The Relationship between Diffusion-Weighted Magnetic Resonance Imaging Lesions and 24-Hour Rhythm Holter Findings in Patients with Cryptogenic Stroke

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
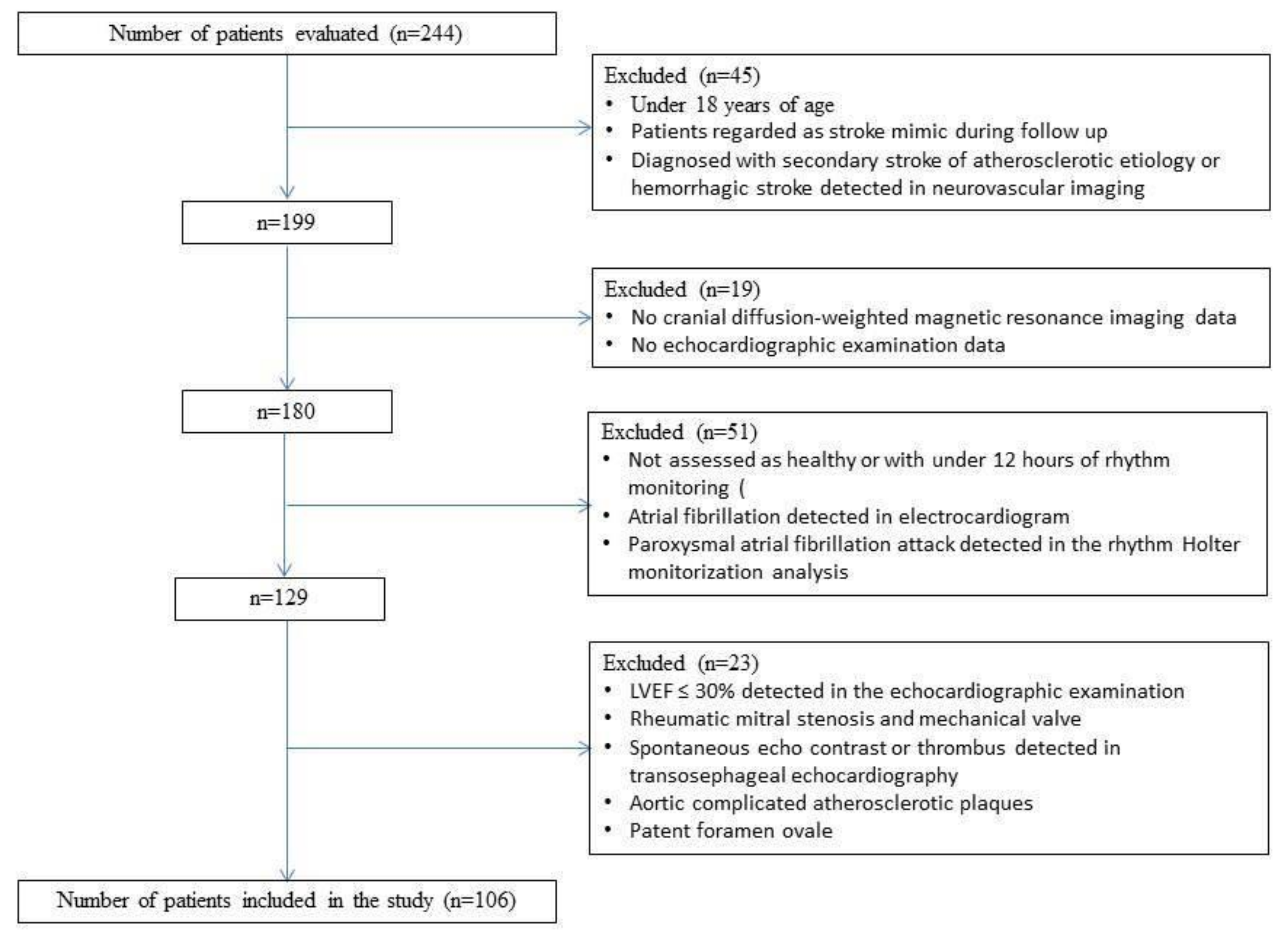
2.1. Subject Selection
2.2. Collection of Data
2.3. MR Protocol and Evaluation
2.4. Statistical Examinations
3. Results
4. Discussion
5. Limitations
6. Conclusion
Author Contributions
Funding
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 4, 29–322. [Google Scholar]
- Warlow, C.; Sudlow, C.; Dennis, M.; Wardlaw, J.; Sandercock, P. Stroke. Lancet 2003, 11, 211–1224. [Google Scholar] [CrossRef]
- European Registers of Stroke (EROS) Investigators; Heuschmann, P.U.; Di Carlo, A.; Bejot, Y.; Rastenyte, D.; Ryglewicz, D.; Sarti, C.; Torrent, M.; Wolfe, C.D. İncidence of stroke in Europe at the beginning of the 21st century. Stroke 2009, 5, 1557–1563. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., III. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of ORG 10172 in Acute Stroke Treatment. Stroke 1993, 1, 35–41. [Google Scholar] [CrossRef]
- Yang, H.; Nassif, M.; Khairy, P.; de Groot, J.R.; Roos, Y.; de Winter, R.J.; Mulder, B.J.M.; Bouma, B.J. Cardiac diagnostic work-up of ischaemic stroke. Eur. Heart J. 2018, 5, 1851–1860. [Google Scholar] [CrossRef] [PubMed]
- Kolominsky-Rabas, P.L.; Weber, M.; Gefeller, O.; Neundoerfer, B.; Heuschmann, P.U. Epidemiology of ischaemic stroke subtypes according to TOAST criteria: Incidence, recurrence, and long-term survival in ischaemic stroke subtypes: A population-based study. Stroke 2001, 12, 2735–2740. [Google Scholar] [CrossRef]
- Fuster, V.; Rydén, L.E.; Cannom, D.S.; Crijns, H.J.; Curtis, A.B.; Ellenbogen, K.A.; Halperin, J.L.; Kay, G.N.; Le Huezey, J.Y.; Lowe, J.E. 2011 ACCF/ AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2011, 10, 269–367. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 3, 233–270. [Google Scholar] [CrossRef]
- Kang, D.W.; Chalela, J.A.; Ezzeddine, M.A.; Warach, S. Association of ischemic lesion patterns on early diffusion-weighted imaging with TOAST stroke subtypes. Arch. Neurol. 2003, 12, 1730–1734. [Google Scholar] [CrossRef]
