
Bone Regeneration of Critical-Size Calvarial Defects in Rats Using Highly Pressed Nano-Apatite/Collagen Composites

 , and
, and 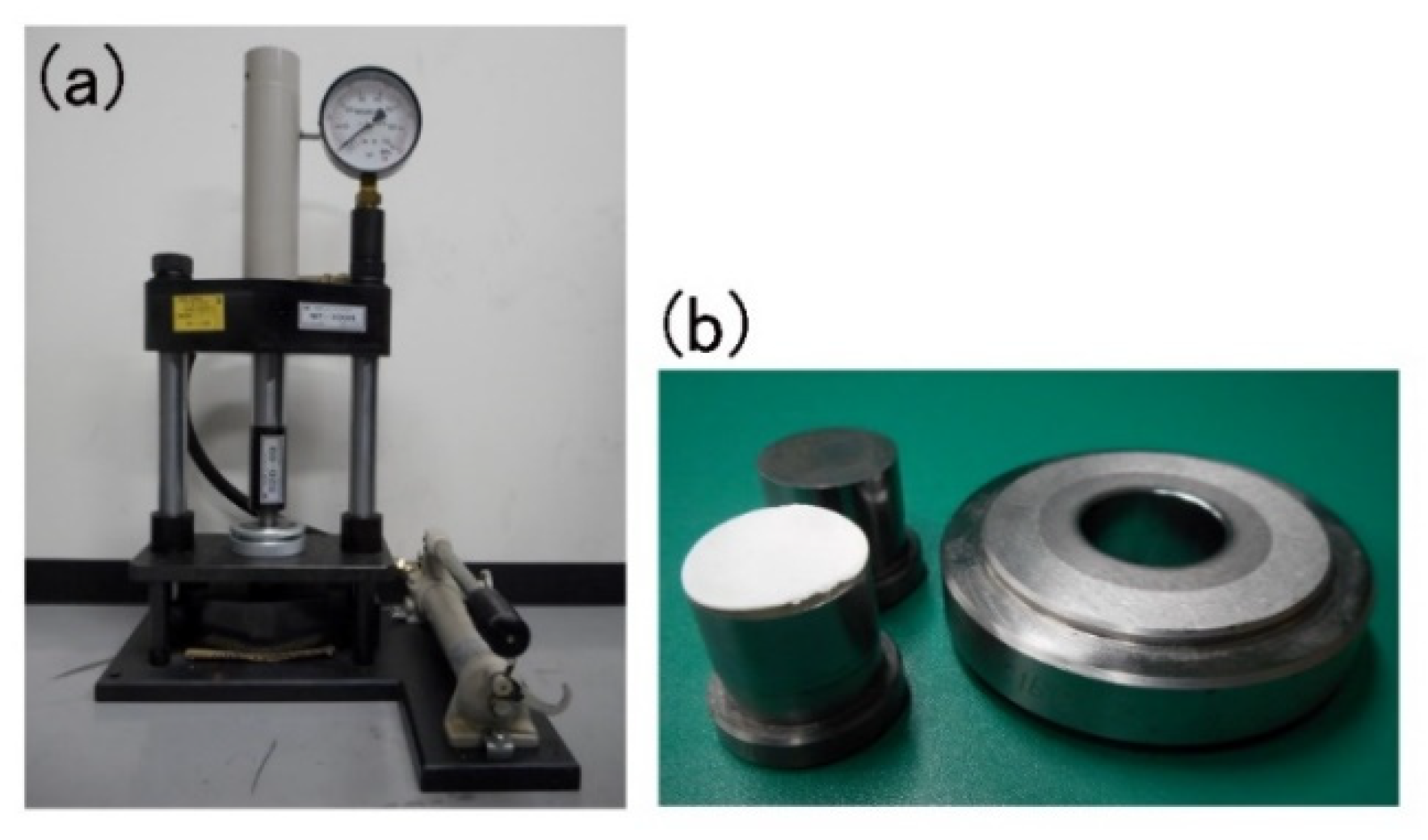{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of P-nHAP/Col Composite Material
