Effects of Composite Supplement Containing Collagen Peptide and Ornithine on Skin Conditions and Plasma IGF-1 Levels—A Randomized, Double-Blind, Placebo-Controlled Trial


Abstract
:1. Introduction
2. Results
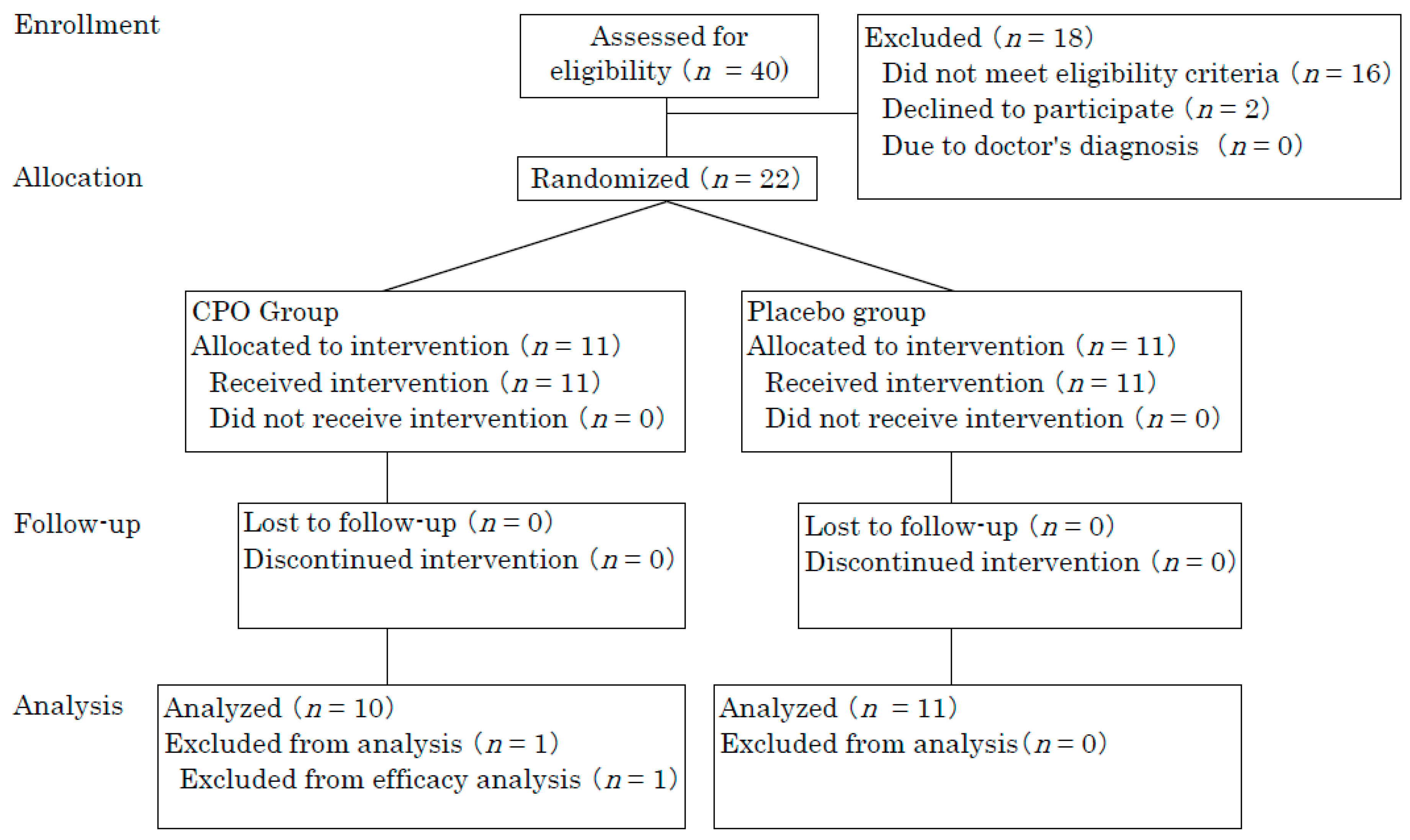
2.1. Participants
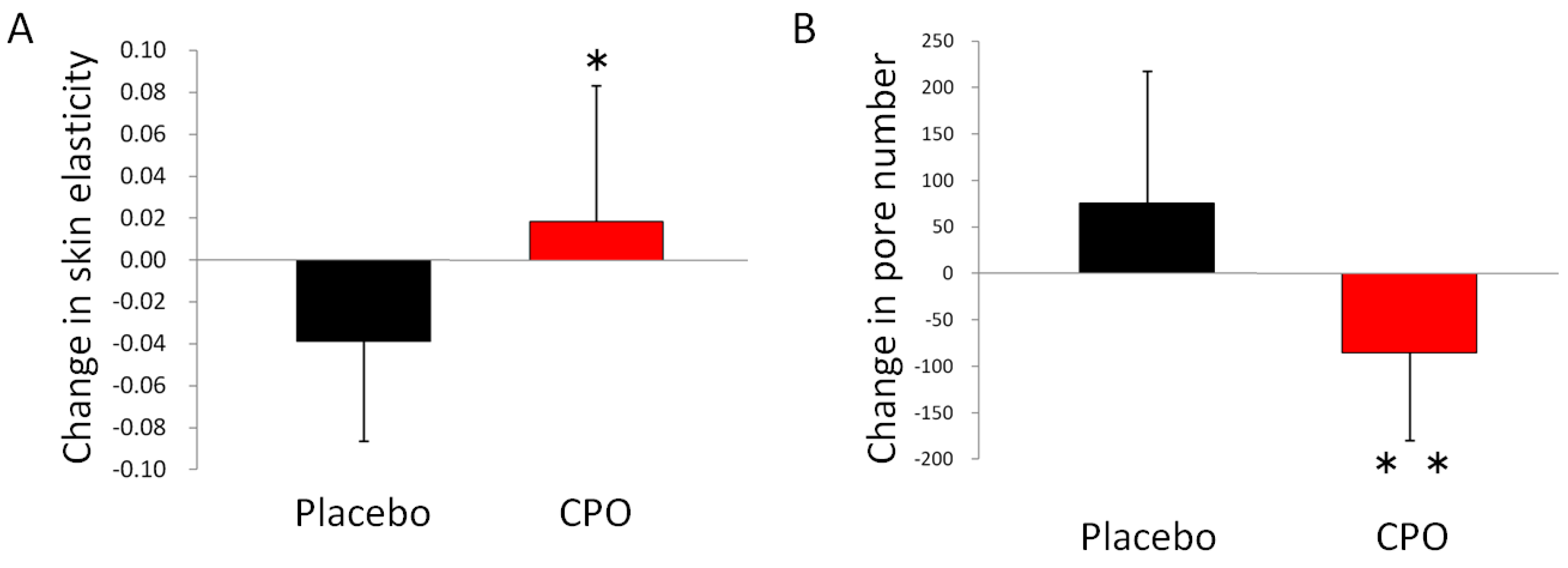
2.2. Skin Conditions
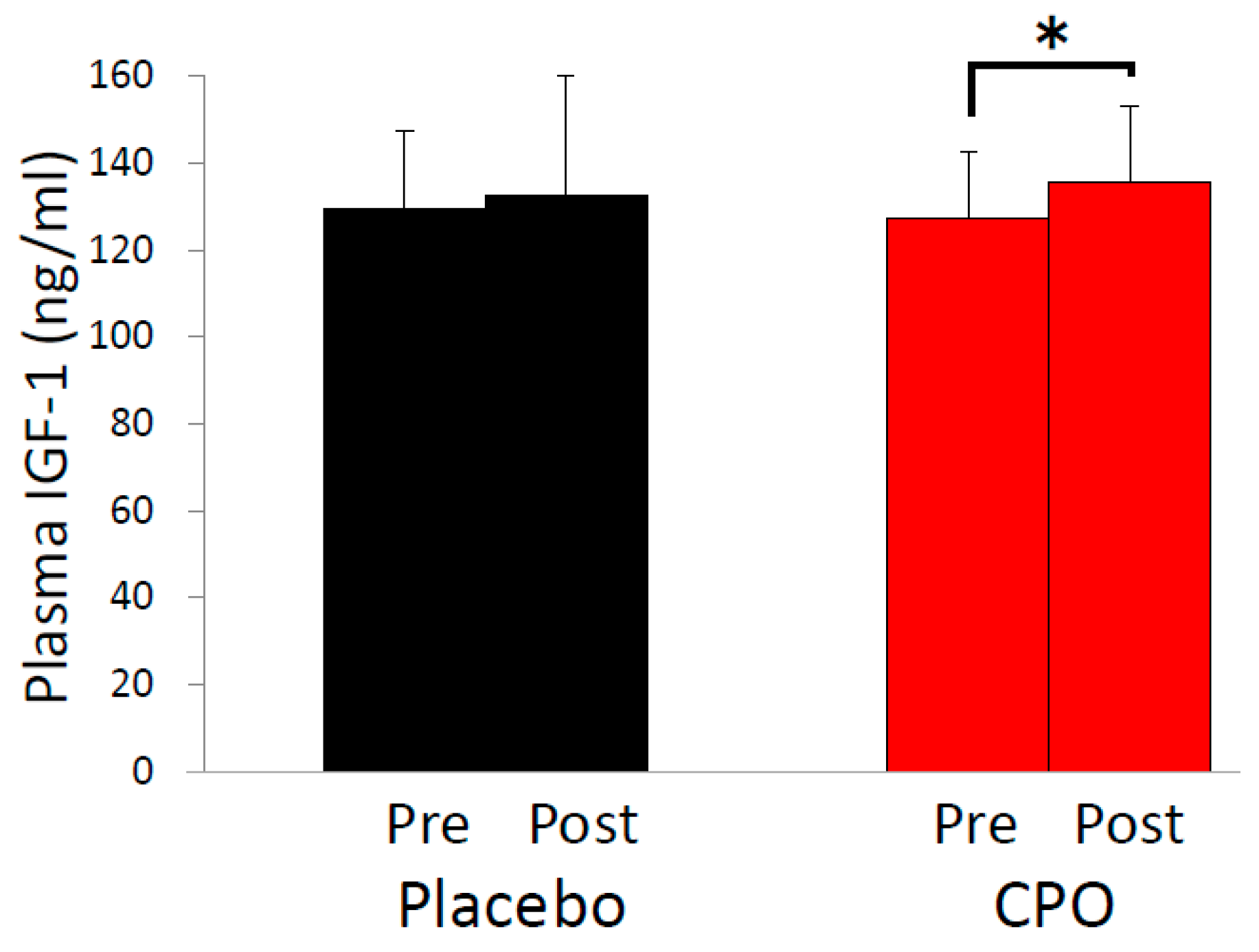
2.3. Plasma Growth Hormone and Insulin-Like Growth Factor-1 (IGF-1) Levels
2.4. Clinical Safety
3. Discussion
4. Materials and Methods
4.1. Study Design, Randomization and Blinding
4.2. Participants
4.3. Supplement Formulation
4.4. Evaluation of Skin Condition
4.5. Blood Sampling and Safety Evaluation
4.6. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fore, J. A review of skin and the effects of aging on skin structure and function. Ostomy Wound Manag. 2006, 52, 24–37. [Google Scholar]
- Weihermann, A.C.; Lorencini, M.; Brohem, C.A.; de Carvalho, C.M. Elastin structure and its involvement in skin photoageing. Int. J. Cosmet. Sci. 2017, 39, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Ganceviciene, R.; Liakou, A.I.; Theodoridis, A.; Makrantonaki, E.; Zouboulis, C.C. Skin anti-aging strategies. Dermatoendocrinology 2012, 4, 308–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kittiphattanabawon, P.; Nalinanon, S.; Benjakul, S.; Kishimura, H. Characteristics of pepsin-solubilised collagen from the skin of splendid squid (Loligo formosana). J. Chem. 2015. [Google Scholar] [CrossRef]
- Berillis, P. The Role of Collagen in the Aorta’s Structure. Open Circ. Vasc. J. 2013. [Google Scholar] [CrossRef]
- Mays, P.K.; McAnulty, R.J.; Campa, J.S.; Laurent, G.J. Age-related changes in collagen synthesis and degradation in rat tissues. Importance of degradation of newly synthesized collagen in regulating collagen production. Biochem. J. 1991, 276, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Varani, J.; Dame, M.K.; Rittie, L.; Fligiel, S.E.G.; Kang, S.; Fisher, G.J.; Voorhees, J.J. Decreased collagen production in chronologically aged skin: Roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. Am. J. Pathol. 