Prediction of the Ideal Implant Size Using 3-Dimensional Healthy Breast Volume in Unilateral Direct-to-Implant Breast Reconstruction



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
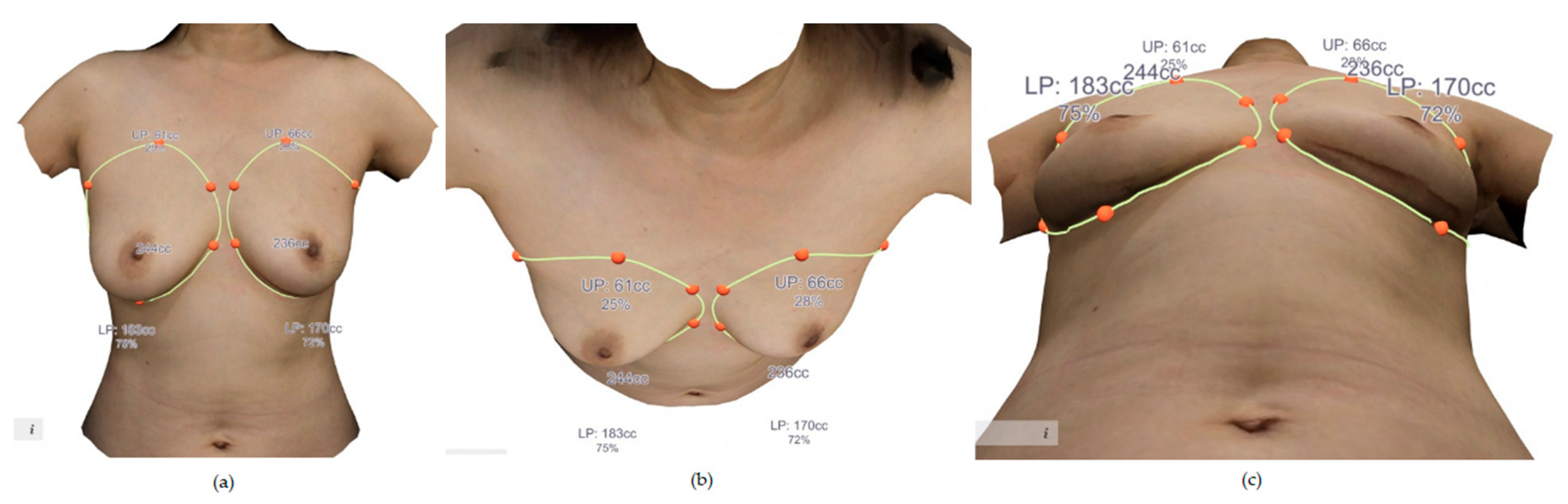
2.2. Method for 3-Dimensional Surface Imaging and Volume Extraction
2.3. Reconstruction after Nipple-Sparing Mastectomy
2.4. Calculation of Ideal Implant Size
2.5. Statistical Analysis
3. Results
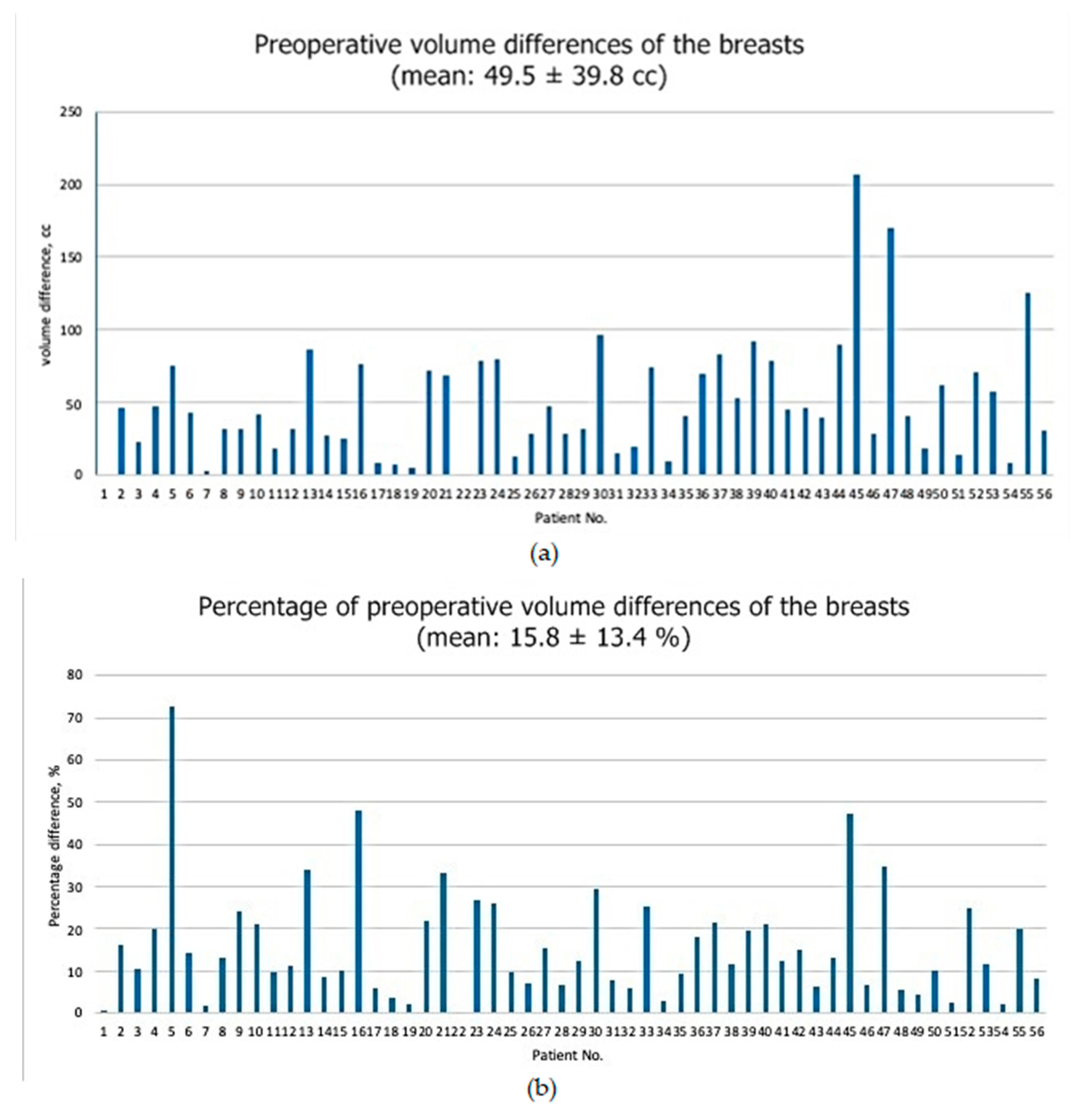
3.1. Patient Demographics and Operative Data
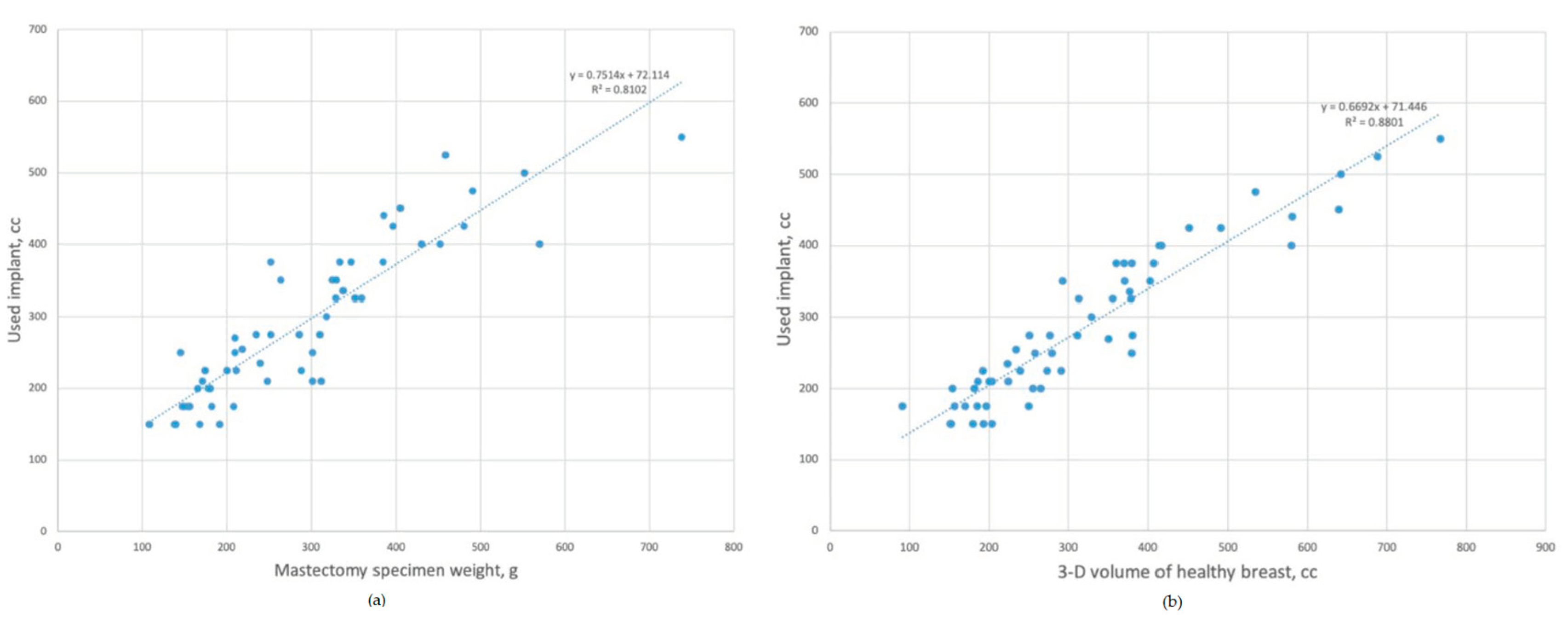
3.2. Prediction Model for the Inserted Implant Volume
- Inserted implant volume = 0.75 × mastectomy specimen weight (g) + 72 cc (R2 = 81.0%, p < 0.001).
- 2.
- Inserted implant volume = 0.66 × healthy breast volume + 71 cc (R2 = 88.0%, p < 0.001).
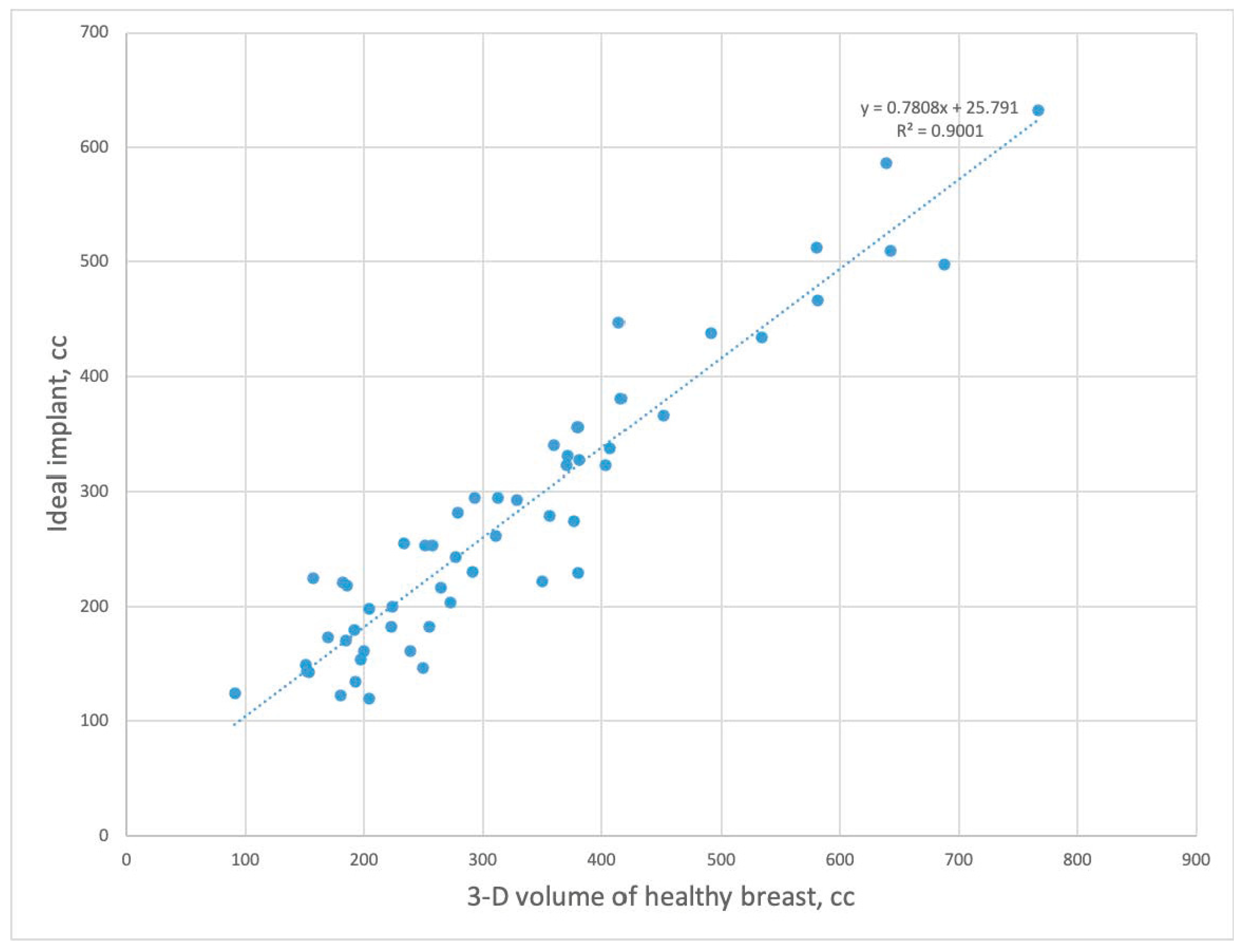
3.3. Prediction Model for Ideal Implant Volume
- Mastectomy specimen weight as a predictor variable.
- 2.
- Healthy breast volume as a predictor variable.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Azouz, V.; Lopez, S.; Wagner, D.S. Surgeon-Controlled Comparison of Direct-to-Implant and 2-Stage Tissue Expander-Implant Immediate Breast Reconstruction Outcomes. Ann. Plast. Surg. 2018, 80, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Kamali, P.; Koolen, P.G.L.; Ibrahim, A.M.S.; Paul, M.; Dikmans, R.E.; Schermerhorn, M.L.; Lee, B.T.; Lin, S.J. Analyzing Regional Differences over a 15-Year Trend of One-Stage versus Two-Stage Breast Reconstruction in 941,191 Postmastectomy Patients. Plast. Reconstr. Surg. 2016, 138, 1e–14e. [Google Scholar] [CrossRef] [PubMed]
