
Melatonin as a Topical/Systemic Formulation for the Management of Periodontitis: A Systematic Review

 , , , ,
, , , ,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Focus Question
- PICOS question 1: Is TF effective as a therapeutic measure in the management of periodontitis in human patients who have not undergone SRP?
- PICOS question 2: Is SF effective as an adjunctive therapeutic measure in the management of periodontitis in human patients who have undergone SRP?
2.5. Search Strategy
2.6. Study Selection and Data Extraction
2.7. Risk of Bias Assessment, SIGN 50, and GRADE Scoring of the Included Studies
2.8. Meta-Analysis
3. Results
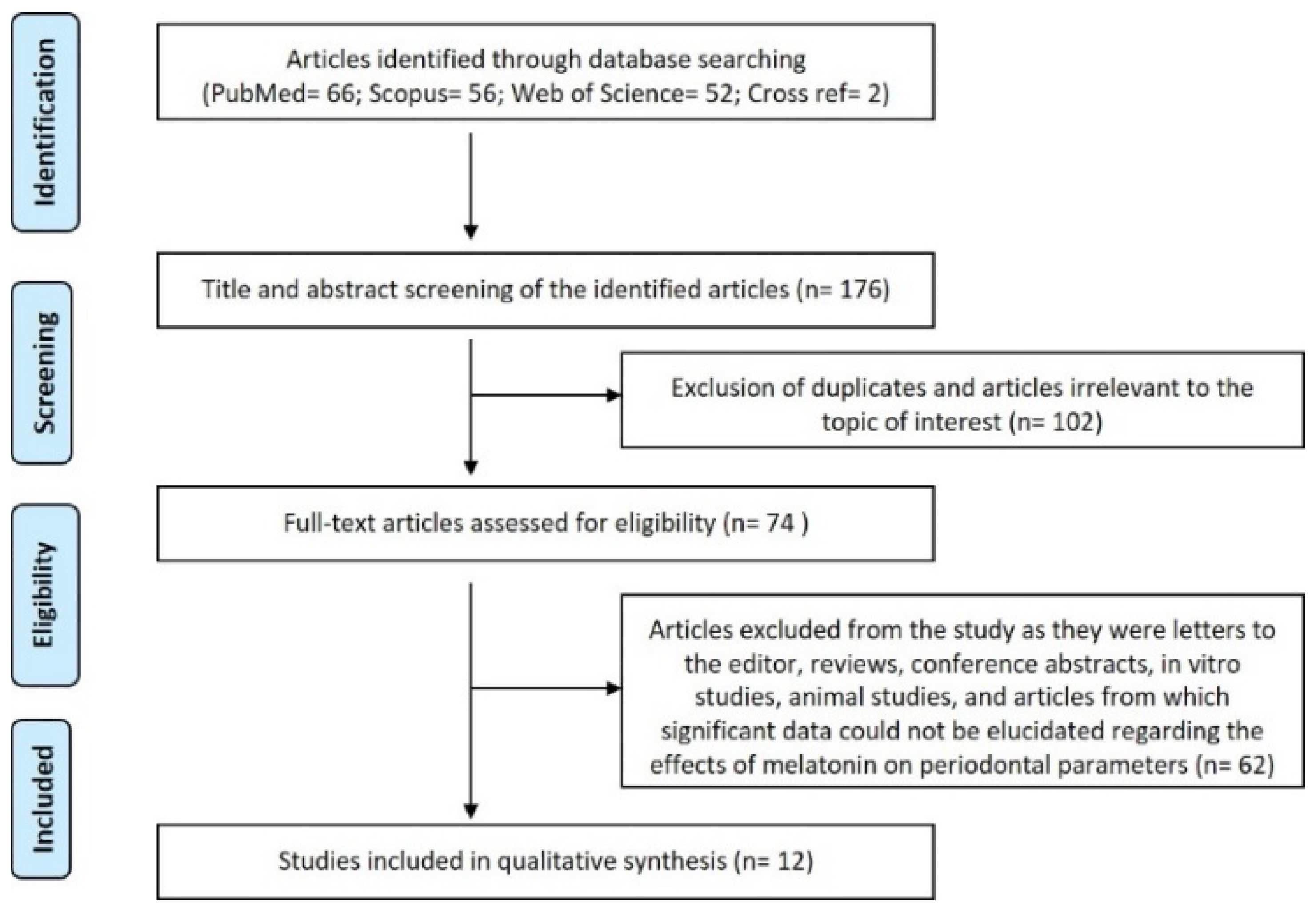
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Effect of Topical Melatonin Administration on Periodontal Parameters and Biomarker Levels
3.2.2. Effect of Systemic Melatonin Administration on Periodontal Parameters and Biomarker Levels
3.3. Risk of Bias Assessment
3.4. SIGN 50 Scorings of RCT
3.5. GRADE Scoring of the Recruited Studies
3.6. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Drisko, C.H. Nonsurgical periodontal therapy. Periodontology 2000 2001, 25, 77–88. [Google Scholar] [CrossRef]
- Slots, J. Selection of antimicrobial agents in periodontal therapy. J. Periodontal Res. 2002, 37, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Castro, M.M.L.; Duarte, N.N.; Nascimento, P.C.; Magno, M.B.; Fagundes, N.C.F.; Flores-Mir, C.; Monteiro, M.C.; Rösing, C.K.; Maia, L.C.; Lima, R.R. Antioxidants as Adjuvants in Periodontitis Treatment: A Systematic Review and Meta-Analysis. Oxid. Med. Cell. Longev. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-Y.; Cho, I.-W.; Shin, H.-S.; Ahn, H.-S.; Kim, H.-J.; Park, J.-C. Effects of host modulation by nonsteroidal anti-inflammatory drugs on periodontal disease: A systematic review and meta-analysis. J. Dent. Rehabil. Appl. Sci. 2017, 33, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Ramanauskaite, E.; Machiulskiene, V. Antiseptics as adjuncts to scaling and root planing in the treatment of periodontitis: A systematic literature review. BMC Oral Health 2020, 20, 143. [Google Scholar] [CrossRef] [PubMed]
- Cutando, A.; López-Valverde, A.; de Diego, R.G.; de Vicente, J.; Reiter, R.; Herrero Fernández, M.; Ferrera, M.J. Effect of topical application of melatonin to the gingiva on salivary osteoprotegerin, RANKL and melatonin levels in patients with diabetes and periodontal disease. Odontology 2014, 102, 290–296. [Google Scholar] [CrossRef]
- Bazyar, H.; Gholinezhad, H.; Moradi, L.; Salehi, P.; Abadi, F.; Ravanbakhsh, M.; Zare Javid, A. The effects of melatonin supplementation in adjunct with non-surgical periodontal therapy on periodontal status, serum melatonin and inflammatory markers in type 2 diabetes mellitus patients with chronic periodontitis: A double-blind, placebo-controlled t. Inflammopharmacology 2019, 27, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Cutando, A.; Montero, J.; Gomez-de Diego, R.; Ferrera, M.; Lopez-Valverde, A. Effect of topical application of melatonin on serum levels of C-reactive protein (CRP), interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-a) in patients with type 1 or type 2 diabetes and periodontal disease. J. Clin. Exp. Dent. 2015, 7, e628–e633. [Google Scholar] [CrossRef]
- Reiter, R.J. Pineal Melatonin: Cell Biology of Its Synthesis and of Its Physiological Interactions. Endocr. Rev. 1991, 12, 151–180. [Google Scholar] [CrossRef] [Green Version]
- Sugden, D. Melatonin biosynthesis in the mammalian pineal gland. Experientia 1989, 45, 922–932. [Google Scholar] [CrossRef]
- Madapusi, B.T.; Rao, S.R. Preliminary Evaluation of Human Gingiva as an Extrapineal Site of Melatonin Biosynthesis in States of Periodontal Health and Disease. J. Clin. Diagn Res. 2018, 12, 1–7. [Google Scholar] [CrossRef]
- Shimozuma, M.; Tokuyama, R.; Tatehara, S.; Umeki, H.; Ide, S.; Mishima, K.; Saito, I.; Satomura, K. Expression and cellular localizaion of melatonin-synthesizing enzymes in rat and human salivary glands. Histochem. Cell Biol. 2011, 135, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Cagnacci, A. Influences of melatonin on human circadian rhythms. Chronobiol. Int. 1997, 14, 205–220. [Google Scholar] [CrossRef]
- Reiter, R.J.; Mayo, J.C.; Tan, D.X.; Sainz, R.M.; Alatorre-Jimenez, M.; Qin, L. Melatonin as an antioxidant: Under promises but over delivers. J. Pineal Res. 2016, 61, 253–278. [Google Scholar] [CrossRef]
- Carrillo-Vico, A.; Reiter, R.J.; Lardone, P.J.; Herrera, J.L.; Fernández-Montesinos, R.; Guerrero, J.M.; Pozo, D. The modulatory role of melatonin on immune responsiveness. Curr. Opin. Investig. Drugs 2006, 7, 423–431. [Google Scholar]
- Bhattacharya, S.; Patel, K.K.; Dehari, D.; Agrawal, A.K.; Singh, S. Melatonin and its ubiquitous anticancer effects. Mol. Cell. Biochem. 2019, 462, 133–155. [Google Scholar] [CrossRef]
- Opez-Martínez, F.L.; Olivares Ponce, P.N.; Guerra Rodríguez, M.; Pedraza, R.M.; Carinci, F. Melatonin: Bone Metabolism in Oral Cavity. Int J Dent. 2012, 2012, 628406. [Google Scholar] [CrossRef]
