Open-Healing Socket Preservation with a Novel Dense Polytetrafluoroethylene (dPTFE) Membrane: A Retrospective Clinical Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
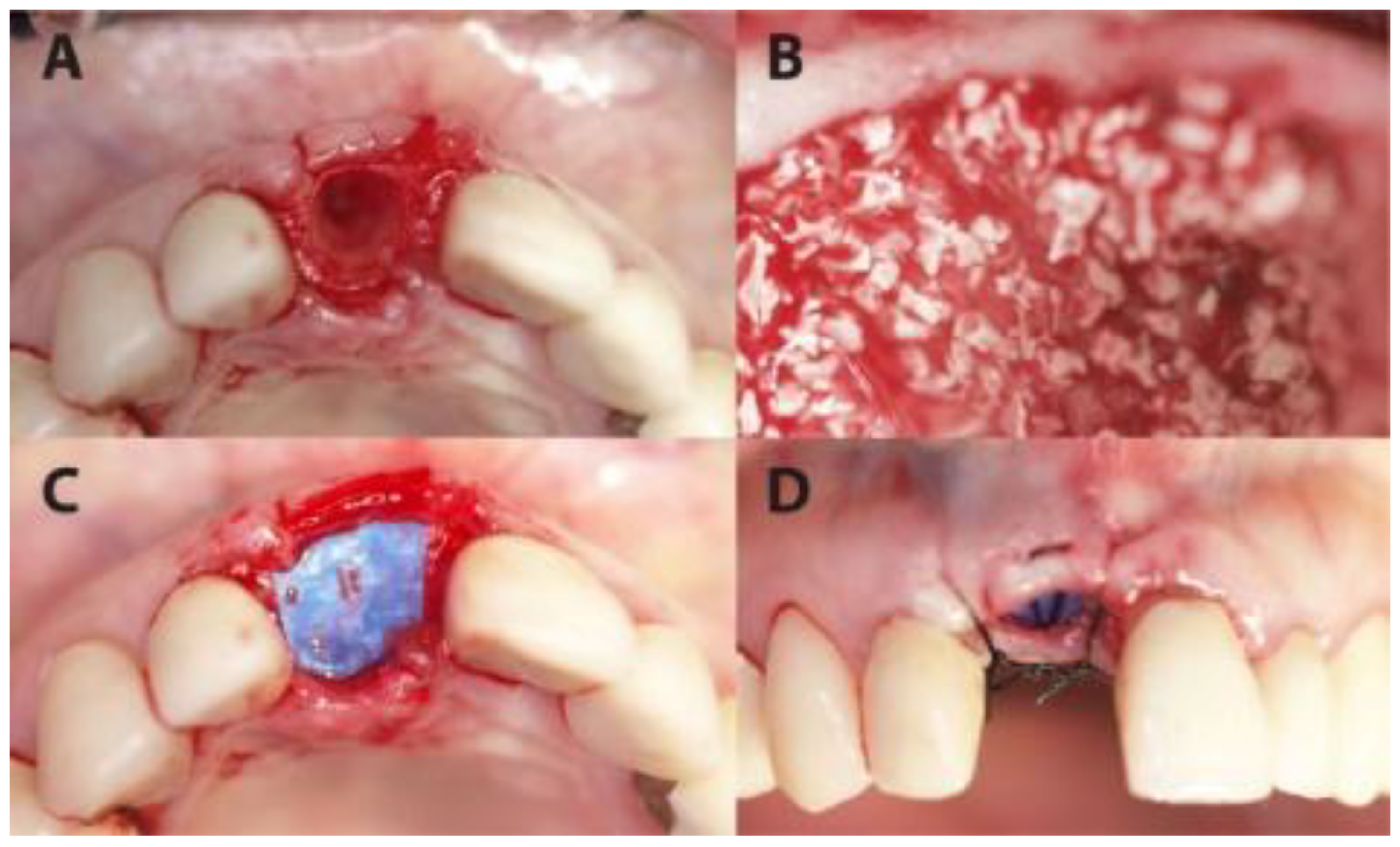
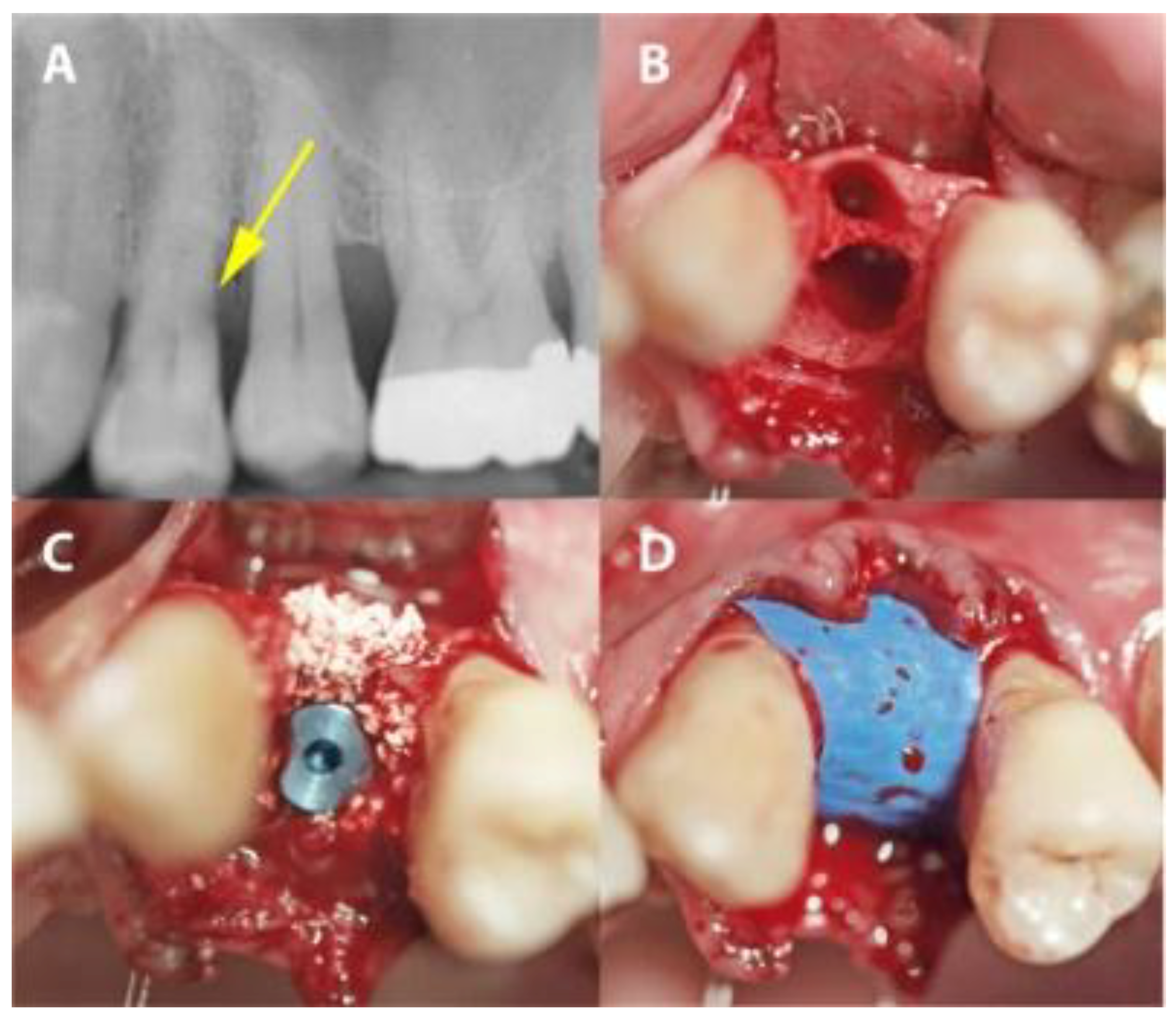
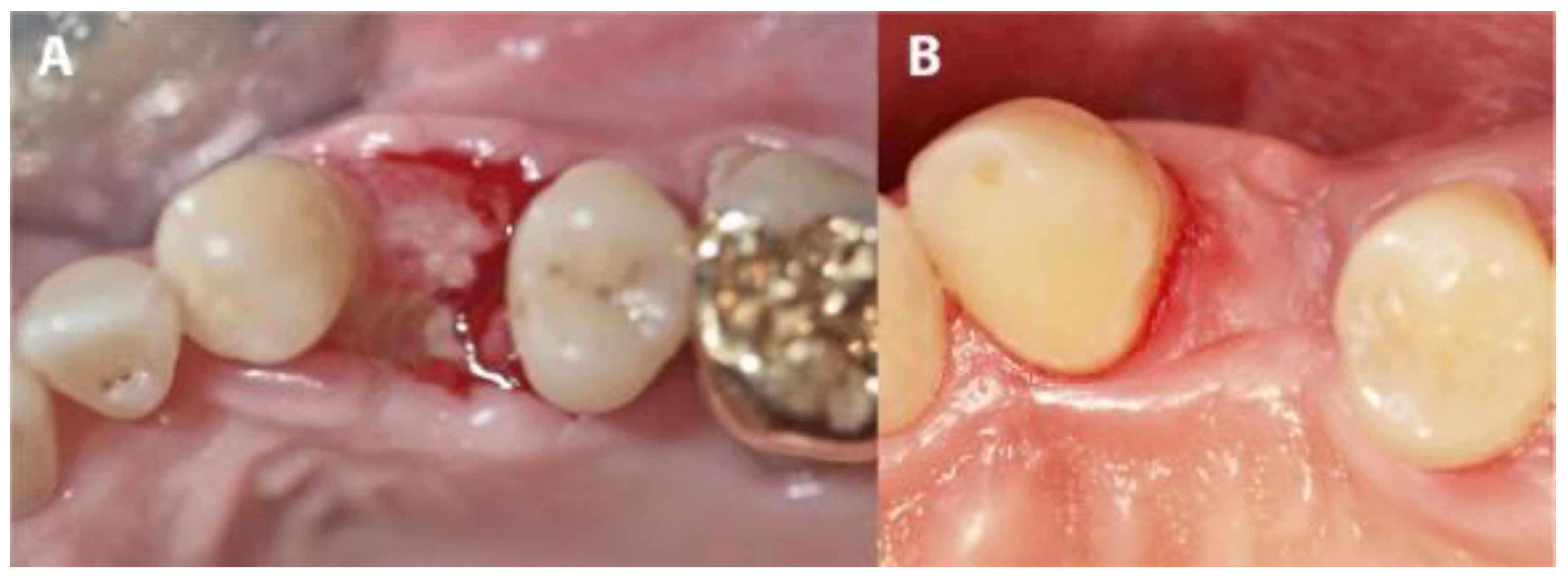
2.2. Surgical Procedure
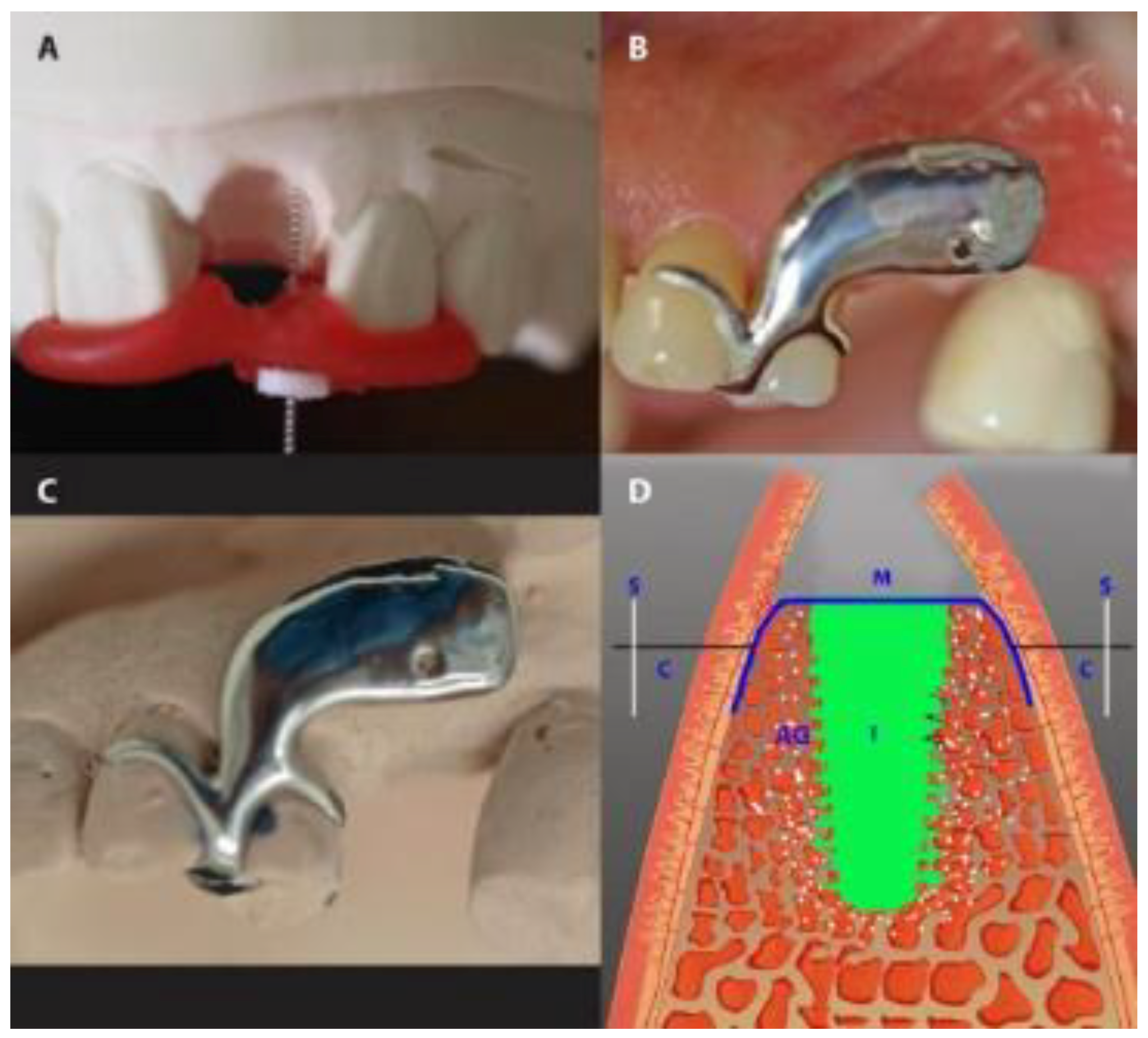
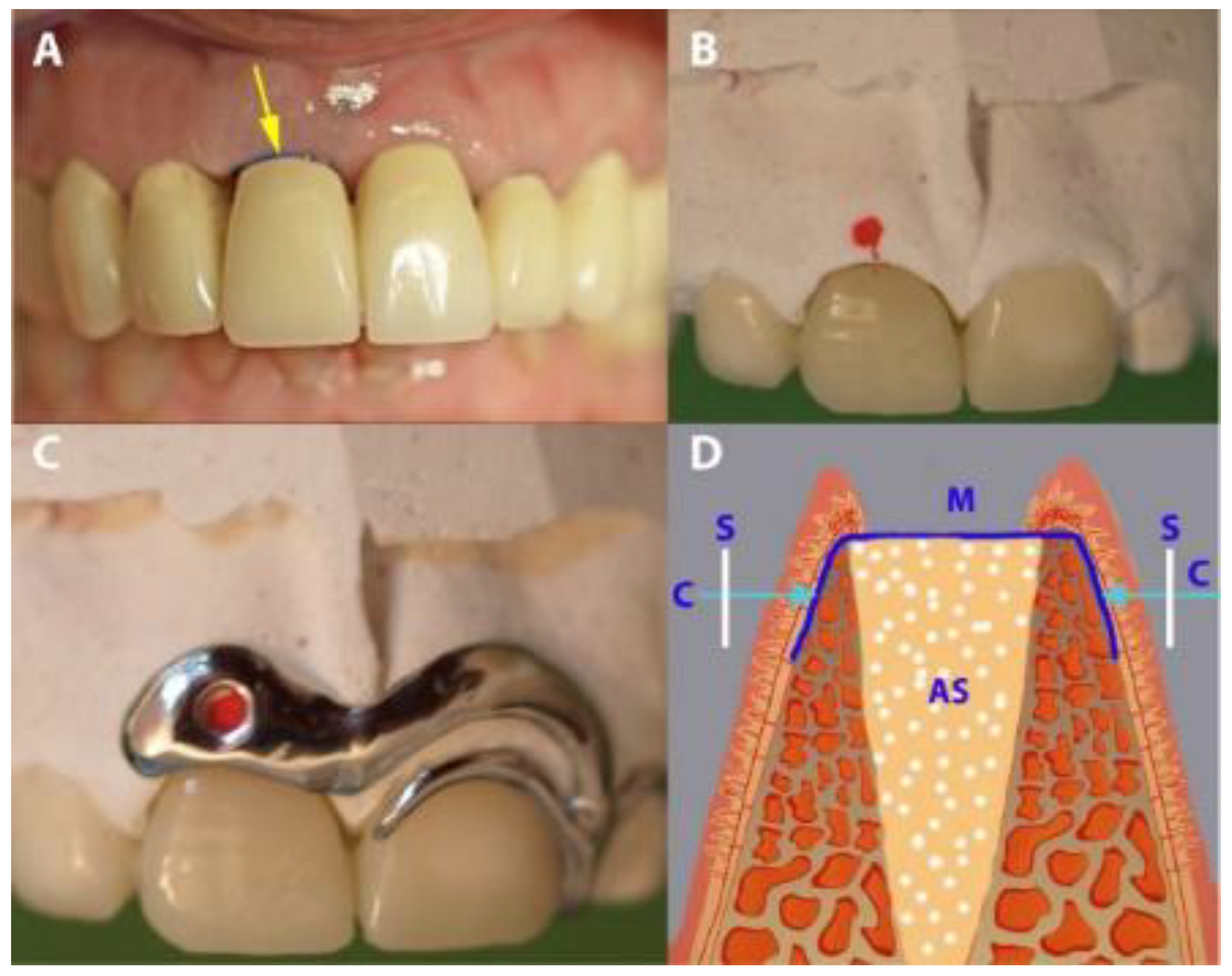
2.3. Measurements and Prosthetic Restoration
2.4. Medication and Postoperative Care
2.5. Prosthetic Restoration
2.6. Data Analysis
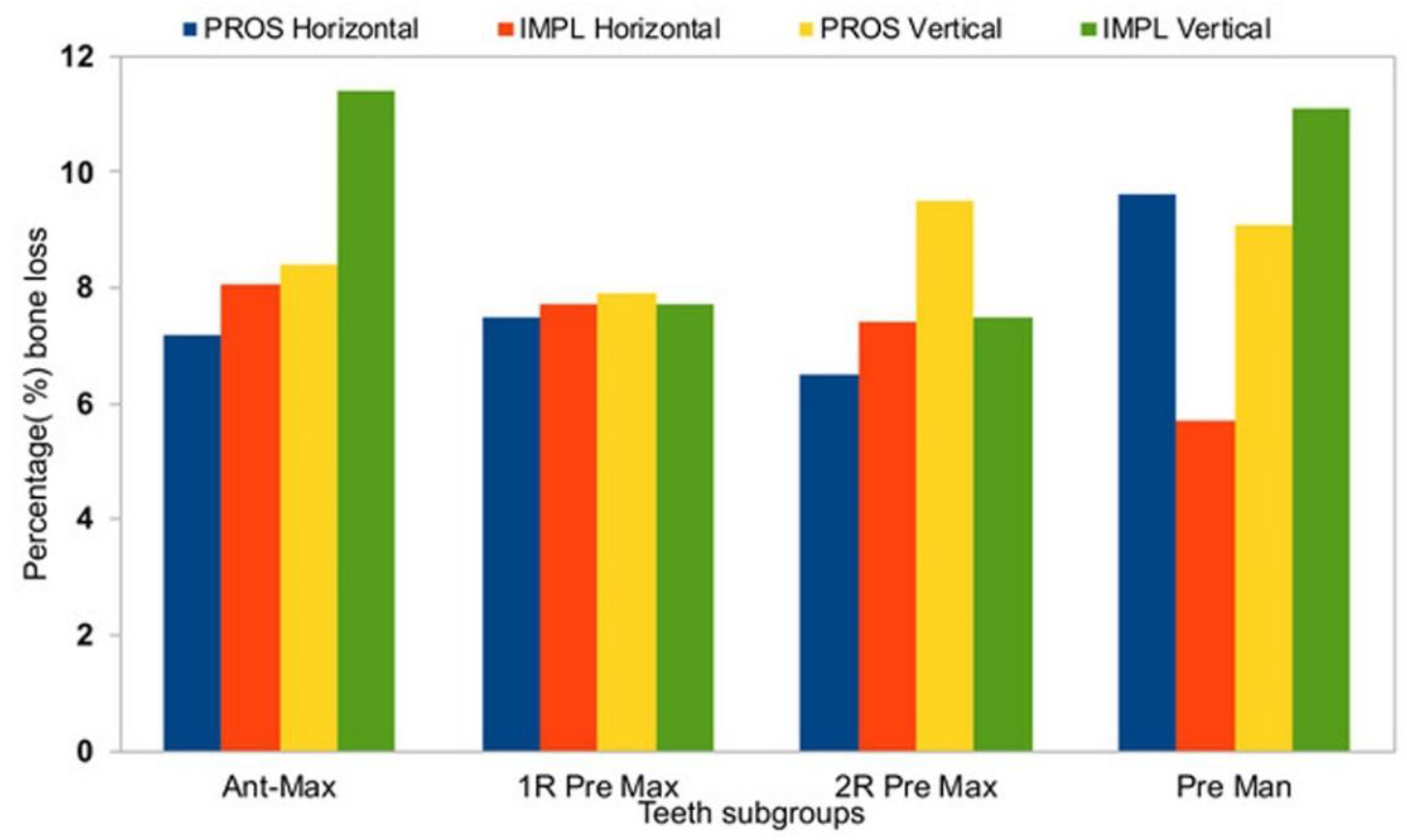
3. Results
4. Discussion
5. Conclusions
Disclosure Statement
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Johnson, K. A study of the dimensional changes occurring in the maxilla following closed face immediate denture treatment*. Aust. Dent. J. 1969, 14, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Pietrokovski, J.; Massler, M. Alveolar ridge resorption following tooth extraction. J. Prosthet. Dent. 1967, 17, 21–27. [Google Scholar] [CrossRef]
- Choquet, V.; Hermans, M.; Adriaenssens, P.; Daelemans, P.; Tarnow, D.P.; Malevez, C. Clinical and Radiographic Evaluation of the Papilla Level Adjacent to Single-Tooth Dental Implants. A Retrospective Study in the Maxillary Anterior Region. J. Periodontol. 2001, 72, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Tarnow, D.; Elian, N.; Fletcher, P.; Froum, S.; Magner, A.; Cho, S.-C.; Salama, M.; Salama, H.; Garber, D.A. Vertical Distance from the Crest of Bone to the Height of the Interproximal Papilla between Adjacent Implants. J. Periodontol. 2003, 74, 1785–1788. [Google Scholar] [CrossRef] [Green Version]