- Lee, K.J.; Jung, K.H.; Byun, J.J.; Kim, J.M.; Roh, J.K. Infarct Pattern and Clinical Outcome in Acute Ischemic Stroke Following Middle Cerebral Artery Occlusion. Cerebrovasc. Dis. 2014, 38, 31–38. [Google Scholar] [CrossRef]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Peripheral Vascular Disease. Guidelines for the prevention of stroke in patients with stroke and transient ischaemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 7, 2160–2236. [Google Scholar]
- Hart, R.G.; Diener, H.C.; Coutts, S.B.; Easton, J.D.; Granger, C.B.; O’Donnell, M.J.; Sacco, R.L.; Connolly, S.J. Embolic strokes of undetermined source: The case for a new clinical construct. Lancet Neurol. 2014, 4, 429–438. [Google Scholar] [CrossRef]
- Tomita, H.; Sasaki, S.; Hagii, J.; Metoki, N. Covert atrial fibrillation and atrial high-rate episodes as a potential cause of embolic strokes of undetermined source: Their detection and possible management strategy. J. Cardiol. 2018, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, S.; Sarov, M.; Vandendries, C.; Guedj, T.; Cauquil, C.; Assayag, P.; Lambotte, O.; Ducreux, D.; Denier, C. Significance of acute multiple infarcts in multiple cerebral circulations on initial diffusion weighted imaging in stroke patients. J. Neurol. Sci. 2014, 1–2, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Altieri, M.; Metz, R.J.; Müller, C.; Maeder, P.; Meuli, R.; Bogousslavsky, J. Multiple brain infarcts: Clinical and neuroimaging patterns using diffusion-weighted magnetic resonance. Eur. Neurol. 1999, 2, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Bogousslavsky, J.; Cachin, C.; Regli, F.; Despland, P.A.; Van Melle, G.; Kappenberger, L. Cardiac sources of embolism and cerebral infarction–clinical consequences and vascular concomitants: The lausanne stroke registry. Neurology 1991, 6, 855–859. [Google Scholar] [CrossRef]
- Lin, H.J.; Wolf, P.A.; Kelly-Hayes, M.; Beiser, A.S.; Kase, C.S.; Benjamin, E.J.; D’Agostino, R.B. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996, 10, 1760–1764. [Google Scholar] [CrossRef]
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch. Intern. Med. 1994, 13, 1449–1457.
