Lung Ultrasound B-lines Occurrence in Relation to Left Ventricular Function and Hydration Status in Hemodialysis Patients


Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Clinical and Anthropometric Measurements
2.3. Laboratory Measurements
2.4. Carotid Artery IMT
2.5. Echocardiography
2.6. Lung Ultrasound
2.7. IVC Diameter Measurement
2.8. Bioelectrical Impedance (BIA)
2.9. Statistical Analysis
3. Results
3.1. Study Group
3.2. Comparison of LC Score Categories
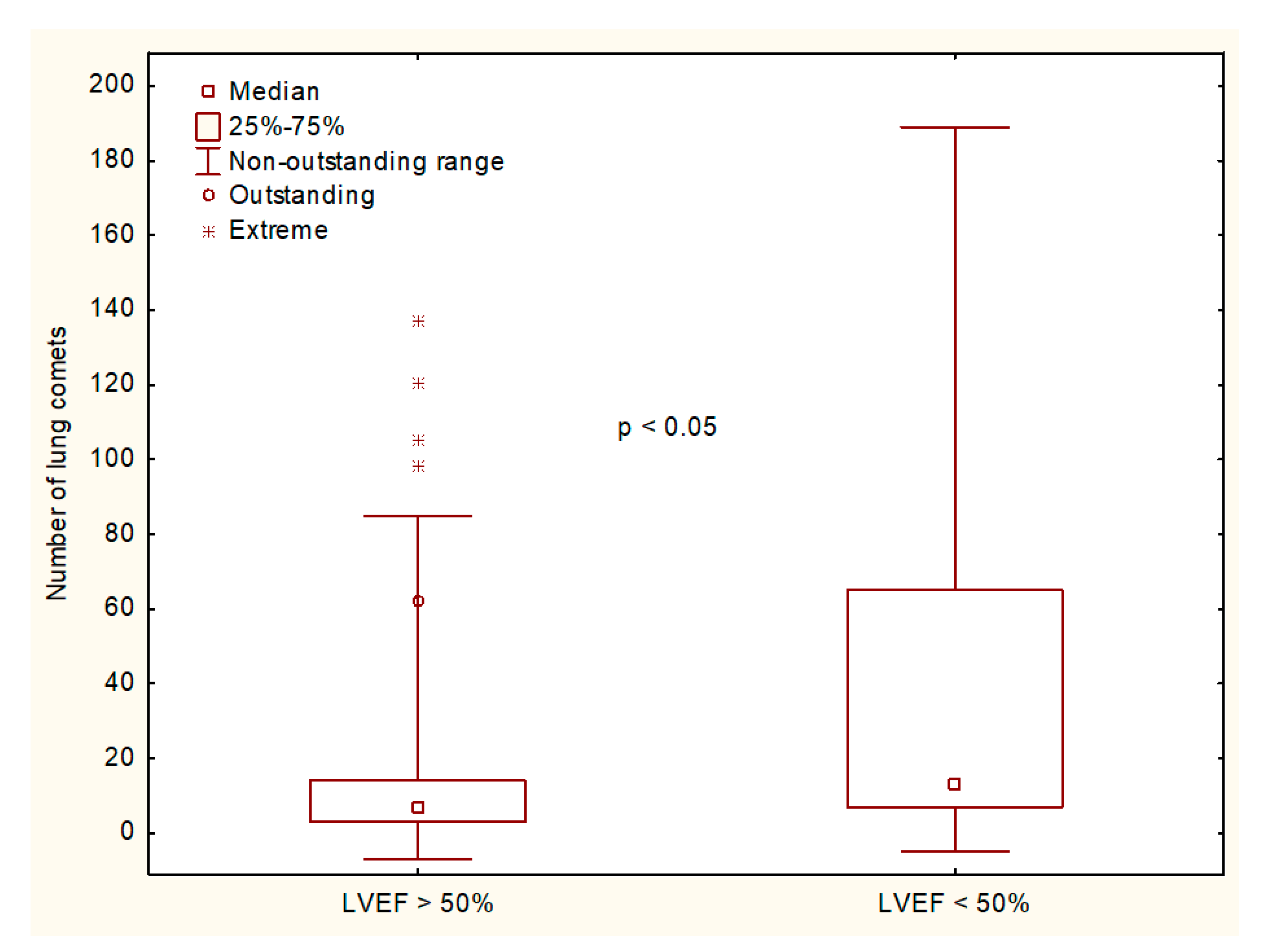
3.3. A Comparison of the Assessments Scored According to LVEF ≥ or < 50%, RVSP Value >35 mmHg, and BIA-Derived RFO > or ≤ 7%
3.4. Multivariate Linear Regression Analysis of the LC Number
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kuhlmann, M.K.; Zhu, F.; Seibert, E.; Levin, N.W. Bioimpedance, dry weight and blood pressure control: New methods and consequences. Curr. Opin. Nephrol. Hypertens. 2005, 14, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Nolan, C.R. Strategies for improving long-term survival in patients with ESRD. J. Am. Soc. Nephrol. 2005, 16 (Suppl. 2), S12–S127. [Google Scholar] [CrossRef] [PubMed]
- Stegmayr, B.G. Ultrafiltration and dry weight—What are the cardiovascular consequences? Artif. Organs 2003, 27, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Basso, F.; Milan Manani, S.; Cruz, D.N.; Teixeira, C.; Brendolan, A.; Nalessio, F.; Zanella, M.; Ronco, C. Comparison and reproducibility of techniques for fluid statsu assessment in chronic hemodialysis patients. Cardiorenal Med. 2013, 3, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, C.; Karabork, M.; Siriopol, D.; Dincer, N.; Covic, A.; Kanbay, M. Effects of volume overload and current techniques for the assessment of fluid status in patients with renal disease. Blood Purif. 2018, 46, 34–47. [Google Scholar] [CrossRef]
- Jambrik, Z.; Monti, S.; Coppola, V.; Agricola, E.; Mottola, G.; Miniati, M.; Picano, E. Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water. Am. J. Cardiol. 2004, 93, 1265–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallamaci, F.; Benedetto, F.A.; Tripepi, R.; Rastelli, S.; Castellino, P.; Tripepi, G.; Picano, E.; Zoccali, C. Detection of pulmonary congestion by chest ultrasound in dialysis patients. JACC Cardiovasc. Imaging 2010, 3, 586–594. [Google Scholar] [CrossRef]
