Innovative Spine Implants for Improved Augmentation and Stability in Neoplastic Vertebral Compression Fracture

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
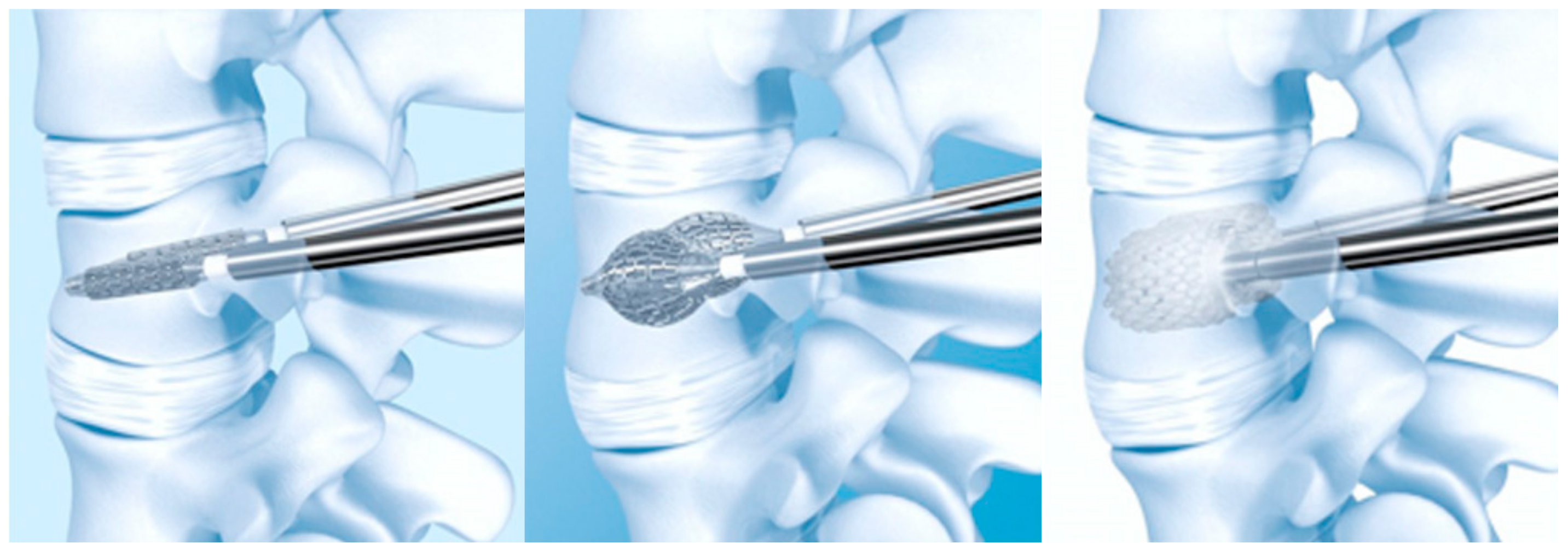
3.1. Vertebral Body Stent®
3.2. Osseofix ®
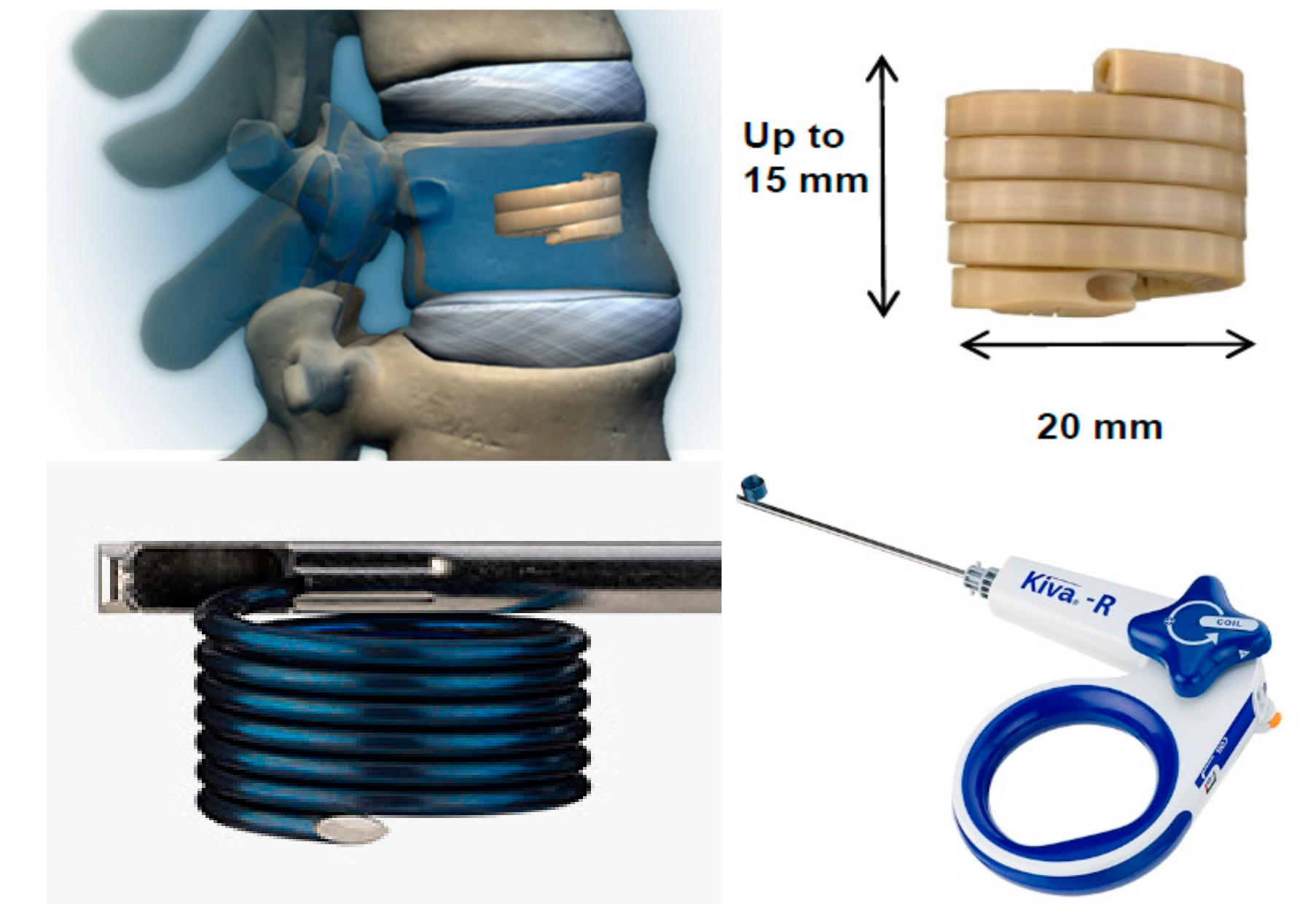
3.3. KIVA® Vertebral Compression Fractures Treatment System
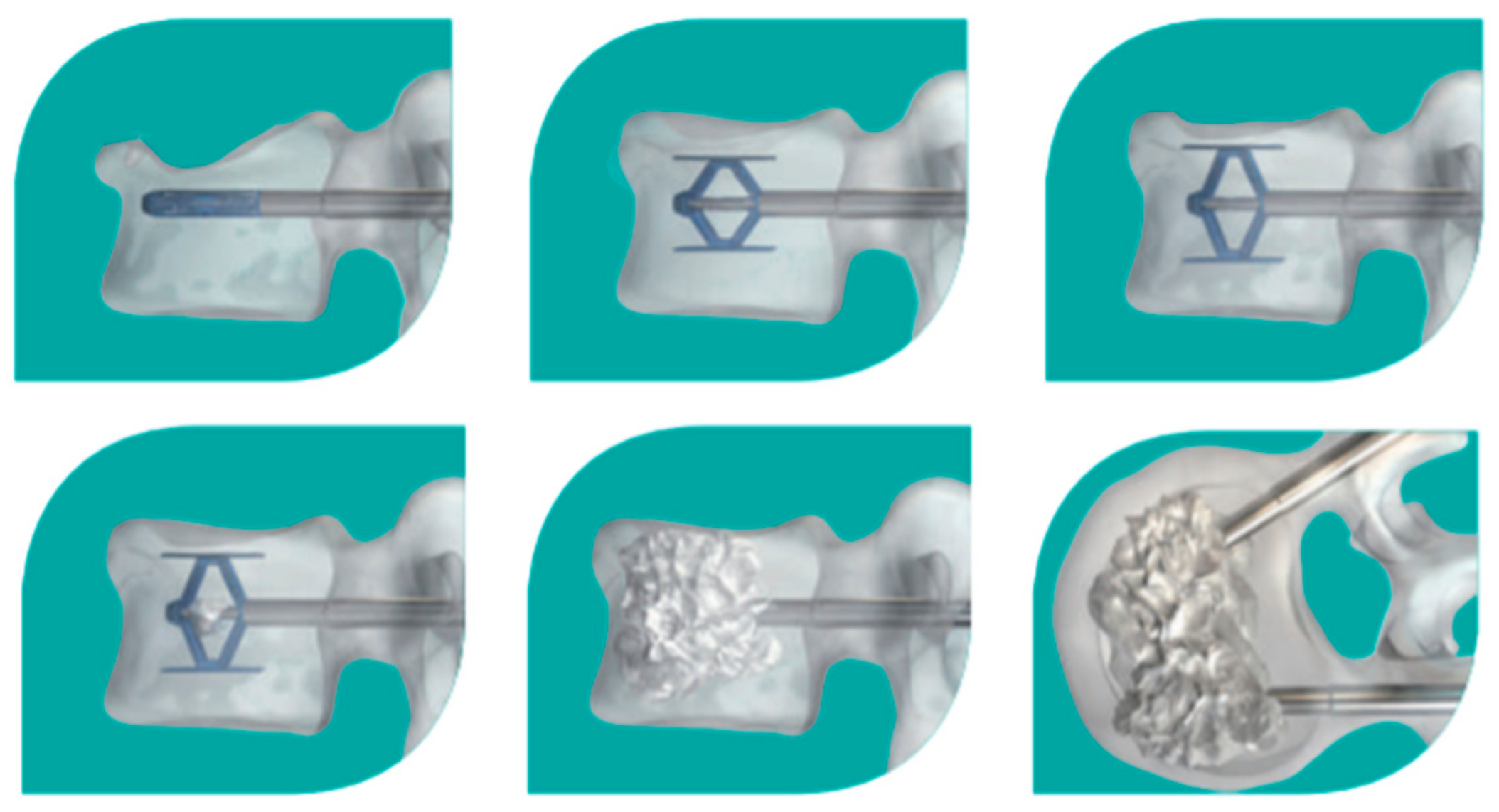
3.4. SpineJack® Expansion Kit
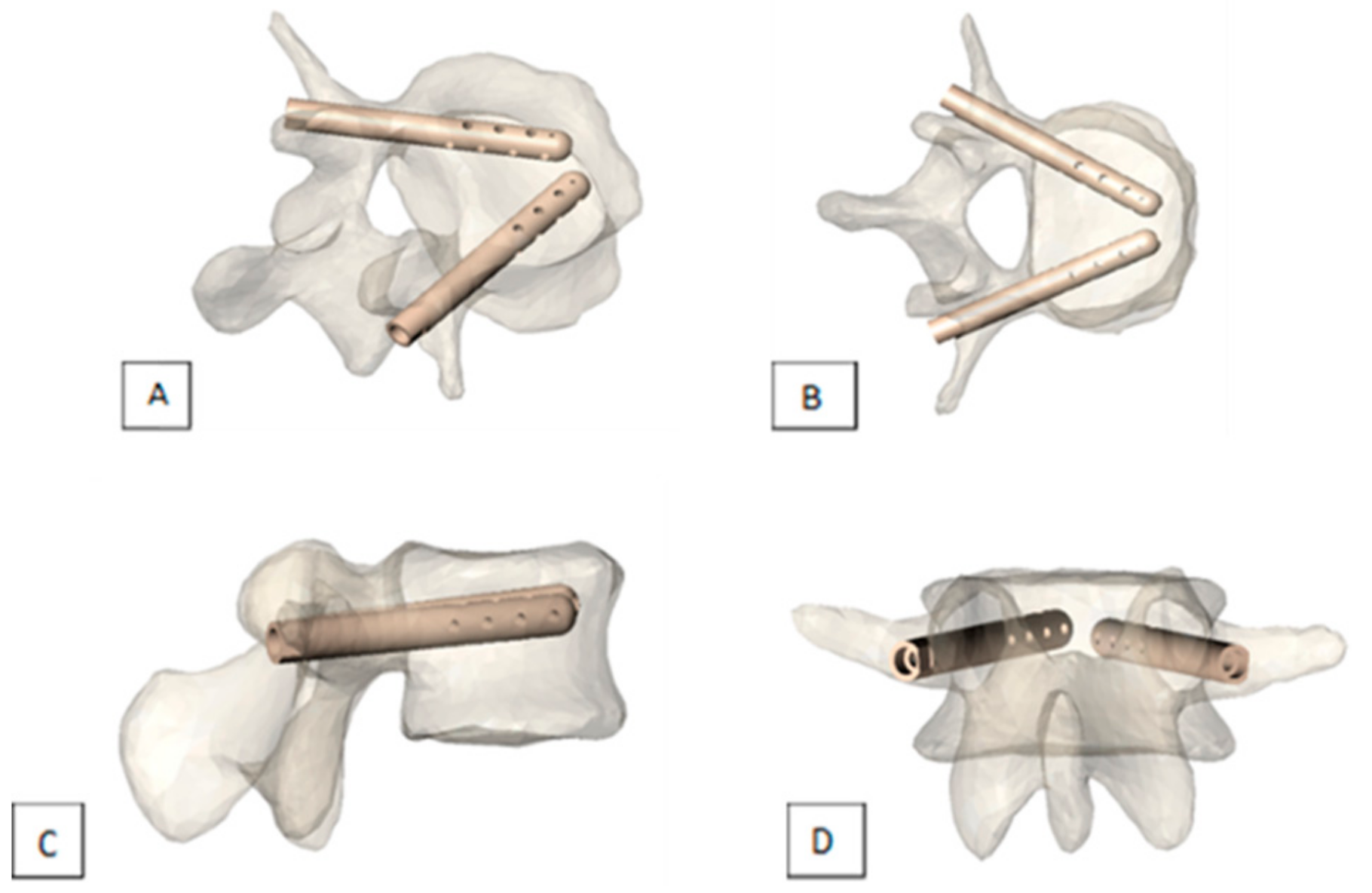
3.5. V-STRUT© Transpedicular Vertebral System
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hazzard, M.A.; Huang, K.T.; Toche, U.N.; Ugiliweneza, B.; Patil, C.G.; Boakye, M.; Lad, S.P. Compression fractures and impact on US healthcare resource utilization. Asian Spine J. 2014, 8, 605. [Google Scholar] [CrossRef]
- Li, C.; Zhang, H.-B.; Zhang, H.; Li, Q.; Zhang, J.; Wang, J.; Guo, K.-J.; Wang, L.-X. Severe pathological fractures caused by vertebral hemangiomas with posterior decompression, bone cement augmentation and internal fixation. Orthop. Traumatol. Surg. Res. 2016, 102, 489–494. [Google Scholar] [CrossRef]
- Becker, N. Epidemiology of Multiple Myeloma. In Side Effects of Medical Cancer Therapy, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 277–284. [Google Scholar] [CrossRef]
- Ali, T.; Bornemann, R.; Roessler, P.P.; Sander, K.; Wirtz, D.C.; Pflugmacher, R.; Frey, S.P. Mid-term outcomes after radiofrequency-targeted vertebral augmentation in the treatment of myeloma associated vertebral fractures. Technol. Heal. Care 2016, 24, 745–751. [Google Scholar] [CrossRef]
- Yuh, W.T.; Zachar, C.K.; Barloon, T.J.; Sato, Y.; Sickels, W.J.; Hawes, D.R. Vertebral compression fractures: Distinction between benign and malignant causes with MR imaging. Radiology 1989, 172, 215–218. [Google Scholar] [CrossRef]
