Disparities in Access to Autologous Breast Reconstruction

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
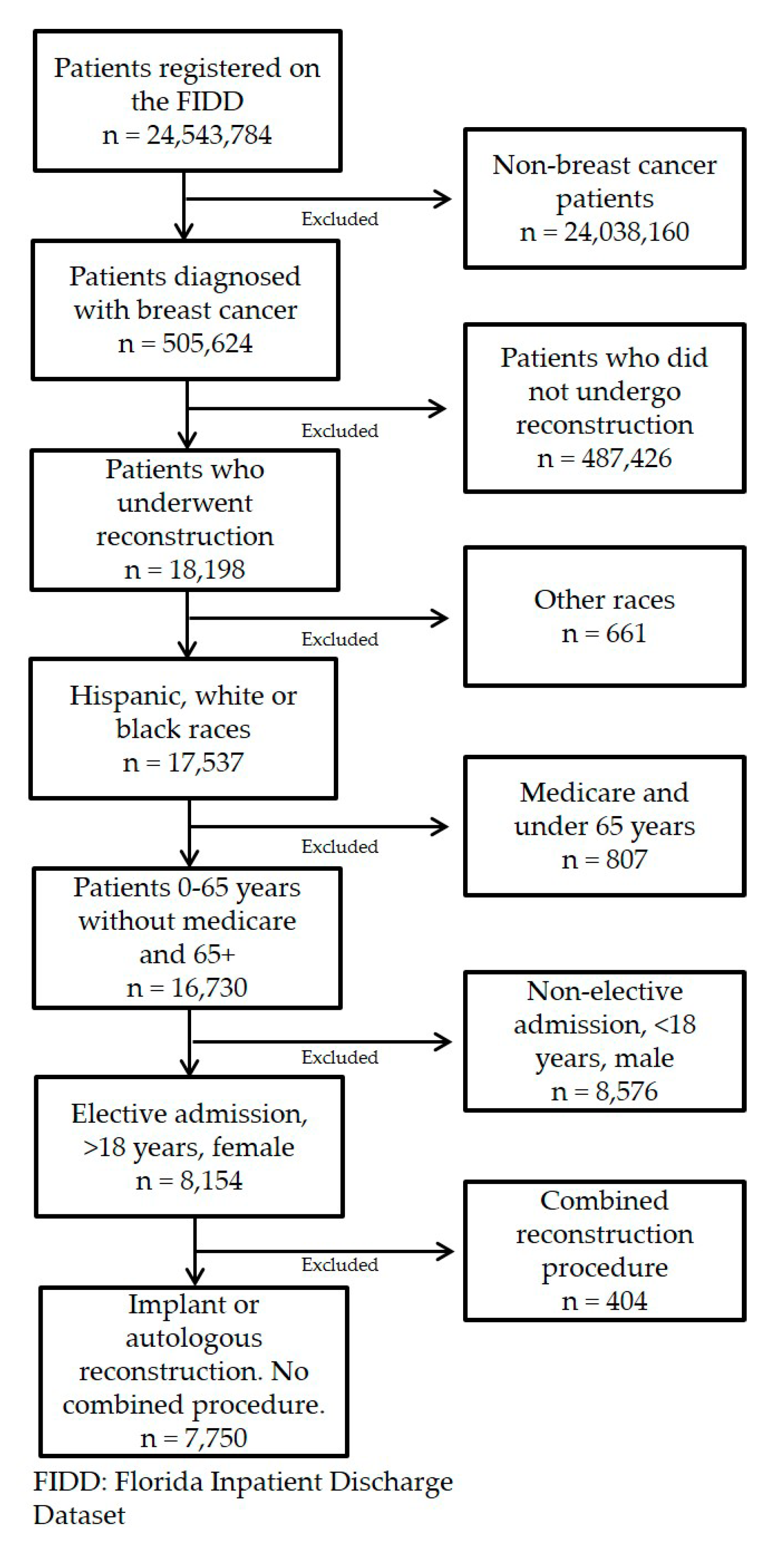
2.1. Data Source
2.2. Population and Variables
2.3. Dependent Variables
2.4. Independent Variables
2.5. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Sisti, A.; Huayllani, M.T.; Boczar, D.; Restrepo, D.J.; Spaulding, A.C.; Emmanuel, G.; Bagaria, S.P.; McLaughlin, S.A.; Parker, A.S.; Forte, A.J. Breast cancer in women: A descriptive analysis of the national cancer database. Acta Biomed. 2020, 91, 332–341. [Google Scholar] [PubMed]
- Fanakidou, I.; Zyga, S.; Alikari, V.; Tsironi, M.; Stathoulis, J.; Theofilou, P. Mental health, loneliness, and illness perception outcomes in quality of life among young breast cancer patients after mastectomy: The role of breast reconstruction. Qual. Life Res. 2018, 27, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Trejo-Ochoa, J.L.; Maffuz-Aziz, A.; Said-Lemus, F.M.; Dominguez-Reyes, C.A.; Hernandez-Hernandez, B.; Villegas-Carlos, F.; Rodriguez-Cuevas, S. Impact on quality of life with breast reconstructive surgery after mastectomy for breast cancer. [Article in Spanish]. Ginecol. Obstet. Mex. 2013, 81, 510–518. [Google Scholar]
- Panchal, H.; Matros, E. Current Trends in Postmastectomy Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 7S–13S. [Google Scholar] [CrossRef]
- Yang, R.L.; Newman, A.S.; Reinke, C.E.; Lin, I.C.; Karakousis, G.C.; Czerniecki, B.J.; Wu, L.C.; Kelz, R.R. Racial disparities in immediate breast reconstruction after mastectomy: Impact of state and federal health policy changes. Ann. Surg. Oncol. 2013, 20, 399–406. [Google Scholar] [CrossRef]
- Leuzzi, S.; Stivala, A.; Shaff, J.B.; Maroccia, A.; Rausky, J.; Revol, M.; Bertrand, B.; Cristofari, S. Latissimus dorsi breast reconstruction with or without implants: A comparison between outcome and patient satisfaction. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 381–393. [Google Scholar] [CrossRef]
- Fracon, S.; Renzi, N.; Manara, M.; Ramella, V.; Papa, G.; Arnez, Z.M. Patient Satisfaction After Breast Reconstruction: Implants vs. Autologous Tissues. Acta. Chir. Plast. 2018, 59, 120–128. [Google Scholar]
- DeSantis, C.; Ma, J.; Bryan, L.; Jemal, A. Breast cancer statistics, 2013. C.A. Cancer J. Clin. 2014, 64, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Alderman, A.K.; McMahon, L., Jr.; Wilkins, E.G. The national utilization of immediate and early delayed breast reconstruction and the effect of sociodemographic factors. Plast. Reconstr. Surg. 2003, 111, 695–703, discussion 704–705. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Tang, Y.; Wehby, G.L. Federal Health Coverage Mandates and Health Care Utilization: The Case of the Women’s Health and Cancer Rights Act and Use of Breast Reconstruction Surgery. J. Womens Health (Larchmt). 2015, 24, 655–662. [Google Scholar] [CrossRef]