- Weitzel, W.F.; Hamilton, J.; Wang, X.; Bull, J.L.; Vollmer, A.; Bowman, A.; Rubin, J.; Kruger, G.H.; Gao, J.; Heung, M.; et al. Quantitative lung ultrasound comet measurement: Method and initial clinical results. Blood Purif. 2015, 39, 37–44. [Google Scholar] [CrossRef]
- Wang, Z.L.; Liu, J.Y.; Zhou, C.J.; Wang, M.B.; Wang, H.Y.; Xu, Y. Risk factors and impacts on prognosis of ultrasound lung comets in patients undergoing hemodialysis. Zhonghua Yi Xue Za Zhi 2017, 97, 3796–3801. [Google Scholar]
- Unal, A.; Tasdemir, K.; Oymak, S.; Duran, M.; Kocyigit, I.; Oguz, F.; Tokgoz, B.; Sipahioglu, M.H.; Utas, C.; Oymak, O. The long-term effects of arteriovenous fistula creation on the development of pulmonary hypertension in hemodialysis patients. Hemodial. Int. 2010, 14, 398–402. [Google Scholar] [CrossRef]
- Beigi, A.A.; Sadeghi, A.M.; Khosravi, A.R.; Karami, M.; Masoudpour, H. Effects of the arteriovenous fistula on pulmonary artery pressure and cardiac output in patients with chronic renal failure. J. Vasc. Access 2009, 10, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Korsheed, S.; Eldehni, M.T.; John, S.G.; Fluck, R.J.; McIntyre, C.W. Effects of arteriovenous fistula formation on arterial stiffness and cardiovascular performance and function. Nephrol. Dial. Transplant. 2011, 26, 3296–3302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panuccio, V.; Enia, G.; Tripepi, R.; Torino, C.; Garozzo, M.; Battaglia, G.G.; Marcantoni, C.; Infantone, L.; Giordano, G.; De Giorgi, M.L.; et al. Chest ultrasound and hidden lung congestion in peritoneal dialysis patients. Nephrol. Dial. Transplant. 2012, 27, 3601–3605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palazzuoli, A.; Ruocco, G.; Beltrami, M.; Nuti, R.; Cleland, J.G. Combined use of lung ultrasound, B-type natriuretic peptide, and echocardiography for outcome prediction in patients with acute HFrEF and HFpEF. Clin. Res. Cardiol. 2018, 107, 586–596. [Google Scholar] [CrossRef] [PubMed]
- Platz, E.; Lewis, E.F.; Uno, H.; Peck, J.; Pivetta, E.; Merz, A.A.; Hempel, D.; Wilson, C.; Frasure, S.E.; Jhund, P.S.; et al. Detection and prognostic value of pulmonary congestion by lung ultrasound in ambulatory heart failure patients. Eur. Heart J. 2016, 37, 1244–1251. [Google Scholar] [CrossRef] [Green Version]
- Bitar, Z.; Maadarani, O.; Almerri, K. Sonographic chest B-lines anticipate elevated B-type natriuretic peptide level, irrespective of ejection fraction. Ann. Intensive Care 2015, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [PubMed]
