Resistance Trends and Epidemiology of Citrobacter-Enterobacter-Serratia in Urinary Tract Infections of Inpatients and Outpatients (RECESUTI): A 10-Year Survey



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Data Collection
2.2. Identification of Isolates
2.3. Antimicrobial Susceptibility Testing
2.4. Statistical Analysis
3. Results
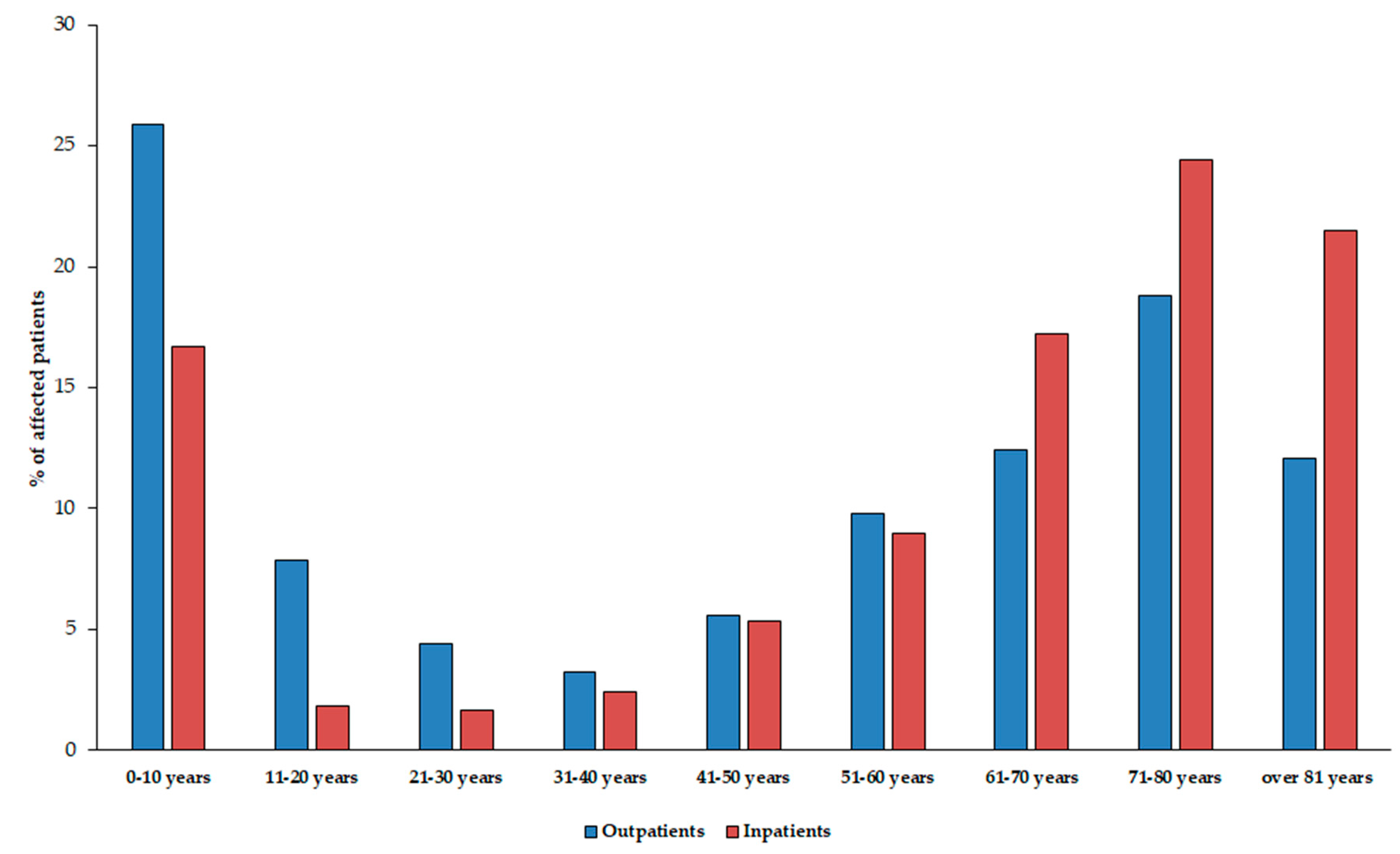
3.1. Demographic Characteristics, Sample Types
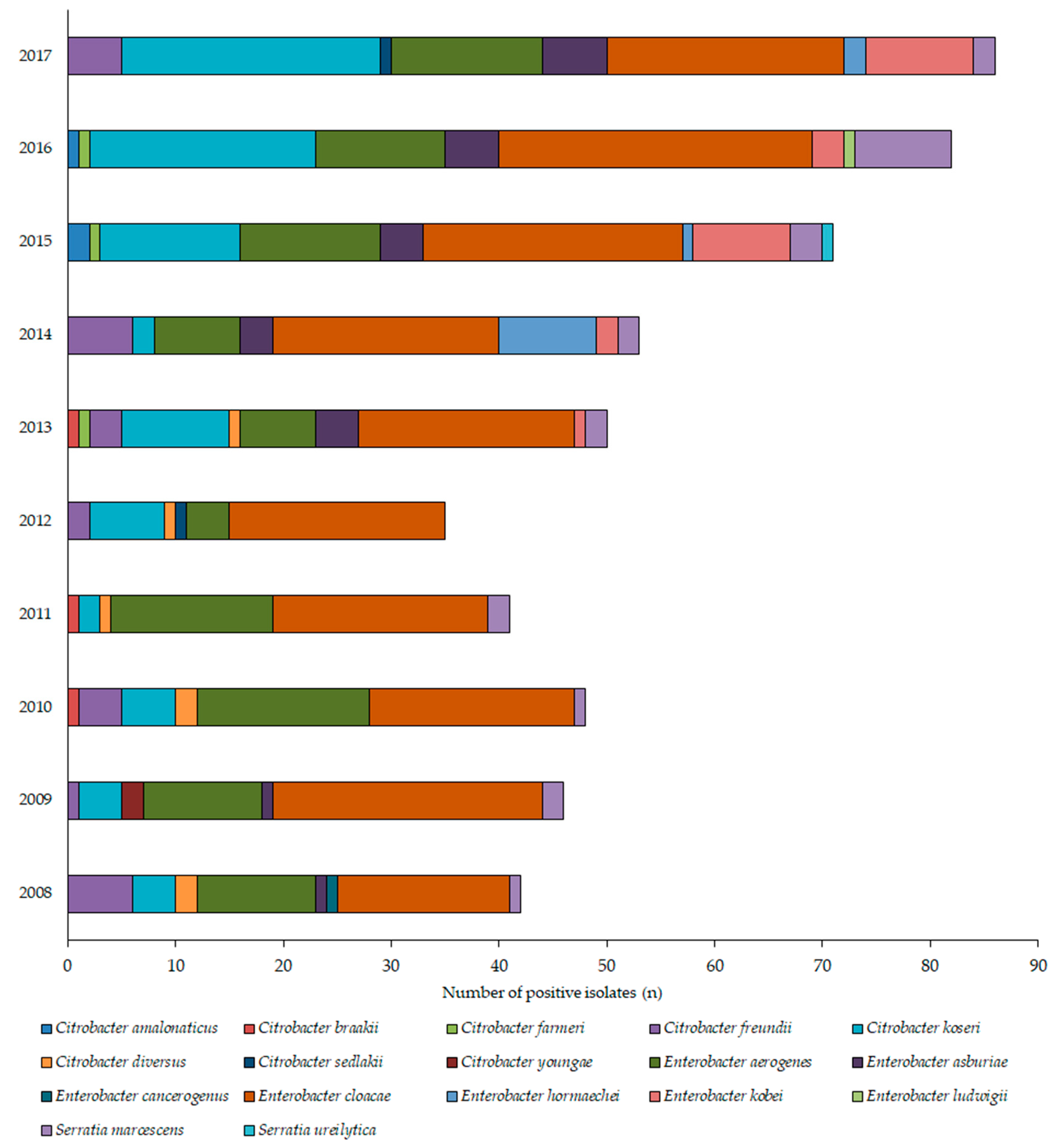
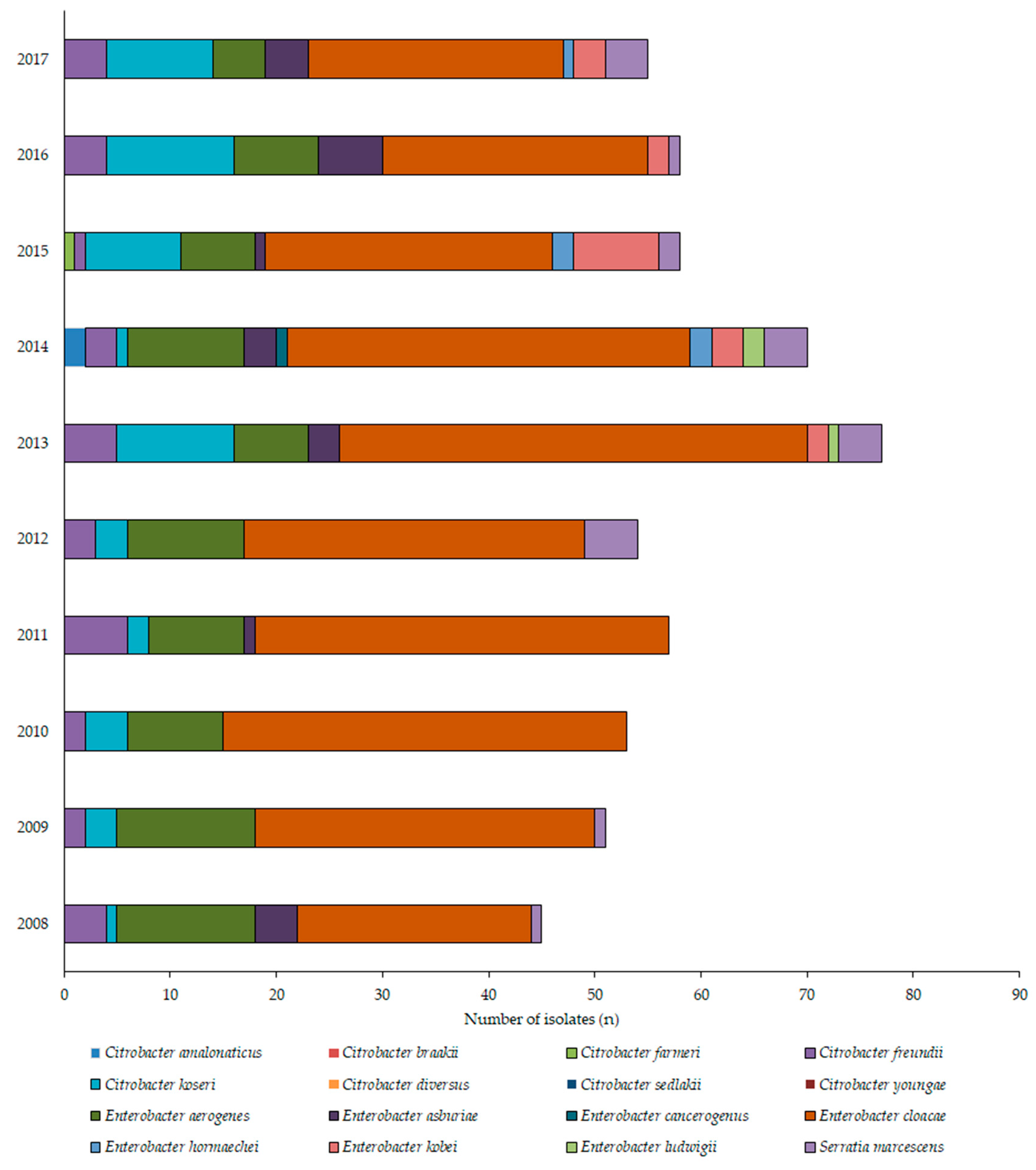
3.2. Distribution of Citrobacter-Enterobacter-Serratia Isolates
3.3. Antibiotic Susceptibility Trends among CES Isolates
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef]
- Wiedemann, B.; Heisig, A.; Heisig, P. Uncomplicated urinary tract infections and antibiotic resistance-epidemiological and mechanistic aspects. Antibiotics 2014, 3, 341–352. [Google Scholar] [CrossRef]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Stefaniuk, E.; Suchocka, U.; Bosacka, K.; Hryniewicz, W. Etiology and antibiotic susceptibility of bacterial pathogens responsible for community-acquired urinary tract infections in Poland. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1363–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calzi, A.; Grignolo, S.; Caviglia, I.; Calevo, M.G.; Losurdo, G.; Piaggio, G.; Bandettini, R.; Castagnola, E. Resistance to oral antibiotics in 4569 Gram-negative rods isolated from urinary tract infection in children. Eur. J. Pediatr. 2016, 175, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D.; Kaye, D. 74-Urinary Tract Infections. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 8th ed.; Bennett, J.E., Dolin, R., Blaser, M.J., Eds.; Content Repository Only: Philadelphia, PA, USA, 2015; pp. 886–913.e3. ISBN 978-1-4557-4801-3. [Google Scholar]
