
Effect of Light-Sources and Thicknesses of Composite Onlays on Micro-Hardness of Luting Composites

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
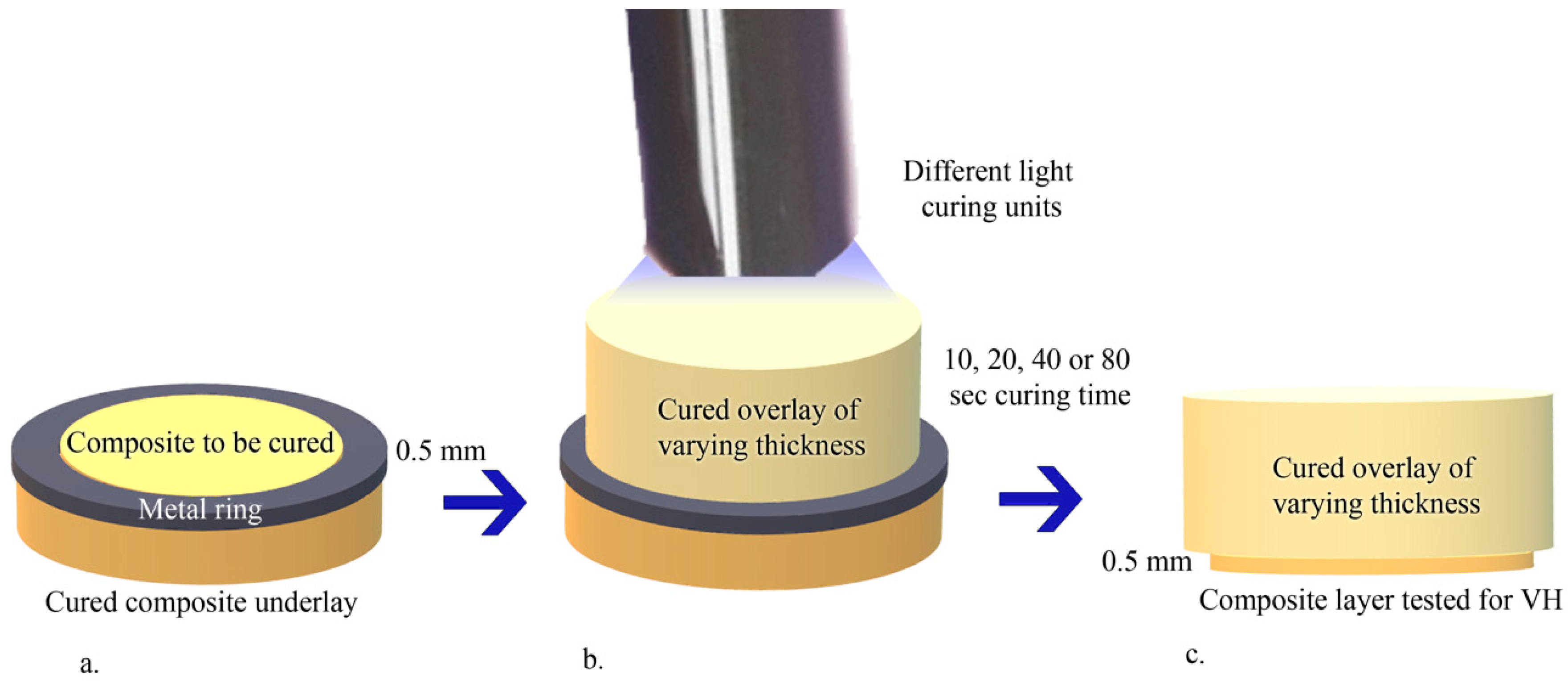
2.1. Resin Composite Overlays and Underlays Production
2.2. Experimental Group Specimen Production
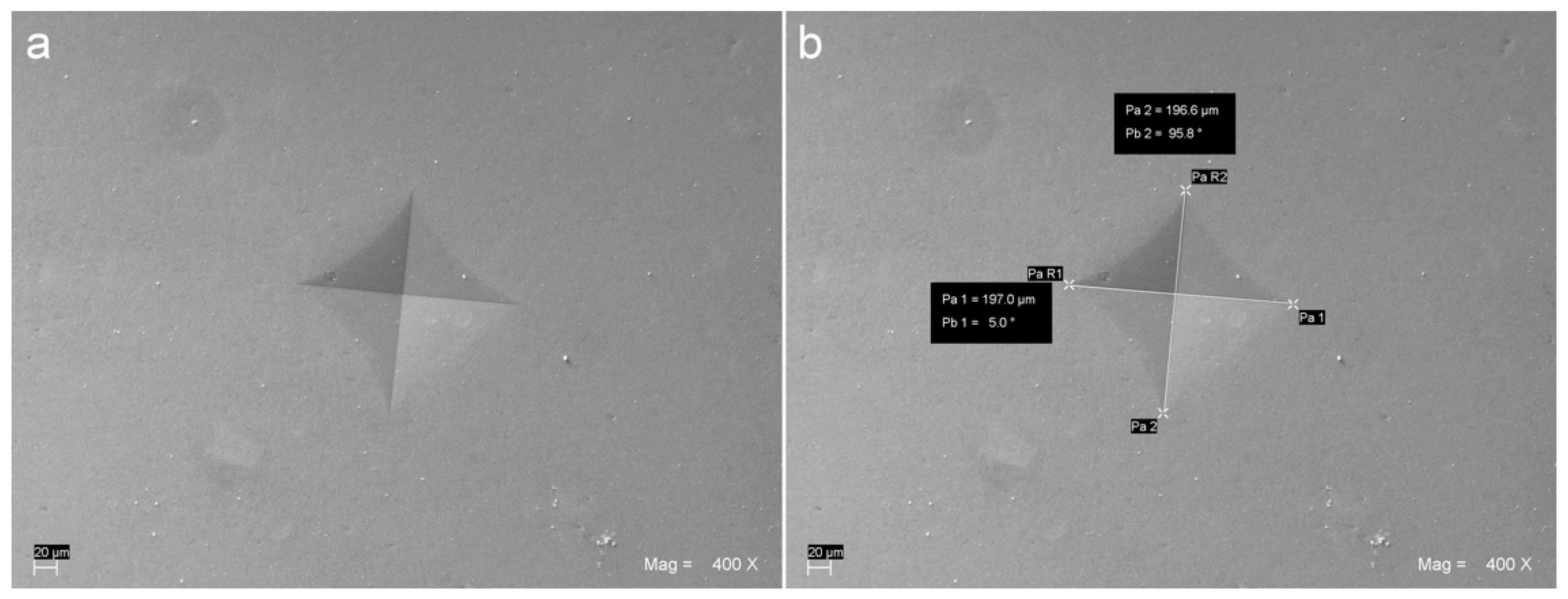
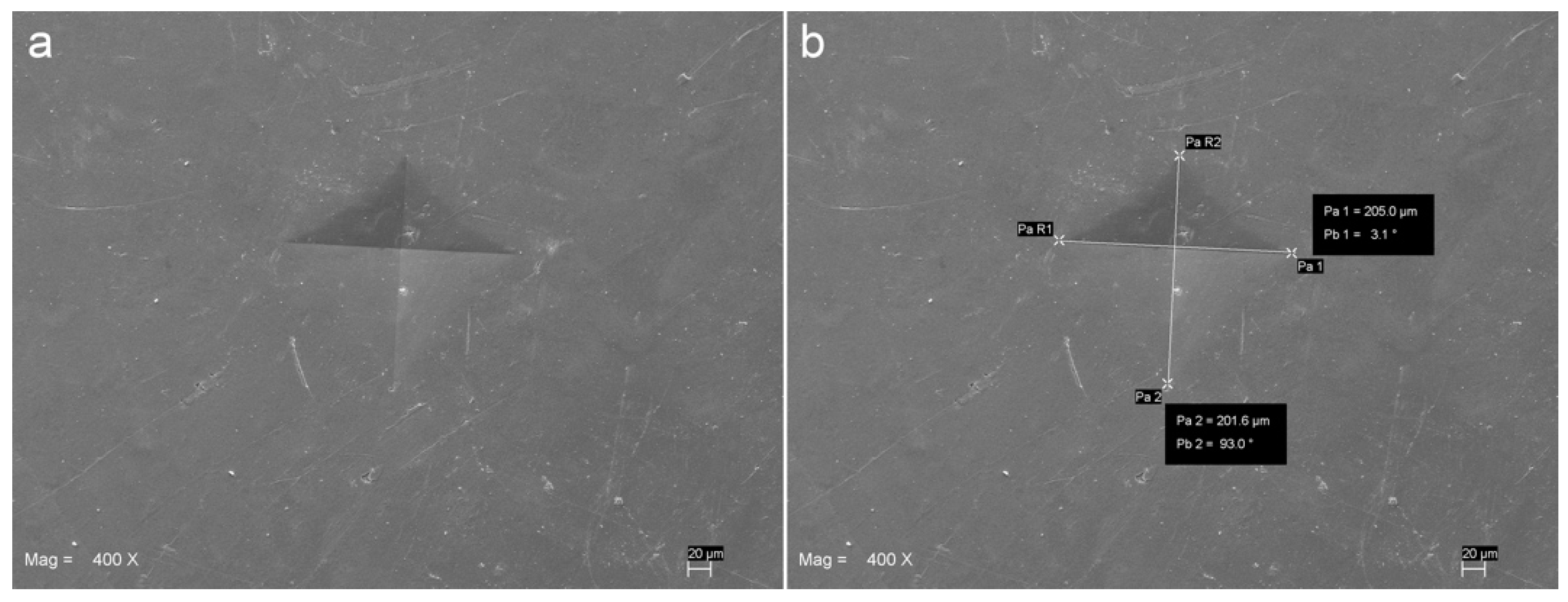
2.3. Vickers Hardness Measurement
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Radovic, I.; Monticelli, F.; Goracci, C.; Vulicevic, Z.R.; Ferrari, M. Self-adhesive resin cements: A literature review. J. Adhes. Dent. 2008, 10, 251–258. [Google Scholar]
- D’Arcangelo, C.; De Angelis, F.; Vadini, M.; Carluccio, F.; Vitalone, L.M.; D’Amario, M. Influence of curing time, overlay material and thickness on three light-curing composites used for luting indirect composite restorations. J. Adhes. Dent. 2012, 14, 377–384. [Google Scholar]
- Kameyama, A.; Bonroy, K.; Elsen, C.; Luhrs, A.K.; Suyama, Y.; Peumans, M.; Van Meerbeek, B.; De Munck, J. Luting of CAD/CAM ceramic inlays: Direct composite versus dual-cure luting cement. Biomed. Mater. Eng. 2015, 25, 279–288. [Google Scholar] [CrossRef] [Green Version]
- D’Amario, M.; Pacioni, S.; Capogreco, M.; Gatto, R.; Baldi, M. Effect of repeated preheating cycles on flexural strength of resin composites. Oper. Dent. 2013, 38, 33–38. [Google Scholar] [CrossRef] [Green Version]
- D’Amario, M.; De Angelis, F.; Vadini, M.; Marchili, N.; Mummolo, S.; D’Arcangelo, C. Influence of a repeated preheating procedure on mechanical properties of three resin composites. Oper. Dent. 2015, 40, 181–189. [Google Scholar] [CrossRef] [Green Version]
- D’Arcangelo, C.; De Angelis, F.; Vadini, M.; D’Amario, M. Clinical evaluation on porcelain laminate veneers bonded with light-cured composite: Results up to 7 years. Clin. Oral. Investig. 2012, 16, 1071–1079. [Google Scholar] [CrossRef]