2006, 168, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Schagen, S.K.; Zampeli, V.A.; Makrantonaki, E.; Zouboulis, C.C. Discovering the link between nutrition and skin aging. Dermatoendocrinology 2012, 4, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Ito, N.; Seki, S.; Ueda, F. The protective role of astaxanthin for UV-induced skin deterioration in healthy people—A randomized, double-blind, placebo-controlled trial. Nutrients 2018, 10, 817. [Google Scholar] [CrossRef]
- Van Cauter, E.; Plat, L. Physiology of growth hormone secretion during sleep. J. Pediatr. 1996, 128, S32–S37. [Google Scholar] [CrossRef]
- Bartke, A. Growth hormone and aging: A challenging controversy. Clin. Interv. Aging 2008, 3, 659–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonntag, W.E.; Csiszar, A.; De Cabo, R.; Ferrucci, L.; Ungvari, Z. Diverse roles of growth hormone and insulin-like growth factor-1 in mammalian aging: Progress and controversies. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, F.; Karaca, Z.; Unluhizarci, K.; Kelestimur, F. Unusual effects of GH deficiency in adults: A review about the effects of GH on skin, sleep, and coagulation. Endocrine 2014, 47, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. Insulin-like growth factor 1 (IGF-1): A growth hormone. Mol. Pathol. 2001, 54, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Oliveira, A.; Faje, A.; Barkan, A. Postglucose growth hormone nadir and insulin-like growth factor-1 in naïve-active acromegalic patients: Do these parameters always correlate? Arq. Bras. Endocrinol. Metabol. 2011, 55, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Guntur, A.R.; Rosen, C.J. IGF-1 regulation of key signaling pathways in bone. Bonekey Rep. 2013, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiaffino, S.; Mammucari, C. Regulation of skeletal muscle growth by the IGF1-Akt/PKB pathway: Insights from genetic models. Skelet. Muscle 2011, 1. [Google Scholar] [CrossRef] [PubMed]