- Leber, A.L. (Ed.) Clinical Microbiology Procedures Handbook, 4th ed.; ASM Press: Washington, DC, USA, 2016; ISBN 978-1-55581-880-7. [Google Scholar]
- Jha, P.; Kim, C.-M.; Kim, D.-M.; Chung, J.-H.; Yoon, N.-R.; Jha, B.; Kim, S.W.; Jang, S.J.; Ahn, Y.-J.; Chung, J.K.; et al. Transmission of Enterobacter aerogenes septicemia in healthcare workers. Springerplus 2016, 5, 1397. [Google Scholar] [CrossRef]
- Cabral, A.B.; Maciel, M.A.V.; Barros, J.F.; Antunes, M.M.; Barbosa de Castro, C.M.M.; Lopes, A.C.S. Clonal spread and accumulation of β-lactam resistance determinants in Enterobacter aerogenes and Enterobacter cloacae complex isolates from infection and colonization in patients at a public hospital in Recife, Pernambuco, Brazil. J. Med. Microbiol. 2017, 66, 70–77. [Google Scholar] [CrossRef]
- Davin-Regli, A.; Pagès, J.-M. Enterobacter aerogenes and Enterobacter cloacae; versatile bacterial pathogens confronting antibiotic treatment. Front. Microbiol. 2015, 6, 392. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.-H.; Kim, Y.S.; Chung, J.-W.; Kim, T.H.; Choo, E.J.; Kim, M.-N.; Kim, B.-N.; Kim, N.J.; Woo, J.H.; Ryu, J. Serratia bacteremia in a large university hospital: Trends in antibiotic resistance during 10 years and implications for antibiotic use. Infect. Control Hosp. Epidemiol. 2002, 23, 740–747. [Google Scholar] [CrossRef]
- Laupland, K.B.; Parkins, M.D.; Gregson, D.B.; Church, D.L.; Ross, T.; Pitout, J.D.D. Population-based laboratory surveillance for Serratia species isolates in a large Canadian health region. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 89–95. [Google Scholar] [CrossRef]