2.2. Animal Experiments
2.3. Micro-CT Imaging
2.4. Histological Observations
3. Results
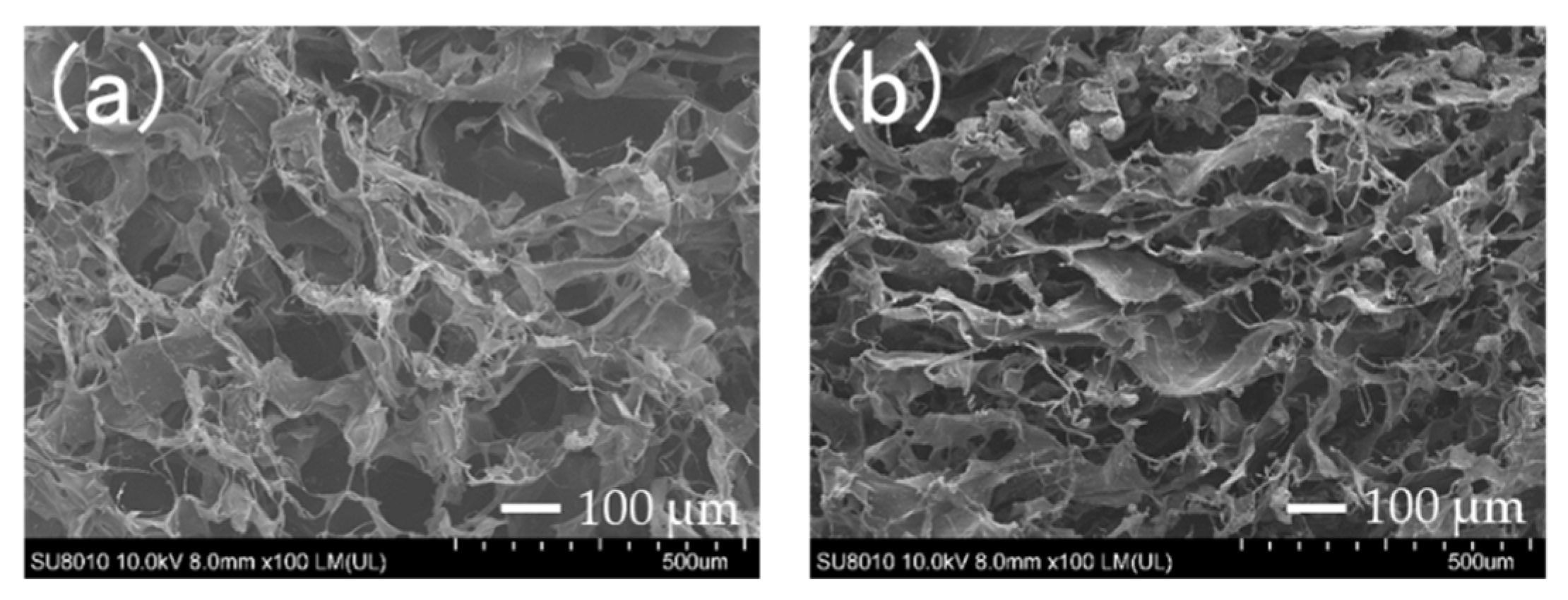
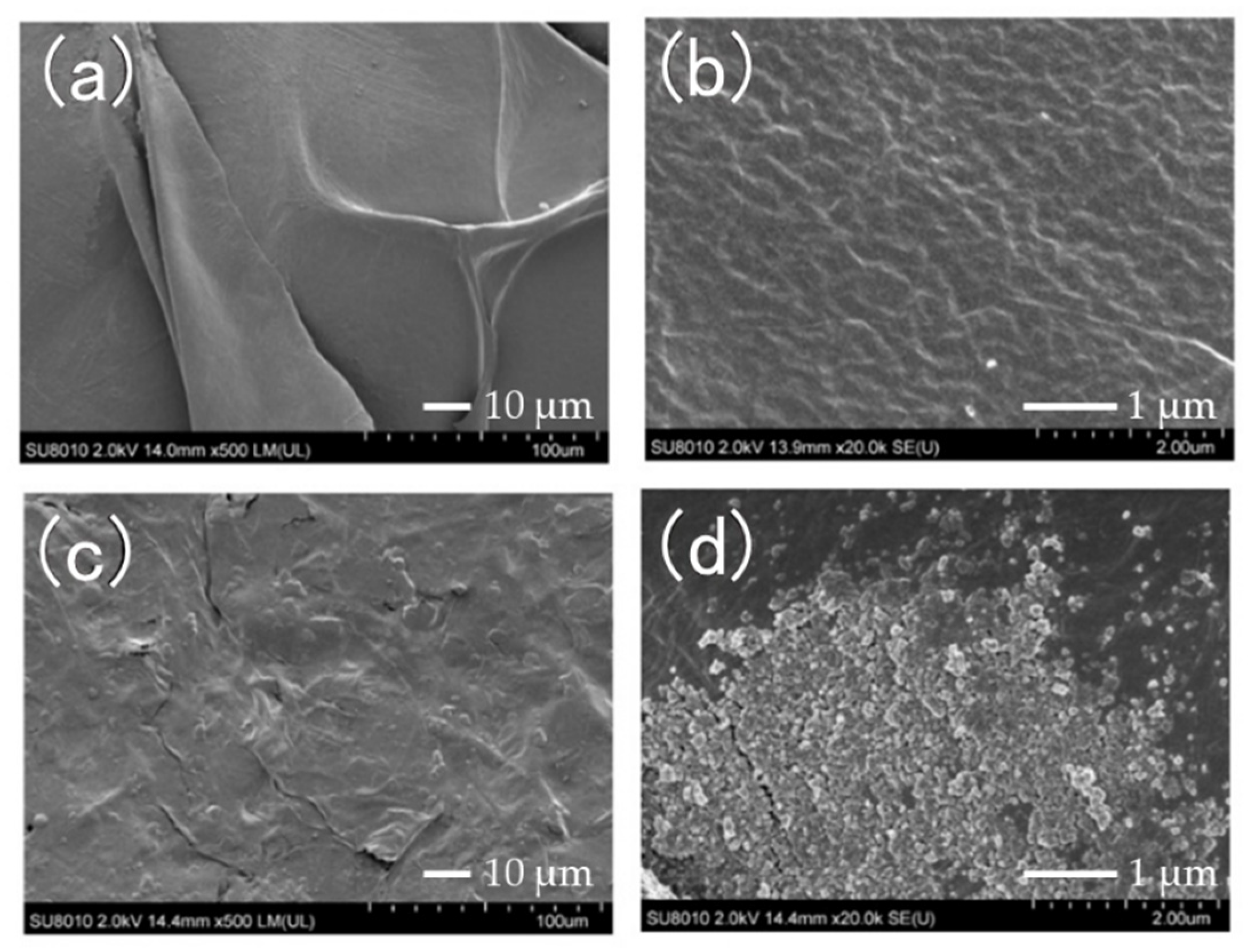