- Do Nascimento, Y.A.; de Oliveira Correia, A.M.; Lima, D.M.; Griza, S.; Takeshita, W.M.; Melo de Mendonca, A.A. Effect of Ceramic Barriers of Different Thicknesses on Microhardness of Light-Cured Resin Cements. Int J. Periodontics Restor. Dent. 2017, 37, e204–e209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Arcangelo, C.; Zarow, M.; De Angelis, F.; Vadini, M.; Paolantonio, M.; Giannoni, M.; D’Amario, M. Five-year retrospective clinical study of indirect composite restorations luted with a light-cured composite in posterior teeth. Clin. Oral Investig. 2014, 18, 615–624. [Google Scholar] [CrossRef] [PubMed]
- D’Arcangelo, C.; Vanini, L.; Casinelli, M.; Frascaria, M.; De Angelis, F.; Vadini, M.; D’Amario, M. Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature Review. Compend. Contin. Educ. Dent. 2015, 36, 570–577; quiz 578. [Google Scholar] [PubMed]
- Benetti, A.R.; Peutzfeldt, A.; Asmussen, E.; Pallesen, U.; Franco, E.B. Influence of curing rate on softening in ethanol, degree of conversion, and wear of resin composite. Am. J. Dent. 2011, 24, 115–118. [Google Scholar]
- Wambier, L.; Malaquias, T.; Wambier, D.S.; Patzlaff, R.T.; Bauer, J.; Loguercio, A.D.; Reis, A. Effects of prolonged light exposure times on water sorption, solubility and cross-linking density of simplified etch-and-rinse adhesives. J. Adhes. Dent. 2014, 16, 229–234. [Google Scholar]
- Aguiar, F.H.; Lazzari, C.R.; Lima, D.A.; Ambrosano, G.M.; Lovadino, J.R. Effect of light curing tip distance and resin shade on microhardness of a hybrid resin composite. Braz. Oral Res. 2005, 19, 302–306. [Google Scholar] [CrossRef] [Green Version]
- DeWald, J.P.; Ferracane, J.L. A comparison of four modes of evaluating depth of cure of light-activated composites. J. Dent. Res. 1987, 66, 727–730. [Google Scholar] [CrossRef]
- Yoon, T.H.; Lee, Y.K.; Lim, B.S.; Kim, C.W. Degree of polymerization of resin composites by different light sources. J. Oral Rehabil. 2002, 29, 1165–1173. [Google Scholar] [CrossRef]