- Balaji, T.M.; Vasanthi, H.R.; Rao, S.R. Gingival, Plasma and Salivary Levels of Melatonin in Periodontally Healthy Individuals and Chronic Periodontitis Patients: A Pilot Study. J. Clin. Diagn. Res. 2015, 9, ZC23. [Google Scholar] [CrossRef]
- Abdolsamadi, H.; Goodarzi, M.T.; Ahmadi Motemayel, F.; Jazaeri, M.; Feradmal, J.; Zarabadi, M.; Hoseyni, M.; Torkzaban, P. Reduction of Melatonin Level in Patients with Type II Diabetes and Periodontal Diseases. J. Dent. Res. Dent. Clin. Dent. Prospects 2014, 8, 160–165. [Google Scholar] [PubMed]
- Srinath, R.; Acharya, A.B.; Thakur, S.L. Salivary and Gingival Crevicular Fluid Melatonin in Periodontal Health and Disease. J. Periodontol. 2010, 81, 277–283. [Google Scholar] [CrossRef]
- Balaji, T.M.; Varadarajan, S.; Jagannathan, R.; Gupta, A.A.; Raj, A.T.; Patil, S.; Fageeh, H.I.; Fageeh, H.N. Melatonin levels in periodontitis vs. the healthy state: A systematic review and meta-analysis. Oral Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Florit, M.; Ramis, J.M.; Monjo, M. Anti-fibrotic and anti-inflammatory properties of melatonin on human gingival fibroblasts in vitro. Biochem. Pharmacol. 2013, 86, 1784–1790. [Google Scholar] [CrossRef]
- Virto, L.; Cano, P.; Jiménez-Ortega, V.; Fernández-Mateos, P.; González, J.; Haugen, H.J.; Esquifino, A.I.; Sanz, M. Melatonin as adjunctive therapy in the treatment of periodontitis associated with obesity. J. Clin. Periodontol. 2018, 45, 1336–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kose, O.; Arabaci, T.; Kara, A.; Yemenoglu, H.; Kermen, E.; Kizildag, A.; Gedikli, S.; Ozkanlar, S. Effects of Melatonin on Oxidative Stress Index and Alveolar Bone Loss in Diabetic Rats With Periodontitis. J. Periodontol. 2016, 87, e82–e90. [Google Scholar] [CrossRef] [PubMed]
- Cutando, A.; Lopez-Valverde, A.; Gomez-de-Diego, R.; Arias-Santiago, S.; de Vicente-Jimenez, J. Effect of gingival application of melatonin on alkaline and acid phosphatase, osteopontin and osteocalcin in patients with diabetes and periodontal disease. Med. Oral Patol. Oral y Cir. Bucal 2013, 18, e657–e663. [Google Scholar] [CrossRef]
- Montero, J.; Lopez-Valverde, N.; Ferrera, M.; Lopez-Valverde, A. Changes in crevicular cytokines after application of melatonin in patients with periodontal disease. J. Clin. Exp. Dent. 2017, 9, e1081–e1087. [Google Scholar] [CrossRef] [Green Version]
- Mhaske, N.; Sheker, A.; Marawar, P.; Mote, N. Evaluation of melatonin levels in saliva in periodontal health and disease: A clinico-biochemical study. J. Int. Clin. Dent. Res. Organ. 2010, 2, 119. [Google Scholar] [CrossRef]
- Chitsazi, M.; Faramarzie, M.; Sadighi, M.; Shirmohammadi, A.; Hashemzadeh, A. Effects of adjective use of melatonin and vitamin C in the treatment of chronic periodontitis: A randomized clinical trial. J. Dent. Res. Dent. Clin. Dent. Prospects 2017, 11, 236–240. [Google Scholar] [PubMed]
- El-Sharkawy, H.; Elmeadawy, S.; Elshinnawi, U.; Anees, M. Is dietary melatonin supplementation a viable adjunctive therapy for chronic periodontitis?—A randomized controlled clinical trial. J. Periodontal Res. 2019, 54, 190–197. [Google Scholar] [CrossRef]
- Marawar, A.; Marawar, P.; H, N.D.; Kunkulol, R.; Narwane, S. Evaluation of Effect of Melatonin on Hematological Parameters in Patients of Periodontitis. Int. J. Clin. Biomed. Res. 2019, 5, 46–49. [Google Scholar] [CrossRef]
- Tinto, M.; Sartori, M.; Pizzi, I.; Verga, A.; Longoni, S. Melatonin as host modulating agent supporting nonsurgical periodontal therapy in patients affected by untreated severe periodontitis: A preliminary randomized, triple-blind, placebo-controlled study. J. Periodontal Res. 2020, 55, 61–67. [Google Scholar]
- Marawar, A.P.; Marawar, P.P.; Nandal, D.H.; Kunkulol, R.R. Evaluation of antioxidant potential of melatonin in periodontitis with a focus on vitamin C. Int. J. Basic Clin. Pharmacol. 2020, 9, 378. [Google Scholar]
- Zare Javid, A.; Hosseini, S.A.; Gholinezhad, H.; Moradi, L.; Haghighi-zadeh, M.H.; Bazyar, H. Antioxidant and Anti-Inflammatory Properties of Melatonin in Patients with Type 2 Diabetes Mellitus with Periodontal Disease Under Non-Surgical Periodontal Therapy: A Double-Blind, Placebo-Controlled Trial. Diabetes, Metab. Syndr. Obes. Targets Ther. 2020, 13, 753–761. [Google Scholar]
- Suvan, J.; Leira, Y.; Moreno Sancho, F.M.; Graziani, F.; Derks, J.; Tomasi, C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J. Clin. Periodontol. 2020, 47, 155–175. [Google Scholar]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.-J.; Sheen, S.-S.; Hahn, S.; Jang, B.-H.; Son, H.-J. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Scottish Intercollegiate Guidelines Network. A Guideline Developer’s Handbook; SIGN Publication No. 50; NHS Scotland: Edinburgh, UK, 2019; ISBN 9781909103733. [Google Scholar]
- Costello, R.B.; Lentino, C.V.; Boyd, C.C.; O’Connell, M.L.; Crawford, C.C.; Sprengel, M.L.; Deuster, P.A. The effectiveness of melatonin for promoting healthy sleep: A rapid evidence assessment of the literature. Nutr. J. 2014, 13, 106. [Google Scholar]
- GRADE Home. Available online: https://www.gradeworkinggroup.org/ (accessed on 12 September 2020).
