Correlation of Thyroid Transcription Factor-1 Expression with EGFR Mutations in Non-Small-Cell Lung Cancer: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Publication Search Strategy
2.2. Eligibility Criteria
2.3. Article Review and Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
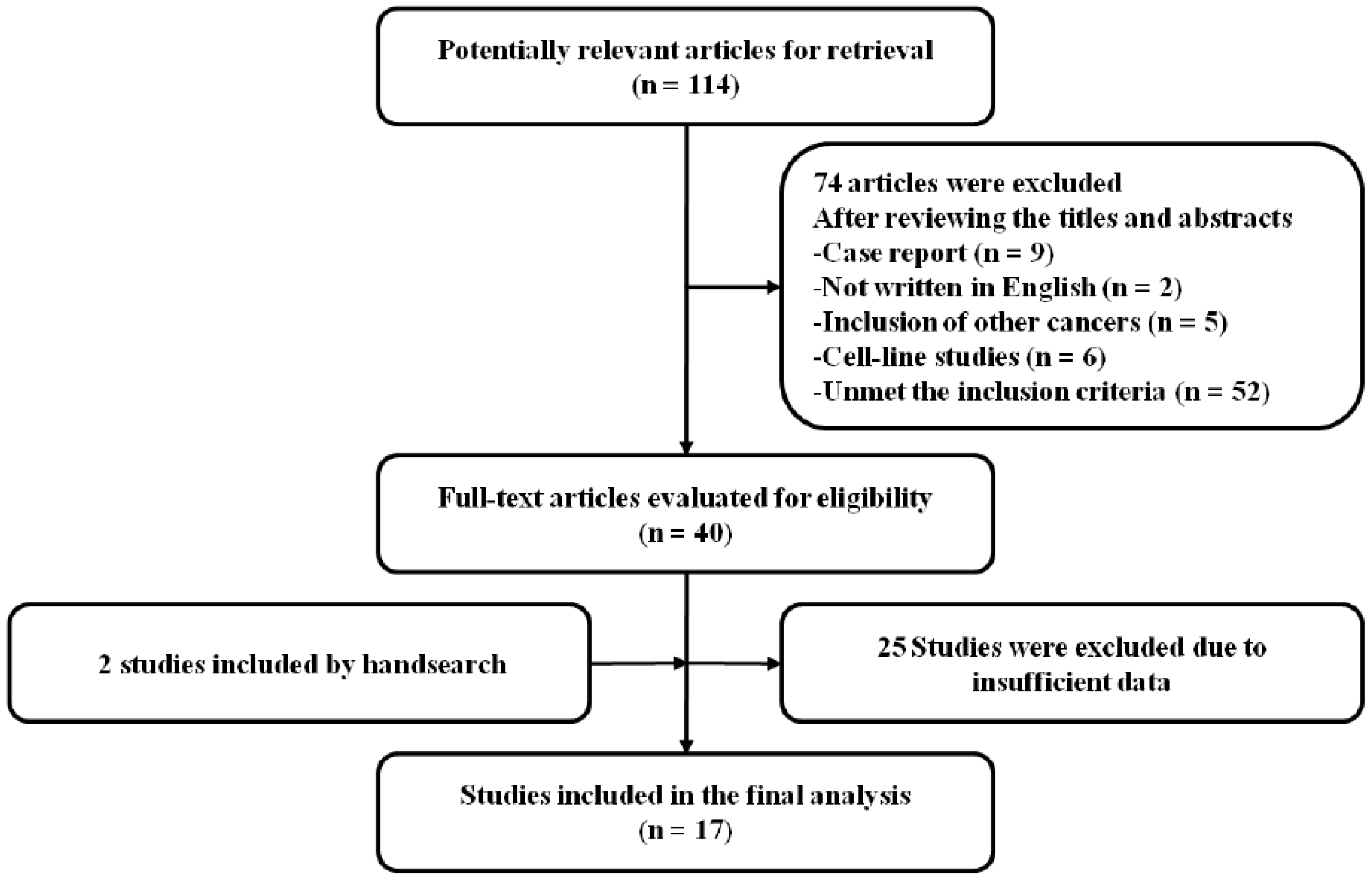
3.1. Search Results
3.2. Characteristics of the Included Studies
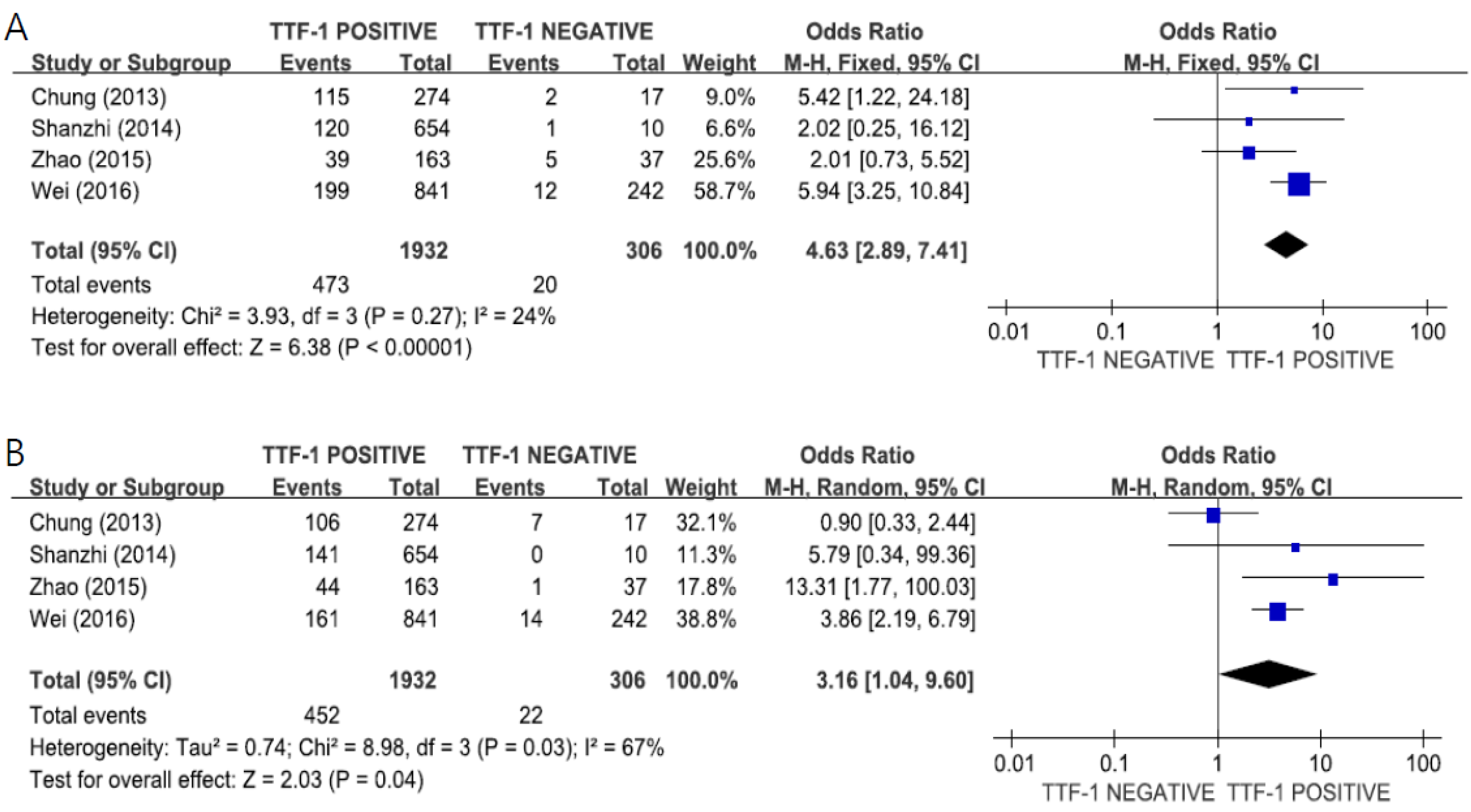
3.3. Correlation of TTF-1 Expression and EGFR Mutations
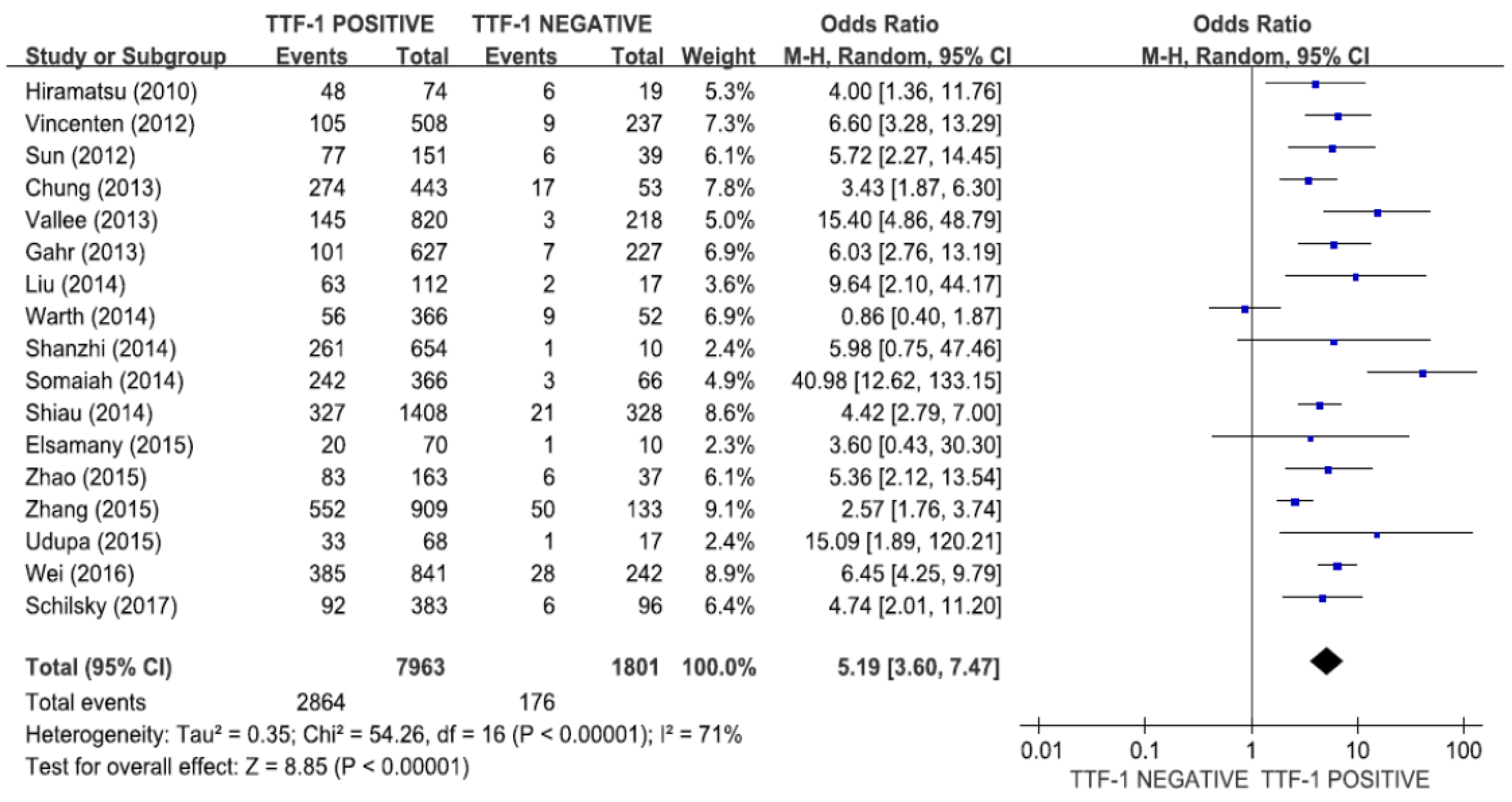
3.3.1. Overall
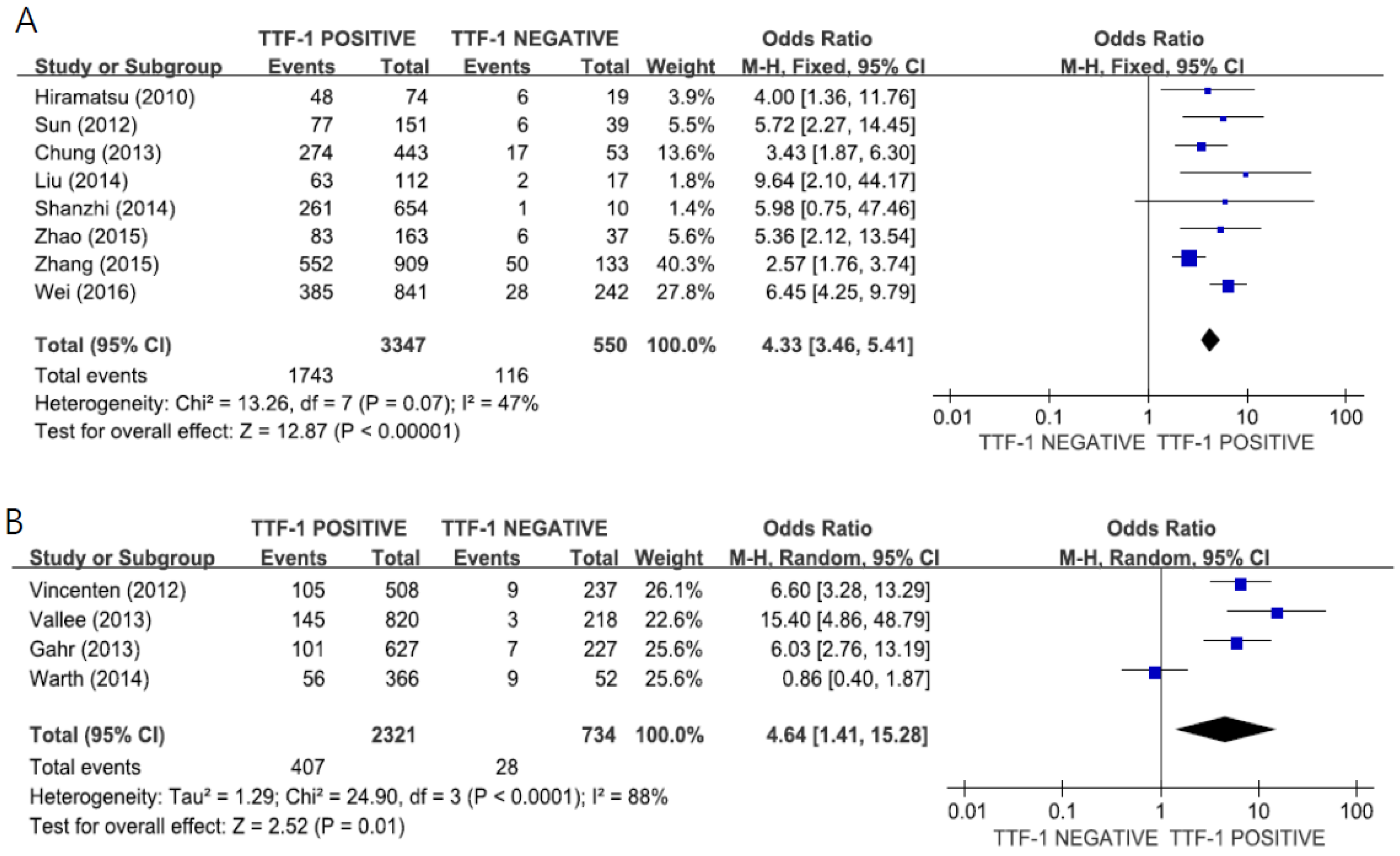
3.3.2. Subgroup Analysis According to the Ethnic Group
3.3.3. Subgroup Analysis According to the Gender
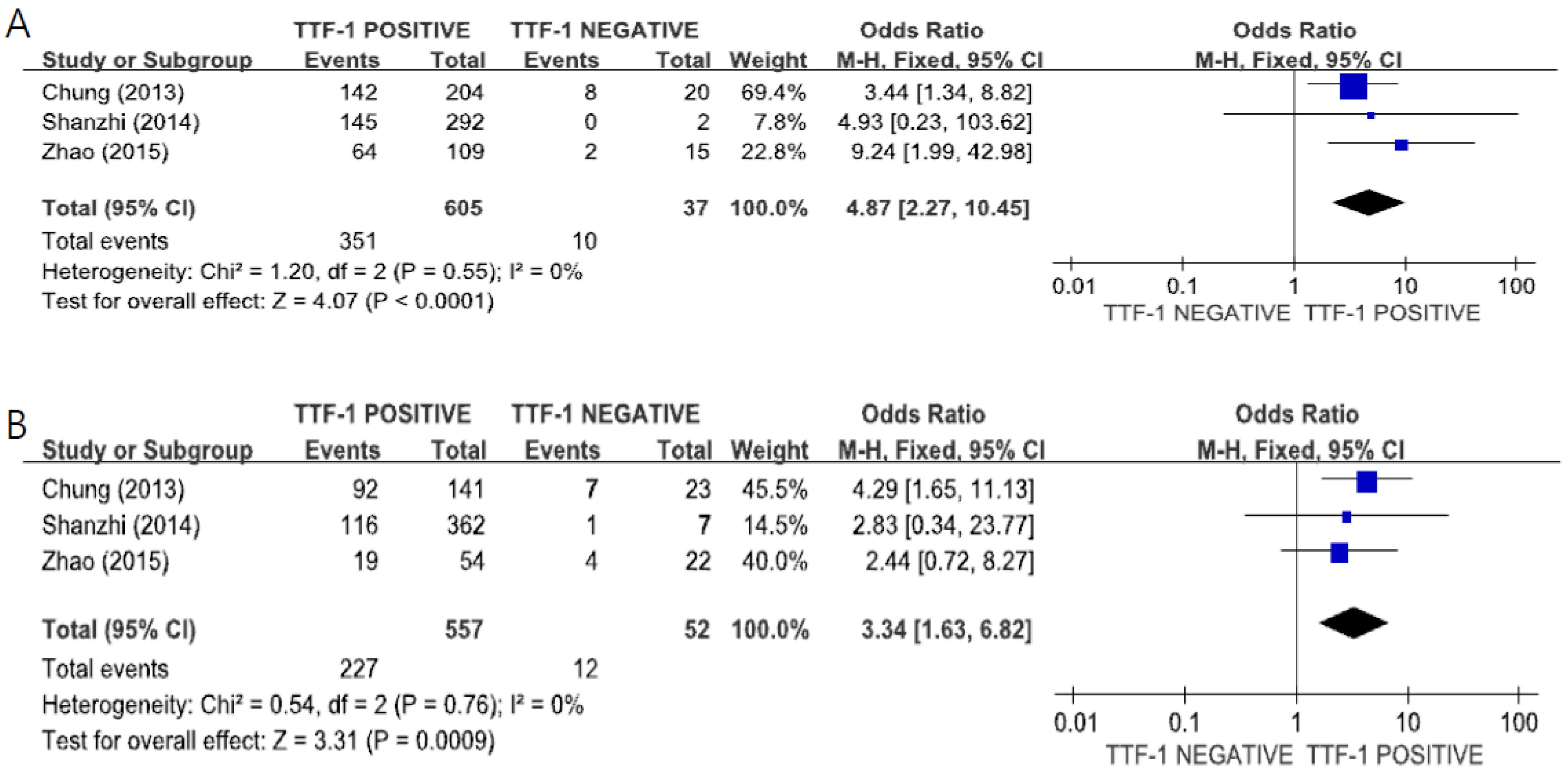
3.3.4. Subgroup Analysis According to the Mutational Subtype
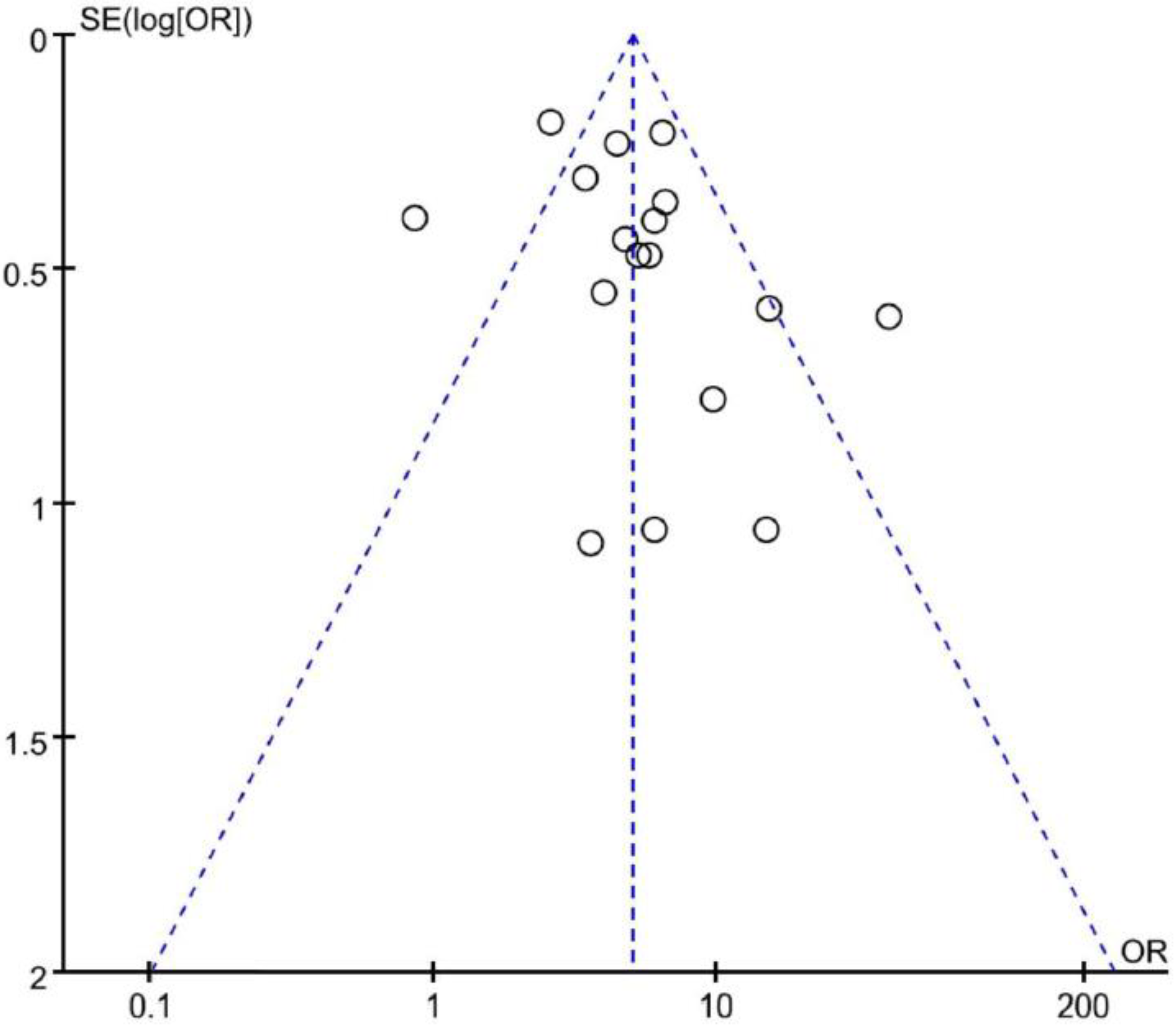
3.4. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA. Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S. Community of population-based regional cancer registries. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2015. Cancer Res. Treat. 2018, 50, 303–316. [Google Scholar] [CrossRef] [PubMed]
- NSCLC Meta-Analyses Collaborative Group. Chemotherapy in addition to supportive care improves survival in advanced non-small-cell lung cancer: A systematic review and meta-analysis of individual patient data from 16 randomized controlled trials. J. Clin. Oncol. 2008, 26, 4617–4625. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: Two-year outcomes from two randomized, open-label, phase III trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef]
- Bulbul, A.; Husain, H. First-line treatment in EGFR mutant non-small cell lung cancer: Is there a best option? Front. Oncol. 2018, 8. [Google Scholar] [CrossRef]