- Rathnayake, N.; Trajkovski, B.; Rahman, B.; Zafiropoulos, G.-G. Clinical applications and outcomes of non-resorbable polytetrafluoroethylene (PTFE) membranes: Review. J. Int. Med. Dent. Res. 2019, 12, 1626–1635. [Google Scholar]
- Lombardi, T.; Bernardello, F.; Berton, F.; Porrelli, D.; Rapani, A.; Camurri Piloni, A.; Fiorillo, L.; Di Lenarda, R.; Stacchi, C. Efficacy of Alveolar Ridge Preservation after Maxillary Molar Extraction in Reducing Crestal Bone Resorption and Sinus Pneumatization: A Multicenter Prospective Case-Control Study. Biomed. Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Barallat, L.; Ruíz-Magaz, V.; Levi, P.A.J.; Mareque-Bueno, S.; Galindo-Moreno, P.; Nart, J. Histomorphometric Results in Ridge Preservation Procedures Comparing Various Graft Materials in Extraction Sockets With Nongrafted Sockets in Humans: A Systematic Review. Implant Dent. 2014, 23, 539–554. [Google Scholar] [CrossRef]
- Troiano, G.; Zhurakivska, K.; Lo Muzio, L.; Laino, L.; Cicciù, M.; Lo Russo, L. Combination of Bone Graft and Resorbable Membrane for Alveolar Ridge Preservation: A Systematic Review, Meta-analysis and Trial Sequential Analysis. J. Periodontol. 2018, 89, 46–57. [Google Scholar] [CrossRef]
- MacBeth, N.; Trullenque-Eriksson, A.; Donos, N.; Mardas, N. Hard and soft tissue changes following alveolar ridge preservation: A systematic review. Clin. Oral Implant. Res. 2017, 28, 982–1004. [Google Scholar] [CrossRef]