- Marawar, A.; Marawar, P.P.; Nandal, D.H.; Tilak, A.V.; Bhalsinge, R.; Barde, A.A. Therapeutic Potential of Melatonin in Periodontitis: A Randomised, Placebo Controlled, Double Blind Study. Res. J. Pharm. Biol. Chem. Sci. 2014, 5, 31–39. [Google Scholar]
- Holt, S.C.; Ebersole, J.L. Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: The “red complex”, a prototype polybacterial pathogenic consortium in periodontitis. Periodontology 2000 2005, 38, 72–122. [Google Scholar] [CrossRef]
- Kinane, D.F.; Lappin, D.F. Immune Processes in Periodontal Disease: A Review. Ann. Periodontol. 2002, 7, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C. The Pathobiology of Periodontal Diseases May Affect Systemic Diseases: Inversion of a Paradigm. Ann. Periodontol. 1998, 3, 108–120. [Google Scholar] [CrossRef]
- Wang, Y.; Andrukhov, O.; Rausch-Fan, X. Oxidative Stress and Antioxidant System in Periodontitis. Front. Physiol. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Tan, D.X.; Chen, L.D.; Poeggeler, B.; Manchester, L.C.; Reiter, R.J. Melatonin a potent endogenous hydroxyl radical scavenger. Endocr. J. 1993, 14, 57–60. [Google Scholar]
- Reiter, R.J.; Acuña-Castroviejo, D.; Tan, D.X.; Burkhardt, S. Free radical-mediated molecular damage. Mechanisms for the protective actions of melatonin in the central nervous system. Ann. N. Y. Acad. Sci. 2001, 939, 200–215. [Google Scholar] [CrossRef]
- Mayo, J.C.; Tan, D.-X.; Sainz, R.M.; Lopez-Burillo, S.; Reiter, R.J. Oxidative Damage to Catalase Induced by Peroxyl Radicals: Functional Protection by Melatonin and Other Antioxidants. Free Radic. Res. 2003, 37, 543–553. [Google Scholar] [CrossRef]
- Escames, G.; Guerrero, J.M.; Reiter, R.J.; Garcia, J.J.; Munoz-Hoyos, A.; Ortiz, G.G.; Oh, C.S. Melatonin and vitamin E limit nitric oxide-induced lipid peroxidation in rat brain homogenates. Neurosci. Lett. 1997, 230, 147–150. [Google Scholar] [CrossRef]
- Cagnoli, C.M.; Atabay, C.; Kharlamova, E.; Manev, H. Melatonin protects neurons from singlet oxygen-induced apoptosis. J. Pineal Res. 1995, 18, 222–226. [Google Scholar] [CrossRef]
- Ressmeyer, A.-R.; Mayo, J.C.; Zelosko, V.; Sáinz, R.M.; Tan, D.-X.; Poeggeler, B.; Antolín, I.; Zsizsik, B.K.; Reiter, R.J.; Hardeland, R. Antioxidant properties of the melatonin metabolite N 1 -acetyl-5-methoxykynuramine (AMK): Scavenging of free radicals and prevention of protein destruction. Redox Rep. 2003, 8, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, C.; Mayo, J.C.; Sainz, R.M.; Antolin, I.; Herrera, F.; Martin, V.; Reiter, R.J. Regulation of antioxidant enzymes: A significant role for melatonin. J. Pineal Res. 2004, 36, 1–9. [Google Scholar] [CrossRef]
- Harpsøe, N.G.; Andersen, L.P.H.; Gögenur, I.; Rosenberg, J. Clinical pharmacokinetics of melatonin: A systematic review. Eur. J. Clin. Pharmacol. 2015, 71, 901–909. [Google Scholar] [CrossRef]
- Poon, A.M.; Liu, Z.M.; Pang, S.F. Cross-talk between the pineal gland and immune system. Chin. Med. J. 1998, 111, 7–11. [Google Scholar] [PubMed]
- Hardeland, R. Melatonin and inflammation-Story of a double-edged blade. J. Pineal Res. 2018, 65, e12525. [Google Scholar] [CrossRef] [Green Version]
- Mohan, N.; Sadeghi, K.; Reiter, R.J.; Meltz, M.L. The neurohormone melatonin inhibits cytokine, mitogen and ionizing radiation induced NF-kappa B. Biochem. Mol. Biol. Int. 1995, 37, 1063–1070. [Google Scholar]
- Nabavi, S.M.; Nabavi, S.F.; Sureda, A.; Xiao, J.; Dehpour, A.R.; Shirooie, S.; Silva, A.S.; Baldi, A.; Khan, H.; Daglia, M. Anti-inflammatory effects of Melatonin: A mechanistic review. Crit. Rev. Food Sci. Nutr. 2019, 59, S4–S16. [Google Scholar] [CrossRef] [PubMed]
- Pioli, C.; Caroleo, M.C.; Nistico’, G.; Doriac, G. Melatonin increases antigen presentation and amplifies specific and non specific signals for T-cell proliferation. Int. J. Immunopharmacol. 1993, 15, 463–468. [Google Scholar] [CrossRef]
- Lissoni, P.; Barni, S.; Tancini, G.; Rovelli, F.; Ardizzoia, A.; Conti, A.; Maestroni, G.J.M. A Study of the Mechanisms Involved in the Immunostimulatory Action of the Pineal Hormone in Cancer Patients. Oncology 1993, 50, 399–402. [Google Scholar] [CrossRef]
- Seithikurippu R, A.M. Melatonin, the Hormone of Darkness: From Sleep Promotion to Ebola Treatment. Brain Disord. Ther. 2015, 4, 1000151. [Google Scholar]
- Yu, H.; Dickson, E.J.; Jung, S.-R.; Koh, D.-S.; Hille, B. High membrane permeability for melatonin. J. Gen. Physiol. 2016, 147, 63–76. [Google Scholar] [CrossRef] [Green Version]
- Amstrup, A.K.; Sikjaer, T.; Mosekilde, L.; Rejnmark, L. Melatonin and the skeleton. Osteoporos. Int. 2013, 24, 2919–2927. [Google Scholar] [CrossRef]
- Lamster, I.B. Evaluation of Components of Gingival Crevicular Fluid as Diagnostic Tests. Ann. Periodontol. 1997, 2, 123–137. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PICOS Criteria Category | Details of the Recruited Studies |
|---|---|
| population | Patients diagnosed with clinical features of periodontitis and periodontally and systemically healthy individuals |
| intervention |
|
| comparison | Periodontal and biochemical parameters in the melatonin versus the placebo/group receiving no treatment |
| outcomes | Pocket depth, clinical attachment loss, gingival index, periodontal disease index, community periodontal index, salivary and plasma levels of cytokines, oxidant and antioxidant markers |
| study |
|
| S.No | First Author Name/Year of Publication/Country of Origin | Type of Study/Sample Size | Melatonin/ Placebo Formulation Details | Method and Frequency of Melatonin Application with Details of the Intervention | Samples Collected | Markers Measured | Results | Inference |
|---|---|---|---|---|---|---|---|---|
| 1. | Antonio Cutando/2013/Spain | Clinical intervention study with 2 groups
| Test group: orabase cream with 1% melatonin Placebo group: ora base cream without melatonin | No periodontal treatment performed. All subjects in the study were instructed to apply orabase formulation (the amount that fit toothbrush surface) on upper and lower arch attached gingiva surfaces with aid of toothbrush in the night time for 20 days | Fasting stimulated saliva and plasma samples collected at baseline and 20 days post-application | Salivary acid phosphatase (ACP) and alkaline phosphatase (ALP) measured by spectrophotometric method. Salivary osteocalcin (OCN) measured by electrochemiluminescence method. Salivary osteopontin (OPN) measured by sandwich ELISA technique. | Values provided only for group 2: Baseline findings: Mean Gingival index: 15.8 ± 10.26 Mean Pocket depth: 28.3 ± 19.48 Mean ALP: 40.51 ± 4.83 Mean ACP: 83.08 ± 6.85 Mean OCN: 5.83 ± 1.41 Mean OPN: 12.49 ± 1.78 After 20 days of intervention: Mean Gingival index: 5.59 ± 4.08 Mean Pocket depth: 11.9 ± 9.01 Mean ALP: 26.88 ± 4.03 Mean ACP: 43.2 ± 5.52 Mean OCP: 5.78 ± 1.39 Mean OPN: 8.34 ± 1.45 The pocket depth and gingival index reduced significantly following melatonin application and correlated with all 4 markers significantly. | Melatonin application reduced the gingival index and pocket depths significantly and also, the levels of the 4 markers measured changes in gingival index correlated with salivary acid phosphatase and osteopontin while pocket depth changes correlated with acid, alkaline phosphatase, and osteopontin |