- Guazzi, S.; Price, M.; De Felice, M.; Damante, G.; Mattei, M.G.; Di Lauro, R. Thyroid nuclear factor 1 (TTF-1) contains a homeodomain and displays a novel DNA binding specificity. EMBO J. 1990, 9, 3631–3639. [Google Scholar] [CrossRef]
- Zhang, L.; Whitsett, J.A.; Stripp, B.R. Regulation of Clara cell secretory protein gene transcription by thyroid transcription factor-1. Biochim. Biophys. Acta 1997, 1350, 359–367. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, H.S.; Kim, B.J.; Han, B.; Choi, D.R.; Kwon, J.H. Prognostic impact ofTTF-1 expression in non-squamous non-small-cell lung cancer: A meta-analysis. J. Cancer 2018, 9, 4279–4286. [Google Scholar] [CrossRef]
- Qian, H.H.; Xu, T.S.; Cai, X.Q.; Ji, T.L.; Guo, H.X. Prognostic value of TTF-1 expression in patients with non-small cell lung cancer: A meta-analysis. Clin. Chim. Acta 2015, 451, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Lynch, T.J.; Bell, D.W.; Sordella, R.; Gurubhagavatula, S.; Okimoto, R.A.; Brannigan, B.W.; Harris, P.L.; Haserlat, S.M.; Supko, J.G.; Haluska, F.G.; et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004, 350, 2129–2139. [Google Scholar] [CrossRef]
- Paez, J.G.; Janne, P.A.; Lee, J.C.; Tracy, S.; Greulich, H.; Gabriel, S.; Herman, P.; Kaye, F.J.; Lindeman, N.; Boggon, T.J.; et al. EGFR mutations in lung cancer: Correlation with clinical response to gefitinib therapy. Science 2004, 304, 1497–1500. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, H.; Gazdar, A.F. Somatic mutations of epidermal growth factor receptor signaling pathway in lung cancers. Int. J. Cancer 2006, 118, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Mitsudomi, T.; Yatabe, Y. Mutations of the epidermal growth factor receptor gene and related genes as determinants of epidermal growth factor receptor tyrosine kinase inhibitors sensitivity in lung cancer. Cancer Sci. 2007, 98, 1817–1824. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Kosaka, T.; Yatabe, Y.; Endoh, H.; Kuwano, H.; Takahashi, T.; Mitsudomi, T. Mutations of the epidermal growth factor receptor gene in lung cancer: Biological and clinical implications. Cancer Res. 2004, 64, 8919–8923. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Kosaka, T.; Yatabe, Y. Biological and clinical implications of EGFR mutations in lung cancer. Int. J. Clin. Oncol. 2006, 11, 190–198. [Google Scholar] [CrossRef]
- Jie, L.; Li, X.Y.; Zhao, Y.Q.; Liu, R.Q.; Zhang, J.B.; Ma, J.; Chen, L.J.; Hu, X.F. Genotype-phenotype correlation in Chinese patients with pulmonary mixed type adenocarcinoma: Relationship between histologic subtypes, TITF-1/SP-A expressions and EGFR mutations. Pathol. Res. Pract. 2014, 210, 176–181. [Google Scholar]
- Tang, X.; Kadara, H.; Behrens, C.; Liu, D.D.; Xiao, Y.; Rice, D.; Gazdar, A.F.; Fujimoto, J.; Moran, C.; Varella-Garcia, M.; et al. Abnormalities of the TITF-1 lineage-specific oncogene in NSCLC: Implications in lung cancer pathogenesis and prognosis. Clin. Cancer Res. 2011, 17, 2434–2443. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed]
- Eagger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Hiramatsu, M.; Ninomiya, H.; Inamura, K.; Nomura, K.; Takeuchi, K.; Satoh, Y.; Okumura, S.; Nakagawa, K.; Yamori, T.; Matsuura, M.; et al. Activation status of receptor tyrosine kinase downstream pathways in primary lung adenocarcinoma with reference of KRAS and EGFR mutations. Lung Cancer 2010, 70, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Vincenten, J.; Smit, E.F.; Vos, W.; Grünberg, K.; Postmus, P.E.; Heideman, D.A.; Snijders, P.J.; Meijer, G.; Kuik, J.; Witte, B.I.; et al. Negative NKX2-1 (TTF-1) as temporary surrogate marker for treatment selection during EGFR-mutation analysis in patients with non-small-cell lung cancer. J. Thorac. Oncol. 