- Serrurier, L.C.J.; Rayne, S.; Venter, M.; Benn, C.-A. Direct-to-Implant Breast Reconstruction without the Use of an Acellular Dermal Matrix Is Cost Effective and Oncologically Safe. Plast. Reconstr. Surg. 2017, 139, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.B.; Small, K.H.; Choi, M.; Karp, N.S. Three-Dimensional surface imaging in plastic surgery: Foundation, practical applications, and beyond. Plast. Reconstr. Surg. 2015, 135, 1295–1304. [Google Scholar] [CrossRef] [Green Version]
- Galdino, G.M.; Nahabedian, M.; Chiaramonte, M.; Geng, J.Z.; Klatsky, S.; Manson, P. Clinical Applications of Three-Dimensional Photography in Breast Surgery. Plast. Reconstr. Surg. 2002, 110, 58–70. [Google Scholar] [CrossRef]
- Tzou, C.H.; Artner, N.M.; Pona, I.; Hold, A.; Placheta, E.; Kropatsch, W.G.; Frey, M. Comparison of three-dimensional surface-imaging systems. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 489–497. [Google Scholar] [CrossRef]
- Yip, J.M.; Mouratova, N.; Jeffery, R.M.; Veitch, D.E.; Woodman, R.J.; Dean, N.R. Accurate assessment of breast volume: A study comparing the volumetric gold standard (direct water displacement measurement of mastectomy specimen) with a 3D laser scanning technique. Ann. Plast. Surg. 2012, 68, 135–141. [Google Scholar] [CrossRef]
- Georgii, J.; Eder, M.; Bürger, K.; Klotz, S.; Ferstl, F.; Kovács, L.; Westermann, R. A Computational Tool for Preoperative Breast Augmentation Planning in Aesthetic Plastic Surgery. IEEE J. Biomed. Health Inform. 2014, 18, 907–919. [Google Scholar] [CrossRef]