- Cordeiro, P.G. Breast reconstruction after surgery for breast cancer. N. Engl. J. Med. 2008, 359, 1590–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkins, E.G.; Alderman, A.K. Breast reconstruction practices in north america: Current trends and future priorities. Semin. Plast. Surg. 2004, 18, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyomard, V.; Leinster, S.; Wilkinson, M. Systematic review of studies of patients’ satisfaction with breast reconstruction after mastectomy. Breast. 2007, 16, 547–567. [Google Scholar] [CrossRef]
- Ilonzo, N.; Tsang, A.; Tsantes, S.; Estabrook, A.; Thu Ma, A.M. Breast reconstruction after mastectomy: A ten-year analysis of trends and immediate postoperative outcomes. Breast. 2017, 32, 7–12. [Google Scholar] [CrossRef]
- Offodile, A.C., 2nd; Tsai, T.C.; Wenger, J.B.; Guo, L. Racial disparities in the type of postmastectomy reconstruction chosen. J. Surg. Res. 2015, 195, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Albornoz, C.R.; Bach, P.B.; Pusic, A.L.; McCarthy, C.M.; Mehrara, B.J.; Disa, J.J.; Cordeiro, P.G.; Matros, E. The influence of sociodemographic factors and hospital characteristics on the method of breast reconstruction, including microsurgery: A U.S. population-based study. Plast. Reconstr. Surg. 2012, 129, 1071–1079. [Google Scholar] [CrossRef]
- Sergesketter, A.R.; Thomas, S.M.; Lane, W.O.; Orr, J.P.; Shammas, R.L.; Fayanju, O.M.; Greenup, R.A.; Hollenbeck, S.T. Decline in Racial Disparities in Postmastectomy Breast Reconstruction: A Surveillance, Epidemiology, and End Results Analysis from 1998 to 2014. Plast. Reconstr. Surg. 2019, 143, 1560–1570. [Google Scholar] [CrossRef]
- Rodby, K.A.; Danielson, K.K.; Shay, E.; Robinson, E.; Benjamin, M.; Antony, A.K. Trends in Breast Reconstruction by Ethnicity: An Institutional Review Centered on the Treatment of an Urban Population. Am. Surg. 2016, 82, 497–504. [Google Scholar]
- Restrepo, D.J.; Boczar, D.; Huayllani, M.T.; Sisti, A.; Gabriel, E.; McLaughlin, S.A.; Bagaria, S.; Spaulding, A.C.; Rinker, B.D.; Forte, A.J. Influence of Race, Income, Insurance, and Education on the Rate of Breast Reconstruction. Anticancer Res. 2019, 39, 2969–2973. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, D.J.; Sisti, A.; Boczar, D.; Huayllani, M.T.; Fishe, J.; Gabriel, E.; McLaughlin, S.A.; Bagaria, S.; Spaulding, A.; Rinker, B.D.; et al. Characteristics of Breast Cancer Patients Who Refuse Surgery. Anticancer Res. 2019, 39, 4941–4945. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, D.J.; Boczar, D.; Huayllani, M.T.; Sisti, A.; McLaughlin, S.A.; Spaulding, A.; Parker, A.S.; Carter, R.E.; Leppin, A.L.; Forte, A.J. Survival Disparities in Male Patients With Breast Cancer. Anticancer Res. 2019, 39, 5669–5674. [Google Scholar] [CrossRef] [PubMed]