- Faria-Almeida, R.; Astramskaite-Januseviciene, I.; Puisys, A.; Correia, F. Extraction Socket Preservation with or without Membranes, Soft Tissue Influence on Post Extraction Alveolar Ridge Preservation: A Systematic Review. J. Oral Maxillofac. Res. 2019, 10. [Google Scholar] [CrossRef]
- Dimitriou, R.; Mataliotakis, G.I.; Calori, G.M.; Giannoudis, P.V. The role of barrier membranes for guided bone regeneration and restoration of large bone defects: Current experimental and clinical evidence. BMC Med. 2012, 10, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldatos, N.K.; Stylianou, P.; Koidou, V.P.; Angelov, N.; Yukna, R.; Romanos, G.E. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017, 48, 131–147. [Google Scholar] [PubMed]
- Hämmerle, C.H.F.; Jung, R.E. Bone augmentation by means of barrier membranes. Periodontol. 2000 2003, 33, 36–53. [Google Scholar]
- Becker, W.; Dahlin, C.; Becker, B.; Lekholm, U.; van Steenberghe, D.; Higuchi, K.; Kultje, C. The use of e-PTFE barrier membranes for bone promotion around titanium implants placed into extraction sockets: A prospective multicenter study. Int. J. Oral Maxillofac. Implant. 1994, 9, 31–40. [Google Scholar]
- Carbonell, J.M.; Martín, I.S.; Santos, A.; Pujol, A.; Sanz-Moliner, J.D.; Nart, J. High-density polytetrafluoroethylene membranes in guided bone and tissue regeneration procedures: A literature review. Int. J. Oral Maxillofac. Surg. 2014, 43, 75–84. [Google Scholar] [CrossRef]