- Sadagurski, M.; Yakar, S.; Weingarten, G.; Holzenberger, M.; Rhodes, C.J.; Breitkreutz, D.; Leroith, D.; Wertheimer, E. Insulin-like growth factor 1 receptor signaling regulates skin development and inhibits skin keratinocyte differentiation. Mol. Cell. Biol. 2006, 26, 2675–2687. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.A.; Travers, J.B.; Somani, A.K.; Spandau, D.F. The IGF-1/IGF-1R signaling axis in the skin: A new role for the dermis in aging-associated skin cancer. Oncogene 2010, 29, 1475–1485. [Google Scholar] [CrossRef]
- Rudman, D.; Feller, A.G.; Nagraj, H.S.; Gergans, G.A.; Lalitha, P.Y.; Goldberg, A.F.; Schlenker, R.A.; Cohn, L.; Rudman, I.W.; Mattson, D.E. Effects of human growth hormone in men over 60 years old. N. Engl. J. Med. 1990, 323, 1–6. [Google Scholar] [CrossRef]
- Sontakke, S.B.; Jung, J.H.; Piao, Z.; Chung, H.J. Orally available collagen tripeptide: Enzymatic stability, intestinal permeability, and absorption of gly-pro-hyp and pro-hyp. J. Agric. Food Chem. 2016, 64, 7127–7133. [Google Scholar] [CrossRef] [PubMed]
- Mari, W.K.; Muneshige, S.; Shin, K.; Yasuki, T.; Hideyuki, S.; Fumiki, M.; Hitoshi, S.; Yuji, F.; Michio, K. Absorption and effectiveness of orally administered low molecular weight collagen hydrolysate in rats. J. Agric. Food Chem. 2010, 58, 835–841. [Google Scholar] [CrossRef]
- König, D.; Oesser, S.; Scharla, S.; Zdzieblik, D.; Gollhofer, A. Specific collagen peptides improve bone mineral density and bone markers in postmenopausal women—A randomized controlled study. Nutrients 2018, 10, 97. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Sugihara, F.; Suzuki, K.; Inoue, N.; Venkateswarathirukumara, S. A double-blind, placebo-controlled, randomised, clinical study on the effectiveness of collagen peptide on osteoarthritis. J. Sci. Food Agric. 2014, 95, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Zdzieblik, D.; Oesser, S.; Baumstark, M.W.; Gollhofer, A.; König, D. Collagen peptide supplementation in combination with resistance training improves body composition and increases muscle strength in elderly sarcopenic men: A randomised controlled trial. Br. J. Nutr. 2015, 114, 1237–1245. [Google Scholar] [CrossRef]