2012, 7, 1522–1527. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.L.; Seol, H.; Lee, H.J.; Yoo, S.B.; Kim, H.; Xu, X.; Jheon, S.; Lee, C.T.; Lee, J.S.; Chung, J.H. High incidence of EGFR mutations in Korean men smokers with no intratumoral heterogeneity of lung adenocarcinomas: Correlation with histologic subtypes, EGFR/TTF-1 expressions, and clinical features. J. Thorac. Oncol. 2012, 7, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.P.; Huang, Y.T.; Chang, Y.L.; Yu, C.J.; Yang, C.H.; Chang, Y.C.; Shih, J.Y.; Yang, P.C. Clinical significance of thyroid transcription factor-1 in advanced lung adenocarcinoma under epidermal growth factor receptor tyrosine kinase inhibitor treatment. Chest 2012, 141, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Vallee, A.; Sagan, C.; Le Loupp, A.G.; Bach, K.; Dejoie, T.; Denis, M.G. Detection of EGFR gene mutations in non-small cell lung cancer: Lessons from a single-institution routine analysis of 1,403 tumor samples. Int. J. Oncol. 2013, 43, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Gahr, S.; Stoehr, R.; Geissinger, E.; Ficker, J.H.; Brueckl, W.M.; Gschwendtner, A.; Gattenloehner, S.; Fuchs, F.S.; Schulz, C.; Rieker, R.J.; et al. EGFR mutational status in a large series of Caucasian European NSCLC patients: Data from daily practice. Br. J. Cancer 2013, 109, 1821–1828. [Google Scholar] [CrossRef] [PubMed]
- Warth, A.; Penzel, R.; Lindenmaier, H.; Brandt, R.; Stenzinger, A.; Herpel, E.; Goeppert, B.; Thomas, M.; Herth, F.J.; Dienemann, H.; et al. EGFR, KRAS, BRAF and ALK gene alterations in lung adenocarcinomas: Patient outcome, interplay with morphology and immunophenotype. Eur. Respir. J. 2014, 43, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Shanzhi, W.; Yiping, H.; Ling, H.; Jianming, Z.; Qiang, L. The relationship between TTF-1 expression and EGFR mutations in lung adenocarcinomas. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Somaiah, N.; Fidler, M.J.; Garrett-Mayer, E.; Wahlquist, A.; Shirai, K.; Buckingham, L.; Hensing, T.; Bonomi, P.; Simon, G.R. Epidermal growth factor receptor (EGFR) mutations are exceptionally rare in thyroid transcription factor (TTF-1)-negative adenocarcinomas of the lung. Oncoscience 2014, 1, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Shiau, C.J.; Babwah, J.P.; da Cunha Santos, G.; Sykes, J.R.; Boerner, S.L.; Geddie, W.R.; Leighl, N.B.; Wei, C.; Kamel-Reid, S.; Hwang, D.M.; et al. Sample features associated with success rates in population-based EGFR mutation testing. J. Thorac. Oncol. 2014, 9, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Elsamany, S.A.; Al-Fayea, T.M.; Alzahrani, A.S.; Abozeed, W.N.; Darwish, W.; Farooq, M.U.; Almadani, A.S.; Bukhari, E.A. Thyroid transcription factor-1 expression in advanced non- small cell lung cancer: Impact on survival outcome. Asian Pac. J. Cancer Prev 2015, 16, 2987–2991. [Google Scholar] [CrossRef]
- Zhao, Q.; Xu, S.; Liu, J.; Li, Y.; Fan, Y.; Shi, T.; Wei, S.; Tang, S.C.; Liu, H.; Chen, J. Thyroid transcription factor-1 expression is significantly associated with mutations in exon 21 of the epidermal growth factor receptor gene in Chinese patients with lung adenocarcinoma. OncoTargets Ther. 2015, 8, 2469–2478. [Google Scholar]
- Zhang, Y.; Wang, R.; Li, Y.; Pan, Y.; Hu, H.; Zhang, Y.; Li, H.; Shen, L.; Yu, Y.; Sun, Y.; et al. Negative thyroid transcription factor 1 expression defines an unfavorable subgroup of lung adenocarcinomas. J. Thorac. Oncol. 2015, 10, 1444–1450. [Google Scholar] [CrossRef]