3.1. Scanning Electron Microscopy (SEM) Observations
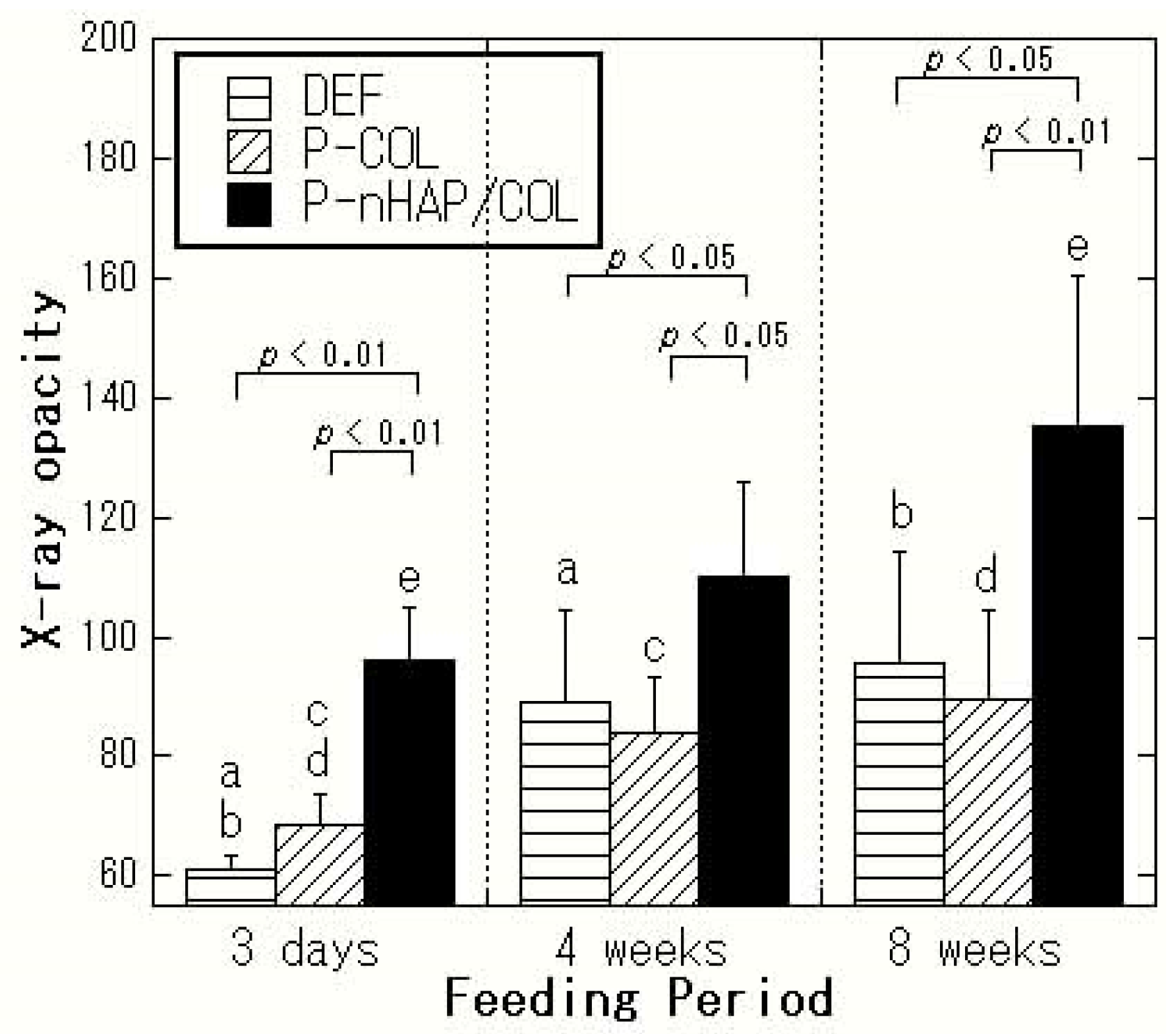
3.2. Micro-CT
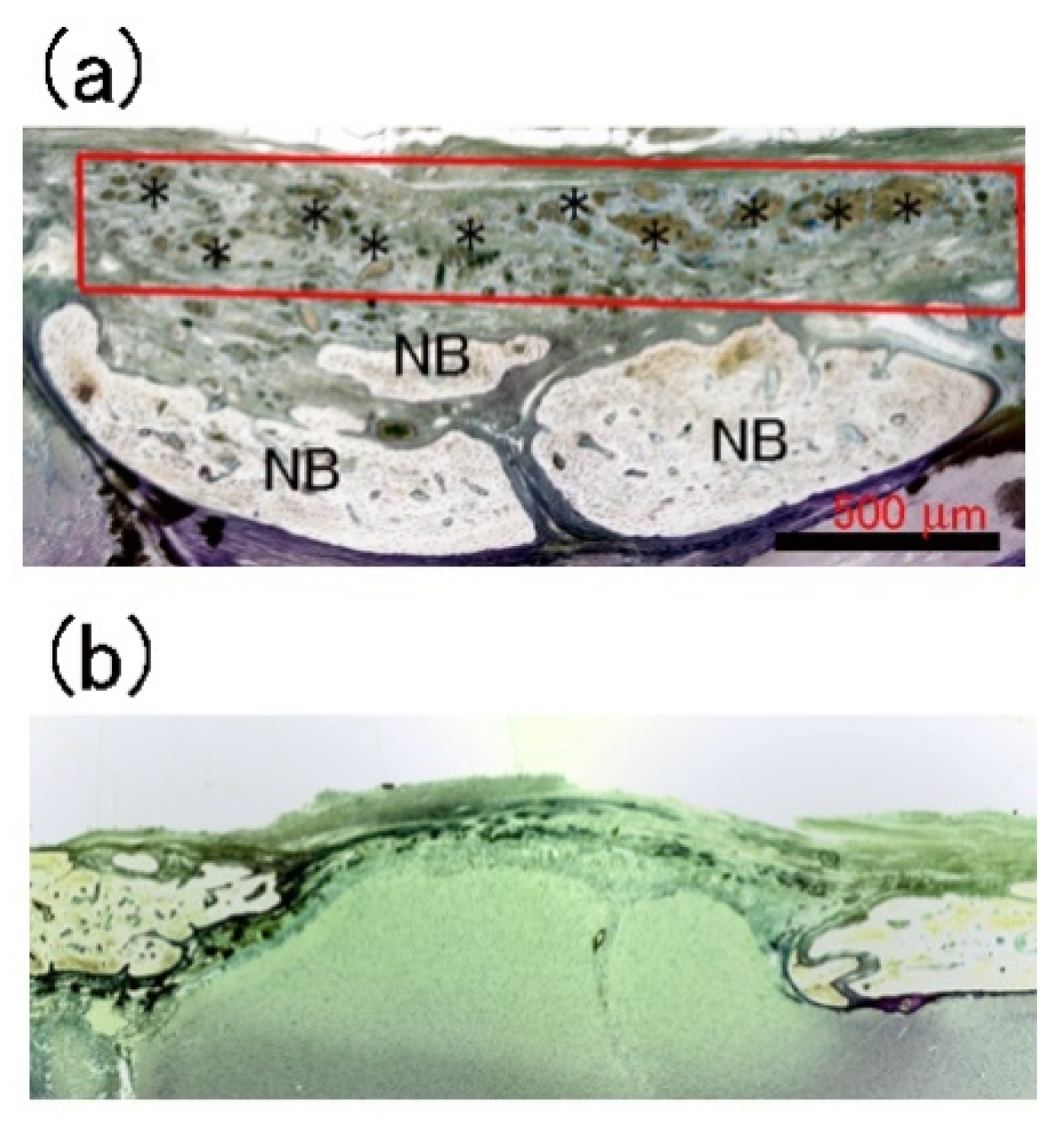
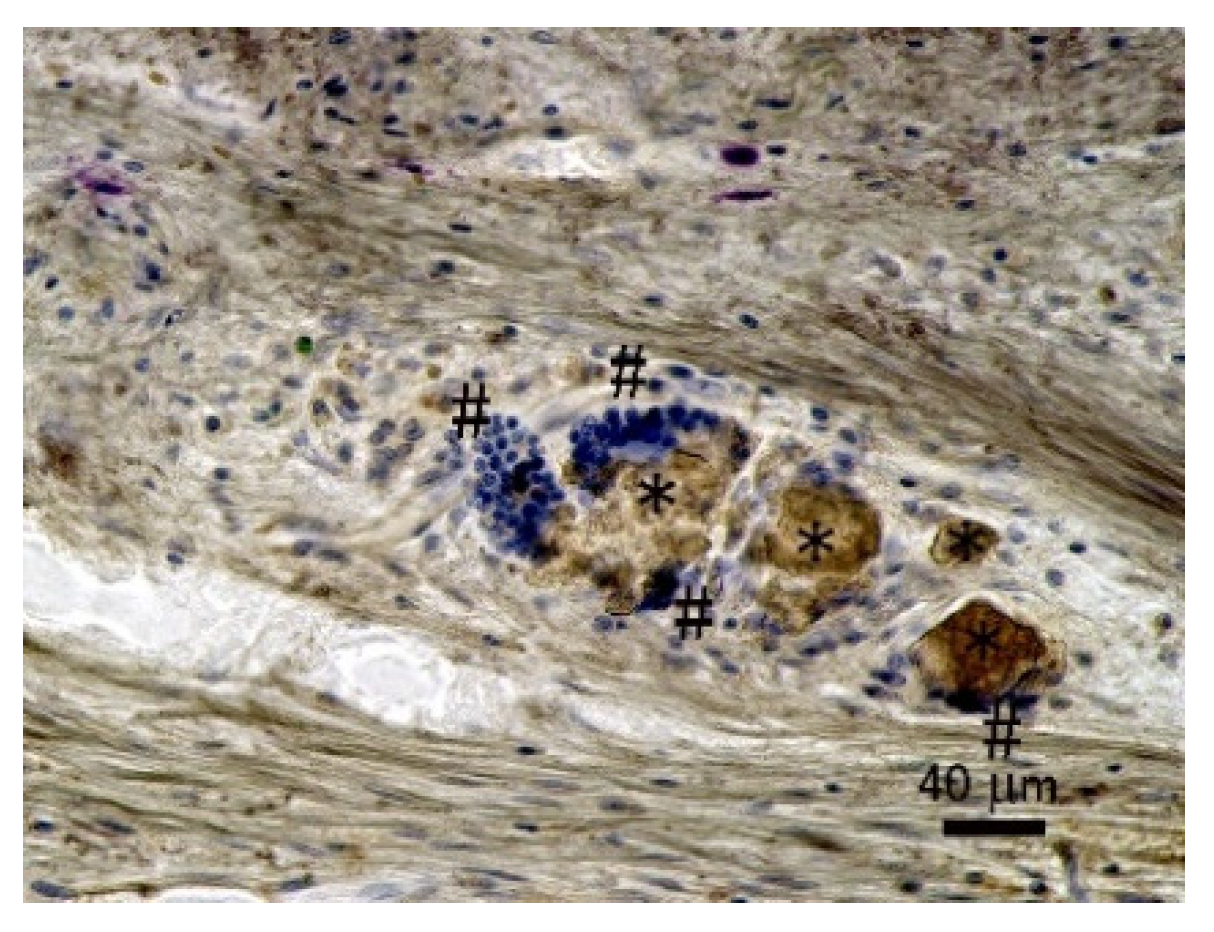
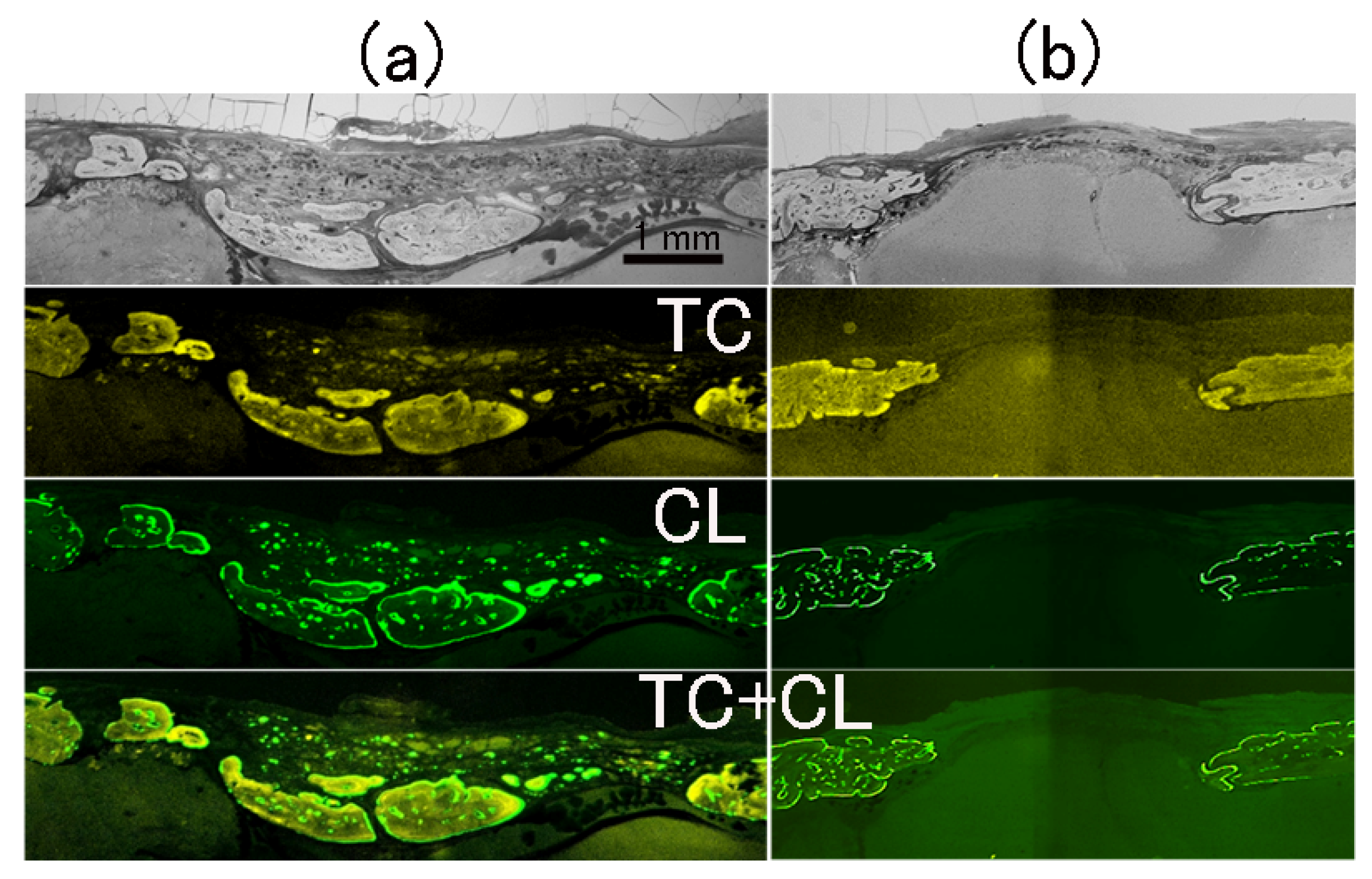
3.3. Histological Observations
4. Discussion
5. Conclusions
- P-nHAP/COL composite was prepared by mechanical mixing, freeze drying, dehydrothermal cross-linking, and hydraulic press. The composite was punched into critical-size disks.