- Minaguchi, J.; Koyama, Y.; Meguri, N.; Hosaka, Y.; Ueda, H.; Kusubata, M.; Hirota, A.; Irie, S.; Mafune, N.; Takehana, K. Effects of ingestion of collagen peptide on collagen fibrils and glycosaminoglycans in Achilles tendon. J. Nutr. Sci. Vitaminol. 2005, 51, 169–174. [Google Scholar] [CrossRef]
- Asserin, J.; Lati, E.; Shioya, T.; Prawitt, J. The effect of oral collagen peptide supplementation on skin moisture and the dermal collagen network: Eevidence from an ex vivo model and randomized, placebo-controlled clinical trials. J. Cosmet. Dermatol. 2015, 14, 291–301. [Google Scholar] [CrossRef]
- Inoue, N.; Sugihara, F.; Wang, X. Ingestion of bioactive collagen hydrolysates enhance facial skin moisture and elasticity and reduce facial ageing signs in a randomised double-blind placebo-controlled clinical study. J. Sci. Food Agric. 2016, 96, 4077–4081. [Google Scholar] [CrossRef]
- Sugihara, F.; Inoue, N.; Wang, X. Clinical effects of ingesting collagen hydrolysate on facial skin properties: -A randomized, placebo-controlled, double-blind trial. Jpa. Pharmacol. Ther. 2015, 43, 67–70. [Google Scholar]
- Silva, T.H.; Moreira-Silva, J.; Marques, A.L.P.; Domingues, A.; Bayon, Y.; Reis, R.L. Marine origin collagens and its potential applications. Mar. Drugs 2014, 12, 5881–5901. [Google Scholar] [CrossRef] [Green Version]
- Muthumari, K.; Anand, M.; Maruthupandy, M. Collagen extract from marine finfish scales as a potential mosquito larvicide. Protein J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Yang, P.; Zhou, C.; Li, S.; Hong, P. Marine collagen peptides from the skin of Nile Tilapia (Oreochromis niloticus): Characterization and wound healing evaluation. Mar. Drugs 2017, 15, 102. [Google Scholar] [CrossRef] [PubMed]
- Xuan Ri, S.; Hideyuki, K.; Koretaro, T. Characterization of molecular species of collagen in scallop mantle. Food Chem. 2007. [Google Scholar] [CrossRef]
- Mizuta, S.; Tanaka, T.; Yoshinaka, R. Comparison of collagen types of arm and mantle muscles of the common octopus (Octopus vulgaris). Food Chem. 2003. [Google Scholar] [CrossRef]
- Kołodziejska, I.; Sikorski, Z.E.; Niecikowska, C. Parameters affecting the isolation of collagen from squid (Illex argentinus) skins. Food Chem. 1999. [Google Scholar] [CrossRef]