- Devereux, R.B.; Reichek, N. Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation 1977, 55, 613–618. [Google Scholar] [CrossRef]
- Gargani, L. Lung ultrasound: A new tool for the cardiologist. Cardiovasc. Ultrasound 2011, 9, 6. [Google Scholar] [CrossRef]
- Torterue, X.; Dehoux, L.; Macher, M.-A.; Niel, O.; Kwon, T.; Deschenes, G.; Hogan, J. Fluid status evaluation by inferior vena cava diameter and bioimpedance spectroscopy in pediatric chronic hemodialysis. BMC Nephrol. 2017, 18, 373. [Google Scholar] [CrossRef]
- Zoccali, C.; Tripepi, R.; Torino, C.; Bellantoni, M.; Tripepi, G.; Mallamaci, F. Lung congestion as a risk factor in end-stage renal disease. Blood Purif. 2013, 36, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Dekker, M.J.E.; Marcelli, D.; Canaud, B.J.; Carioni, P.; Wang, Y.; Grassmann, A.; Konings, C.J.; Kotanko, P.; Leunissen, K.M.; Levin, N.W.; et al. Impact of fluid status and inflammation and their interaction on survival: A study in an international hemodialysis patients cohort. Kindey Int. 2017, 91, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Moissl, U.; Chazot, C.; Mallamaci, F.; Tripepi, G.; Arkossy, O.; Wabel, P.; Stuard, S. Chronic fluid overload and mortality in ESRD. J. Am. Soc. Nephrol. 2017, 28, 2491–2497. [Google Scholar] [CrossRef] [PubMed]
- Dekker, M.J.E.; Kooman, J.P. Fluid status assessment in hemodialysis patients and the association with outcome: Review of recent literature. Curr. Opin. Nephrol. Hypertens. 2018, 27, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Ok, E.; Levin, N.W.; Asci, G.; Chazot, C.; Toz, H.; Ozkahya, M. Interplay of volume, blood pressure, organ ischemia, residual renal function, and diet: Certainties and uncertainties with dialytic management. Semin. Dial. 2017, 30, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Siriopol, D.; Hogas, S.; Voroneanu, L.; Onofriescu, M.; Apetrii, M.; Oleniuc, M.; Moscalu, M.; Sascau, R.; Covic, A. Predicting mortality in haemodialysis patients: A comparison between lung ultrasonography, bioimpedance data and echocardiographic parameters. Nephrol. Dial. Transplant. 2013, 28, 2851–2859. [Google Scholar] [CrossRef] [PubMed]
- Onofriescu, M.; Mardare, N.G.; Segall, L.; Voroneanu, L.; Cusai, C.; Hogas, S.; Ardeleanu, S.; Nistor, I.; Prisada, O.V.; Sascau, R.; et al. Randomized trial of bioelectrical impedance analysis versus clinical criteria for guiding ultrafiltration in hemodialysis patients: Effects on blood pressure, hydration status, and arterial stiffness. Int. Urol. Nephrol. 2012, 44, 583–591. [Google Scholar] [CrossRef]