- Udupa, K.S.; Rajendranath, R.; Sagar, T.G.; Sundersingh, S.; Joseph, T. Dual surrogate markers for rapid prediction of epidermal growth factor receptor mutation status in advanced adenocarcinoma of the lung: A novel approach in resource-limited setting. Indian J. Cancer 2015, 52, 266–268. [Google Scholar] [CrossRef]
- Wei, W.E.; Mao, N.Q.; Ning, S.F.; Li, J.L.; Liu, H.Z.; Xie, T.; Zhong, J.H.; Feng, Y.; Wei, C.H.; Zhang, L.T. An Analysis of EGFR Mutations among 1506 Cases of Non-Small Cell Lung Cancer Patients in Guangxi, China. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Schilsky, J.B.; Ni, A.; Ahn, L.; Datta, S.; Travis, W.D.; Kris, M.G.; Chaft, J.E.; Rekhtman, N.; Hellmann, M.D. Prognostic impact of TTF-1 expression in patients with stage IV lung adenocarcinomas. Lung Cancer 2017, 108, 205–211. [Google Scholar] [CrossRef]
- Li, X.; Wan, L.; Shen, H.; Geng, J.; Nie, J.; Wang, G.; Jia, N.; Dai, M.; Bai, X. Thyroid transcription factor-1 amplification and expressions in lung adenocarcinoma tissues and pleural effusions predict patient survival and prognosis. J. Thorac. Oncol. 2012, 7, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, Y.; Hosomi, Y.; Saito, M.; Ogawa, M.; Hishima, T.; Okamura, T.; Sasaki, J.; Masuda, N. Predictive significance of thyroid transcription factor-1 expression in patients with non-squamous non-small cell lung cancer with wild-type epidermal growth factor receptor treated with erlotinib. Mol. Clin. Oncol. 2016, 5, 14–18. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) [Ref.] | Country | Design | Sample Size | Inclusion Period | Pathology | Tumor Stage | IHC Criteria for TTF-1 (+): Nuclear Staining | Test for EGFR Mutations | TTF-1 Expression | EGFR MT a/t TTF-1 (%) | Significance | NOS Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hiramatsu (2010) [27] | Japan | Pro | 93 | 1998–2001 | ADC | I–IV | Stronger than xenograft staining | PCR | (+): 74 (79.6%) (−): 19 (20.4%) | 48 (64.9%) 6 (31.6%) | p = 0.017 | 6 |