- Pereira, C.N.; De Magalhaes, C.S.; Daleprane, B.; Peixoto, R.T.; Ferreira Rda, C.; Cury, L.A.; Moreira, A.N. LED and Halogen Light Transmission through a CAD/CAM Lithium Disilicate Glass-Ceramic. Braz. Dent. J. 2015, 26, 648–653. [Google Scholar] [CrossRef]
- .Park, S.H.; Kim, S.S.; Cho, Y.S.; Lee, C.K.; Noh, B.D. Curing units’ ability to cure restorative composites and dual-cured composite cements under composite overlay. Oper. Dent. 2004, 29, 627–635. [Google Scholar]
- Gregor, L.; Bouillaguet, S.; Onisor, I.; Ardu, S.; Krejci, I.; Rocca, G.T. Microhardness of light- and dual-polymerizable luting resins polymerized through 7. 5-mm-thick endocrowns. J. Prosthet Dent. 2014, 112, 942–948. [Google Scholar] [CrossRef]
- Hardy, C.M.F.; Bebelman, S.; Leloup, G.; Hadis, M.A.; Palin, W.M.; Leprince, J.G. Investigating the limits of resin-based luting composite photopolymerization through various thicknesses of indirect restorative materials. Dent. Mater. 2018, 34, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Rueggeberg, F.A.; Craig, R.G. Correlation of parameters used to estimate monomer conversion in a light-cured composite. J. Dent. Res. 1988, 67, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Sailynoja, E.S.; Shinya, A.; Koskinen, M.K.; Salonen, J.I.; Masuda, T.; Shinya, A.; Matsuda, T.; Mihara, T.; Koide, N. Heat curing of UTMA-based hybrid resin: Effects on the degree of conversion and cytotoxicity. Odontology 2004, 92, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Takeshige, F.; Kinomoto, Y.; Torii, M. Additional heat-curing of light-cured composite resin for inlay restoration. J. Osaka Univ. Dent. Sch. 1995, 35, 59–66. [Google Scholar] [PubMed]
- Breeding, L.C.; Dixon, D.L.; Caughman, W.F. The curing potential of light-activated composite resin luting agents. J. Prosthet. Dent. 1991, 65, 512–518. [Google Scholar] [CrossRef]
