Split-Mouth Trial. J. Oral Implatol. 2018, 44, 62–69. [Google Scholar] [CrossRef]
- Zhai, W.; Lu, H.; Chen, L.; Lin, X.; Huang, Y.; Dai, K.; Naoki, K.; Chen, G.; Chang, J. Silicate bioceramics induce angiogenesis during bone regeneration. Acta Biomater. 2012, 8, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Alt, V.; Kögelmaier, D.V.; Lips, K.S.; Witt, V.; Pacholke, S.; Heiss, C.; Kampschulte, M.; Heinemann, S.; Hanke, T.; Thormann, U.; et al. Assessment of angiogenesis in osseointegration of a silica-collagen biomaterial using 3D-nano-CT. Acta Biomater. 2011, 7, 3773–3779. [Google Scholar] [CrossRef]
- Laczkó, J.; Lévai, G. A simple differential staining method for semi-thin sections of ossifying cartilage and bone tissues embedded in epoxy resin. Mikroskopie 1975, 31, 1–4. [Google Scholar]
- Knabe, C.; Knauf, T.; Adel-Khattab, D.; Peleska, B.; Hübner, W.D.; Peters, F.; Rack, A.; Gildenhaar, R.; Berger, G.; Günster, J.; et al. Effect of a rapidly resorbable calcium alkali phosphate bone grafting material on osteogenesis after sinus floor augmentation in humans. Key Eng. Mat. 2017, 758, 239–244. [Google Scholar] [CrossRef]
- Crespi, R.; Capparé, P.; Romanos, G.E.; Mariani, E.; Benasciutti, E.; Gherlone, E. Corticocancellous porcine bone in the healing of human extraction sockets: Combining histomorphometry with osteoblast gene expression profiles in vivo. Int. J. Oral Maxillofac. Implants 2011, 26, 866–872. [Google Scholar]
- Jeong, K.I.; Kim, S.G.; Oh, J.S.; Jeong, M.A. Consideration of various bone quality evaluation methods. Implant Dent. 2013, 22, 55–59. [Google Scholar] [CrossRef]
- Misch, C.E. Contemporary Implant Dentistry, 3rd ed.; Mosby: St. Louis, MO, USA, 2008; pp. 134–146. [Google Scholar]
- Henao, S.L.; Morales, L.M.; Valencia, C.; Arce, S.; Jaramillo, A.; Cruz, C.; Martínez, C. Determination of changes in height and bone density after process preservation with synthetic bone substitute. Rev. Estomatol. 2016, 24, 11–17. [Google Scholar] [CrossRef]
- Del Canto-Díaz, A.; de Elío-Oliveros, J.; Del Canto-Díaz, M.; Alobera-Gracia, M.A.; Del Canto-Pingarrón, M.; Martínez-González, J.M. Use ofautologoustooth-derivedgraft material in thepost-extraction dental socket. Pilot study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e53–e60. [Google Scholar] [CrossRef]
- Barone, A.; Toti, P.; Quaranta, A.; Alfonsi, F.; Cucchi, A.; Negri, B.; Di Felice, R.; Marchionni, S.; Calvo-Guirado, J.L.; Covani, U.; et al. Clinical and Histological changes after ridge preservation with two xenografts: Preliminary results from a multicentre randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Aimetti, M.; Romano, F.; Griga, F.B.; Godio, L. Clinical and histologic healing of human extraction sockets filled with calcium sulfate. Int. J. Oral Maxillofac. Implants 2009, 24, 902–909. [Google Scholar] [PubMed]
- Capparé, P.; Teté, G.; Romanos, G.E.; Nagni, M.; Sannino, G.; Gherlone, E.F. The ‘All-on-four’ protocol in HIV-positive patients: A prospective, longitudinal 7-year clinical study. Int. J. Oral. Implantol. 2019, 12, 501–510. [Google Scholar]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Scala, A.; Lang, N.P.; Schweikert, M.T.; de Oliveira, J.A.; Rangel-Garcia, I.; Botticelli, D. Sequential healing of open extraction sockets. An experimental study in monkeys. Clin. Oral Implants Res. 2014, 25, 288–295. [Google Scholar] [CrossRef]