| Vincenten (2012) [28] | Netherlands | Retro | 745 | 2004–2010 | NSCLC | I–IV | Percentage (0–100%) × intensity (0–3) ≥10 | PCR sequencing | (+): 508 (68.2%) (−): 237 (31.8%) | 105 (20.7%) 9 (3.8%) | p < 0.00001 | 8 |
| Sun (2012) [29] | Korea | Retro | 190 | 2006–2010 | NSCLC | NA | Percentage (0–100%) × intensity (0–3) >100 | PCR sequencing | (+): 151 (79.4%) (−): 39 (20.6%) | 77 (60.0%) 6 (15.4%) | p < 0.001 | 8 |
| Chung (2012) [30] | Taiwan | Pro | 496 | 2004–2009 | ADC | IIIB–IV | Any definite nuclear staining | PCR sequencing | (+): 443 (89.3%) (−): 53 (10.7%) | 274 (61.9%) 17 (32.1%) | p < 0.001 | 8 |
| Vallee (2013) [31] | France | Retro | 1038 | 2010–2012 | NSCLC | I–IV | NA | PCR | (+): 820 (79.0%) (−): 218 (21.0% | 145 (17.7%) 3 (1.4%) | p < 0.0001 | 8 |
| Gahr (2013) [32] | Germany | Pro | 854 | 2010 | NSCLC | Mainly IV | NA | Sanger sequencing | (+): 627 (73.4%) (−): 227 (26.6%) | 101 (16.1%) 7 (3.1%) | p < 0.001 | 8 |
| Liu (2014) [21] | China | Pro | 139 | 2008–2011 | ADC | I–III | Intensity (0–3) x reactivity (0–100) > 100 | ARMS PCR | (+): 122 (87.8%) (−): 17 (12.2%) | 63 (51.6%) 2 (11.8%) | p = 0.002 | 7 |
| Warth (2014) [33] | Germany | Retro | 418 | 2002–2008 | ADC | I–IV | NA | Sanger sequencing | (+): 366 (87.6%) (−): 52 (12.4%) | 56 (15.3%) 9 (17.3%) | p = 0.685 | 8 |
| Shanzhi (2014) [34] | China | Pro | 664 | 2010–2013 | ADC | I–IV | >10% of tumor cells | PCR sequencing | (+): 654 (98.5%) (−): 10 (1.5%) | 261 (39.9%) 1 (10%) | p < 0.001 | 8 |
| Somaiah (2014) [35] | USA | NA | 431 | NA | ADC | NA | NA | Allele-specific PCR | (+): 366 (84.9%) (−): 66 (15.3%) | 242 (66.1%) 3 (4.5%) | p < 0.00001 | 8 |
| Shiau (2014) [36] | Canada | Retro | 1736 | 2010–2012 | Non-SQCC | Mainly III–IV | NA | PCR | (+): 1408 (81.1) (−): 328 (18.9) | 327 (23.2) 21 (6.4) | p < 0.00001 | 8 |