- Wang, L.; An, X.; Yang, F.; Xin, Z.; Zhao, L.; Hu, Q. Isolation and characterisation of collagens from the skin, scale and bone of deep-sea redfish (Sebastes mentella). Food Chem. 2008. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Wang, Y.M.; Chi, C.F.; Luo, H.Y.; Deng, S.G.; Ma, J.Y. Isolation and characterization of collagen and antioxidant collagen peptides from scales of croceine croaker (Pseudosciaena crocea). Mar. Drugs 2013, 11, 4641–4661. [Google Scholar] [CrossRef]
- Xu, L.; Dong, W.; Zhao, J.; Xu, Y. Effect of marine collagen peptides on physiological and neurobehavioral development of male rats with perinatal asphyxia. Mar. Drugs 2015, 13, 3653–3671. [Google Scholar] [CrossRef]
- Tanaka, M.; Koyama, Y.; Nomura, Y. Effects of collagen peptide ingestion on UV-B-induced skin damage. Biosci. Biotechnol. Biochem. 2009, 73, 930–932. [Google Scholar] [CrossRef]
- Lee, J.K.; Kang, S.I.; Kim, Y.J.; Kim, M.J.; Heu, M.S.; Choi, B.D.; Kim, J.S. Comparison of collagen characteristics of sea- and freshwater-rainbow trout skin. Food Sci. Biotechnol. 2016. [Google Scholar] [CrossRef]
- Tziveleka, L.A.; Ioannou, E.; Tsiourvas, D.; Berillis, P.; Foufa, E.; Roussis, V. Collagen from the marine sponges Axinella cannabina and Suberites carnosus: Isolation and morphological, biochemical, and biophysical characterization. Mar. Drugs 2017, 15, 152. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Kirisako, T.; Kokubo, T.; Miura, Y.; Morishita, K.; Okamura, H.; Tsuda, A. Randomised controlled trial of the effects of L-ornithine on stress markers and sleep quality in healthy workers. Nutr. J. 2014, 13, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demura, S.; Morishita, K.; Yamada, T.; Yamaji, S.; Komatsu, M. EVect of L-ornithine hydrochloride ingestion on intermittent maximal anaerobic cycle ergometer performance and fatigue recovery after exercise. Eur. J. Appl. Physiol. 2011, 111, 2837–2843. [Google Scholar] [CrossRef] [PubMed]