| 2. | Antonio Cutando/2014/Spain | Clinical intervention study with 2 groups
| Test group: orabase cream with 1% melatonin. Placebo group: ora base cream without melatonin | No periodontal treatment performed. All subjects in the study were instructed to apply orabase formulation (the amount that fit toothbrush surface) on upper and lower arch attached gingiva surfaces with aid of toothbrush in the night time for 20 days | Fasting stimulated saliva samples collected at baseline and 20 days post-application | Salivary and plasma melatonin(radioimmunoassay) measured only at baseline. Salivary Receptor activator of nuclear factor kappa B ligand (RANKL) and osteoprotegerin (OPG) (ELISA) measured at baseline and 20 days after clinical intervention | Values provided only for group 2: Baseline findings: Mean Gingival index: 15.8 ± 10.26 Mean Pocket depth: 28.3 ± 19.48 Mean salivary RANKL: 102.6 ± 66.67 Mean salivary OPG: 10.4 ± 7.61 After 20 days of intervention: Mean Gingival index: 5.6 ± 4.08 Mean Pocket depth: 11.9 ± 9.01 Mean salivary RANKL: 73.5 ± 47.39 Mean salivary OPG: 16.9 ± 7.20 Significant reduction in pocket depth, gingival index, and salivary RANK L levels and a significant increase in salivary OPG values were observed following intervention (p < 0.001). the decrease in pocket depth and gingival index correlated with a parallel increase in salivary OPG values. | Melatonin is a protective molecule in periodontal treatment especially in diabetic patients. Melatonin application reduced the gingival index and pocket depths significantly Melatonin application could inhibit RANK L mediated bone resorption in could alter the RANKL OPG ratios favorably. |
| 3. | Antonio Cutando/2015/Spain | Clinical trial study with 2 groups
| Test group: orabase cream with 1% melatonin, 16.5% sodium carboxymethyl cellulose, 16.5% pectin, 16.5% jello, plastibase c.s.p 100. Placebo group: ora base cream with the same composition as above without melatonin | No periodontal treatment performed. All subjects in the study were instructed to apply orabase formulation (the amount that fit toothbrush surface) on upper and lower arch attached gingiva surfaces with aid of toothbrush in the night time for 20 days | Fasting stimulated saliva and plasma samples collected at baseline and 20 days post-application | Salivary and plasma melatonin(radioimmunoassay) measured only at baseline. Serum C-reactive protein (CRP) measured by nephelometry and TNF alpha and IL 6 measured by ELISA | Values provided only for group 2: Baseline findings: Gingival index: 15.84 ± 10.26 Pocket depth: 28.29 ± 19.48 TNF alpha: 1.79 ± 0.19 IL 6: 0.57 ± 0.07 CRP: 0.39 ± 0.11 After 20 days of intervention: Gingival index: 5.59 ± 4.08 Pocket depth: 11.90 ± 9.01 TNF alpha: 1.76 ± 0.19 IL 6: 0.47 ± 0.07 CRP: 0.31 ± 0.11 All markers measured correlated positively with gingival index and pocket depth values. | Melatonin topical application for 20 days resulted in a significant reduction of pocket depth, gingival index, IL 6, and CRP values (p < 0.001) but not that of TNF alpha (p > 0.001) There was a positive correlation of all the 3 markers with gingival index and pocket depth after the intervention which meant that a reduction of pocket depth and gingival index also denoted a significant parallel reduction in the level of the markers It was concluded that melatonin application modulates the inflammatory response in periodontal disease |
| 4. | Javier Montero/2017/Spain | Clinical trial study with 3 groups
| Test group: orabase cream with 1% melatonin. Placebo group: ora base cream without melatonin | No periodontal treatment performed. All subjects in the study were instructed to apply orabase formulation (the amount that fit toothbrush surface) on upper and lower arch attached gingiva surfaces with aid of toothbrush in the night time for 20 days | Gingival crevicular fluid (GCF) was sampled from 2 periodontal pocket sites and pooled for the assays | GCF IL 1 beta, IL 6, and PGE 2 were measured by ELISA | Values provided for group 1 and 2 only at baseline and after 20 days of orabase application: Baseline findings: Group 1: Gingival index: 15.84 ± 10.2 Pocket depth: 2.8 ± 1.9 GCF IL 1 beta: 127.73 ± 99.50 IL 6: 0.57 ± 0.07 PGE2: 265.42 ± 101.60 Group 2: Gingival index: 14.51 ± 9.70 Pocket depth: 2.7 ± 1.5 GCF IL 1 beta: 122.47 ± 95.2 IL 6: 0.56 ± 0.07 PGE2: 263.45 ± 98.7 After 20 days of intervention: Group 1: Gingival index: 5.59 ± 4.08 Pocket depth: 1.8 ± 1.2 GCF IL 1 beta: 114.34 ± 74.88 IL 6: 0.47 ± 0.07 PGE2: 222.78 ± 87.88 Group 2: Gingival index: 14.13 ± 10.15 Pocket depth: 2.6 ± 1.2 GCF IL 1 beta: 120.93 ± 101.4 IL 6: 0.54 ± 0.07 PGE2: 260.26 ± 99.1 All values were statistically significant in Group 1 following the intervention. No significance was found in parameters before and after intervention in group 2. There was a direct and significant correlation between GCF IL1 beta, IL 6 and PGE2 values and gingival index and pocket depth in Group 1 while this correlation was absent in Group 2 | Treatment of diabetic patients with periodontal disease with topical melatonin improved the gingival index and pocket depth significantly and resulted in a significant reduction in the levels of pro-inflammatory mediators IL 1 beta, IL 6 and PGE2 |
| S.No | First Author Name/Year of Publication/Country of Origin | Type of Study/Sample Size | Melatonin/Placebo Formulation Details | Method and Frequency of Melatonin Application with Details of the Intervention | Samples Collected | Markers Measured | Results | Inference |
|---|---|---|---|---|---|---|---|---|