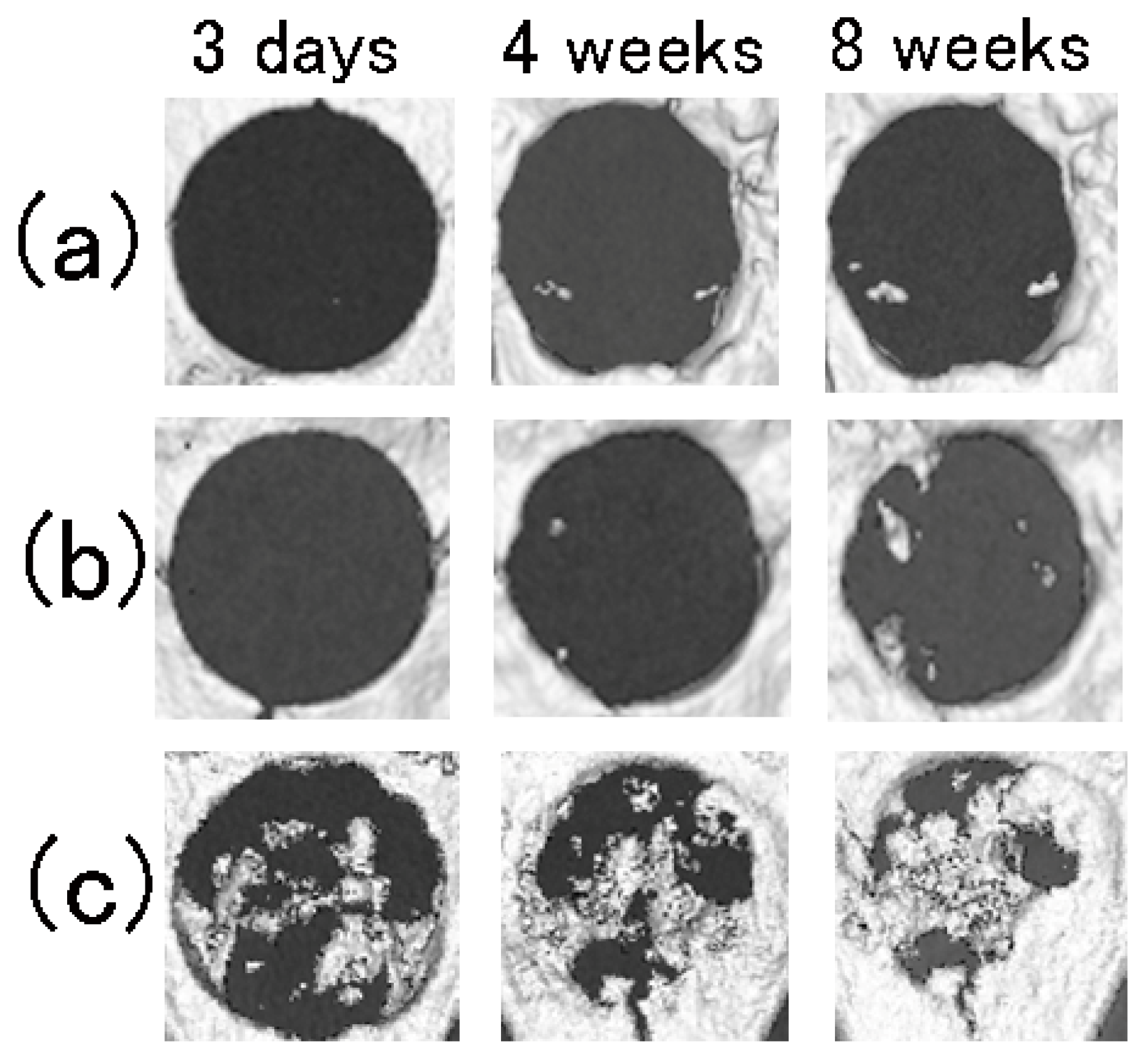
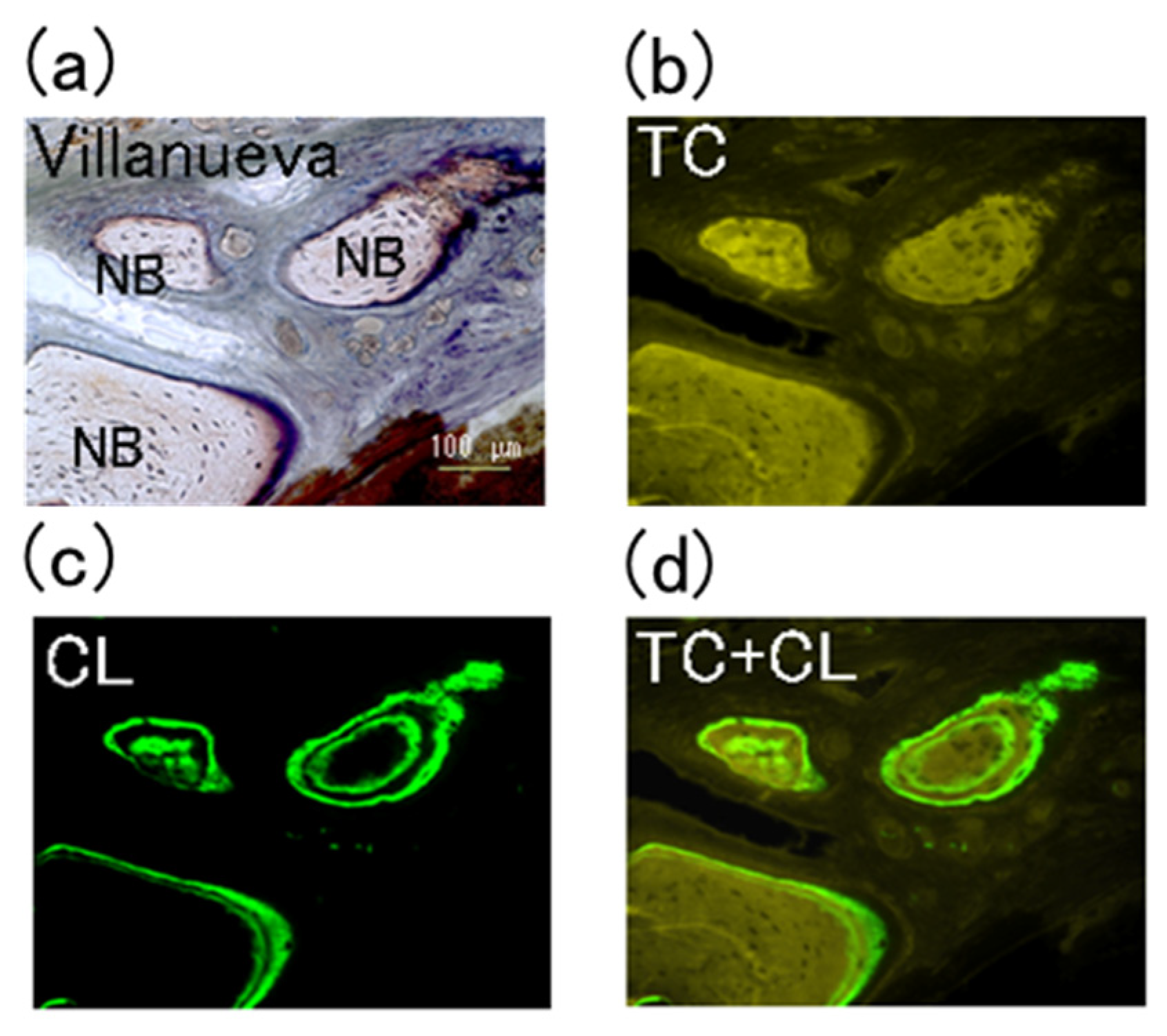
- P-nHAP/COL disks were implanted into rat critical-size cranial defects, and bone regeneration status was evaluated by micro-CT imaging and histological examination. After 8 weeks of observation, P-nHAP/COL was highly osteo-conductive in vivo. The defect zone implanted with P-nHAP/COL rapidly became X-ray opaque, indicating newly formed bone. Active bone remodeling composed of both osteoblasts and osteoclasts was histologically observed.