- Kochhäuser, S.; Dechering, D.G.; Dittrich, R.; Reinke, F.; Ritter, M.A.; Ramtin, S.; Duning, T.; Frommeyer, G.; Eckardt, L. Supraventricular premature beats and short atrial runs predict atrial fibrillation in continuously monitored patients with cryptogenic stroke. Stroke 2014, 3, 884–886. [Google Scholar] [CrossRef]
- Kishore, A.; Vail, A.; Majid, A.; Dawson, J.; Lees, K.R.; Tyrrell, P.J.; Smith, C.J. Detection of atrial fibrillation after ischemic stroke or transient ischemic attack: A systematic review and meta-analysis. Stroke 2014, 2, 520–526. [Google Scholar] [CrossRef]
- Sanna, T.; Diener, H.C.; Passman, R.S.; Crystal AF Steering Committee. Cryptogenic stroke and underlying atrial fibrillation. N. Engl. J. Med. 2014, 13, 2478–2486. [Google Scholar] [CrossRef] [PubMed]
- Todo, K.; Moriwaki, H.; Saito, K.; Naritomi, H. Frequent premature atrial contractions in stroke of undetermined etiology. Eur. Neurol. 2009, 5, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Chong, B.H.; Pong, V.; Lam, K.F.; Liu, S.; Zuo, M.L.; Lau, Y.F.; Lau, C.P.; Tse, H.F.; Siu, C.W. Frequent premature atrial complexes predict new occurrence of atrial fibrillation and adverse cardiovascular events. Europace 2012, 7, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Glotzer, T.V.; Hellkamp, A.S.; Zimmerman, J.; Sweeney, M.O.; Yee, R.; Marinchak, R.; Cook, J.; Paraschos, A.; Love, J.; Radoslovich, G.; et al. Atrial high rate episodes detected by pacemaker diagnostics predict death and stroke: Report of the atrial diagnostics ancillary study of the MOde Selection Trial (MOST). Circulation 2003, 12, 1614–1619. [Google Scholar] [CrossRef] [PubMed]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998, 10, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Jauch, E.C.; Saver, J.L.; Adams, H.P., Jr.; Bruno, A.; Connors, J.J.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W., Jr.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the american heart association/american stroke association. Stroke 2013, 3, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.J.; Spring, M.; Dorian, P.; Panzov, V.; Thorpe, K.E.; Hall, J.; Vaid, H.; O’Donnell, M.; Laupacis, A.; Côté, R. Atrial fibrillation in patients with cryptogenic stroke. N. Engl. J. Med. 2014, 26, 2467–2477. [Google Scholar] [CrossRef]
- Arsava, E.M.; Bas, D.F.; Atalar, E.; Has, A.C.; Oguz, K.K.; Topcuoglu, M.A. Ischemic stroke phenotype in patients with nonsustained atrial fibrillation. Stroke 2015, 3, 634–640. [Google Scholar] [CrossRef]
- Naess, H.; Gjerde, G.; Waje-Andreassen, U. Ischemic stroke in patients older and younger than 80 years. Acta Neurol. Scand. 2014, 6, 399–404. [Google Scholar] [CrossRef]
- Chang, K.C.; Lee, H.C.; Tseng, M.C.; Huang, Y.C. Three-year survival after first-ever ischemic stroke is predicted by initial stroke severity: A hospital-based study. Clin. Neurol. Neurosurg. 2010, 4, 296–301. [Google Scholar] [CrossRef]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 3, 28–292. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.D. Controlling resistant hypertension. Stroke Vasc. Neurol. 2018, 2, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Lei, C.; Wu, B.; Liu, M.; Chen, Y. Risk Factors and Clinical Outcomes Associated with Intracranial and Extracranial Atherosclerotic Stenosis Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2014, 5, 1112–1117. [Google Scholar] [CrossRef] [PubMed]