| 1. | Marawar A.P/2014/India | A randomized, double-blind, placebo-controlled, comparative clinical study with 2 groups Group A(80): Periodontitis patients receiving placebo after scaling and root planing Group B(80): Periodontitis patients receiving melatonin after scaling and root planing | Melatonin 3 mg tablet formulation for oral consumption Placebo details not mentioned | Melatonin tablet of 3 mg dosage was prescribed in the test group (Group B) as a daily night once dose for 4 weeks following scaling and root planing Placebo was prescribed in Group A in the same manner and frequency as above | No samples were collected | No molecular or biochemical markers measured | Gingival index Group A Baseline: 1.86 ± 0.60 30 days: 1.73 ± 0.59 60 days: 1.65 ± 0.60 90 days: 1.56 ± 0.58 Group B Baseline:1.77 ± 0.55 30 days: 1.52 ± 0.59 60 days: 1.24 ± 0.55 90 days: 1.01 ± 0.56 Statistically significant lowering of Gingival index found in the test group at 30, 60, 90 days compared to the placebo group. Periodontal disease index Group A Baseline: 4.73 ± 0.52 30 days: 4.71 ± 0.50 60 days: 4.53 ± 0.49 90 days: 4.49 ± 0.49 Group B Baseline: 4.67 ± 0.43 30 days: 4.51 ± 0.48 60 days: 4.49 ± 0.34 90 days: 4.27 ± 0.33 Statistically significant lowering of Periodontal disease index found in the test group at 30, 90 days compared to the placebo group. Community periodontal index Group A Baseline: 4.69±0.95 30 days: 4.56 ± 0.98 60 days: 4.46 ± 0.94 90 days: 4.41 ± 0.91 Group B Baseline: 4.51 ± 1.06 30 days: 2.96 ± 1.03 60 days: 2.68 ± 0.98 90 days: 2.41 ± 0.94 Statistically significant lowering of Community periodontal index found in the test group at 30, 60, 90 days compared to the placebo group (p < 0.05) | In the present study, the gingival index indicated gingival inflammation, the Periodontal disease index and Community periodontal index indicated connective tissue and bone loss. Melatonin administration was found to improve the gingival index, periodontal disease index, and community periodontal index values as an adjunctive agent following scaling and root planing. Melatonin has been inferred to combat oxidative stress and inflammation and regulates some components of the immune system thereby aiding in the management of periodontal disease |
| 2. | Chitsazi M/2017/Iran | Randomized single mask clinical trial with 3 groups Group 1(20): Chronic periodontitis patients who underwent only non-surgical therapy Group 2(20) Chronic periodontitis patients who underwent non-surgical therapy along with melatonin Group 3(20): Chronic periodontitis patients who underwent non-surgical therapy along with melatonin and vitamin C | Melatonin tablet 2 mg tablet formulation for oral consumption with or without Vitamin C tablets (60 mg for female patients and 75 mg for male patients) No placebo was used in the present study | Group 1 received scaling and root planing with no adjunctive medication or placebo Group 2 received scaling and root planing followed by melatonin 2 mg once daily dose for 4 weeks Group 3 received scaling and root planing followed by melatonin 2 mg and Vitamin C(60/75 mg) once daily dose for 4 weeks | No samples collected | No molecular or biochemical markers measured | Gingival index(GI) difference values: Group 1: Baseline to 3 months: 0.45 ± 0.13 Baseline to 6 months: 0.63 ± 0.24 3 to 6 months: 0.33 ± 0.22 Group 2: Baseline to 3 months: 0.54 ± 0.12 Baseline to 6 months: 0.83 ± 0.21 3 to 6 months: 0.62 ± 0.14 Group 3: Baseline to 3 months: 0.63 ± 0.11 Baseline to 6 months: 0.92 ± 0.22 3 to 6 months: 0.75 ± 0.13 Probing depth(PD) in mm: Group 1: Baseline: 6.40 ± 1.20 3 months: 5.23 ± 1.89 6 months: 4.92 ± 1.53 Group 2: Baseline: 6.41 ± 1.02 3 months: 4.56 ± 1.31 6 months: 3.54 ± 1.45 Group 3: Baseline: 6.43 ± 1.17 3 months: 4.41 ± 1.15 6 months: 3.08 ± 1.12 Clinical attachment loss(CAL): Group 1: Baseline: 6.23 ± 1.22 3 months: 5.14 ± 1.23 6 months: 4.56 ± 1.16 Group 2: Baseline: 6.29 ± 1.16 3 months: 4.23 ± 1.43 6 months: 3.22 ± 1.52 Group 3: Baseline: 6.30 ± 1.21 3 months: 4.12 ± 1.95 6 months: 3.00 ± 1.53 Mean GI was significantly lower in group 2 and group 3 compared to baseline after 3 and 6 months (p < 0.001), however, the difference between 3 and the 6-month interval was not significant (p > 0.05) Scaling and root planing improved PD and CAL values at 3 months and 6 months in all the three groups compared to baseline (p < 0.001). Significant PD and CAL reduction was seen in Group 3 compared to Group 1 and 2 at 6 months compared to 3 months (p < 0.05). This change was not seen in Group 1 and 2 (p > 0.05) | Melatonin plays a critical role in the pathogenesis of the periodontal disease Vitamin C is known to play a critical role in matrix remodeling and connective tissue homeostasis in the periodontium. Previous studies on Vitamin C administration after non-surgical periodontal therapy have not shown significant improvement in periodontal parameters However, a combination of Melatonin and Vitamin C is according to the present study more efficient in combating periodontal disease as Vitamin C is known to recycle and replenish melatonin level |
| 3. | Hadi Bazyar/2019/Iran | Randomized double-blinded placebo-controlled single-center trial with 2 groups The control group (22) Type 2 diabetes mellitus patients with severe symptoms of periodontal disease underwent non-surgical periodontal therapy (NSPT) including scaling and root planing with dental hygiene instructions followed by placebo tablet consumption for 8 weeks Intervention group (22) Type 2 diabetes mellitus patients with severe symptoms of periodontal disease underwent non-surgical periodontal therapy (NSPT)including scaling and root planing with dental hygiene instructions followed by melatonin tablet consumption for 8 weeks | Melatonin 250 mg tablets were procured from Nature Made, USA, composed of 3 mg melatonin net, sodium starch glycolate, magnesium stearate Placebo 250 mg tablets were made in Ahvaz Jundishapur University containing cellulose, silicon dioxide, magnesium stearate, and starch with peppermint oil for flavor | The Control group received NSPT followed by 2 placebo tablets once a day for 8 weeks to be consumed 1 h before bedtime. The intervention group received NSPT followed by 2 melatonin tablets once a day for 8 weeks to be consumed 1 h before bedtime. | Blood sample (5 mL) collected at baseline and 8 weeks post NSPT after 12 h overnight fasting | Serum melatonin, IL-6, TNF- alpha, and hc-CRP were measured in the samples using commercially available ELISA kits | Control group: Melatonin Baseline: 4.32 ± 1.93 pg/mL Post intervention: 4.07 ± 1.91 pg/mL TNF alpha Baseline: 8.65 ± 3.87 pg/mL Post intervention: 8.5 ± 3.95 pg/mL IL 6 Baseline: 2.16 ± 0.9 pg/mL Post intervention: 2.08 ± 0.87 pg/mL Hc CRP Baseline: 2.31 ± 0.96 pg/mL Post intervention: 2.4 ± 0.94 