- Alvarez, R.; Adan, A.; Martinez, J.A.; Casale, A.; Miro, J.M. Haematogenous Serratia marcescens endophthalmitis in an HIV-infected intravenous drug addict. Infection 1990, 18, 29–30. [Google Scholar] [CrossRef]
- Barabás, E.; Maier, A.; Maier, I.; Cighir, T.; Mártha, O. Multidrug-resistant serratia marcescens strain isolated in a urology unit-case report. Acta Microbiol. Immunol. Hung. 2015, 62, 5–6. [Google Scholar]
- Gupta, N.; Hocevar, S.N.; Moulton-Meissner, H.A.; Stevens, K.M.; McIntyre, M.G.; Jensen, B.; Kuhar, D.T.; Noble-Wang, J.A.; Schnatz, R.G.; Becker, S.C.; et al. Outbreak of Serratia marcescens bloodstream infections in patients receiving parenteral nutrition prepared by a compounding pharmacy. Clin. Infect. Dis. 2014, 59, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Moradigaravand, D.; Boinett, C.J.; Martin, V.; Peacock, S.J.; Parkhill, J. Recent independent emergence of multiple multidrug-resistant Serratia marcescens clones within the United Kingdom and Ireland. Genome Res. 2016, 26, 1101–1109. [Google Scholar] [CrossRef]
- Metri, B.C.; Jyothi, P.; Peerapur, B.V. Antibiotic resistance in Citrobacter spp. isolated from urinary tract infection. Urol. Ann. 2013, 5, 312. [Google Scholar] [CrossRef]
- Mair, E.; Hummler, H.; Haberl, H. Cerebral abscesses due to neonatal Citrobacter koseri infection. Monatsschrif Kinderheilkd. 2016, 164, S175. [Google Scholar]
- Ranjan, K.P.; Ranjan, N. Citrobacter: An emerging health care associated urinary pathogen. Urol. Ann. 2013, 5, 313–314. [Google Scholar] [PubMed]
- Samonis, G.; Karageorgopoulos, D.E.; Kofteridis, D.P.; Matthaiou, D.K.; Sidiropoulou, V.; Maraki, S.; Falagas, M.E. Citrobacter infections in a general hospital: Characteristics and outcomes. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 61–68. [Google Scholar] [CrossRef]