- Andersson, J.; Johansson, L.; Ladenvall, P.; Wiklund, P.G.; Stegmayr, B.; Jern, C.; Boman, K. C-reactive protein is a determinant of first-ever stroke: Prospective nested case-referent study. Cerebrovasc. Dis. 2009, 6, 544–551. [Google Scholar] [CrossRef]
- Elkind, M.S.; Tai, W.; Coates, K.; Paik, M.C.; Sacco, R.L. High-sensitivity C-reactive protein, lipoprotein-associated phospholipase A2, and outcome after ischemic stroke. Arch. Intern. Med. 2006, 19, 2073–2080. [Google Scholar] [CrossRef]
- Shantikumar, S.; Grant, P.J.; Catto, A.J.; Bamford, J.M.; Carter, A.M. Elevated C-reactive protein and longterm mortality after ischaemic stroke: Relationship with markers of endothelial cell and platelet activation. Stroke 2009, 3, 977–979. [Google Scholar] [CrossRef]
- Grote Beverborg, N.; van Veldhuisen, D.J.; van der Meer, P. Anemia in Heart Failure: Still Relevant? JACC Heart Fail. 2018, 3, 201–208. [Google Scholar] [CrossRef]
- Hao, Z.; Wu, B.; Wang, D.; Lin, S.; Tao, W.; Liu, M. A cohort study of patients with anemia on admission and fatality after acute ischemic stroke. J. Clin. Neurosci. 2013, 1, 37–42. [Google Scholar] [CrossRef]
- Barlas, R.S.; Honney, K.; Loke, Y.K.; McCall, S.J.; Bettencourt-Silva, J.H.; Clark, A.B.; Bowles, K.M.; Metcalf, A.K.; Mamas, M.A.; Potter, J.F.; et al. Impact of Hemoglobin Levels and Anemia on Mortality in Acute Stroke: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis. J. Am. Heart Assoc. 2016, 8, e003019. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Single Vascular Territory (n = 73) | Multiple Vascular Territory (n = 33) | p value |
|---|---|---|---|
| Age | 59.07 14.21 | 65.12 12.79 | 0.039* |
| Gender | |||
| Female | 21 (61.8) | 13 (38.2) | 0.278 |
| Male | 52 (72.2) | 20 (27.8) | |
| Alcohol | |||
| No | 62 (68.1) | 29 (31.9) | 0.773 |
| Yes | 11 (73.3) | 4 (26.7) | |
| Smoking | |||
| No | 46 (64.8) | 25 (35.2) | 0.196 |
| Yes | 27 (77.1) | 8 (22.9) | |
| HT | |||
| No | 40 (78.4) | 11 (21.6) | 0.041* |
| Yes | 33 (60.0) | 22 (40.0) | |
| DM | |||
| No | 54 (74.0) | 19 (26.0) | 0.091 |
| Yes | 19 (57.6) | 14 (42.4) | |
| HL | |||
| No | 50 (74.6) | 17 (25.4) | 0.093 |
| Yes | 23 (59.0) | 16 (41.0) | |
| CAD | |||
| No | 55 (71.4) | 22 (28.6) | 0.354 |
| Yes | 18 (62.1) | 11 (37.9) |
| Variables | Single Vascular Territory (n = 73) | Multiple Vascular Territory (n = 33) | p value |
|---|---|---|---|
| Rhythm Holter Duration | 23.15 (22.00–24.00) | 23.18 (21.16–24.00) | 0.795 |
| Maximum Heart Rate | 113.63 18.91 | 112.18 19.21 | 0.3633 |
| Mean Heart Rate | 71.9589 8.8858 | 75.36 12.52 | 0.113 |
| Minimum Heart Rate | 50.51 8.23 | 52.97 12.75 | 0.236 |
| Total PAC Count | 167.00 (37.00–447.00) | 1196.00 (1061.00–1813.00) | <0.001* |
| Atrial Run | 0.00 (0.00–0.00) | 13.50 (11.00–34.25) | <0.001* |
| Total Run | 11.42 (11.31–11.54) | 11.38 (11.31–11.53) | 0.286 |
| PAC/Total heart rate | 0.0018 (0.0004–0.0051) | 0.0174 (0.0098–0.0275) | <0.001* |
| EF | 60.00 (55.00–63.00) | 58.00 (55.00–60.00) | 0.337 |
| LA | 36.99 6.07 | 37.09 5.26 | 0.932 |
| LVDD | |||
| No | 29 (72.5) | 11 (27.5) | 0.530 |
| Yes | 44 (66.7) | 22 (33.3) | |
| CHA2DS2-VASc | 3.00 (2.00–5.00) | 5.00 (3.00–6.00) | 0.059 |
| logPLT | 12.36±0.45 | 12.39 ± 0.30 | 0.873 |
| logWBC | 8.96 0.26 | 8.98 0.35 | 0.790 |
| CRP | 0.60 (0.30–1.06) | 1.00 (0.40–3.20) | 0.037* |
| TSH | 0.80 (0.40–1.20) | 1.00 (0.40–1.90) | 0.479 |