- Bilsky, M.H. New therapeutics in spine metastases. Expert Rev. Neurother. 2005, 5, 831–840. [Google Scholar] [CrossRef]
- Hage, W.D.; Aboulafia, A.J.; Aboulafia, D.M. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orthop. Clin. N. Am. 2000, 31, 515–528. [Google Scholar] [CrossRef]
- Cho, J.H.; Ha, J.-K.; Hwang, C.J.; Lee, D.-H.; Lee, C.S. Patterns of treatment for metastatic pathological fractures of the spine: The efficacy of each treatment modality. Clin. Orthop. Surg. 2015, 7, 476–482. [Google Scholar] [CrossRef]
- Toquart, A.; Graillon, T.; Mansouri, N.; Adetchessi, T.; Blondel, B.; Fuentes, S. Prise en charge des métastases rachidiennes par technique chirurgicale mini-invasive: Principes chirurgicaux, indications: Revue de la littérature Management of spinal metastasis by minimal invasive surgery technique: Surgical principles, indications: A literature review. Neurochirurgie 2016, 62, 157–164. [Google Scholar]
- Boehling, N.S.; Grosshans, D.R.; Allen, P.K.; McAleer, M.F.; Burton, A.W.; Azeem, S.; Rhines, L.D.; Chang, E.L. Vertebral compression fracture risk after stereotactic body radiotherapy for spinal metastases. J. Neurosurg. Spine 2012, 16, 379–386. [Google Scholar] [CrossRef]
- Rose, P.S.; Laufer, I.; Boland, P.J.; Hanover, A.; Bilsky, M.H.; Yamada, J.; Lis, E. Risk of fracture after single fraction image-guided intensity-modulated radiation therapy to spinal metastases. J. Clin. Oncol. 2009, 27, 5075–5079. [Google Scholar] [CrossRef]
- Sahgal, A.; Atenafu, E.G.; Chao, S.; Al-Omair, A.; Boehling, N.; Balagamwala, E.H.; Cunha, M.; Thibault, I.; Angelov, L.; Brown, P.; et al. vertebral compression fracture after spine stereotactic body radiotherapy: A multi-institutional analysis with a focus on radiation dose and the spinal instability neoplastic score. J. Clin. Oncol. 2013, 31, 3426–3431. [Google Scholar] [CrossRef]