- Pick, B.; Gonzaga, C.C.; Junior, W.S.; Kawano, Y.; Braga, R.R.; Cardoso, P.E. Influence of curing light attenuation caused by aesthetic indirect restorative materials on resin cement polymerization. Eur. J. Dent. 2010, 4, 314–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuguimiya, R.N.; Rode, K.M.; Carneiro, P.M.; Aranha, A.C.; Turbino, M.L. Influence of Curing Units and Indirect Restorative Materials on the Hardness of Two Dual-curing Resin Cements Evaluated by the Nanoindentation Test. J. Adhes. Dent. 2015, 17, 243–248. [Google Scholar]
- Myers, M.L.; Caughman, W.F.; Rueggeberg, F.A. Effect of restoration composition, shade, and thickness on the cure of a photoactivated resin cement. J. Prosthodont. 1994, 3, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Alovisi, M.; Scotti, N.; Comba, A.; Manzon, E.; Farina, E.; Pasqualini, D.; Michelotto Tempesta, R.; Breschi, L.; Cadenaro, M. Influence of polymerization time on properties of dual-curing cements in combination with high translucency monolithic zirconia. J. Prosthodont. Res. 2018, 62, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Leprince, J.G.; Palin, W.M.; Hadis, M.A.; Devaux, J.; Leloup, G. Progress in dimethacrylate-based dental composite technology and curing efficiency. Dent. Mater. 2013, 29, 139–156. [Google Scholar] [CrossRef]
- D’Arcangelo, C.; Vanini, L.; Rondoni, G.D.; Pirani, M.; Vadini, M.; Gattone, M.; De Angelis, F. Wear properties of a novel resin composite compared to human enamel and other restorative materials. Oper Dent. 2014, 39, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Trubiani, O.; Caputi, S.; Di Iorio, D.; D’Amario, M.; Paludi, M.; Giancola, R.; Di Nardo Di Maio, F.; De Angelis, F.; D’Arcangelo, C. The cytotoxic effects of resin-based sealers on dental pulp stem cells. Int. Endod. J. 2010, 43, 646–653. [Google Scholar] [CrossRef]
- Tsai, P.C.; Meyers, I.A.; Walsh, L.J. Depth of cure and surface microhardness of composite resin cured with blue LED curing lights. Dent. Mater. 2004, 20, 364–369. [Google Scholar] [CrossRef]