- Boczar, D.; Restrepo, D.J.; Sisti, A.; Huayllani, M.T.; Spaulding, A.C.; Gabriel, E.; Bagaria, S.; McLaughlin, S.; Parker, A.S.; Forte, A.J. Influence of Facility Characteristics on Access to Breast Reconstruction: A 12-Year National Cancer Database Analysis. Anticancer Res. 2019, 39, 6881–6885. [Google Scholar] [CrossRef]
- Ahn, S.H.; Park, B.W.; Noh, D.Y.; Nam, S.J.; Lee, E.S.; Lee, M.K.; Kim, S.H.; Lee, K.M.; Park, S.M.; Yun, Y.H. Health-related quality of life in disease-free survivors of breast cancer with the general population. Ann. Oncol. 2007, 18, 173–182. [Google Scholar] [CrossRef]
- Lagares-Borrego, A.; Gacto-Sanchez, P.; Infante-Cossio, P.; Barrera-Pulido, F.; Sicilia-Castro, D.; Gomez-Cia, T. A comparison of long-term cost and clinical outcomes between the two-stage sequence expander/prosthesis and autologous deep inferior epigastric flap methods for breast reconstruction in a public hospital. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 196–205. [Google Scholar] [CrossRef]
- Fischer, J.P.; Wes, A.M.; Nelson, J.A.; Basta, M.; Rohrbach, J.I.; Wu, L.C.; Serletti, J.M.; Kovach, S.J. Propensity-matched, longitudinal outcomes analysis of complications and cost: Comparing abdominal free flaps and implant-based breast reconstruction. J. Am. Coll. Surg. 2014, 219, 303–312. [Google Scholar] [CrossRef]
- Spear, S.L.; Newman, M.K.; Bedford, M.S.; Schwartz, K.A.; Cohen, M.; Schwartz, J.S. A retrospective analysis of outcomes using three common methods for immediate breast reconstruction. Plast. Reconstr. Surg. 2008, 122, 340–347. [Google Scholar] [CrossRef]
- Mioton, L.M.; Smetona, J.T.; Hanwright, P.J.; Seth, A.K.; Wang, E.; Bilimoria, K.Y.; Gaido, J.; Fine, N.A.; Kim, J.Y. Comparing thirty-day outcomes in prosthetic and autologous breast reconstruction: A multivariate analysis of 13.082 patients? J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 917–925. [Google Scholar] [CrossRef]
- Lista, F.; Ahmad, J. Evidence-based medicine: Augmentation mammaplasty. Plast. Reconstr. Surg. 2013, 132, 1684–1696. [Google Scholar] [CrossRef]
- Bank, J.; Phillips, N.A.; Park, J.E.; Song, D.H. Economic analysis and review of the literature on implant-based breast reconstruction with and without the use of the acellular dermal matrix. Aesthetic Plast. Surg. 2013, 37, 1194–1201. [Google Scholar] [CrossRef] [PubMed]