- Leclercq, R.; Cantón, R.; Brown, D.F.J.; Giske, C.G.; Heisig, P.; MacGowan, A.P.; Mouton, J.W.; Nordmann, P.; Rodloff, A.C.; Rossolini, G.M.; et al. EUCAST expert rules in antimicrobial susceptibility testing. Clin. Microbiol. Infect. 2013, 19, 141–160. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of infections caused by extended-spectrum-beta-lactamase-, ampC-, and carbapenemase-producing enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31. [Google Scholar] [CrossRef] [PubMed]
- Baquero, F.; Hortelano, J.G.; Navarro, M.; Scarpellini, A.; Jara, P.; Cañedo, T.; Rodríguez, A. Antibiotherapy of Serratia marcescens septicemia in children. Chemotherapy 1977, 23 (Suppl. 1), 416–422. [Google Scholar] [CrossRef] [PubMed]
- Moy, S.; Sharma, R. Treatment Outcomes in Infections Caused by “SPICE” (Serratia, Pseudomonas, Indole-positive Proteus, Citrobacter, and Enterobacter) Organisms: Carbapenem versus Noncarbapenem Regimens. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/28034519 (accessed on 20 May 2019).
- Codjoe, F.S.; Donkor, E.S. Carbapenem Resistance: A Review. Med. Sci. 2017, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Abraham, O. Appropriate therapy for carbapenem-resistant Enterobacteriaceae (CRE). Int. J. Infect. Dis. 2016, 45, 5. [Google Scholar] [CrossRef] [Green Version]
- Gajdács, M. The Concept of an Ideal Antibiotic: Implications for Drug Design. Molecules 2019, 24, 892. [Google Scholar] [CrossRef]
- Al-Zarouni, M.; Senok, A.; Al-Zarooni, N.; Al-Nassay, F.; Panigrahi, D. Extended-spectrum beta-lactamase-producing Enterobacteriaceae: In vitro susceptibility to fosfomycin, nitrofurantoin and tigecycline. Med. Princ. Pract. 2012, 21, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M. Extra deaths due to pandrug resistant bacteria: A survey of the literature. Egészségfejlesztés 2019, 60, 31–36. [Google Scholar]