- Reges, R.V.; Moraes, R.R.; Correr, A.B.; Sinhoreti, M.A.; Correr-Sobrinho, L.; Piva, E.; Nouer, P.R. In-depth polymerization of dual-cured resin cement assessed by hardness. J. Biomater. Appl. 2008, 23, 85–96. [Google Scholar] [CrossRef]
- Rasetto, F.H.; Driscoll, C.F.; von Fraunhofer, J.A. Effect of light source and time on the polymerization of resin cement through ceramic veneers. J. Prosthodont. 2001, 10, 133–139. [Google Scholar] [CrossRef]
- Hooshmand, T.; Mahmoodi, N.; Keshvad, A. Microhardness of a resin cement polymerized by light-emitting diode and halogen lights through ceramic. J. Prosthodont. 2009, 18, 411–416. [Google Scholar] [CrossRef]
- Cho, S.H.; Lopez, A.; Berzins, D.W.; Prasad, S.; Ahn, K.W. Effect of Different Thicknesses of Pressable Ceramic Veneers on Polymerization of Light-cured and Dual-cured Resin Cements. J. Contemp. Dent. Pract. 2015, 16, 347–352. [Google Scholar] [CrossRef]
- Lee, J.W.; Cha, H.S.; Lee, J.H. Curing efficiency of various resin-based materials polymerized through different ceramic thicknesses and curing time. J. Adv. Prosthodont. 2011, 3, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Cadenaro, M.; Maravic, T.; Comba, A.; Mazzoni, A.; Fanfoni, L.; Hilton, T.; Ferracane, J.; Breschi, L. The role of polymerization in adhesive dentistry. Dent. Mater. 2019, 35, e1–e22. [Google Scholar] [CrossRef]
- Rueggeberg, F.A. State-of-the-art: Dental photocuring—A review. Dent. Mater. 2011, 27, 39–52. [Google Scholar] [CrossRef]
- Miyazaki, M.; Hattori, T.; Ichiishi, Y.; Kondo, M.; Onose, H.; Moore, B.K. Evaluation of curing units used in private dental offices. Oper Dent. 1998, 23, 50–54. [Google Scholar] [PubMed]
- Kramer, N.; Lohbauer, U.; Garcia-Godoy, F.; Frankenberger, R. Light curing of resin-based composites in the LED era. Am. J. Dent. 2008, 21, 135–142. [Google Scholar] [PubMed]