- Lee, J.; Kim, Y.; Yun, P.; Oh, J.; Kim, S. Guided bone regeneration using two types of non-resorbable barrier membranes. J. Korean Assoc. Oral Maxillofac. Surg. 2010, 36, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Bartee, B.K.; Carr, J.A. Evaluation of a high-density polytetrafluoroethylene (n-PTFE) membrane as a barrier material to facilitate guided bone regeneration in the rat mandible. J. Oral Implantol. 1995, 21, 88–95. [Google Scholar]
- Gutta, R.; Baker, R.A.; Bartolucci, A.A.; Louis, P.J. Barrier Membranes Used for Ridge Augmentation: Is There an Optimal Pore Size? J. Oral Maxillofac. Surg. 2009, 67, 1218–1225. [Google Scholar] [CrossRef]
- Hoffmann, O.; Bartee, B.K.; Beaumont, C.; Kasaj, A.; Deli, G.; Zafiropoulos, G.-G. Alveolar Bone Preservation in Extraction Sockets Using Non-Resorbable dPTFE Membranes: A Retrospective Non-Randomized Study. J. Periodontol. 2008, 79, 1355–1369. [Google Scholar] [CrossRef]
- Bartee, B.K. Extraction Site Reconstruction for Alveolar Ridge Preservation. Part 2: Membrane-Assisted Surgical Technique. J. Oral Implantol. 2001, 27, 194–197. [Google Scholar] [CrossRef]
- Barber, H.D.; Lignelli, J.; Smith, B.M.; Bartee, B.K. Using a Dense PTFE Membrane without Primary Closure to Achieve Bone and Tissue Regeneration. J. Oral Maxillofac. Surg. 2007, 65, 748–752. [Google Scholar] [CrossRef]
- Schropp, L.; Isidor, F. Timing of implant placement relative to tooth extraction. J. Oral Rehabil. 2008, 35, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Wilson, T.G.; Hämmerle, C.H.F. Immediate or early placement of implants following tooth extraction: Review of biologic basis, clinical procedures, and outcomes. Int. J. Oral Maxillofac. Implant. 