- Nomiya, T.; Teruyama, K.; Wada, H.; Nemoto, K. Time course of pain relief in patients treated with radiotherapy for cancer pain. Clin. J. Pain 2010, 26, 38–42. [Google Scholar] [CrossRef]
- Gomez-Iturriaga, A.; Cacicedo, J.; Navarro, A.; Morillo, V.; Willisch, P.; Carvajal, C.; Hortelano, E.; López-Guerra, J.L.; Illescas, A.; Casquero, F.; et al. Incidence of pain flare following palliative radiotherapy for symptomatic bone metastases: Multicenter prospective observational study. BMC Palliat. Care 2015, 14, 84. [Google Scholar] [CrossRef]
- Deramond, H.; Depriester, C.; Toussaint, P.; Galibert, P. Percutaneous vertebroplasty. Semin. Muscol. Radiol. 1997, 1, 285–295. [Google Scholar] [CrossRef]
- Mansoorinasab, M.; Abdolhoseinpour, H. A review and update of vertebral fractures due to metastatic tumors of various sites to the spine: Percutaneous vertebroplasty. Interv. Med. Appl. Sci. 2018, 10, 1–6. [Google Scholar] [CrossRef]
- Health Quality Ontario. Vertebral augmentation involving vertebroplasty or kyphoplasty for cancer-related vertebral compression fractures: A systematic review. Ont. Health Technol. Assess. Ser. 2016, 16, 1–202. [Google Scholar]
- Klezl, Z.; Majeed, H.; Bommireddy, R.; John, J. Early results after vertebral body stenting for fractures of the anterior column of the thoracolumbar spine. Injury 2011, 42, 1038–1042. [Google Scholar] [CrossRef]
- Cianfoni, A.; Distefano, D.; Pravatà, E.; Espeli, V.; Pesce, G.; Mordasini, P.; La Barbera, L.; Scarone, P.; Bonaldi, G. Vertebral body stent augmentation to reconstruct the anterior column in neoplastic extreme osteolysis. J. NeuroInterv. Surg. 2018, 11, 313–318. [Google Scholar] [CrossRef]