- P-nHAP/COL could be used as a new osteo-conductive bone substitute in dental implants, although further studies using larger animals (e.g., rabbits and dogs) are needed prior to clinical testing.
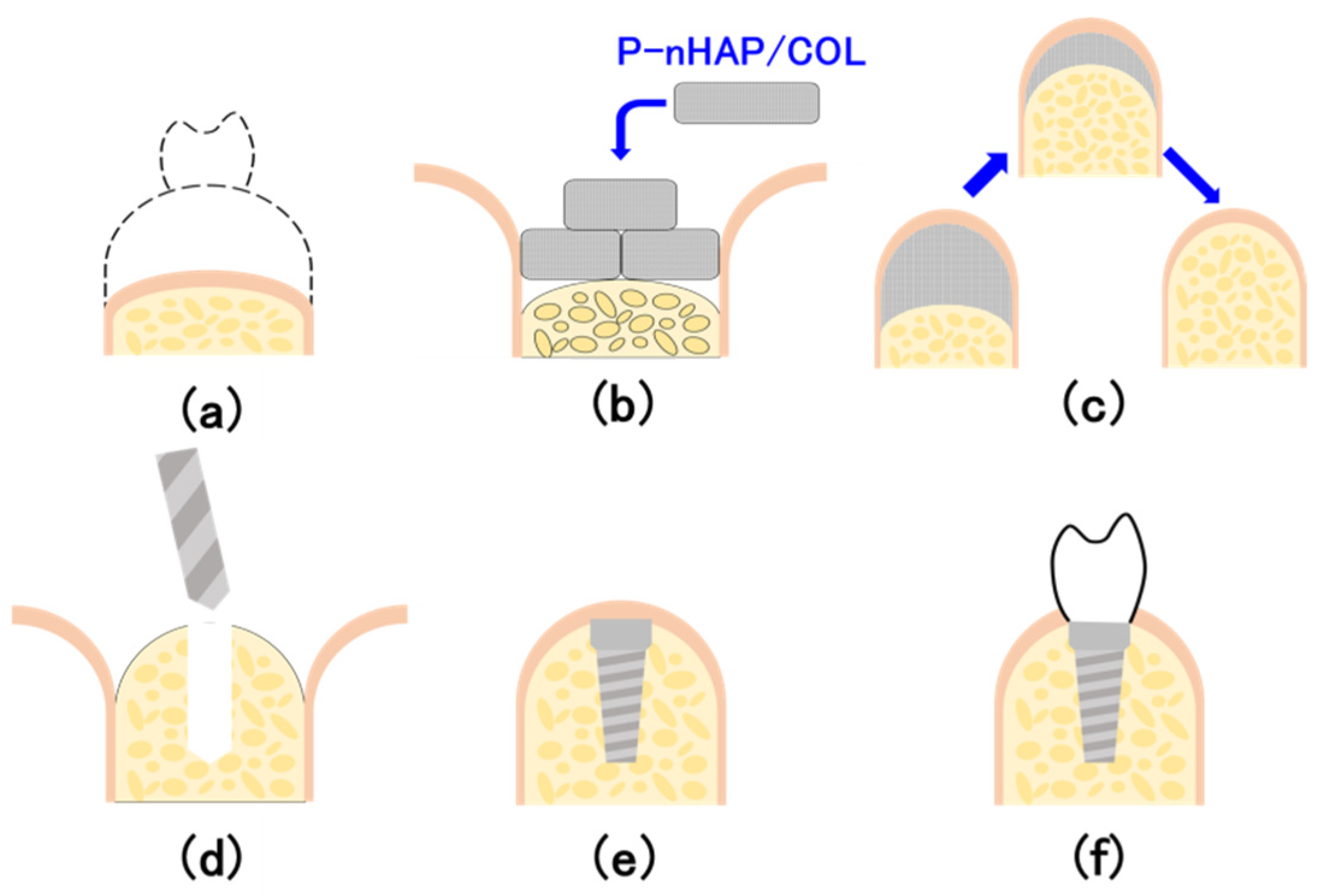
- P-nHAP/COL would be applied to bone-shallow area, followed by dental implant treatment (Figure 10).