2004, 19, 12–25. [Google Scholar]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Ferro, A.; Botto, J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow-up. Clin. Implant Dent. Relat. Res. 2019, 21, 565–577. [Google Scholar] [CrossRef]
- Schropp, L.; Kostopoulos, L.; Wenzel, A.; Isidor, F. Clinical and radiographic performance of delayed-immediate single-tooth implant placement associated with peri-implant bone defects. A 2-year prospective, controlled, randomized follow-up report. J. Clin. Periodontol. 2005, 32, 480–487. [Google Scholar] [CrossRef]
- Korzinskas, T.; Jung, O.; Smeets, R.; Stojanovic, S.; Najman, S.; Glenske, K.; Hahn, M.; Wenisch, S.; Schnettler, R.; Barbeck, M. In vivo analysis of the biocompatibility and macrophage response of a non-resorbable PTFE membrane for guided bone regeneration. Int. J. Mol. Sci. 2018, 19, 2952. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.E.; Zarb, G.A. Criteria for success of osseointegrated endosseous implants. J. Prosthet. Dent. 1989, 62, 567–572. [Google Scholar] [CrossRef]
- Reddy, K.; Hegde, V.; Aparna, I.N.; Dhanaseka, B. Incorporating modified ovate pontic design for anterior tooth replacement: A report of two cases. J. Indian Prosthodont. Soc. 2009, 9, 100–104. [Google Scholar] [CrossRef]