- Sugino, T.; Shirai, T.; Kajimoto, Y.; Kajimoto, O. l-Ornithine supplementation attenuates physical fatigue in healthy volunteers by modulating lipid and amino acid metabolism. Nutr. Res. 2008, 28, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Koyama, Y.I.; Kuwaba, K.; Kondo, S.; Tsukada, Y. Supplemental ingestion of collagen peptide suppresses ultraviolet-induced erythema—A randomized double-blind placebo-controlled study. Jpn. Pharmacol. Ther. 2014, 42, 781–790. [Google Scholar]
- Evain-Brion, D.; Donnadieu, M.; Roger, M.; Job, J.C. Simultaneous study of somatotrophic and corticotrophic pituitary secretions during ornithine infusion test. Clin. Endocrinol. 1982, 17, 119–122. [Google Scholar] [CrossRef]
- Kim, D.U.; Chung, H.C.; Choi, J.; Sakai, Y.; Lee, B.Y. Oral intake of low-molecular-weight collagen peptide improves hydration, elasticity, and wrinkling in human skin: A randomized, double-blind, placebo-controlled study. Nutrients 2018, 10, 826. [Google Scholar] [CrossRef]
- Sugihare, F.; Inoue, N. Clinical effects of collagen hydrolysates ingestion on UV-induced pigmented spots of human skin: A preliminary study. Heal. Sci. 2012, 28, 153–156.1. [Google Scholar]
- Proksch, E.; Schunck, M.; Zague, V.; Segger, D.; Degwert, J.; Oesser, S. Oral intake of specific bioactive collagen peptides reduces skin wrinkles and increases dermal matrix synthesis. Skin Pharmacol. Physiol. 2014, 27, 113–119. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, J.; Ding, Y.; Dai, X.; Li, Y. Oral administration of marine collagen peptides from Chum Salmon skin enhances cutaneous wound healing and angiogenesis in rats. J. Sci. Food Agric. 2011. [Google Scholar] [CrossRef]
- Wang, J.; Xu, M.; Liang, R.; Zhao, M.; Zhang, Z.; Li, Y. Oral administration of marine collagen peptides prepared from chum salmon (Oncorhynchus keta) improves wound healing following cesarean section in rats. Food Nutr. Res. 2015, 59. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.P.; Fishel, R.S.; Efron, D.T.; Williams, J.Z.; Fishel, M.H.; Barbul, A. Effect of supplemental ornithine on wound healing. J. Surg. Res. 2002, 106, 299–302. [Google Scholar] [CrossRef]
- Darlenski, R.; Kazandjieva, J.; Tsankov, N. Skin barrier function: Morphological basis and regulatory mechanisms. J. Clin. Med. 2011, 4, 36–45. [Google Scholar]