- Vanni, D.; Galzio, R.; Kazakova, A.; Pantalone, A.; Grillea, G.; Bartolo, M.; Salini, V.; Magliani, V. Third-generation percutaneous vertebral augmentation systems. J. Spine Surg. 2016, 2, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Muto, M.; Greco, B.; Setola, F.; Vassallo, P.; Ambrosanio, G.; Guarnieri, G. vertebral body stenting system for the treatment of osteoporotic vertebral compression fracture: Follow-up at 12 months in 20 cases. Neuroradiol. J. 2011, 24, 610–619. [Google Scholar] [CrossRef]
- Cornelis, F.H.; Petitpierre, F.; Fabre, T.; Gille, O.; Amoretti, N.; Hauger, O. Percutaneous low-pressure bone stenting to control cement deposition in extensive lytic lesions. Eur. Radiol. 2017, 27, 3942–3946. [Google Scholar] [CrossRef]
- Ender, S.; Gradl, G.; Ender, M.; Langner, S.; Merk, H.; Kayser, R. Osseofix® system for percutaneous stabilization of osteoporotic and tumorous vertebral compression fractures-clinical and radiological results after 12 months. RöFo-Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgebenden Verfahren 2014, 186, 380–387. [Google Scholar] [CrossRef]
- Ender, S.A.; Wetterau, E.; Ender, M.; Kühn, J.-P.; Merk, H.R.; Kayser, R. Percutaneous stabilization system Osseofix® for treatment of osteoporotic vertebral compression fractures-clinical and radiological results after 12 months. PLoS ONE 2013, 8, e65119. [Google Scholar] [CrossRef]
- Eschler, A.; Ender, S.A.; Ulmar, B.; Herlyn, P.; Mittlmeier, T.; Gradl, G. Cementless fixation of osteoporotic VCFs using titanium mesh implants (OsseoFix): Preliminary results. BioMed Res. Int. 2014, 2014, 1–8. [Google Scholar] [CrossRef]