- Henseler, H.; Hille-Betz, U.; Vogt, P. Validation of Subjective Estimates of Female Breast Volume and Comparison with Objective Methods. Handchir. Mikrochir. Plast. Chir. 2015, 47, 371–377. [Google Scholar] [CrossRef]
- Baek, W.Y.; Byun, I.H.; Kim, Y.S.; Lew, D.H.; Jeong, J.; Roh, T.S. Patient Satisfaction with Implant Based Breast Reconstruction Associated with Implant Volume and Mastectomy Specimen Weight Ratio. J. Breast Cancer 2017, 20, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Georgiou, C.; Ihrai, T.; Chamorey, E.; Flipo, B.; Chignon-Sicard, B. A formula for implant volume choice in breast reconstruction after nipple sparing mastectomy. Breast 2012, 21, 781–782. [Google Scholar] [CrossRef]
- Shia, W.; Yang, H.-J.; Wu, H.-K.; Lin, S.-L.; Lai, H.-W.; Huang, Y.-L.; Chen, D.-R. Implant volume estimation in direct-to-implant breast reconstruction after nipple-sparing mastectomy. J. Surg. Res. 2018, 231, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wazir, U.; Chehade, H.E.H.; Choy, C.; Kasem, A.; Mokbel, K. A Study of the Relation Between Mastectomy Specimen Weight and Volume with Implant Size in Oncoplastic Reconstruction. Vivo 2019, 33, 125–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parmar, C.; West, M.; Pathak, S.; Nelson, J.; Martin, L. Weight versus volume in breast surgery: An observational study. JRSM Short Rep. 2011, 2, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Luan, J.; Mu, L.; Ji, K. The Role of Three-Dimensional Scanning Technique in Evaluation of Breast Asymmetry in Breast Augmentation: A 100-Case Study. Plast. Reconstr. Surg. 2010, 126, 2125–2132. [Google Scholar] [CrossRef]