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| ATPase | Adenosine triphosphatase |
| CL | Calcein |
| COL | Collagen |
| DEF | Defect only |
| HAP | Hydroxyapatite |
| HAP/COL | Hydroxyapatite/collagen |
| micro-CT | micro-computed tomography |
| nHAP | Nano-hydroxyapatite |
| PBS | Phosphate-buffered saline |
| P-COL | Pressed collagen |
| P-nHAP/COL | Pressed nano-hydroxyapatite/collagen |
| RANK | Receptor activator of nuclear factor κB |
| RANKL | Receptor activator of nuclear factor κB ligand |
| ROI | Region of interest |
| SEM | Scanning Electron Microscopy |
| TC | Tetracycline |
| VFF | Vextus Factor-compiled storage files |
| 3D | Three-Dimensional |
References
- Kim, D.M.; Nevins, M.L.; Lin, Z.; Fateh, A.; Kim, S.-W.; Schupbach, P.; Nevins, M. The clinical and histologic outcome of dental implant in large ridge defect regenerated with alloplast: A randomized controlled preclinical trial. J. Oral Implantol. 2013, 39, 148–153. [Google Scholar] [CrossRef]
- Rogers, G.F.; Greene, A.K. Autogenous bone graft: Basic science and clinical implications. J. Craniofac. Surg. 2012, 23, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Chavda, S.; Levin, L. Human studies of vertical and horizontal alveolar ridge augmentation comparing different types of bone graft materials: A systematic review. J. Oral Implantol. 2018, 44, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Kattimani, V.S.; Chakravarthi, P.S.; Prasad, L.K. Biograft block hydroxyapatite: A ray of hope in the reconstruction of maxillofacial defects. J. Craniofac. Surg. 2016, 27, 247–252. [Google Scholar] [CrossRef]
- Ishikawa, K.; Miyamoto, Y.; Tsuchiya, A.; Hayashi, K.; Tsuru, K.; Ohe, G. Physical and histological comparison of hydroxyapatite, carbonate apatite, and β-tricalcium phosphate bone substitutes. Materials 2018, 11, 1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roh, H.-S.; Myung, S.W.; Jung, S.C.; Kim, B.H. Fabrication of 3D scaffolds with nano-hydroxyapatite for improving the preosteoblast cell-biological performance. J. Nanosci. Nanotechnol. 2015, 15, 5585–5588. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.-W.; Jang, H.L.; Nam, K.T.; Beck, G.R., Jr. Nano-hydroxyapatite modulates osteoblast lineage commitment by stimulation of DNA methylation and regulation of gene expression. Biomaterials 2015, 65, 32–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Wang, C.; Chen, Q.; Liu, H.; Deng, C.; Ling, P.; Cui, F.-Z. Effects of the bilayer nano-hydroxyapatite/mineralized collagen-guided bone regeneration membrane on site preservation in dogs. J. Biomater. Appl. 2017, 32, 242–256. [Google Scholar] [CrossRef]
- Park, H.; Jaeyoung, R.; Jung, S.; Park, H.; Oh, H.; Kook, M. Effect of hydroxyapatite nanoparticles and nitrogen plasma treatment on osteoblast biological behaviors of 3D-printed HDPE scaffold for bone tissue regeneration applications. Materials 2022, 15, 827. [Google Scholar] [CrossRef]
- Choi, J.-W.; Kim, J.-W.; Jo, I.-H.; Koh, Y.-H.; Kim, H.-E. Novel self-assembly-induced gelation for nanofibrous collagen/hydroxyapatite composite microspheres. Materials 2017, 10, 1110. [Google Scholar] [CrossRef] [Green Version]
- Hatakeyama, W.; Taira, M.; Takafuji, K.; Kihara, H.; Kondo, H. Bone regeneration trial of rat critical-size calvarial defects using nano-apatite/collagen composites. Nano Biomed. 2013, 5, 95–103. [Google Scholar]
- Taira, M.; Nezu, T.; Sasaki, K.; Saitoh, S.; Kagiya, T.; Harada, H.; Takada, Y.; Araki, Y. Preparation and in vivo evaluation of apatite/collagen packed composite by alternate immersion method and Newton press. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 90, 566–573. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, L.; Qiu, Y.; Fan, X.; Zhang, L.; Yu, Q. Valorization of cattle slaughtering industry by-products: Modification of the functional properties and structural characteristics of cowhide gelatin induced by high hydrostatic pressure. Gels 2022, 8, 243. [Google Scholar] [CrossRef]
- Chen, L.; Ma, L.; Zhou, M.; Liu, Y.; Zhang, Y. Effects of pressure on gelatinization of collagen and properties of extracted gelatins. Food Hydrocoll. 2014, 36, 316–322. [Google Scholar] [CrossRef]
- Itoh, H.; Wakisaka, Y.; Ohmura, Y.; Kuboki, Y. A new porous hydroxyapatite ceramic prepared by cold isostatic pressing and sintering synthesized flaky powder. Dent. Mater. J. 1994, 13, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Kalita, S.J.; Bose, S.; Hosick, H.L.; Bandyopadhyay, A. CaO--P2O5--Na2O-based sintering additives for hydroxyapatite (HAp) ceramics. Biomaterials 2004, 25, 2331–2339. [Google Scholar] [CrossRef]
- Buchi Suresh, M.; Biswas, P.; Mahender, V.; Johnson, R. Comparative evaluation of electrical conductivity of hydroxyapatite ceramics densified through ramp and hold, spark plasma and post sinter hot isostatic pressing routes. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 70, 364–370. [Google Scholar] [CrossRef]
- Ikeda, K.; Taira, M.; Yokota, J.; Hattori, M.; Ishisaki, A.; Kondo, H. Effects of addition of nano-hydroxyapatite to highly-pressed collagen on osteogenic differentiation in osteoblastic SaOS-2 cells. Nano Biomed. 2016, 8, 91–100. [Google Scholar]
- Qin, D.; Wang, N.; You, X.-G.; Zhang, A.-D.; Chen, X.-G.; Liu, Y. Collagen-based biocomposites inspired by bone hierarchical structures for advanced bone regeneration: Ongoing research and perspectives. Biomater. Sci. 2022, 10, 318–353. [Google Scholar] [CrossRef]
- Kim, R.-W.; Kim, J.-H.; Moon, S.-Y. Effect of hydroxyapatite on critical-sized defect. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 26. [Google Scholar] [CrossRef] [Green Version]
- Kotake, B.G.S.; Gonzaga, M.G.; Coutinho-Netto, J.; Ervolino, E.; de Figueiredo, F.A.T.; Issa, J.P.M. Bone repair of critical-sized defects in Wistar rats treated with autogenic, allogenic or xenogenic bone grafts alone or in combination with natural latex fraction F1. Biomed. Mater. 2018, 13, 25022. [Google Scholar] [CrossRef]