- Solderer, A.; Kaufmann, M.; Hofer, D.; Wiedemeier, D.; Attin, T.; Schmidlin, P.R. Efficacy of chlorhexidine rinses after periodontal or implant surgery: A systematic review. Clin. Oral Investig. 2019, 23, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- Irinakis, T. Rationale for socket preservation after extraction of a single-rooted tooth when planning for future implant placement. J. Can. Dent. Assoc. 2006, 72, 917–922. [Google Scholar] [PubMed]
- Cardaropoli, G.; Araújo, M.; Hayacibara, R.; Sukekava, F.; Lindhe, J. Healing of extraction sockets and surgically produced—Augmented and non-augmented—Defects in the alveolar ridge. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, G.; Araújo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Marzola, A.; Bozzi, L.; Liljenberg, B.; Lindhe, J. Modeling and remodeling of human extraction sockets. J. Clin. Periodontol. 2008, 35, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Schenk, R.; Buser, D.; Hardwick, W.; Dahlin, C. Healing pattern of bone regeneration in membrane-protected defects: A histologic study in the canine mandible. Int. J. Oral Maxillofac. Implant. 1994, 9, 13–29. [Google Scholar]
- Ronda, M.; Rebaudi, A.; Torelli, L.; Stacchi, C. Expanded vs. dense polytetrafluoroethylene membranes in vertical ridge augmentation around dental implants: A prospective randomized controlled clinical trial. Clin. Oral Implant. Res. 2014, 25, 859–866. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases | Gender, N (%) | Age | Total, N (%) | |
|---|---|---|---|---|
| Female | Male | Mean (Range) | ||
| Treated Cases (Total) | 24 (54.54) | 20 (45.45) | 48.02 (26–42) | 44 (100.0) |
| Tooth type | ||||