- Gomes de Araujo-Neto, V.; Sebold, M.; Fernandes de Castro, E.; Feitosa, V.P.; Giannini, M. Evaluation of physico-mechanical properties and filler particles characterization of conventional, bulk-fill, and bioactive resin-based composites. J. Mech. Behav. Biomed. Mater. 2021, 115, 104288. [Google Scholar] [CrossRef] [PubMed]
- Morresi, A.L.; D’Amario, M.; Monaco, A.; Rengo, C.; Grassi, F.R.; Capogreco, M. Effects of critical thermal cycling on the flexural strength of resin composites. J. Oral Sci. 2015, 57, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, E.; Wang, R.; Zhu, X.X. Correlation of resin viscosity and monomer conversion to filler particle size in dental composites. Dent. Mater. 2018, 34, 1501–1508. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, A.S.; Labruna Moreira, A.D.; de Albuquerque, P.P.; de Menezes, L.R.; Pfeifer, C.S.; Schneider, L.F. Effect of monomer type on the CC degree of conversion, water sorption and solubility, and color stability of model dental composites. Dent. Mater. 2017, 33, 394–401. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Resin Composite | Resin Matrix | Filler | Content % (w/v) | Manufacturer |
|---|---|---|---|---|---|
| ENA | Enamel Plus HRI (UD3 shade) (Batch n. 2014001144) | BisGMA, UDMA, TEGMA | Glass filler, SiO2 | 75/53 | Micerium S.p.A. (Avegno, Genova, Italy) |
| AUR | AURA SDI (MC3 shade) (Batch n. 130810) | BisGMA, UDMA, BisEMA | Ba–Al–B–Si glass, Ba glass | 78/63 | SDI Limited (Bayswater, Australia) |
| LCU | LCU Type | Output (mW/cm2) | Tip Diameter (mm) | Manufacturer |
|---|---|---|---|---|
| Demetron LC | QTH | 600 | 7.9 | Kerr Corporation, (Orange, CA, USA) |
| Bluephase C8 | LED | 800 | 9.8 | Ivoclar Vivadent AG (Schaan, Liechtenstein) |
| Starlight Uno | LED | 1500 | 8.0 | Mectron S.p.A. (Genova, Italy) |
| ENA Group | |||||
| Factor | Degrees of Freedom | Sum of Squares | Mean Squares | F | p |
| Curing Time | 3 | 100,050.491 | 33,350.164 | 853.147 | <0.001 |
| Overlay Thickness | 2 | 24,272.817 | 12,136.409 | 310.468 | <0.001 |
| LCU | 2 | 8374.910 | 4187.455 | 107.121 | <0.001 |