pg/mL Probing depth Baseline: 4.54 ± 1.01 mm Post-intervention: 4.36 ± 1.04 mm Clinical attachment loss Baseline: 3 ± 0.75 mm Post-intervention: 2.77 ± 0.68 mm Plaque Baseline: 22 Post-intervention: 18 Bleeding on probing Baseline: 22 Post intervention: 20 Intervention group: Melatonin Baseline: 4.52 ± 1.78 pg/mL Post intervention: 5.03 ± 1.68 pg/mL TNF alpha Baseline: 9.05 ± 3.56 pg/mL Post intervention: 8.24 ± 3.45 pg/mL IL 6 Baseline: 2 ± 0.92 pg/mL Post intervention: 1.42 ± 0.73 pg/mL Hc CRP Baseline: 2.53 ± 0.77 pg/mL Post intervention: 1.6 ± 0.91 pg/mL Probing depth Baseline: 4.45 ± 0.96 mm Post intervention: 2.59 ± 1.04 mm Clinical attachment loss Baseline: 3.04 ± 0.78 mm Post intervention: 1.59 ± 0.59 mm Plaque Baseline: 22 Post intervention: 13 Bleeding on probing Baseline: 22 Post intervention: 15 Melatonin levels in serum increased significantly in the intervention group post-treatment. Additionally, IL 6 and hs CRP levels were significantly decreased in the intervention group (p < 0.05). but not in the control group (p > 0.05) post for 8 weeks. Melatonin supplementation along with NSPT significantly lowered probing depth and clinical attachment loss values post 8 weeks compared to baseline (p < 0.05). in the control group, NSPT alone led to a significant lowering of clinical attachment values 8 weeks post-treatment (p < 0.05). In both, the groups no improvement in plaque and bleeding on probing values was noted post 8 weeks compared to baseline(p > 0.05) | Diabetes mellitus type 2 modulates and worsens periodontal disease and vice versa Melatonin supplementation improves the periodontal status of diabetes type 2 patients by altering the levels of IL-6 and hs CRP. No effect was exerted by melatonin supplementation of TNF alpha values in serum. It was noted that melatonin supplementation with non-surgical periodontal therapy also led to a significant lowering of pocket depth and clinical attachment loss Melatonin supplementation also significantly raised serum melatonin levels Melatonin supplementation may be used as a significant adjunct in periodontal management of type 2 diabetic subjects |
| 4. | Hesham-El-Sharkawy/2019/Egypt | A randomized placebo-controlled clinical trial with 2 groups Melatonin plus SRP/Group 1(38): Chronic periodontitis patients with insomnia receiving melatonin supplementation following scaling and root planing Placebo plus SRP/Group 2(36): Chronic periodontitis patients with insomnia receiving placebo following scaling and root planing | 10 mg oral melatonin capsule (Puritans pride, Inc., Holbrook, NY, USA) was given to the Group 1 participants An equivalent placebo was given to the Group 2 participants, composition not mentioned | Both groups received thorough scaling and root planing following periodontal diagnosis and inclusion into the study. Thorough oral hygiene instructions were given to the patients and 0.12% chlorhexidine mouthwash was prescribed for 2 weeks after scaling and root planing. The patients were also subjected to professional scaling and deplaquing every month until the trial was completed. 10 mg melatonin or placebo was given to the patients 1 h before bedtime as a daily dose for 2 months from the start of the trial | Saliva samples were collected from the patients after overnight fasting between 8 and 10 a.m. at baseline, 3 and 6 months after therapy. Whole unstimulated saliva was sampled by expectoration into 5 mL sterile polypropylene tubes and used for the study | Tumor necrosis factor-alpha was measured in the saliva samples using the ELISA technique | Group 1: PI: Baseline: 2.35 ± 0.45 3 months: 0.84 ± 0.26 6 months: 0.81 ± 0.23 GI: Baseline: 2.14 ± 0.36 3 months: 0.73 ± 0.19 6 months: 0.68 ± 0.17 BOP (%) Baseline: 63 ± 21 3 months: 11 ± 2.3 6 months: 12 ± 2.1 PD: Baseline: 4.3 ± 0.8 3 months: 2.4 ± 1.0 6 months: 2.3 ± 0.9 CAL: Baseline: 4.8 ± 0.9 3 months: 2.7 ± 1.1 6 months: 2.6 ± 1.0 Group 2: PI: Baseline: 2.44 ± 0.67 3 months: 0.92 ± 0.14 6 months: 0.95 ± 0.17 GI: Baseline: 2.21 ± 0.24 3 months: 0.67 ± 0.14 6 months: 0.69 ± 0.15 BOP (%) Baseline: 59 ± 19 3 months: 16 ± 2.2 6 months: 18 ± 2.8 PD: Baseline: 4.4 ± 0.7 3 months: 3.1 ± 0.9 6 months: 3.0 ± 0.8 CAL: Baseline: 4.7 ± 1.0 3 months: 3.5 ± 0.9 6 months: 3.4 ± 1.2 PD and CAL were significantly reduced in both group 1 and group 2 at 3 and 6 months compared to baseline (p < 0.001). However, a more effective reduction in PD and CAL were noted in Group 1 compared to group 2 (p < 0.01). the PI, GI, BOP values were also significantly lower in both the groups after 3 and 6 months compared to baseline (p < 0.05), with no variation between the 3 months and 6 months values (p > 0.05). The mean TNF alpha values in saliva samples and AIS scores have been only graphically depicted without actual numerical values. It was found that there was a statistically significant reduction in salivary TNF alpha and AIS scores in Group 1 compared to group 2 (p < 0.01). Correlation analysis found no significant correlation between salivary TNF alpha values with any of the other parameters assessed in both the groups | In the present trial, the efficacy of melatonin in the management of insomnia and periodontal disease was assessed. A combination of melatonin plus scaling and root planing was found to effectively reduce PD and improve CAL values and also resulted in a significant reduction of salivary TNF alpha and AIS (Athens Insomnia Score) scores. The study concluded that 10 mg of melatonin given once in the night as an adjunct to periodontal treatment will result in improvement of periodontal parameters and sleep pattern. This could also be a treatment modality in patients without sleep disorders. The effects of melatonin on the reduction of salivary TNF alpha and AIS shows its health benefits |