- Wang, D.; Tabassum, A.; Wu, G.; Deng, L.; Wismeijer, D.; Liu, Y. Bone regeneration in critical-sized bone defect enhanced by introducing osteoinductivity to biphasic calcium phosphate granules. Clin. Oral. Implants Res. 2017, 28, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.; Watson, M.; Callon, K.E.; Tuari, D.; Dray, M.; Naot, D.; Amirapu, S.; Munro, J.T.; Cornish, J.; Musson, D.S. Local application of lactoferrin promotes bone regeneration in a rat critical-sized calvarial defect model as demonstrated by micro-CT and histological analysis. J. Tissue Eng. Regen. Med. 2018, 12, e620–e626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Y.; Komasa, S.; Li, P.; Nishizaki, M.; Chen, L.; Terada, C.; Yoshimine, S.; Nishizaki, H.; Okazaki, J. Synergistic effect of nanotopography and bioactive ions on peri-implant bone response. Int. J. Nanomed. 2017, 12, 925–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatakeyama, W.; Taira, M.; Kihara, H.; Sasaki, M.; Kimura, S.; Kondo, H. Subcutaneous tissue reactions against nano-apatite collagen composites. Nano Biomed. 2012, 4, 118–124. [Google Scholar]
- Frost, H.M. Preparation of thin undercalcified bone sections by rapid manual method. Stain Technol. 1958, 33, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Hatakeyama, W.; Taira, M.; Ikeda, K.; Takafuji, K.; Kihara, H.; Kondo, H.; Hattori, M. In vivo evaluation of noble porous apatite disks implanted in rat critical-size calvarial defects by micro-CT and histological observations. J. Oral Tissue Eng. 2014, 12, 13–19. [Google Scholar]
- Watari, F.; Takashi, N.; Yokoyama, A.; Uo, M.; Akasaka, T.; Sato, Y.; Abe, S.; Totsuka, Y.; Tohji, K. Material nanosizing effect on living organisms: Non-specific, biointeractive, physical size effects. J. R. Soc. Interface 2009, 6, S371–S388. [Google Scholar] [CrossRef]
- Fang, C.-H.; Sun, C.-K.; Lin, Y.-W.; Hung, M.-C.; Lin, H.-Y.; Li, C.-H.; Lin, I.-P.; Chang, H.-C.; Sun, J.-S.; Chang, J.Z.-C. Metformin-incorporated gelatin/nano-hydroxyapatite scaffolds promotes bone regeneration in critical size rat alveolar bone defect model. Int. J. Mol. Sci. 2022, 23, 558. [Google Scholar] [CrossRef]
- Klar, R.M.; Duarte, R.; Dix-Peek, T.; Dickens, C.; Ferretti, C.; Ripamonti, U. Calcium ions and osteoclastogenesis initiate the induction of bone formation by coral-derived macroporous constructs. J. Cell. Mol. Med. 2013, 17, 1444–1457. [Google Scholar] [CrossRef]
- Ferreira, A.M.; Gentile, P.; Chiono, V.; Ciardelli, G. Collagen for bone tissue regeneration. Acta Biomater. 2012, 8, 3191–3200. [Google Scholar] [CrossRef] [PubMed]
- Wahl, D.A.; Czernuszka, J.T. Collagen-hydroxyapatite composites for hard tissue repair. Eur. Cells Mater. 2006, 11, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Miller, A. Collagen: The organic matrix of bone. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1984, 304, 455–477. [Google Scholar]
- Nesbitt, S.A.; Horton, M.A. Trafficking of matrix collagens through bone-resorbing osteoclasts. Science 1997, 276, 266–269. [Google Scholar] [CrossRef]
- Sahara, T.; Itoh, K.; Debari, K.; Sasaki, T. Specific biological functions of vacuolar-type H(+)-ATPase and lysosomal cysteine proteinase, cathepsin K, in osteoclasts. Anat. Rec. A Discov. Mol. Cell. Evol. Biol. 2003, 270, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Wu, J.; Xia, Y.; Yuan, Y.; Zhang, H.; Xu, S.; Lin, K. Loading BMP-2 on nanostructured hydroxyapatite microspheres for rapid bone regeneration. Int. J. Nanomed. 2018, 13, 4083–4092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Polman, M.; Mohammad, A.F.; Hermens, I.; Zhuang, Z.; Wang, H.; van den Beucken, J.J. Species-independent stimulation of osteogenic differentiation induced by osteoclasts. Biochem. Biophys. Res. Commun. 2022, 606, 149–155. [Google Scholar] [CrossRef]
- Issa, J.P.; Gonzaga, M.; Kotake, B.G.; de Lucia, C.; Ervolino, E.; Iyomasa, M. Bone repair of critical size defects treated with autogenic, allogenic, or xenogenic bone grafts alone or in combination with rhBMP-2. Clin. Oral Implants Res. 2016, 27, 558–566. [Google Scholar] [CrossRef]
- Ciapetti, G.; Di Pompo, G.; Avnet, S.; Martini, D.; Diez-Escudero, A.; Montufar, E.B.; Ginebra, M.P.; Baldini, N. Osteoclast differentiation from human blood precursors on biomimetic calcium-phosphate substrates. Acta Biomater. 2017, 50, 102–113. [Google Scholar] [CrossRef] [Green Version]
- Suda, T.; Kobayashi, K.; Jimi, E.; Udagawa, N.; Takahashi, N. The molecular basis of osteoclast differentiation and activation. Novartis Found. Symp. 2001, 232, 235–247. [Google Scholar]
- Ikeda, K.; Takeshita, S. Factors and mechanisms involved in the coupling from bone resorption to formation: How osteoclasts talk to osteoblasts. J. Bone Metab. 2014, 21, 163–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kylmaoja, E.; Nakamura, M.; Tuukkanen, J. Osteoclasts and remodeling based bone formation. Curr. Stem. Cell. Res. Ther. 2016, 11, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Mima, Y.; Fukumoto, S.; Koyama, H.; Okada, M.; Tanaka, S.; Shoji, T.; Emoto, M.; Furuzono, T.; Nishizawa, Y.; Inaba, M. Enhancement of cell-based therapeutic angiogenesis using a novel type of injectable scaffolds of hydroxyapatite-polymer nanocomposite microspheres. PLoS ONE 2012, 7, e35199. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.; Wang, T.; Zhu, J.; Cai, P. Osteoinduction of calcium phosphate ceramics in four kinds of animals for 1 year: Dog, rabbit, rat, and mouse. Transplant. Proc. 2016, 48, 1309–1314. [Google Scholar] [CrossRef]
- Shamsoddin, E.; Houshmand, B.; Golabgiran, M. Biomaterial selection for bone augmentation in implant dentistry: A systematic review. J. Adv. Pharm. Technol. Res. 2019, 10, 46–50. [Google Scholar]
- Zitzmann, N.U.; Schärer, P.; Marinello, C.P.; Schüpbach, P.; Berglundh, T. Alveolar ridge augmentation with Bio-Oss: A histologic study in humans. Int. J. Periodontics Restor. Dent. 2001, 21, 288–295. [Google Scholar]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatakeyama, W.; Taira, M.; Sawada, T.; Hoshi, M.; Hachinohe, Y.; Sato, H.; Takafuji, K.; Kihara, H.; Takemoto, S.; Kondo, H. Bone Regeneration of Critical-Size Calvarial Defects in Rats Using Highly Pressed Nano-Apatite/Collagen Composites. Materials 2022, 15, 3376. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15093376
Hatakeyama W, Taira M, Sawada T, Hoshi M, Hachinohe Y, Sato H, Takafuji K, Kihara H, Takemoto S, Kondo H. Bone Regeneration of Critical-Size Calvarial Defects in Rats Using Highly Pressed Nano-Apatite/Collagen Composites. Materials. 2022; 15(9):3376. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15093376
Chicago/Turabian StyleHatakeyama, Wataru, Masayuki Taira, Tomofumi Sawada, Miki Hoshi, Yuki Hachinohe, Hirotaka Sato, Kyoko Takafuji, Hidemichi Kihara, Shinji Takemoto, and Hisatomo Kondo. 2022. "Bone Regeneration of Critical-Size Calvarial Defects in Rats Using Highly Pressed Nano-Apatite/Collagen Composites" Materials 15, no. 9: 3376. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15093376