| Curing Time × Overlay Thickness | 6 | 1276.274 | 212.712 | 5.441 | <0.001 |
| Curing Time × LCU | 6 | 1057.676 | 176.279 | 4.509 | <0.001 |
| Overlay Thickness × LCU | 4 | 2026.656 | 506.664 | 12.961 | <0.001 |
| Curing Time × Overlay Thickness × LCU | 12 | 1529.133 | 127.428 | 3.260 | <0.001 |
| Residual | 288 | 11,258.136 | 39.091 | ||
| Total | 323 | 149,846.094 | 463.920 | ||
| AUR Group | |||||
| Factor | Degrees of Freedom | Sum of Squares | Mean Squares | F | p |
| Curing Time | 3 | 52,042.761 | 17,347.587 | 348.362 | <0.001 |
| Overlay Thickness | 2 | 9791.130 | 4895.565 | 98.309 | <0.001 |
| LCU | 2 | 6106.842 | 3053.421 | 61.317 | <0.001 |
| Curing Time × Overlay Thickness | 6 | 1146.312 | 191.052 | 3.837 | 0.001 |
| Curing Time × LCU | 6 | 1058.841 | 176.473 | 3.544 | 0.002 |
| Overlay Thickness × LCU | 4 | 336.654 | 84.163 | 1.690 | 0.152 |
| Curing Time × Overlay Thickness × LCU | 12 | 297.039 | 24.753 | 0.497 | 0.916 |
| Residual | 288 | 14,341.690 | 49.798 | ||
| Total | 323 | 85,121.267 | 263.533 | ||
| ENA Group (Optimum Micro-Hardness (OM) Reference Value Recorded in the Control Group = 85.1 (4.6) MPa) | ||||||||||||
| Curing Time with Halogen Unit (600 mW/cm2) | Curing Time with LED Unit (800 mW/cm2) | Curing Time with LED Unit (1500 mW/cm2) | ||||||||||
| Overlay Thickness | 10 s | 20 s | 40 s | 80 s | 10 s | 20 s | 40 s | 80 s | 10 s | 20 s | 40 s | 80 s |
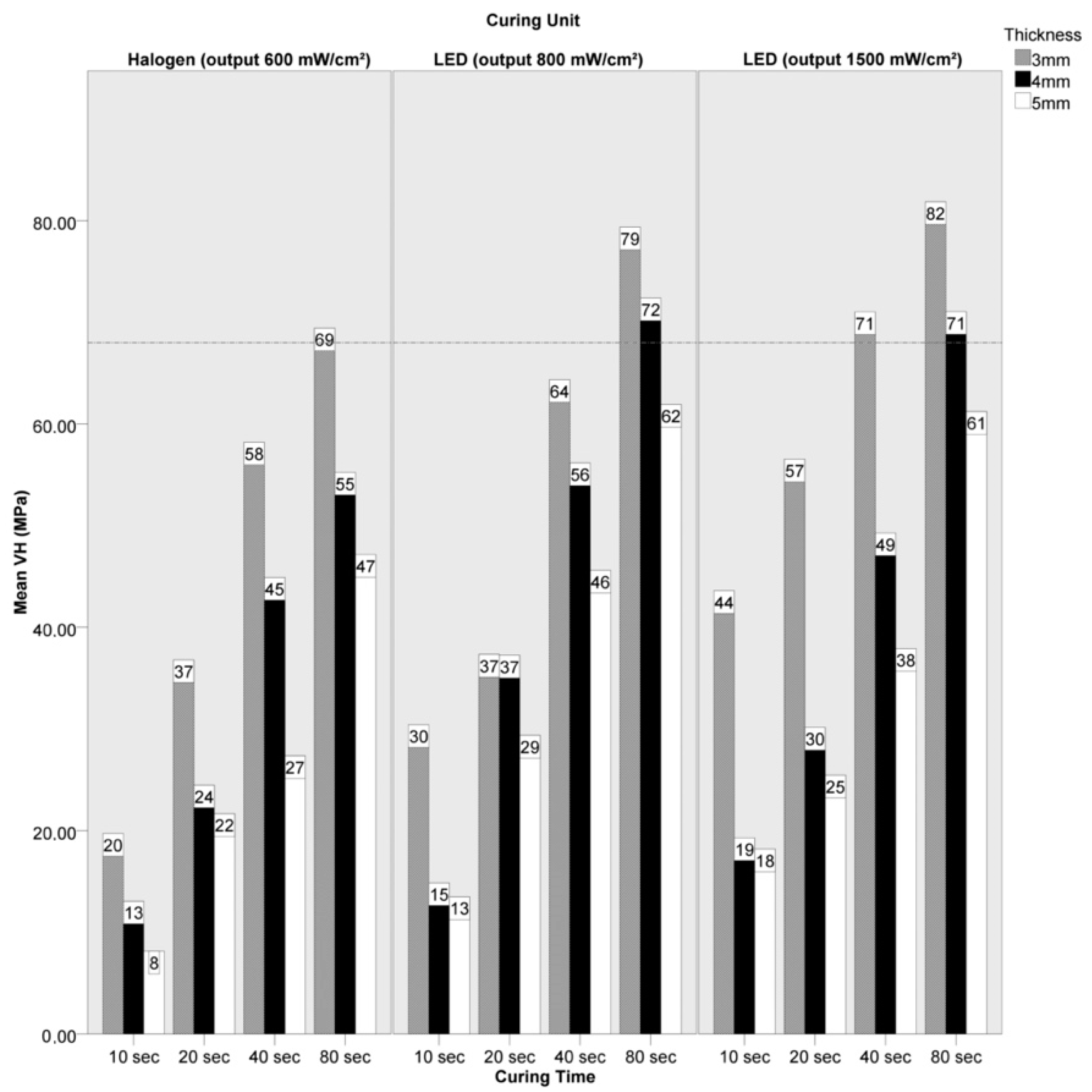
| 3 mm | 19.7 d1 (2.8) | 36.8 c1 (7.6) | 58.2 b1 (5.0) | 69.4 a1 (6.7) | 30.4 d1 (5.8) | 37.3 c1 (11.0) | 64.4 b1 (8.9) | 79.4 a1 (8.7) | 43.6 d1 (4.8) | 56.5 c1 (6.1) | 71.0 b1 (2.8) | 82.3 a1 (4.0) |
| 4 mm | 13.1 d2 (2.2) | 24.5 c2 (5.5) | 44.9 b2 (7.4) | 55.2 a2 (2.4) | 14.9 d2 (3.8) | 37.2 c1 (8.8) | 56.2 b2 (7.2) | 72.4 a2 (3.0) | 19.3 d2 (5.1) | 30.2 c2 (7.0) | 49.3 b2 (7.2) | 71.0 a2 (4.0) |
| 5 mm | 8.1 d2 (4.8) | 21.7 c2 (6.4) | 27.4 b3 (7.3) | 47.2 a3 (8.6) | 13.5 d2 (5.5) | 29.4 c1 (7.2) | 45.6 b3 (5.3) | 61.9 a3 (7.4) | 18.2 d2 (8.3) | 25.5 c2 (3.4) | 37.9 b3 (4.4) | 61.3 a3 (5.9) |