| HG | 14.00 (12.70–15.00) | 13.00 (11.30–13.70) | <0.001* |
| MPV | 10.00 (9.20–10.90) | 9.60 (9.20–10.30) | 0.305 |
| Variable | Coefficient (Standard Error) | Odds Ratio (95% CI) | p value |
|---|---|---|---|
| Age | 0.034 (0.017) | 1.034 (1.001–1.068) | 0.042* |
| Gender (Female) | 0.476 (0.440) | 1.610 (0.679–3.814) | 0.280 |
| Alcohol (Yes) | −0.252 (0.626) | 0.777 (0.228–2.650) | 0.687 |
| Smoking (Yes) | −0.607 (0.473) | 0.545 (0.216–1.378) | 0.200 |
| HT (Yes) | 0.886 (0.438) | 2.424 (1.028–5.718) | 0.043* |
| DM (Yes) | 0.739 (0.442) | 2.094 (0.881–4.978) | 0.094* |
| HL (Yes) | 0.716 (0.430) | 2.046 (0.881–4.752) | 0.096* |
| CAD (Yes) | 0.424 (0.458) | 1.528 (0.622–3.752) | 0.355 |
| Rhythm Holter Duration | 0.034 (0.075) | 1.034 (0.893–1.198) | 0.652 |
| Maximum Heart Rate | −0.004 (0.011) | 0.996 (0.974–1.018) | 0.714 |
| Mean Heart Rate | 0.033 (0.021) | 1.033 (0.992–1.076) | 0.117* |
| Minimum Heart Rate | 0.026 (0.022) | 1.026 (0.983–1.070) | 0.238 |
| Total PAC Count | 0.003 (0.001) | 1.003 (1.002–1.004) | <0.001* |
| Atrial Run | 0.119 (0.030) | 1.126 (1.062–1.195) | <0.001* |
| Total Run | −0.000012 (0.000010) | 1.000 (0.999–1.000) | 0.250 |
| EF | -0.016 (0.030) | 0.984 (0.927–1.044) | 0.586 |
| LA | 0.003 (0.036) | 1.003 (0.934–1.077) | 0.931 |
| LVDD (Yes) | 0.276 (0.440) | 1.318 (0.557–3.122) | 0.530 |
| CHA2DS2-VASc | 0.220 (0.116) | 1.246 (0.993–1.565) | 0.058* |
| logPLT | 0.232 (0.553) | 1.261 (0.426–3.729) | 0.675 |
| logWBC | 0.194 (0.720) | 1.214 (0.296–4.978) | 0.787 |
| CRP | 0.162 (0.076) | 1.175 (1.014–1.363) | 0.032* |
| TSH | 0.174 (0.145) | 1.190 (0.896–1.581) | 0.230 |
| HG | −0.373 (0.127) | 0.689 (0.537–0.884) | 0.003* |
| MPV | −0.124 (0.174) | 0.884 (0.629–1.242) | 0.477 |
| Variable | Coefficient (Standard Error) | Odds Ratio (95% CI) | p value |
|---|---|---|---|
| Age | 0.034 (0.041) | 1.035 (0.956–1.121) | 0.396 |
| HT (Yes) | 0.028 (1.145) | 1.028 (0.109–9.706) | 0.980 |
| DM (Yes) | 1.529 (0.994) | 4.612 (0.657–32.382) | 0.124 |
| HL (Yes) | 0.903 (0.981) | 2.467 (0.360–16.883) | 0.358 |
| Mean Heart Rate | 0.020 (0.040) | 1.020 (0.942–1.104) | 0.626 |
| Total PAC Count | 0.002 (0.001) | 1.002 (1.001–1.004) | 0.001* |
| Atrial Run | 0.083 (0.031) | 1.086 (1.021–1.155) | 0.008* |
| CHA2DS2-VASc | −0.872 (0.499) | 0.418 (0.157–1.112) | 0.080 |
| CRP | 0.094 (0.097) | 1.099 (0.909–1.328) | 0.332 |
| HG | −0.286 (0.214) | 0.751 (0.494–1.142) | 0.180 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gürdoğan, M.; Kehaya, S.; Korkmaz, S.; Altay, S.; Özkan, U.; Kaya, Ç. The Relationship between Diffusion-Weighted Magnetic Resonance Imaging Lesions and 24-Hour Rhythm Holter Findings in Patients with Cryptogenic Stroke. Medicina 2019, 55, 38. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020038
Gürdoğan M, Kehaya S, Korkmaz S, Altay S, Özkan U, Kaya Ç. The Relationship between Diffusion-Weighted Magnetic Resonance Imaging Lesions and 24-Hour Rhythm Holter Findings in Patients with Cryptogenic Stroke. Medicina. 2019; 55(2):38. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020038
Chicago/Turabian StyleGürdoğan, Muhammet, Sezgin Kehaya, Selçuk Korkmaz, Servet Altay, Uğur Özkan, and Çağlar Kaya. 2019. "The Relationship between Diffusion-Weighted Magnetic Resonance Imaging Lesions and 24-Hour Rhythm Holter Findings in Patients with Cryptogenic Stroke" Medicina 55, no. 2: 38. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020038