- Goad, N.; Gawkrodger, D.J. Ambient humidity and the skin: The impact of air humidity in healthy and diseased states. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.; Blanco, M.; Correa, B.; Perez-Martin, R.I.; Sotelo, C.G. Effect of fish collagen hydrolysates on type I collagen mRNA levels of human dermal fibroblast culture. Mar. Drugs 2018, 16, 144. [Google Scholar] [CrossRef]
- Ghahary, A.; Tredget, E.E.; Shen, Q.; Kilani, R.T.; Scott, P.G.; Houle, Y. Mannose-6-phosphate/IGF-II receptors mediate the effects of IGF-1-induced latent transforming growth factor beta 1 on expression of type I collagen and collagenase in dermal fibroblasts. Growth Factors 2000, 17, 167–176. [Google Scholar] [CrossRef]
- Hegde, S.; Raghavan, S. A skin-depth analysis of integrins: Role of the integrin network in health and disease. Cell Commun. Adhes. 2013, 20, 155–169. [Google Scholar] [CrossRef]
- Allen, E.; Bhimji, S.S. Anatomy, Head and Neck, Thyroid; StatPearls Publishing LLC.: Petersburg, FL, USA, 2018. [Google Scholar]
- Ayano, I.; Yuriko, O.; Shinobu, S.; Hiroyuki, S.; Takashi, K.; Koh, M.; Masami, S. Effects of capsule containing astaxanthin on skin condition in healthy subjects—A randomized, double-blind, parallel-group, placebo-controlled study. Jpn. Pharmacol. Ther. 2016, 44, 1209–1216. [Google Scholar]
- Shigemura, Y.; Kubomura, D.; Sato, Y.; Sato, K. Dose-dependent changes in the levels of free and peptide forms of hydroxyproline in human plasma after collagen hydrolysate ingestion. Food Chem. 2014. [Google Scholar] [CrossRef]
- Goldsberry, A.; Hanke, C.W.; Hanke, K.E. VISIA system: A possible tool in the cosmetic practice. J. Drugs Dermatol. 2014, 13, 1312–1314. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Placebo (n = 11) | Collagen Peptide and Ornithine (CPO) (n = 10) | p Value | |
|---|---|---|---|
| Age (mean ± standard deviation (SD)) | 40.4 ± 5.2 | 40.0 ± 6.8 | 0.89 |
| Female, n (%) | 9 (81.8) | 8 (80.0) | |
| Body mass index (BMI) (mean ± SD) | 20.6 ± 1.8 | 21.2 ± 2.2 | 0.55 |
| Week | |||
|---|---|---|---|
| 0 | 8 | ||
| Skin Conditions | Group | Mean ± SD | Mean ± SD |
| Moisture (A.U.) | Placebo | 57.3 ± 13.3 | 60.9 ± 10.7 |