| Anterior maxilla | 7 (58.33) | 5 (41.66) | 43.75 (26–63) | 12 (28) |
| 1-root premolar maxilla | 5 (35.71) | 9 (64.28) | 47.14 (32–74) | 14 (32) |
| 2-root premolar maxilla | 4 (44.44) | 5 (55.55) | 52.22 (37–72) | 9 (20) |
| Premolar mandible | 7 (77.77) | 2 (22.22) | 50.88 (35–65) | 9 (20) |
| Treatment group | ||||
| IMPL group (Total) | 12 (48.0) | 13 (52.0) | 50.88 (35–65) | 25 (57) |
| PROS group (Total) | 12 (63.15) | 6 (31.57) | 45.05 (32–65) | 19 (43) |
| Group | Vertical Dimension | Horizontal Dimension | ||||
|---|---|---|---|---|---|---|
| Subgroup | T0 | T1 | p | T0 | T1 | p |
| IMPL | 7.5 ± 1.6 | 7.0 ± 1.6 | 0.121 | 11.9 ± 2.1 | 10.6 ± 2.1 | 0.020 * |
| Anterior maxilla | 6.2 ± 1.6 | 5.7 ± 0.8 | 0.157 | 10.5 ± 1.1 | 9.3 ± 1.3 | 0.067 |
| 1-root premolar maxilla | 7.8 ± 0.7 | 7.2 ± 0.9 | 0.074 | 7.8 ± 0.7 | 7.2 ± 0.9 | 0.074 |
| 2-root premolar maxilla | 9.5 ± 0.8 | 8.8 ± 0.8 | 0.111 | 13.3 ± 1.2 | 12.3 ± 0.9 | 0.140 |
| Premolar mandible | 5.3 ± 0.5 | 5.0 ± 0.7 | 0.211 | 9.0 ± 0.8 | 8.0 ± 0.8 | 0.144 |
| PROS | 6.6 ± 1.7 | 6.1 ± 1.7 | 0.205 | 10.5 ± 1.1 | 9.3 ± 1.4 | 0.043 * |
| Anterior maxilla | 5.7 ± 0.9 | 5.3 ± 1.0 | 0.291 | 11.2 ± 2.2 | 10.3 ± 2.2 | 0.163 |
| 1-root premolar maxilla | 8.0 ± 0.7 | 7.4 ± 0.6 | 0.199 | 12.7 ± 1.9 | 11.8 ± 2.0 | 0.337 |
| 2-root premolar maxilla | 9.3 ± 0.5 | 8.7 ± 0.6 | 0.103 | 9.5 ± 1.3 | 8.6 ± 1.3 | 0.156 |
| Premolar mandible | 5.2 ± 0.4 | 4.7 ± 0.4 | 0.092 | 11.0 ± 2.0 | 10.0 ± 2.1 | 0.064 |
| Dimension | PROS | IMPL | p | ||
|---|---|---|---|---|---|
| Tooth Type | C-mm | %C | C-mm | %C | |