- Chae, M.P.; Hunter-Smith, D.J.; Spychal, R.T.; Rozen, W.M. 3D volumetric analysis for planning breast reconstructive surgery. Breast Cancer Res. Treat. 2014, 146, 457–460. [Google Scholar] [CrossRef]
- Erić, M.; Anderla, A.; Stefanović, D.; Drapšin, M. Breast volume estimation from systematic series of CT scans using the Cavalieri principle and 3D reconstruction. Int. J. Surg. 2014, 12, 912–917. [Google Scholar] [CrossRef] [Green Version]
- Fujii, T.; Yamaguchi, S.; Yajima, R.; Tsutsumi, S.; Asao, T.; Kuwano, H. Accurate Assessment of Breast Volume by Computed Tomography Using Three-dimensional Imaging Device. Am. Surg. 2012, 78, 933–935. [Google Scholar] [CrossRef]
- Kim, H.; Mun, G.-H.; Wiraatmadja, E.S.; Lim, S.-Y.; Pyon, J.-K.; Oh, K.S.; Lee, J.E.; Nam, S.J.; Lim, S.Y. Preoperative Magnetic Resonance Imaging-Based Breast Volumetry for Immediate Breast Reconstruction. Aesthet. Plast. Surg. 2015, 39, 369–376. [Google Scholar] [CrossRef]
- Yoo, A.; Minn, K.W.; Jin, U.S. Magnetic Resonance Imaging-Based Volumetric Analysis and Its Relationship to Actual Breast Weight. Arch. Plast. Surg. 2013, 40, 203–208. [Google Scholar] [CrossRef] [Green Version]
- Creasman, C.N.; Mordaunt, D.; Liolios, T.; Chiu, C.; Gabriel, A.; Maxwell, G.P. Four-Dimensional Breast Imaging, Part II: Clinical Implementation and Validation of a Computer Imaging System for Breast Augmentation Planning. Aesthet. Surg. J. 2011, 31, 925–938. [Google Scholar] [CrossRef] [PubMed]