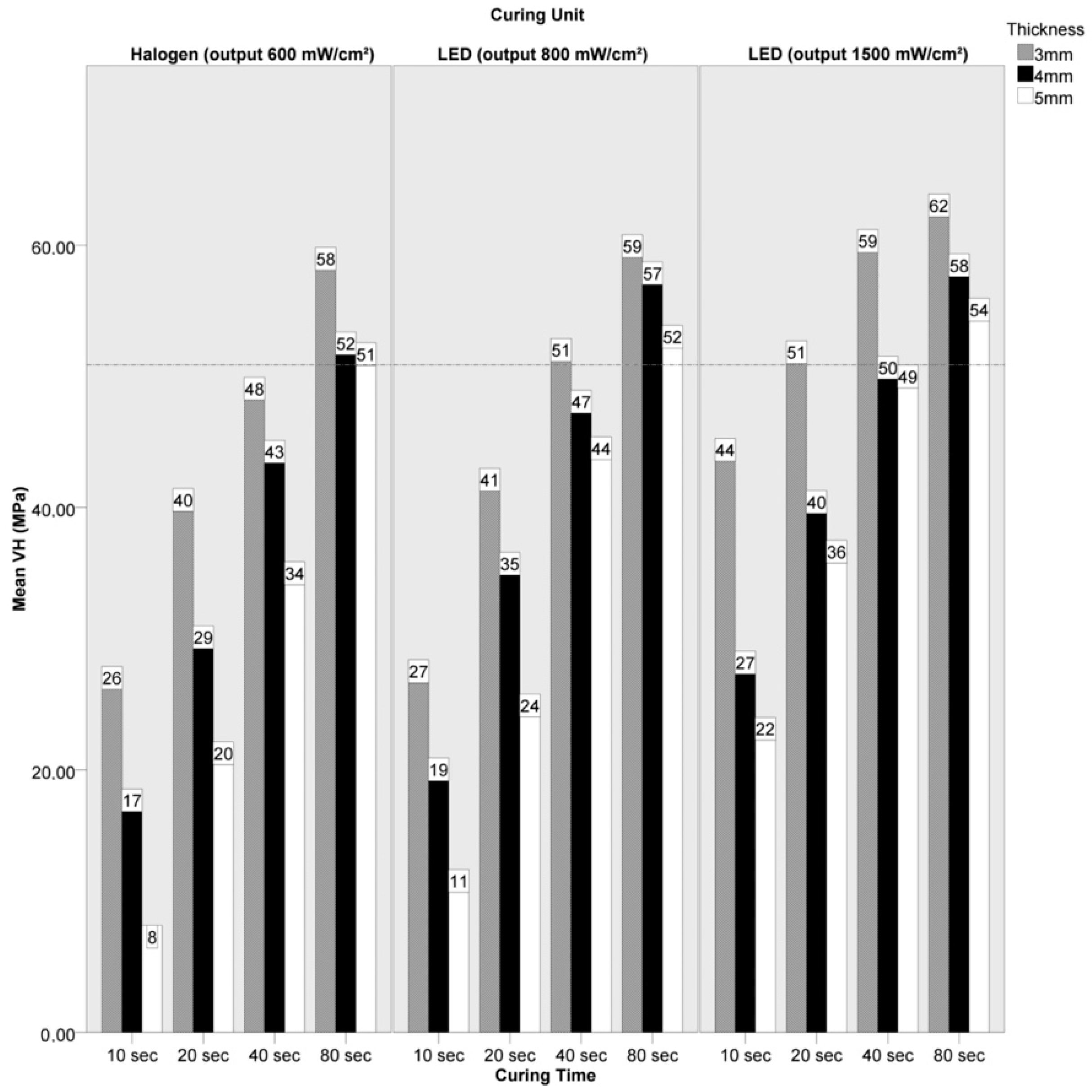
| AUR Group (Optimum Micro-Hardness (OM) Reference Value Recorded in the Control Group = 63.6 (2.3) MPa) | ||||||||||||
| Curing Time with Halogen Unit (600 mW/cm2) | Curing Time with LED Unit (800 mW/cm2) | Curing Time with LED Unit (1500 mW/cm2) | ||||||||||
| Overlay Thickness | 10 s | 20 s | 40 s | 80 s | 10 s | 20 s | 40 s | 80 s | 10 s | 20 s | 40 s | 80 s |
| 3 mm | 26.2 d1 (4.2) | 39.7 c1 (5.7) | 48.2 b1 (4.3) | 58.1 a1 (3.0) | 26.7 d1 (22.0) | 41.3 c1 (3.2) | 51.1 b1 (4.6) | 59.1 a1 (5.3) | 43.5 d1 (4.0) | 51.0 c1 (3.6) | 59.4 b1 (4.2) | 62.6 a1 (3.2) |
| 4 mm | 16.8 d2 (21.3) | 29.2 c2 (5.5) | 43.4 b2 (4.5) | 51.6 a2 (8.9) | 19.2 d2 (4.8) | 34.8 c2 (10.0) | 47.2 b2 (4.9) | 57.0 a2 (2.6) | 27.3 d2 (2.8) | 39.6 c2 (2.4) | 49.8 b2 (4.1) | 57.3 a2 (4.1) |
| 5 mm | 8.2 d3 (4.8) | 20.4 c3 (6.6) | 34.1 b3 (5.7) | 50.8 a3 (3.6) | 10.7 d3 (2.1) | 24.0 c3 (3.4) | 43.6 b3 (4.8) | 52.1 a3 (7.0) | 22.3 d2 (5.0) | 35.8 c2 (9.4) | 49.1 b2 (4.3) | 54.5 a2 (2.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Angelis, F.; Vadini, M.; Capogreco, M.; D’Arcangelo, C.; D’Amario, M. Effect of Light-Sources and Thicknesses of Composite Onlays on Micro-Hardness of Luting Composites. Materials 2021, 14, 6849. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14226849
De Angelis F, Vadini M, Capogreco M, D’Arcangelo C, D’Amario M. Effect of Light-Sources and Thicknesses of Composite Onlays on Micro-Hardness of Luting Composites. Materials. 2021; 14(22):6849. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14226849
Chicago/Turabian StyleDe Angelis, Francesco, Mirco Vadini, Mario Capogreco, Camillo D’Arcangelo, and Maurizio D’Amario. 2021. "Effect of Light-Sources and Thicknesses of Composite Onlays on Micro-Hardness of Luting Composites" Materials 14, no. 22: 6849. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14226849