- Sando, I.C.; Momoh, A.O.; Chung, K.C.; Kozlow, J.H. The Early Years of Practice: An Assessment of Operative Efficiency and Cost of Free Flap and Implant Breast Reconstruction at an Academic Institution. J. Reconstr. Microsurg. 2016, 32, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Hanwright, P.J.; Davila, A.A.; Hirsch, E.M.; Khan, S.A.; Fine, N.A.; Bilimoria, K.Y.; Kim, J.Y. The differential effect of BMI on prosthetic versus autogenous breast reconstruction: A multivariate analysis of 12.986 patients. Breast. 2013, 22, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Dasari, C.R.; Gunther, S.; Wisner, D.H.; Cooke, D.T.; Gold, C.K.; Wong, M.S. Rise in microsurgical free-flap breast reconstruction in academic medical practices. Ann. Plast. Surg. 2015, 74, S62–S65. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Flap (n = 2809) | Implant (n = 4632) | Total (n = 7441) | p Value |
|---|---|---|---|---|
| Age | 54.0 (20.0–93.0) | 53.0 (21.0–87.0) | 53.0 (20.0–93.0) | <0.0001 1 |
| Year | <0.0001 2 | |||
| 2013 | 752 (26.8%) | 1319 (28.5%) | 2071 (27.8%) | |
| 2014 | 765 (27.2%) | 1147 (24.8%) | 1912 (25.7%) | |
| 2015 | 685 (24.4%) | 1004 (21.7%) | 1689 (22.7%) | |
| 2016 | 382 (13.6%) | 821 (17.7%) | 1203 (16.2%) | |
| 2017 | 225 (8.0%) | 341 (7.4%) | 566 (7.6%) | |
| Race | <0.0001 2 | |||
| White | 1798 (66.2%) | 3146 (70.2%) | 4944 (68.7%) | |
| Black or African American | 400 (14.7%) | 482 (10.8%) | 882 (12.3%) | |
| Hispanic or Latino | 517 (19.0%) | 851 (19.0%) | 1368 (19.0%) | |
| Patient Region | ||||
| South Florida | 1257 (46.1%) | 2465 (54.3%) | 3722 (51.2%) | <0.0001 2 |
| North Florida | 605 (22.2%) | 781 (17.2%) | 1386 (19.1%) | |
| Central Florida | 867 (31.8%) | 1294 (28.5%) | 2161 (29.7%) | |
| Patient Insurance Payer | <0.0001 2 | |||
| Medicare | 479 (17.1%) | 839 (18.1%) | 1318 (17.7%) | |
| Medicaid | 238 (8.5%) | 267 (5.8%) | 505 (6.8%) | |
| Commercial | 1916 (68.2%) | 3341 (72.1%) | 5257 (70.6%) | |
| Other | 176 (6.3%) | 185 (4.0%) | 361 (4.9%) | |
| Elixhauser Score | <0.0001 2 | |||
| No | 1445 (51.4%) | 2740 (59.2%) | 4185 (56.2%) | |
| Yes | 1364 (48.6%) | 1892 (40.8%) | 3256 (43.8%) |
| Implant vs. Flap (Ref) | ||
|---|---|---|
| Variable | OR (95%CI) | p Value |
| Age (10-year increase) | 0.79 (0.75, 0.84) | <0.0001 |
| Race | Overall Test of Difference: p < 0.0001 | |
| White | 1.00 (Ref) | N/A |
| Black or African American | 0.67 (0.57, 0.78) | <0.0001 |
| Hispanic or Latino | 0.81 (0.71, 0.92) | |
| Patient Region | Overall Test of Difference: p < 0.0001 | |
| North Florida | 1.00 (Ref) | N/A |
| South Florida | 1.61 (1.40, 1.83) | <0.0001 |
| Central Florida | 1.17 (1.02, 1.35) | |