- Donfrancesco, A.; Montemurro, P.; Hedén, P. Three-Dimensional simulated images in breast augmentation surgery: An investigation of patients’ satisfaction and the correlation between prediction and actual outcome. Plast. Reconstr. Surg. 2013, 132, 810–822. [Google Scholar] [CrossRef] [PubMed]
- Gladilin, E.; Gabrielova, B.; Montemurro, P.; Hedén, P. Customized Planning of Augmentation Mammaplasty with Silicon Implants Using Three-Dimensional Optical Body Scans and Biomechanical Modeling of Soft Tissue Outcome. Aesthet. Plast. Surg. 2010, 35, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Vorstenbosch, J.; Islur, A. Correlation of Prediction and Actual Outcome of Three-Dimensional Simulation in Breast Augmentation Using a Cloud-Based Program. Aesthet. Plast. Surg. 2017, 133, 481–490. [Google Scholar] [CrossRef]
- Roostaeian, J.; Adams, W.P., Jr. Three-Dimensional Imaging for Breast Augmentation: Is This Technology Providing Accurate Simulations? Aesthet. Surg. J. 2014, 34, 857–875. [Google Scholar] [CrossRef] [Green Version]
- Pöhlmann, S.T.L.; Harkness, E.; Taylor, C.J.; Gandhi, A.; Astley, S.M. Preoperative implant selection for unilateral breast reconstruction using 3D imaging with the Microsoft Kinect sensor. J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 1059–1067. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of patients | 56 |
| Age, mean ± SD, yr | 47.95 ± 8.44 |
| BMI, mean ± SD, kg/m2 | 22.77 ± 2.50 |
| Cancer laterality | |