- Boucher, H.W.; Talbot, G.H.; Bradley, J.S.; Edwards, J.E.; Gilbert, D.; Rice, L.B.; Scheld, M.; Spellberg, B.; Bartlett, J. Bad Bugs, No Drugs: No ESKAPE! An Update from the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 48, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Nasim, J.; Witek, K.; Kincses, A.; Abdin, A.Y.; Żesławska, E.; Marć, M.A.; Gajdács, M.; Spengler, G.; Nitek, W.; Latacz, G.; et al. Pronounced activity of aromatic selenocyanates against multidrug resistant ESKAPE bacteria. New J. Chem. 2019, 43, 6021–6031. [Google Scholar] [CrossRef] [Green Version]
- Magyar, A.; Köves, B.; Nagy, K.; Dobák, A.; Arthanareeswaran, V.K.A.; Bálint, P.; Wagenlehner, F.; Tenke, P. Spectrum and antibiotic resistance of uropathogens between 2004 and 2015 in a tertiary care hospital in Hungary. J. Med. Microbiol. 2017, 66, 788–797. [Google Scholar] [CrossRef]
- Takhar, S.S.; Moran, G.J. Diagnosis and management of urinary tract infection in the emergency department and outpatient settings. Infect. Dis. Clin. N. Am. 2014, 28, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Yang, F.; Wang, S.; Wang, Q.; Liu, Z.; Feng, W.; Sun, F.; Xia, P. Analysis of the spectrum and antibiotic resistance of uropathogens in outpatients a. tertiary hospital. J. Chemother. 2018, 30, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Paulik, E.; Szabó, A. The opinions of community pharmacists related to antibiotic use and resistance. Acta Pharm. Hung. 2018, 88, 249–252. (In Hungarian) [Google Scholar]
- Hospital Bed Count and Patient Turnover Report 2017; National Health Insurance Fund of Hungary: Budapest, Hungary, 2017.