| 5. | Marawar A.P/2019/India | Mentioned as a prospective longitudinal study with 2 groups: Group A(80): chronic periodontitis patients who underwent scaling and root planing alone Group B(80): chronic periodontitis patients who underwent scaling and root planing along with melatonin supplementation. | Melatonin 3 mg tablets (brand not mentioned), composition unknown No placebo tablets administered in the study. | Both the groups visited on day 0 termed baseline and were subjected to full-mouth scaling and root planing. Group A received no medication while group B patients were asked to take one 3 mg melatonin tablet at night for 4 week. | Blood samples were obtained from the patients for leukocyte studies at baseline, day 30, day 60, and day 90. The volume of blood and method of drawing blood sample not mentioned. | Total leukocyte count (TLC), Differential leukocyte count (DLC), and Erythrocyte sedimentation rate (ESR) were the markers studied in the blood samples. | TLC: Group A Baseline: 9117.5 ± 2103.9 Day 30: 9112.5 ± 2098.4 8 Day 60: 8886.2 ± 1783.5 Day 90: 8531.6 ± 1555.4 Group B Baseline: 9370 ± 2278.7 Day 30: 8916.2 ± 1868.1 Day 60: 9205.5 ± 1719.6 Day 90: 7593.7 ± 1493.2 Neutrophils%: Group A Baseline: 74.05 ± 6.15 Day 30: 73.87 ± 5.09 Day 60: 73.97 ± 5.55 Day 90: 75.18 ± 5.79 Group B Baseline: 74.71 ± 6.64 Day 30: 75.57 ± 5.24 Day 60: 74.29 ± 4.87 Day 90: 73.10 ± 4.17 Lymphocytes%: Group A Baseline: 22.70 ± 4.84 Day 30: 23.50 ± 4.89 Day 60: 22.78 ± 4.98 Day 90: 21.62 ± 5.36 Group B Baseline: 22.30 ± 5.88 Day 30: 22.30 ± 5.88 Day 60: 21.67 ± 4.59 Day 90: 22.86 ± 4.34 Eosinophils% Group A Baseline: 0.41 ± 0.84 Day 30: 0.16 ± 0.43 Day 60: 0.38 ± 1.58 Day 90: 0.22 ± 0.55 Group B Baseline: 0.31 ± 0.68 Day 30: 0.27 ± 0.74 Day 60: 0.27 ± 0.55 Day 90: 0.35 ± 0.71 Monocytes% Group A Baseline: 0.95 ± 1.04 Day 30: 0.68 ± 0.72 Day 60: 0.91 ± 0.84 Day 90: 1.0 ± 0.95 Group B Baseline: 0.82 ± 0.97 Day 30: 0.65 ± 0.85 Day 60: 0.63 ± 0.78 Day 90: 0.71 ± 0.79 Basophils%: Group A Baseline: 1.85 ± 1.57 Day 30: 1.67 ± 1.33 Day 60: 1.95 ± 1.70 Day 90: 1.87 ± 1.80 Group B Baseline: 1.64 ± 1.39 Day 30: 1.65 ± 1.64 Day 60: 1.80 ± 1.48 Day 90: 1.73 ± 1.35 A higher percentage of male patients participated in the study. A highly significant reduction in total leukocyte counts was noted at 90 days in the melatonin group (Group B) compared to Group A (p < 0.01). Additionally, a highly significant reduction in neutrophil and lymphocyte counts was noted in group B compared to group A (p < 0.01). No differences were observed in ESR values between the groups (numerical values not provided). | No human study done on patients with periodontal disease to assess the hematological changes brought about by melatonin Only one animal study has reported a lowering of granulocyte counts in cattle receiving melatonin therapy. The present study results also show a similar trend. Melatonin has been proven to be an efficient immunomodulator and can activate several components of the immune system to modulate the pathogenesis of the periodontal disease. |
| 6. | Manuel Tinto/2020/Italy | A preliminary randomized triple-blind placebo-controlled study with 2 groups: Group 1 (control group) (10): periodontitis patients who underwent non-surgical periodontal therapy following one-stage full-mouth protocol associated with oral administration of placebo tablet 1 mg at bedtime for 30 days. Group 2 (experimental group) (10): periodontitis patients who underwent non-surgical periodontal therapy following one stage full mouth protocol associated with oral administration of melatonin tablet 1mg at bedtime for 30 days | Melatonin tablets 1 mg (Farmacia Parati–Dr.SSA Simona Corti, Lentate Sul Seveso, Italy) containing synthetic melatonin, pregelatinized starch USP 22, magnesium stearate, silicon dioxide. Placebo tablets 1mg (Farmacia Parati–Dr.SSA Simona Corti, Lentate Sul Seveso, Italy) containing pregelatinized starch USP 22, magnesium stearate, silicon dioxide. | Both the groups underwent non-surgical periodontal therapy (NSPT) under local anesthesia as a one-stage procedure using ultrasonic instruments and periodontal curettes. Time spent per quadrant was nearly 45 min. Patients were instructed to follow strict oral hygiene and plaque control and were instructed to use 0.2% chlorhexidine mouthwash (Corsodyl mouthwash, GlaxoSmithKline consumer Healthcare S.p. A, Verona, Italy). One anonymous blister pack containing melatonin/placebo tablets were given to the patient to be consumed once a day at bedtime for 30 days | No samples were collected from the patients | No biochemical or molecular markers assessed | Group 1 PD at baseline: 3.40 ± 0.83 PD at 6 months: 2.67 ± 0.85 Group 2 PD at baseline: 3.72 ± 0.90 PD at 6 months: 2.45 ± 0.91 Results of primary outcome: Mean PD change (standard deviation value) of teeth with pockets 4–5 mm and >6 mm: Group 1: PD 4–5 mm: 1.04 (0.69) PD > 6 mm: 2.11 (0.96) Group 2: PD 4–5 mm: 1.86 (0.81) PD > 6 mm: 3.33 (1.43) Both the groups exhibited an overall change in PD at 6 months compared to baseline (p < 0.05). However, no differences were observed between melatonin and placebo group Concerning FMBS% (Full-Mouth Bleeding Score), FMPS% (Full-Mouth Plaque Score)scores no differences were observed between the 2 groups although numerical values are not mentioned Concerning the primary outcome measured, that is the PD change at 6 months compared to baseline for the subgroups, it was found that melatonin was more efficient than placebo in reducing probing depth in both 4–5 mm and >6 mm pockets (p < 0.0001) | Melatonin is considered an efficient host modulatory agent and was well tolerated by all the participants in the present study. The long term effect of melatonin on reducing probing depth is linked to its pleiotropic functions on the immune and antioxidant systems. In the present study with its limitations of low sample size and a low dose of melatonin (1 mg) as recommended by the Italian Ministry of health, melatonin administration was found to provide non-pharmacological support in periodontal healing after non-surgical periodontal therapy. |
| 7. | Marwar A.P/2020/India | Mentioned as a prospective longitudinal study with 3 groups Group A(80): patients with chronic periodontitis who underwent scaling and root planing alone Group B(80): patients with chronic periodontitis who underwent scaling and root planing followed by supplementation with Vitamin E 200 IU at night for 4 weeks Group C(80): patients with chronic periodontitis who underwent scaling and root planing supplemented with melatonin tablet 3 mg daily at night for 4 weeks | Melatonin 3 mg tablets (no manufacturers name or composition mentioned Vitamin E 200 IU (no manufacturers name or composition mentioned No placebo formulation used in the present study. | Participants visited on day 0 and were screened and allocated to one of the 3 groups. No randomization was followed. No blinding details were provided. The patients underwent scaling and root planing. Details of technique not elaborated. They were subjected to either melatonin/Vitamin E tablets daily night for 4 weeks. Recall visits were scheduled on day 30, 60 and 90 | Blood samples were collected from the patients. Detailed protocol not mentioned | Vitamin C assay was done in the blood samples obtained at baseline, day 30, day 