| No. of right (%) No. of left (%) | 35 (62.5) 21 (37.5) |
| Mastectomy type | |
| No. of nipple-sparing (%) No. of skin-sparing (%) | 48 (85.7) 8 (14.3) |
| Mastectomy specimen weight, mean ± SD, g | 287.6 ± 128.2 |
| Inserted implant volume, mean ± SD, cc | 287.5 ± 107.0 |
| Inserted ADM size, mean ± SD, cm2 | 204.0 ± 82.9 |
| Preoperative volume of the breasts | |
| Pre-operative volume of affected breast, mean ± SD, cc Pre-operative volume of contralateral unaffected breast, mean ± SD, cc | 317.6 ± 154.3 322.9 ± 150.0 |
| Postoperative volume of the breasts | |
| Post-operative volume of affected breast, mean ± SD, cc Post-operative volume of contralateral unaffected breast, mean ± SD, cc | 336.8 ± 147.8 321.2 ± 161.1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Park, J.-W.; Woo, K.-J. Prediction of the Ideal Implant Size Using 3-Dimensional Healthy Breast Volume in Unilateral Direct-to-Implant Breast Reconstruction. Medicina 2020, 56, 498. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100498
Kim J-H, Park J-W, Woo K-J. Prediction of the Ideal Implant Size Using 3-Dimensional Healthy Breast Volume in Unilateral Direct-to-Implant Breast Reconstruction. Medicina. 2020; 56(10):498. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100498
Chicago/Turabian StyleKim, Jeong-Hoon, Jin-Woo Park, and Kyong-Je Woo. 2020. "Prediction of the Ideal Implant Size Using 3-Dimensional Healthy Breast Volume in Unilateral Direct-to-Implant Breast Reconstruction" Medicina 56, no. 10: 498. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100498