| Patient Insurance Payer | Overall Test of Difference: p < 0.0001 | |
| Commercial | 1.00 (Ref) | N/A |
| Medicare | 1.59 (1.34, 1.89) | <0.0001 |
| Medicaid | 0.62 (0.51, 0.75) | <0.0001 |
| Other | 0.64 (0.51, 0.80) | |
| Elixhauser Score | ||
| No | 1.00 (Ref) | N/A |
| Yes | 0.75 (0.68, 0.82) | <0.0001 |
| Implant vs. Free Flap (Ref) | Implant vs. Pedicled Flap (Ref) | |||
|---|---|---|---|---|
| Variable | OR (95%CI) | p Value | OR (95%CI) | p Value |
| Age | 0.81 (0.75, 0.88) | <0.0001 | 0.63 (0.54, 0.72) | <0.0001 |
| Race | Overall Test of Difference: p < 0.0001 | Overall Test of Difference: p = 0.009 | ||
| White | 1.00 (Ref) | N/A | 1.00 (Ref) | N/A |
| Black or African American | 0.61 (0.51, 0.74) | <0.0001 | 0.61 (0.44, 0.84) | 0.003 |
| Hispanic or Latino | 0.64 (0.55, 0.76) | <0.0001 | 0.97 (0.72, 1.31) | 0.85 |
| Patient Region | Overall Test of Difference: p < 0.0001 | Overall Test of Difference: p < 0.0001 | ||
| North Florida | 1.00 (Ref) | N/A | 1.00 (Ref) | N/A |
| South Florida | 2.09 (1.78, 2.45) | <0.0001 | 0.82 (0.58, 1.17) | 0.27 |
| Central Florida | 2.11 (1.77, 2.52) | <0.0001 | 0.46 (0.32, 0.65) | <0.0001 |
| Patient Insurance Payer | Overall Test of Difference: p < 0.0001 | Overall Test of Difference: p < 0.0001 | ||
| Commercial | 1.00 (Ref) | N/A | 1.00 (Ref) | N/A |
| Medicare | 2.71 (2.13, 3.44) | <0.0001 | 1.48 (1.03, 2.12) | 0.035 |
| Medicaid | 0.93 (0.72, 1.21) | 0.58 | 0.36 (0.25, 0.52) | <0.0001 |
| Other | 0.66 (0.51, 0.87) | 0.003 | 0.66 (0.39, 1.10) | 0.11 |
| Elixhauser Score | Overall Test of Difference: p < 0.0001 | Overall Test of Difference: p = 0.0004 | ||
| No | 1.00 (Ref) | N/A | 1.00 (Ref) | N/A |
| Yes | 0.60 (0.53, 0.68) | <0.0001 | 1.75 (1.38, 2.22) | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restrepo, D.J.; Huayllani, M.T.; Boczar, D.; Sisti, A.; Nguyen, M.-D.T.; Cochuyt, J.J.; Spaulding, A.C.; Rinker, B.D.; Perdikis, G.; Forte, A.J. Disparities in Access to Autologous Breast Reconstruction. Medicina 2020, 56, 281. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060281
Restrepo DJ, Huayllani MT, Boczar D, Sisti A, Nguyen M-DT, Cochuyt JJ, Spaulding AC, Rinker BD, Perdikis G, Forte AJ. Disparities in Access to Autologous Breast Reconstruction. Medicina. 2020; 56(6):281. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060281
Chicago/Turabian StyleRestrepo, David J., Maria T. Huayllani, Daniel Boczar, Andrea Sisti, Minh-Doan T. Nguyen, Jordan J. Cochuyt, Aaron C. Spaulding, Brian D. Rinker, Galen Perdikis, and Antonio J. Forte. 2020. "Disparities in Access to Autologous Breast Reconstruction" Medicina 56, no. 6: 281. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060281