60, and day 90 | Antioxidant Vitamin C levels in blood samples: Baseline: Group A: 0.61 ± 0.19 Group B: 0.67 ± 0.07 Group C: 1.16 ± 0.54 Day 30: Group A: 0.66 ± 0.05 Group B: 1.10 ± 0.40 Group C: 1.24 ± 0.44 Day 60: Group A: 0.66 ± 0.06 Group B: 1.42 ± 0.41 Group C: 1.54 ± 0.41 Day 90: Group A: 0.66 ± 0.07 Group B: 1.15 ± 0.38 Group C: 1.63 ± 0.26 Statistical analysis revealed that there was a highly significant difference in Vitamin C levels in blood in Group C participants compared to Group A and Group B patients at all visits (p < 0.01) | The present study aimed at evaluating the antioxidant effect of oral administration of melatonin/ Vitamin E to chronic periodontitis patients who underwent scaling and root planing. Vitamin C was measured in the blood as it is a significant antioxidant with effects on the immune system that helps in preventing and resolution of periodontal disease. The results of elevated vitamin C in the blood of patients who underwent melatonin supplementation in contrast to Vitamin E and no supplementation reveals the biochemical effects of melatonin in the management of periodontal disease |
| 8 | Zare Javid A./2020/Iran | Randomized double-blinded placebo-controlled single-center trial with 2 groups The control group (22) Type 2 diabetes mellitus patients with severe symptoms of periodontal disease underwent non-surgical periodontal therapy (NSPT) including scaling and root planing with dental hygiene instructions followed by placebo tablet consumption for 8 weeks Intervention group (22) Type 2 diabetes mellitus patients with severe symptoms of periodontal disease underwent non-surgical periodontal therapy (NSPT) including scaling and root planing with dental hygiene instructions followed by melatonin tablet consumption for 8 weeks. | Melatonin 250 mg tablets were procured from Nature Made, USA, composed of 3 mg melatonin net, sodium starch glycolate, magnesium stearate Placebo 250 mg tablets were made in Ahvaz Jundishapur University containing cellulose, silicon dioxide, magnesium stearate, and starch with peppermint oil for flavor. | The Control group received NSPT followed by 2 placebo tablets once a day for 8 weeks to be consumed 1 h before bedtime. The intervention group received NSPT followed by 2 melatonin tablets once a day for 8 weeks to be consumed 1 h before bedtime. | Venous blood sample collected at baseline and 8 weeks post NSPT after 12 h overnight fasting. Sample centrifuged at 3000 g for 10 min at 4-degree centigrade and the serum was separated and stored at −70 degrees centigrade until further analysis. | IL 1 B, Malondialdehyde (MDA), Total antioxidant capacity (TAC), Superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) were measured by spectrophotometric and ELISA methods in a reliable manner | Control group: IL-1B (pg/mL) Baseline: 2.47 ± 0.48 Post intervention: 2.33 ± 0.54 MDA (micromoles): Baseline: 17.49 ± 1.38 Post-intervention: 17.17 ± 1.39 TAC (millimoles): Baseline: 0.318 ± 0.06 Post intervention: 0.327 ± 0.08 SOD (units/mL): Baseline: 14.27 ± 2.52 Post-intervention: 14.49 ± 2.58 CAT (units/mL): Baseline: 23.14 ± 3.52 Post-intervention; 22.72 ± 5.58 GPx (units/mL): Baseline: 231.18 ± 67.28 Post-intervention; 233.18 ± 62.66 Intervention group: IL-1B (pg/mL) Baseline: 2.41 ± 0.55 Post intervention: 2.06 ± 0.48 MDA (micromoles): Baseline: 17.2 ± 1.82 Post-intervention: 16.13 ± 1.76 TAC (millimoles): Baseline: 0.289 ± 0.04 Post intervention: 0.313 ± 0.05 SOD (units/mL): Baseline: 13.91 ± 2.75 Post-intervention: 15.53 ± 4.37 CAT (units/mL): Baseline: 24.23 ± 4.54 Post-intervention; 27.47 ± 4.12 GPx (units/mL): Baseline: 243.04 ± 68.37 Post-intervention; 262.04 ± 62.45 Mean changes in the inflammatory and antioxidant markers post-intervention in both the groups: IL-1B: Control group: −0.14 ± 0.43 Intervention group: −0.34 ± 0.54 MDA: Control group: −0.31 ± 0.88 Intervention group: −1.07 ± 0.92 TAC: Control group: 0.009 ± 0.06 Intervention group: 0.02 ± 0.04 SOD: Control group: 0.21 ± 0.57 Intervention group: 1.61 ± 2.57 CAT: Control group: −0.41 ± 6.7 Intervention group: 3.23 ± 4.67 GPx: Control group: 2 ± 25.14 Intervention group: 19 ± 27.89 No significant difference in biochemical parameters observed between the 2 groups at baseline (p > 0.05) melatonin administration in the intervention group significantly reduced the levels of IL-1B and MDA at 8 weeks post-intervention compared to baseline (p < 0.05). This change was not observable in the control group. The mean levels of SOD, GPx, CAT, and TAC were elevated in the intervention group at 8 weeks post-baseline. These changes were significant compared to the control group (p < 0.05) | Increased oxidative stress and depleted antioxidants are a feature of periodontal disease and type 2 diabetes mellitus. Melatonin supplementation was found to significantly boost antioxidant levels and could mitigate the levels of inflammatory and oxidative stress markers The dose of 6mg in the present study for melatonin supplementation has a better effect on the biochemical markers than previous studies utilizing 2 mg, 3 mg, and 5 mg. The limitation of the study is the inadequate number of groups which should be planned in the future as follows. Group 1 (diabetes plus no periodontal treatment plus placebo), Group 2 (diabetes plus no periodontal treatment plus melatonin), Group 3 (diabetes plus NSPT plus placebo), Group 4 (diabetes plus NSPT plus melatonin) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balaji, T.M.; Varadarajan, S.; Jagannathan, R.; Mahendra, J.; Fageeh, H.I.; Fageeh, H.N.; Mushtaq, S.; Baeshen, H.A.; Bhandi, S.; Gupta, A.A.; et al. Melatonin as a Topical/Systemic Formulation for the Management of Periodontitis: A Systematic Review. Materials 2021, 14, 2417. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14092417
Balaji TM, Varadarajan S, Jagannathan R, Mahendra J, Fageeh HI, Fageeh HN, Mushtaq S, Baeshen HA, Bhandi S, Gupta AA, et al. Melatonin as a Topical/Systemic Formulation for the Management of Periodontitis: A Systematic Review. Materials. 2021; 14(9):2417. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14092417
Chicago/Turabian StyleBalaji, Thodur Madapusi, Saranya Varadarajan, Raghunathan Jagannathan, Jaideep Mahendra, Hammam Ibrahim Fageeh, Hytham N. Fageeh, Shazia Mushtaq, Hosam Ali Baeshen, Shilpa Bhandi, Archana A. Gupta, and et al. 2021. "Melatonin as a Topical/Systemic Formulation for the Management of Periodontitis: A Systematic Review" Materials 14, no. 9: 2417. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14092417