- Alexiadis, G.; Panagoutsos, S.; Roumeliotis, S.; Stiniris, I.; Markos, A.; Kantartzi, K.; Passadakis, P. Comparison of multiple fluid status assessment methods in patients on chronic hemodialysis. Int. Urol. Nephrol. 2017, 49, 525–532. [Google Scholar] [CrossRef]
- Siriopol, D.; Onofriescu, M.; Voroneanu, L.; Apetrii, M.; Nistor, I.; Hogas, S.; Kanbay, M.; Sascau, R.; Scripcariu, D.; Covic, A. Dry weight assessment by combined ultrasound and bioimpedance monitoring in low cardiovascular risk hemodialysis patients: A randomized controlled trial. Int. Urol. Nephrol. 2017, 49, 143–153. [Google Scholar] [CrossRef]
- Siriopol, D.; Voroneanu, L.; Hogas, S.; Apetrii, M.; Gramaticu, A.; Dumea, R.; Burlacu, A.A.; Sascau, R.; Kanbay, M.; Covic, A. Bioimpedance analysis versus lung ultrasonography for optimal risk prediction in hemodialysis patients. Int. J. Cardiovasc. Imaging 2016, 32, 263–270. [Google Scholar] [CrossRef]
- Davies, S.J.; Davenport, A. A role of bioimpedance and biomarkers in helping to aid clinical decision-making of volume assessment in dialysis patients. Kidney Int. 2014, 86, 489–496. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Lung Comets Score | Statistics | ||||||
|---|---|---|---|---|---|---|---|
| <14 Group 1 n = 76 | 14–30 Group 2 n = 16 | >30 Group 3 n = 16 | ANOVA/Chi2 | 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |
| Age (years) | 58 (54–62) | 56 (45–68) | 62 (56–68) | 0.60 | - | - | - |
| Gender (M/F) | 48/28 | 9/7 | 7/9 | 0.15 | - | - | - |
| Dialysis vintage (mo) * | 29 (7–61) | 61 (5–96) | 21 (8–101) | 0.65 ** | - | - | - |
| Vascular access AVF (n, %) Catheter (n, %) | 48 (63.2) 28 (36.8) | 8 (50.0) 8 (50.0) | 10 (62.5) 6 (37.5) | 0.61 | - | - | - |
| Residual diuresis (mL) * | 500 (250–1000) | 450 (50–850) | 500 (50–1000) | 0.53 ** | - | - | - |
| BMI (kg/m2) | 25.5 (24.4–26.6) | 24.9 (21.3–28.5) | 28.7 (25.6–31.8) | 0.07 | - | - | - |
| IMT (mm) | 0.69 (0.67–0.72) | 0.66 (0.61-0.71) | 0.70 (0.64–0.76) | 0.57 | - | - | - |
| LVMI | 165 (152–177) | 174 (137–210) | 169 (143–195) | 0.83 | - | - | - |
| LVEF (%) | 58.4 (56.6–60.3) | 53.1 (47.2–59.0) | 47.8 (40.4–55.2) | <0.001 | 0.26 | 0.006 | 0.26 |
| RVSP (mm Hg) | 32.7 (30.9–34.5) | 36.1 (31.5–40.8) | 38.1 (33.4–42.9) | 0.03 | 0.45 | 0.15 | 0.77 |
| RVSP > 35 mmHg (n, %) | 27 (35.5) | 9 (56.2) | 10 (62.5) | 0.02 | 0.12 | 0.047 | 0.72 |