- Gajdács, M.; Spengler, G.; Urbán, E. Identification and Antimicrobial Susceptibility Testing of Anaerobic Bacteria: Rubik’s Cube of Clinical Microbiology? Antibiotics 2017, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Nagy, E.; Becker, S.; Kostrzewa, M.; Barta, N.; Urban, E. The value of MALDI-TOF MS for the identification of clinically relevant anaerobic bacteria in routine laboratories. J. Med. Microbiol. 2012, 61, 1393–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matuz, M.; Benkő, R.; Hajdú, E.; Viola, R.; Soós, G. Evaluation of ambulatory antibiotic use in Hungary using drug-specific quality indicators. Orv. Hetil. 2013, 154, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Benkő, R.; Matuz, M.; Hajdú, E.; Bor, A.; Doró, P.; Viola, R.; Soós, G. Antibiotic use in the Hungarian hospitals in the last two decades (1996–2015). Orv. Hetil. 2016, 157, 1839–1846. [Google Scholar] [CrossRef]
- Munoz-Davila, M.J.; Yagüe, G.; Salvador, C.; Blazquez, A.; Roig, M.; Segovia, M. Susceptibility to oral antimicrobials among betalactam-resistant Escherichia coli strains causing community urinary tract infections. Clin. Microbiol. Infect. 2012, 18, 415. [Google Scholar]
- Adeolu, M.; Alnajar, S.; Naushad, S.; Gupta, R.S. Genome-based phylogeny and taxonomy of the “Enterobacteriales”: Proposal for Enterobacterales ord. nov. divided into the families Enterobacteriaceae, Erwiniaceae fam. nov., Pectobacteriaceae fam. nov., Yersiniaceae fam. nov., Hafniaceae fam. nov., Morganellaceae fam. nov., and Budviciaceae fam. nov. Int. J. Syst. Evol. Microbiol. 2016, 66, 5575–5599. [Google Scholar]
- Moehring, R.W.; Hazen, K.C.; Hawkins, M.R.; Drew, R.H.; Sexton, D.J.; Anderson, D.J. Challenges in Preparation of Cumulative Antibiogram Reports for Community Hospitals. J. Clin. Microbiol. 2015, 53, 2977–2982. [Google Scholar] [CrossRef] [Green Version]
- Gajdács, M.; Paulik, E.; Szabó, A. The attitude of community pharmacists towards their widening roles in the prevention and treatment of infectious diseases in the southeast region of Hungary. Gyógyszerészet 2019, 63, 26–30. (In Hungarian) [Google Scholar]
- Hooton, T.M. The current management strategies for community-acquired urinary tract infection. Infect. Dis. Clin. N. Am. 2003, 17, 303–332. [Google Scholar] [CrossRef]
- Bader, M.S.; Loeb, M.; Brooks, A.A. An update on the management of urinary tract infections in the era of antimicrobial resistance. Postgrad. Med. 2017, 129, 242–258. [Google Scholar] [CrossRef] [PubMed]
- Pallett, A.; Hand, K. Complicated urinary tract infections: Practical solutions for the treatment of multiresistant Gram-negative bacteria. J. Antimicrob. Chemother. 2010, 65, iii25–iii33. [Google Scholar] [CrossRef] [PubMed]
- Morrissey, I.; Hackel, M.; Badal, R.; Bouchillon, S.; Hawser, S.; Biedenbach, D. A Review of Ten Years of the Study for Monitoring Antimicrobial Resistance Trends (SMART) from 2002 to 2011. Pharmaceuticals 2013, 6, 1335–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Antimicrobial susceptibility of Gram-negative organisms isolated from patients hospitalised with pneumonia in US and European hospitals: Results from the SENTRY Antimicrobial Surveillance Program, 2009-2012. Int. J. Antimicrob. Agents 2014, 43, 328–334. [Google Scholar] [CrossRef]