| CPO | 58.5 ± 7.4 | 60.3 ± 8.2 | |
| TEWL (g/m2 × h) | Placebo | 14.4 ± 4.3 | 16.2 ± 3.4 |
| CPO | 11.3 ± 4.1 | 11.5 ± 4.2 * | |
| Elasticity | Placebo | 0.818 ± 0.05 | 0.779 ± 0.06 |
| CPO | 0.766 ± 0.07 | 0.784 ± 0.07 | |
| Skin-pH | Placebo | 5.96 ± 0.23 | 6.00 ± 0.24 |
| CPO | 6.03 ± 0.24 | 6.15 ± 0.23 | |
| DermaLab Collagen Score | Placebo | 45.9 ± 17.9 | 40.9 ± 14.6 |
| CPO | 41.1 ± 15.2 | 38.9 ± 13.4 | |
| VISIA Spots | Placebo | 99.9 ± 38.1 | 96.1 ± 37.6 |
| CPO | 83.3 ± 39.0 | 75.1 ± 34.6 | |
| VISIA Wrinkles | Placebo | 172.3 ± 100.5 | 186.9 ± 124.5 |
| CPO | 186.2 ± 108.2 | 209.5 ± 106.9 | |
| VISIA pores | Placebo | 670.2 ± 328.8 | 745.8 ± 354.2 |
| CPO | 848.4 ± 404.6 | 763.5 ± 452.7 | |
| VISIA Texture | Placebo | 1972.0 ± 1171.7 | 1755.8 ± 1172.9 |
| CPO | 1773.4 ± 1276.9 | 1610.5 ± 1243.7 | |
| VISIA Porphyrins | Placebo | 719.9 ± 709.6 | 607.6 ± 585.6 |
| CPO | 694.4 ± 402.4 | 868.2 ± 648.8 | |
| VISIA Spots | Placebo | 193.3 ± 63.7 | 202.0 ± 56.9 |
| CPO | 199.7 ± 56.4 | 209.9 ± 43.1 | |
| Red Areas | Placebo | 49.5 ± 14.6 | 49.3 ± 14.8 |
| CPO | 42.9 ± 17.2 | 36.4 ± 17.3 | |
| Brown Spots | Placebo | 123.5 ± 58.5 | 125.3 ± 61.1 |
| CPO | 104.1 ± 47.4 | 109.6 ± 50.5 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, N.; Seki, S.; Ueda, F. Effects of Composite Supplement Containing Collagen Peptide and Ornithine on Skin Conditions and Plasma IGF-1 Levels—A Randomized, Double-Blind, Placebo-Controlled Trial. Mar. Drugs 2018, 16, 482. https://0-doi-org.brum.beds.ac.uk/10.3390/md16120482
Ito N, Seki S, Ueda F. Effects of Composite Supplement Containing Collagen Peptide and Ornithine on Skin Conditions and Plasma IGF-1 Levels—A Randomized, Double-Blind, Placebo-Controlled Trial. Marine Drugs. 2018; 16(12):482. https://0-doi-org.brum.beds.ac.uk/10.3390/md16120482
Chicago/Turabian StyleIto, Naoki, Shinobu Seki, and Fumitaka Ueda. 2018. "Effects of Composite Supplement Containing Collagen Peptide and Ornithine on Skin Conditions and Plasma IGF-1 Levels—A Randomized, Double-Blind, Placebo-Controlled Trial" Marine Drugs 16, no. 12: 482. https://0-doi-org.brum.beds.ac.uk/10.3390/md16120482