| LAVI | 30.2 (27.9–32.4) | 33.3 (26.3–40.4) | 40.1 (31.9–48.3) | 0.007 | 0.72 | 0.04 | 0.23 |
| RAVI | 18.6 (17.1–20.1) | 21.2 (17.1–26.4) | 24.6 (15.6–33.4) | 0.04 | 0.61 | 0.15 | 0.66 |
| Mitral valve gradient (mmHg) | 3.3 (3.0–3.6) | 4.3 (2.5–6.1) | 5.4 (2.4–8.5) | 0.02 | 0.58 | 0.08 | 0.48 |
| IVC min/BSA | 4.7 (4.3–5.1) | 4.5 (3.5–5.5) | 6.3 (5.1–7.5) | 0.005 | 0.96 | 0.04 | 0.02 |
| IVC max/BSA | 7.1 (6.7–7.5) | 7.3 (6.1–8.5) | 8.9 (7.9–9.9) | 0.002 | 0.93 | 0.02 | 0.04 |
| RFO | 7.9 (6.2–9.5) | 9.3 (5.5–13.1) | 9.8 (7.2–12.4) | 0.52 | - | - | - |
| NT-proBNP (pg/mL) * | 2695 (1551–5231) | 8173 (4259–14264) | 8559 (3832–44582) | <0.001 ** | 0.08 | <0.001 | 0.55 |
| Title | LVEF ≥ 50% n = 90 | LVEF < 50% n = 18 | p | RVSP ≤ 35 mmHg n = 62 | RVSP > 35 mmHg n = 46 | p | RFO ≤ 7% n = 38 | RFO > 7% n = 70 | p |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 57.4 (53.7–61.0) | 62.7 (58.2–67.2) | 0.21 | 58.1 (54.1–62.1) | 58.4 (53.1–63.7) | 0.94 | 59.3 (54.9–63.7) | 57.7 (53.3–62.1) | 0.63 |
| Gender (M/F) | 54/36 | 10/8 | 0.73 | 40/22 | 24/22 | 0.20 | 21/17 | 44/26 | 0.44 |
| BMI (kg/m2) | 25.6 (24.5–26.7) | 27.4 (24.7–30.0) | 0.20 | 26.0 (24.7–27.3) | 25.7 (24.0–27.4) | 0.77 | 25.9 (24.4–27.5) | 25.7 (24.3–27.0 | 0.80 |
| Dialysis vintage (mo) * | 22 (7–68) | 59 (12–96) | 0.26 ** | 47 (7–77) | 21 (7–52) | 0.22 ** | 34 (7–61) | 28 (6–74) | 0.59 ** |
| Vascular access AVF (n, %) Catheter (n, %) | 56 (62.2) 34 (37.8) | 10 (55.6) 8 (44.4)] | 0.60 | 39 (62.9) 23 (37.1) | 27 (58.7) 19 (41.3) | 0.66 | 25 (65.8) 13 (34.2) | 42 (60.0) 28 (40.0) | 0.56 |
| EDD (mm) | 48.6 (47.5–49.7) | 57.0 (55.1–58.9) | <0.001 | 50.0 (48.4–51.6) | 50.0 (48.4–51.5) | 0.93 | 49.5 (47.7–51.4) | 50.1 (48.7–51.6) | 0.61 |
| ESD (mm) | 29.4 (28.5–30.3) | 40.1 (37.8–42.3) | <0.001 | 31.4 (29.8–33.0) | 30.9 (29.3–32.5) | 0.69 | 31.4 (29.6–33.2) | 30.9 (29.5–32.3) | 0.65 |
| IVS (mm) | 13.3 (12.7–13.8) | 13.4 (12.6–14.3) | 0.80 | 13.3 (12.6–14.0) | 13.3 (12.7–14.0) | 1.00 | 12.8 (12.1–13.4) | 13.6 (12.9–14.2) | 0.12 |
| PW (mm) | 12.0 (11.4–12.6) | 12.1 (11.2–13.0) | 0.85 | 11.8 (11.1–12.6) | 12.2 (11.5–12.9) | 0.48 | 11.5 (10.7–12.4) | 12.3 (11.6–13.0) | 0.17 |
| LVM (g) | 295 (271–319) | 384 (340–429) | 0.003 | 309 (277–340) | 311 (281–342) | 0.90 | 287 (254–319) | 322 (292–352) | 0.13 |
| LVMI | 158 (147–170) | 207 (178–236) | <0.001 | 164 (148–179) | 170 (156–185) | 0.56 | 154 (140–168) | 173 (158–188) | 0.09 |
| LVH (%) | 78.9 | 94.4 | 0.12 | 79.0 | 84.8 | 0.45 | 86.8 | 78.3 | 0.28 |