- Ponce-de-Leon, A.; Rodríguez-Noriega, E.; Morfín-Otero, R.; Cornejo-Juárez, D.P.; Tinoco, J.C.; Martínez-Gamboa, A.; Gaona-Tapia, C.J.; Guerrero-Almeida, M.L.; Martin-Onraët, A.; Vallejo Cervantes, J.L.; et al. Antimicrobial susceptibility of gram-negative bacilli isolated from intra-abdominal and urinary-tract infections in Mexico from 2009 to 2015: Results from the Study for Monitoring Antimicrobial Resistance Trends (SMART). PLoS ONE 2018, 13, e0198621. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Chen, Y.-H.; Lu, P.-L.; Lin, W.-R.; Chen, T.-C.; Lin, C.-Y. Proteus mirabilis urinary tract infection and bacteremia: Risk factors, clinical presentation, and outcomes. J. Microbiol. Immunol. Infect. 2012, 45, 228–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen-Nahum, K.; Saidel-Odes, L.; Riesenberg, K.; Schlaeffer, F.; Borer, A. Urinary tract infections caused by multi-drug resistant Proteus mirabilis: Risk factors and clinical outcomes. Infection 2010, 38, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Juhász, Z.; Benkő, R.; Matuz, M.; Viola, R.; Soós, G.; Hajdú, E. Treatment practice of acute cystitis on the basis of national prescription data. Orv. Hetil. 2014, 155, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Abbo, L.M.; Hooton, T.M. Antimicrobial Stewardship and Urinary Tract Infections. Antibiotics 2014, 3, 174–192. [Google Scholar] [CrossRef] [PubMed]
- Kong, K.-F.; Schneper, L.; Mathee, K. Beta-lactam Antibiotics: From Antibiosis to Resistance and Bacteriology. APMIS 2010, 118, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Cantón, R.; González-Alba, J.M.; Galán, J.C. CTX-M Enzymes: Origin and Diffusion. Front. Microbiol. 2012, 3, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denes, E.; Prouzergue, J.; Ducroix-Roubertou, S.; Aupetit, C.; Weinbreck, P. Antibiotic prescription by general practitioners for urinary tract infections in outpatients. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 3079–3083. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.L.N. Outpatient parenteral antimicrobial therapy. BMJ 2013, 346, f1585. [Google Scholar] [CrossRef] [PubMed]
- Beuk, C.; Hill, C.; Whitehead, S.; Blondel-Hill, E.; Wagner, K.; Cheeptham, N. Determination of susceptibility to fosfomycin and tigecycline of Enterobacteriaceae, particularly Escherichia coli isolates, producing extended-spectrum β-lactamases from multiple regional Canadian hospitals. Can. J. Infect. Dis. Med. Microbiol. 2013, 24, e80–e82. [Google Scholar] [CrossRef]
- Giske, C.G. Contemporary resistance trends and mechanisms for the old antibiotics colistin, temocillin, fosfomycin, mecillinam and nitrofurantoin. Clin. Microbiol. Infect. 2015, 21, 899–905. [Google Scholar] [CrossRef] [Green Version]
- Cascio, A.; Mezzatesta, M.L.; Odierna, A.; Di Bernardo, F.; Barberi, G.; Iaria, C.; Stefani, S.; Giordano, S. Extended-spectrum beta-lactamase-producing and carbapenemase-producing Enterobacter cloacae ventriculitis successfully treated with intraventricular colistin. Int. J. Infect. Dis. 2014, 20, 66–67. [Google Scholar] [CrossRef] [Green Version]
- Doi, Y.; Bonomo, R.A.; Hooper, D.C.; Kaye, K.S.; Johnson, J.R.; Clancy, C.J.; Thaden, J.T.; Stryjewski, M.E.; van Duin, D. Gram-Negative Committee of the Antibacterial Resistance Leadership Group (ARLG)a Gram-Negative Bacterial Infections: Research Priorities, Accomplishments, and Future Directions of the Antibacterial Resistance Leadership Group. Clin. Infect. Dis. 2017, 64, S30–S35. [Google Scholar] [CrossRef]