- Velonakis, G.; Filippiadis, D.; Spiliopoulos, S.; Brountzos, E.; Kelekis, N.; Kelekis, A. Evaluation of pain reduction and height restoration post vertebral augmentation using a polyether ether ketone (PEEK) polymer implant for the treatment of split (Magerl A2) vertebral fractures: A prospective, long-term, non-randomized study. Eur. Radiol. 2019, 29, 4050–4057. [Google Scholar] [CrossRef]
- Anselmetti, G.C.; Manca, A.; Tutton, S.; Chiara, G.; Kelekis, A.; Facchini, F.R.; Russo, F.; Regge, D.; Montemurro, F. Percutaneous vertebral augmentation assisted by PEEK implant in painful osteolytic vertebral metastasis involving the vertebral wall: Experience on 40 patients. Pain Phys. 2013, 16, 397–404. [Google Scholar]
- Korovessis, P.; Vardakastanis, K.; Vitsas, V.; Syrimpeis, V. Is kiva implant advantageous to balloon kyphoplasty in treating osteolytic metastasis to the spine? Comparison of 2 percutaneous minimal invasive spine techniques. Spine 2014, 39, E231–E239. [Google Scholar] [CrossRef]
- Filippiadis, D.K.; Marcia, S.; Ryan, A.; Beall, D.P.; Masala, S.; Deschamps, F.; Kelekis, A. New implant-based technologies in the spine. Cardiovasc. Interv. Radiol. 2018, 41, 1463–1473. [Google Scholar] [CrossRef]
- Aebi, M.; Maas, C.; Treuheim, T.D.P.V.; Friedrich, H.; Wilke, H.-J. Comparative biomechanical study of a new transpedicular vertebral device and vertebroplasty for the treatment or prevention of vertebral compression fractures. Clin. Biomech. 2018, 56, 40–45. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | No. of Patients | Technique | Anesthesia | Guidance | Follow-up | Pain | Function | VB height | Complications |
|---|---|---|---|---|---|---|---|---|---|