| LVEF (%) | 60.0 (58.5–60.8) | 38.1 (33.1–43.0) | <0.001 | 55.1 (52.4–57.7) | 57.4 (54.5–60.3) | 0.25 | 56.7 (54.4–59.0) | 56.2 (53.5–58.8) | 0.78 |
| RVSP | 34.3 (32.5–36.0) | 32.7 (28.6–36.8) | 0.47 | 28.4 (27.1–29.7) | 41.5 (40.0–43.1) | <0.001 | 33.4 (31.1–35.6) | 34.5 (32.4–36.7) | 0.48 |
| LAVI | 30.7 (28.4–33.0) | 39.0 (32.7–45.4) | 0.005 | 29.5 (27.0–32.1) | 35.6 (31.7–39.5) | 0.008 | 31.0 (27.3–34.8) | 32.6 (29.7–35.6) | 0.51 |
| RAVI | 19.1 (17.6–20.5) | 24.2 (16.1–32.3) | 0.03 | 16.8 (15.4–18.3) | 24.1 (20.7–27.5) | <0.001 | 19.2 (16.9–21.6) | 20.5 (17.9–23.0) | 0.52 |
| Mitral valve gradient (mmHg) | 3.8 (3.2-4.5) | 3.5 (2.5–4.5) | 0.64 | 3.1 (2.8–3.5) | 4.7 (3.5–5.8) | <0.001 | 3.5 (2.6–4.5) | 3.9 (3.2–4.6) | 0.48 |
| Lung comets LC 0–13 (n, %) LC 14–30 (n, %) LC > 30 (n, %) | 67 (74.4) 13 (14.4) 10 (11.1) | 9 (50.0) 3 (16.7) 6 (33.3) | 0.04 | 49 (79.0) 7 (11.3) 6 (9.7) | 27 (58.7) 9 (19.6) 10 (21.7) | 0.07 | 28 (73.7) 6 (15.8) 4 (10.5) | 49 (70.0) 10 (14.3) 11 (15.7) | 0.76 |
| IVC min/BSA | 4.8 (4.4–5.1) | 5.6 (4.2–7.0) | 0.1 | 4.4 (3.9–4.9) | 5.6 (5.1–6.1) | 0.001 | 4.7 (4.1–5.3) | 5.0 (4.5–5.4) | 0.48 |
| IVC max/BSA | 7.4 (7.0–7.8) | 7.6 (6.3–8.8) | 0.73 | 6.7 (6.3–7.2) | 8.3 (7.8–8.9) | <0.001 | 7.3 (6.7-7.9) | 7.4 (7.0–7.9) | 0.67 |
| RFO | 8.3 (6.8–9.8) | 8.7 (5.2–12.2) | 0.84 | 8.0 (6.2–9.8) | 8.8 (6.8–10.9) | 0.52 | 1.3 (−0.4–3.0) | 12.2 (11.2–13.2) | <0.001 |
| NT-proBNP (pg/mL) * | 2856 (1601–5667) | 13316 (5579–66120) | <0.001 *** | 2810 (1448–9311) | 4556 (2223–9324) | 0.17 *** | 3203 (1331–6255) | 3794 (1880–12024) | 0.07 *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardała, A.; Lupa, M.; Chudek, J.; Kolonko, A. Lung Ultrasound B-lines Occurrence in Relation to Left Ventricular Function and Hydration Status in Hemodialysis Patients. Medicina 2019, 55, 45. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020045
Pardała A, Lupa M, Chudek J, Kolonko A. Lung Ultrasound B-lines Occurrence in Relation to Left Ventricular Function and Hydration Status in Hemodialysis Patients. Medicina. 2019; 55(2):45. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020045
Chicago/Turabian StylePardała, Agnieszka, Mariusz Lupa, Jerzy Chudek, and Aureliusz Kolonko. 2019. "Lung Ultrasound B-lines Occurrence in Relation to Left Ventricular Function and Hydration Status in Hemodialysis Patients" Medicina 55, no. 2: 45. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020045