- Rodríguez, C.; Brengi, S.; Cáceres, M.A.; Mochi, S.; Viñas, M.R.; Rizza, C.A.; Merletti, G.; Bru, E.; Assa, J.D.; Raya, R.R.; et al. Successful management with Fosfomycin + ceftazidime of an infection caused by multiple highly-related subtypes of multidrug-resistant and extensively drug-resistant KPC-producing Serratia marcescens. Int. J. Antimicrob. Agents 2018, 52, 737–739. [Google Scholar] [CrossRef]
- Zhou, M.; Chen, J.; Liu, Y.; Hu, Y.; Liu, Y.; Lu, J.; Zhang, S.; Yu, Y.; Huang, X.; Yang, Q.; et al. In Vitro Activities of Ceftaroline/Avibactam, Ceftazidime/Avibactam, and Other Comparators Against Pathogens from Various Complicated Infections in China. Clin. Infect. Dis. 2018, 67, S206–S216. [Google Scholar] [CrossRef] [PubMed]
- Candel, F.J.; Peñuelas, M. Delafloxacin: Design, development and potential place in therapy. Drug Des. Dev. Ther. 2017, 11, 881–891. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Dóczi, I.; Ábrók, M.; Lázár, A.; Burián, K. Epidemiology of candiduria and Candida urinary tractinfections in inpatients and outpatients: Results from a10-year retrospective survey. Cent. Eur. J. Urol. 2019. accepted. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Overall (±SE) | Statistics | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CIP R% | Outpatient | 2.4 | 23.9 | 18.8 | 26.9 | 8.6 | 7.0 | 5.6 | 8.7 | 6.1 | 5.8 | 11.4 ± 2.7 | p = 0.0189 |
| Inpatient | 36.4 | 37.3 | 45.3 | 54.6 | 44.3 | 40.8 | 8.6 | 8.5 | 6.8 | 3.9 | 28.6 ± 6.1 | ||
| CRO R% | Outpatient | 30.6 | 47.8 | 47.9 | 29.3 | 25.7 | 24.0 | 24.1 | 24.4 | 24.4 | 19.5 | 29.8 ± 3.2 | p = 0.0167 |
| Inpatient | 65.9 | 72.5 | 64.2 | 61.8 | 56.8 | 43.4 | 28.6 | 27.1 | 27.1 | 27. | 47.5 ± 5.9 | ||
| GEN R% | Outpatient | 4.9 | 19.6 | 16.7 | 17.9 | 5.7 | 8.3 | 1.9 | 3.2 | 2.6 | 2.4 | 8.3 ± 2.2 | p = 0.0232 |
| Inpatient | 51.9 | 48.0 | 45.3 | 47.3 | 27.5 | 11.1 | 7.6 | 5.3 | 5.3 | 5. | 25.4 ± 6.5 | ||
| SUM R% | Outpatient | 16.7 | 21.4 | 14.6 | 24.4 | 15.7 | 12.0 | 3.7 | 8.7 | 3.7 | 1.1 | 12.2 ± 2.5 | n.s. (p = 0.0778) |
| Inpatient | 50.0 | 49.0 | 37.3 | 31.8 | 16.1 | 13.2 | 14.3 | 10.2 | 10.2 | 1.9 | 23.5 ± 5.5 | ||
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Overall (±SE) | Statistics | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DOX R% | Outpatient | 31.7 | 30.0 | 27.7 | 38.5 | 35.7 | 32.7 ± 1.9 | p = 0.0342 | |||||
| Inpatient | 48.9 | 44.5 | 33.0 | 39.3 | 40.0 | 41.1 ± 2.7 | |||||||
| FOS R% | Outpatient | 10.0% | 7.4% | 8.7% | 12.2% | 8.1% | 9.3 ± 0.8 | n.s. (p = 0.454) | |||||
| Inpatient | 7.7% | 15.7% | 20.3% | 15.3% | 9.8% | 13.8 ± 2.1 | |||||||
| ESBL % | Outpatient | 0.0 | 0.0 | 8.8 | 9.8 | 2.9 | 8.0 | 1.9 | 4.8 | 1.2 | 2.3 | 3.7 ± 1.2 | (p = 0.0152) |
| Inpatient | 0.0 | 0.0 | 28.3 | 29.1 | 7.8 | 7.9 | 11.4 | 1.7 | 1.7 | 5.9 | 10.9 ± 3.4 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajdács, M.; Urbán, E. Resistance Trends and Epidemiology of Citrobacter-Enterobacter-Serratia in Urinary Tract Infections of Inpatients and Outpatients (RECESUTI): A 10-Year Survey. Medicina 2019, 55, 285. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060285
Gajdács M, Urbán E. Resistance Trends and Epidemiology of Citrobacter-Enterobacter-Serratia in Urinary Tract Infections of Inpatients and Outpatients (RECESUTI): A 10-Year Survey. Medicina. 2019; 55(6):285. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060285
Chicago/Turabian StyleGajdács, Márió, and Edit Urbán. 2019. "Resistance Trends and Epidemiology of Citrobacter-Enterobacter-Serratia in Urinary Tract Infections of Inpatients and Outpatients (RECESUTI): A 10-Year Survey" Medicina 55, no. 6: 285. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060285