| [19] | 29 patients for 41 VCF | VBS | 17 CS 12 GA | Biplane fluoroscopy | Mean 15.3m | NA | NA | 75.6% excellent reconstruction 97% spine stabilization on follow-up | 34% cement leakage 4 adjacent fractures, no symptoms |
| [23] | 8 tumor patients | Osseofix | GA | Uniplanar fluoroscopy | 12m | −6.5 pts | −40.7% | Significant improvement in kyphotic angle | No perioperative or postoperative complications in tumor patients |
| [27] | 40 spine malignancy patients | KIVA | LA | Fluoroscopy/CT | 12m | −9 pts | −78.1% | NA | 3 new VCF due to additional metastases 16.3% cement leakage |
| [28] | 23 patients for 41 VCF | KIVA | GA | Biplane fluoroscopy | 1m | −5.1 pts | −43% | No significant improvement in VB height and kyphotic angle, due to little deformity preoperatively | No cement leakage No general or surgical complications |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cornelis, F.H.; Joly, Q.; Nouri-Neuville, M.; Ben-Ammar, M.; Kastler, B.; Kastler, A.; Amoretti, N.; Hauger, O. Innovative Spine Implants for Improved Augmentation and Stability in Neoplastic Vertebral Compression Fracture. Medicina 2019, 55, 426. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080426
Cornelis FH, Joly Q, Nouri-Neuville M, Ben-Ammar M, Kastler B, Kastler A, Amoretti N, Hauger O. Innovative Spine Implants for Improved Augmentation and Stability in Neoplastic Vertebral Compression Fracture. Medicina. 2019; 55(8):426. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080426
Chicago/Turabian StyleCornelis, Francois H., Quentin Joly, Maud Nouri-Neuville, Mohamed Ben-Ammar, Bruno Kastler, Adrian Kastler, Nicolas Amoretti, and Olivier Hauger. 2019. "Innovative Spine Implants for Improved Augmentation and Stability in Neoplastic Vertebral Compression Fracture" Medicina 55, no. 8: 426. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55080426