| Horizontal | |||||
| Anterior maxilla | −0.3 ± 0.3 | 7.2 | −0.5 ± 0.4 | 8.06 | 0.23 |
| 1-root premolar maxilla | −0.6 ± 0.5 | 7.5 | −0.6 ± 0.4 | 7.7 | 0.5 |
| 2-root premolar maxilla | −0.7 ± 0.3 | 6.5 | −0.7 ± 0.4 | 7.4 | 0.50 |
| Premolar mandible | −0.5 ± 0.4 | 9.6 | −0.3 ± 0.3 | 5.7 | 0.31 |
| Vertical | |||||
| Anterior maxilla | −1.3 ± 0.5 | 8.4 | −1.2 ± 0.5 | 11.4 | 0.39 |
| 1-root premolar maxilla | −1.0 ± 0.4 | 7.9 | −1.5 ± 0.6 | 7.7 | 0.05 |
| 2-root premolar maxilla | −0.8 ± 0.3 | 9.5 | −1.1 ± 0.6 | 7.5 | 0.26 |
| Premolar mandible | −0.9 ± 0.6 | 9.1 | −1.0 ± 0.0 | 11.1 | 0.41 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafiropoulos, G.-G.; Kačarević, Z.P.; Qasim, S.S.B.; Trajkovski, B. Open-Healing Socket Preservation with a Novel Dense Polytetrafluoroethylene (dPTFE) Membrane: A Retrospective Clinical Study. Medicina 2020, 56, 216. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56050216
Zafiropoulos G-G, Kačarević ZP, Qasim SSB, Trajkovski B. Open-Healing Socket Preservation with a Novel Dense Polytetrafluoroethylene (dPTFE) Membrane: A Retrospective Clinical Study. Medicina. 2020; 56(5):216. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56050216
Chicago/Turabian StyleZafiropoulos, Gregor-Georg, Zeljka Perić Kačarević, Syed Saad B. Qasim, and Branko Trajkovski. 2020. "Open-Healing Socket Preservation with a Novel Dense Polytetrafluoroethylene (dPTFE) Membrane: A Retrospective Clinical Study" Medicina 56, no. 5: 216. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56050216