| Elsamany (2015) [37] | Egypt | Retro | 80 | 2011–2012 | Non-SQCC | IIIB–IV | NA | NA | (+): 70 ((87.5%) (−): 10 (12.5%) | 20 (28.6%) 1 (10%) | p = 0.28 | 6 |
| Zhao (2015) [38] | Taiwan | Retro | 200 | 2008–2013 | ADC | I–IV | ≥ 10% of tumor cells | EGFR liquid chip | (+): 163 (81.5%) (−): 37 (18.5%) | 83 (50.9%) 6 (16.2%) | p = 0.000 | 7 |
| Zhang (2015) [39] | China | Pro | 1042 | 2008–2013 | ADC | I–III | Any positive nuclear staining | PCR | (+): 909 (87.26%) (−): 133 (12.8%) | 552 (60.7%) 50 (37.6%) | p < 0.001 | 8 |
| Udupa (2015) [40] | India | NA | 85 | 2009-2013 | ADC | I–IV | NA | ARMS real-time PCR | (+): 68 (80%) (−): 17 (20%) | 33 (48.5%) 1 (5.9%) | p < 0.00001 | 6 |
| Wei (2016) [41] | China | Pro | 1083 | 2010–2016 | NSCLC | I–IV | Tan or brown nuclear staining | ARMS PCR | (+): 841 (77.7%) (−): 242 (22.3%) | 385 (45.8%) 28 (11.6%) | p < 0.001 | 8 |
| Schilsky (2017) [42] | USA | Retro | 479 | 2009–2011 | ADC | IV | Any nuclear reactivity | NA | (+): 383 (80.0%) (−): 96 (20.0%) | 92 (24.0%) 6 (6.3%) | p < 0.001 | 8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Kim, J.H.; Han, B.; Choi, D.R. Correlation of Thyroid Transcription Factor-1 Expression with EGFR Mutations in Non-Small-Cell Lung Cancer: A Meta-Analysis. Medicina 2019, 55, 41. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020041
Kim HS, Kim JH, Han B, Choi DR. Correlation of Thyroid Transcription Factor-1 Expression with EGFR Mutations in Non-Small-Cell Lung Cancer: A Meta-Analysis. Medicina. 2019; 55(2):41. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020041
Chicago/Turabian StyleKim, Hyeong Su, Jung Han Kim, Boram Han, and Dae Ro Choi. 2019. "Correlation of Thyroid Transcription Factor-1 Expression with EGFR Mutations in Non-Small-Cell Lung Cancer: A Meta-Analysis" Medicina 55, no. 2: 41. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020041