- Shim, J.-Y.; Lee, Y.; Lim, J.-H.; Jin, M.-U.; Lee, J.-M.; Suh, J.Y.; Kim, Y.-G. Comparative Evaluation of Recombinant Human Bone Morphogenetic Protein-2/Hydroxyapatite and Bovine Bone for New Bone Formation in Alveolar Ridge Preservation. Implant Dent. 2018, 27, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Ramaglia, L.; Saviano, R.; Matarese, G.; Cassandro, F.; Williams, R.C.; Isola, G. Histologic Evaluation of Soft and Hard Tissue Healing Following Alveolar Ridge Preservation with Deproteinized Bovine Bone Mineral Covered with Xenogenic Collagen Matrix. Int. J. Periodontics Restorative Dent. 2018, 38, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Mardas, N.; Trullenque-Eriksson, A.; MacBeth, N.; Petrie, A.; Donos, N. Does ridge preservation following tooth extraction improve implant treatment outcomes: A systematic review: Group 4: Therapeutic concepts & methods. Clin. Oral Implants Res. 2015, 26, 180–201. [Google Scholar] [CrossRef] [PubMed]
- De Risi, V.; Clementini, M.; Vittorini, G.; Mannocci, A.; De Sanctis, M. Alveolar ridge preservation techniques: A systematic review and meta-analysis of histological and histomorphometrical data. Clin. Oral Implants Res. 2015, 26, 50–68. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Alveolus | Horizontal Loss (mm) Mean ± SD | Vertical Loss (mm) Mean ± SD |
|---|---|---|
| Control (BHA) | 1.3 ± 0.3 | 0.7 ± 0.2 |
| Test (CAPO-Si) | 0.99 ± 0.2 | 0.7 ± 0.3 |
| p | 0.017 | 0.636 |
| Patient | Control Corticalization | Test Corticalization |
|---|---|---|
| 1 | Partial | Complete |
| 2 | Partial | Partial |
| 3 | Complete | Partial |
| 4 | Absent | Absent |
| 5 | Complete | Complete |
| 6 | Partial | Absent |
| 7 | Absent | Complete |
| 8 | Complete | Complete |
| 9 | Partial | Partial |
| 10 | Complete | Complete |
| 11 | Partial | Complete |
| 12 | Complete | Complete |
| Alveolus | % of Neoformed Bone Mean ± SD | % of Lamellar Bone Mean ± SD | % of Residual Biomaterial Mean ± SD | % of Connective Tissue Mean ± SD |
|---|---|---|---|---|
| Control (BHA) | 11 ± 7 | 9 ± 10 | 17 ± 13 | 62 ± 7 |
| Test (CAPO-Si) | 23 ± 15 | 14 ± 10 | 5 ± 10 | 58 ± 16 |
| p | 0.039 | 0.342 | 0.043 | 0.454 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cadenas-Vacas, G.; Martínez-Rodríguez, N.; Barona-Dorado, C.; Sánchez-Labrador, L.; Cortés-Bretón Brinkmann, J.; Meniz-García, C.; Martínez-González, J.M. Calcium Phosphate Modified with Silicon vs. Bovine Hydroxyapatite for Alveolar Ridge Preservation: Densitometric Evaluation, Morphological Changes and Histomorphometric Study. Materials 2021, 14, 940. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14040940
Cadenas-Vacas G, Martínez-Rodríguez N, Barona-Dorado C, Sánchez-Labrador L, Cortés-Bretón Brinkmann J, Meniz-García C, Martínez-González JM. Calcium Phosphate Modified with Silicon vs. Bovine Hydroxyapatite for Alveolar Ridge Preservation: Densitometric Evaluation, Morphological Changes and Histomorphometric Study. Materials. 2021; 14(4):940. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14040940
Chicago/Turabian StyleCadenas-Vacas, Guillermo, Natalia Martínez-Rodríguez, Cristina Barona-Dorado, Luis Sánchez-Labrador, Jorge Cortés-Bretón Brinkmann, Cristina Meniz-García, and José María Martínez-González. 2021. "Calcium Phosphate Modified with Silicon vs. Bovine Hydroxyapatite for Alveolar Ridge Preservation: Densitometric Evaluation, Morphological Changes and Histomorphometric Study" Materials 14, no. 4: 940. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14040940