Histological Aspects and Quantitative Assessment of Ki67 as Prognostic Factors in Breast Cancer Patients: Result from a Single-Center, Cross Sectional Study


Abstract
:1. Introduction
1.1. Ki67
1.1.1. Structure and Function of Ki67
1.1.2. Detection of Ki67
1.1.3. Ki67 Cut-Off
1.2. Histological Type and Grade
2. Materials and Methods
2.1. Ki67 Assessed
2.2. Statistical Analysis
3. Results
3.1. OS Analysis
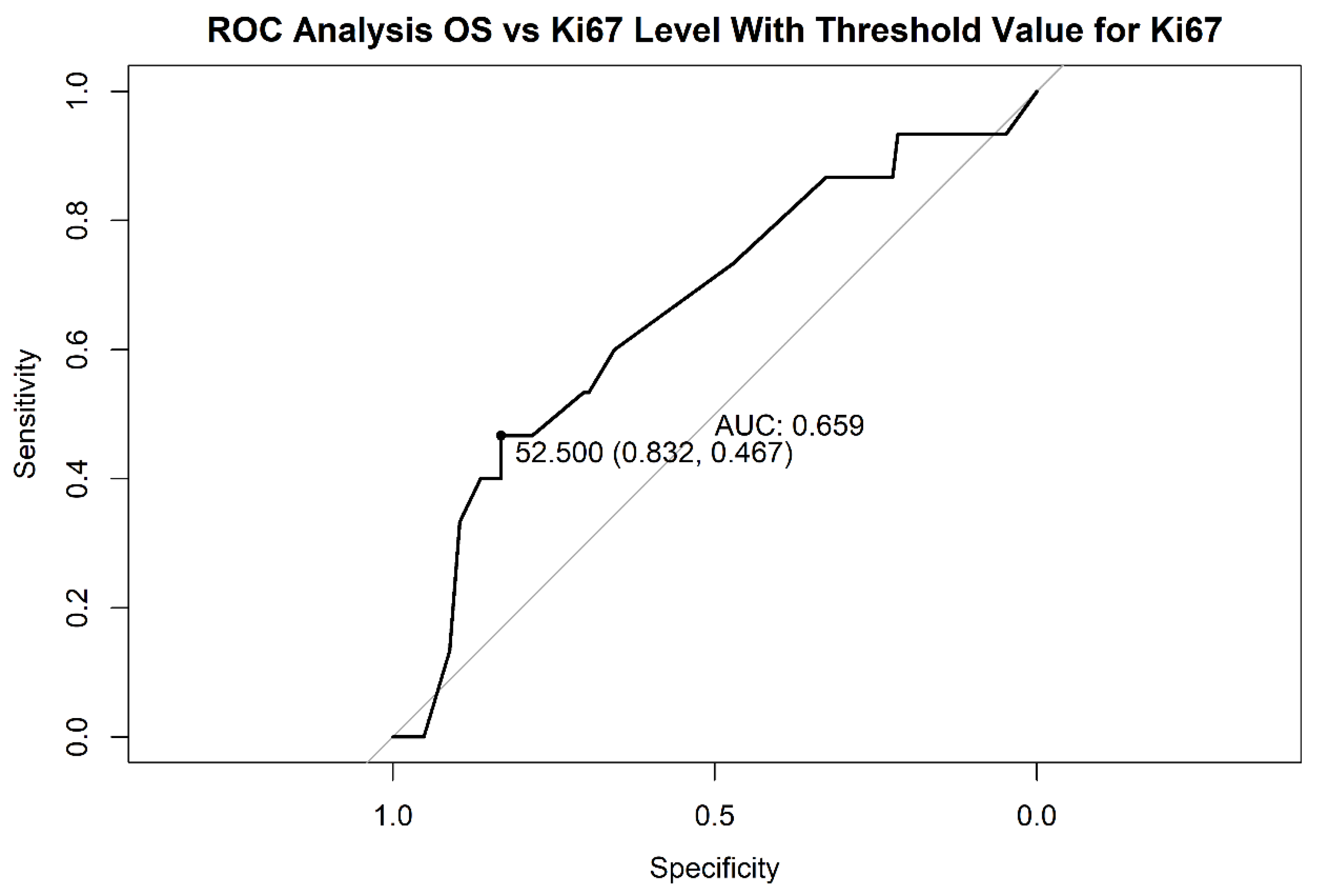
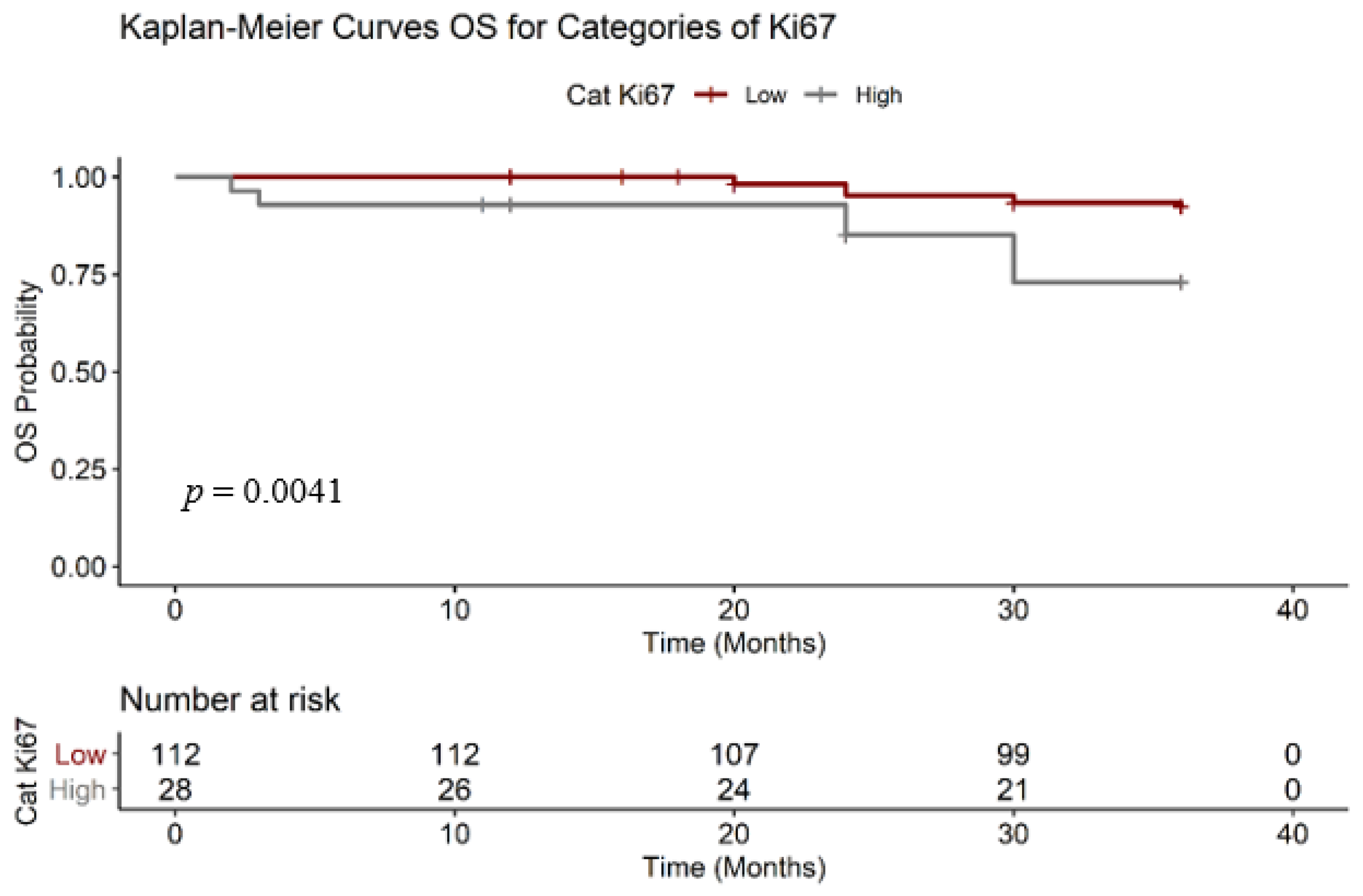
3.1.1. Ki67 Analysis
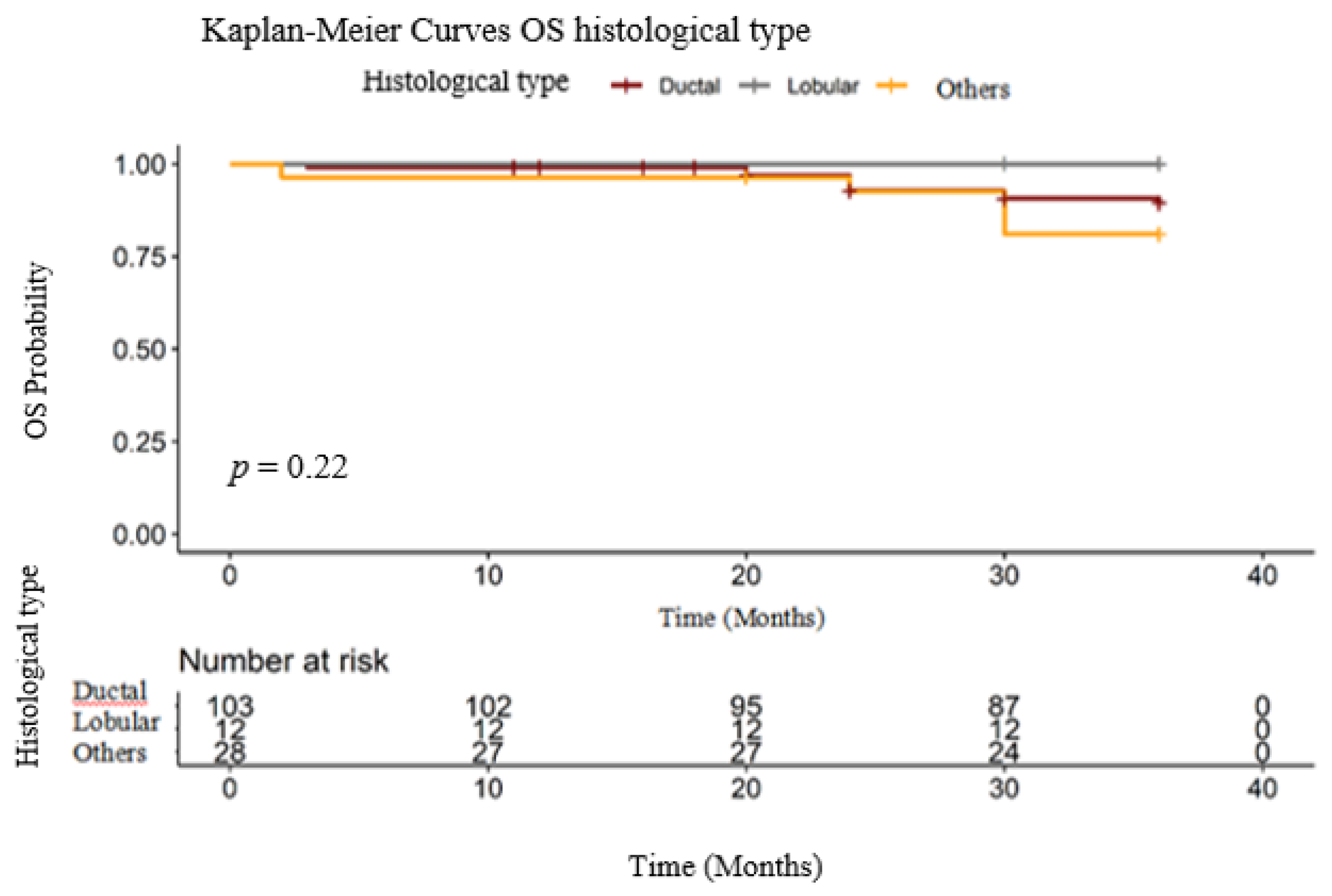
3.1.2. Histological Type
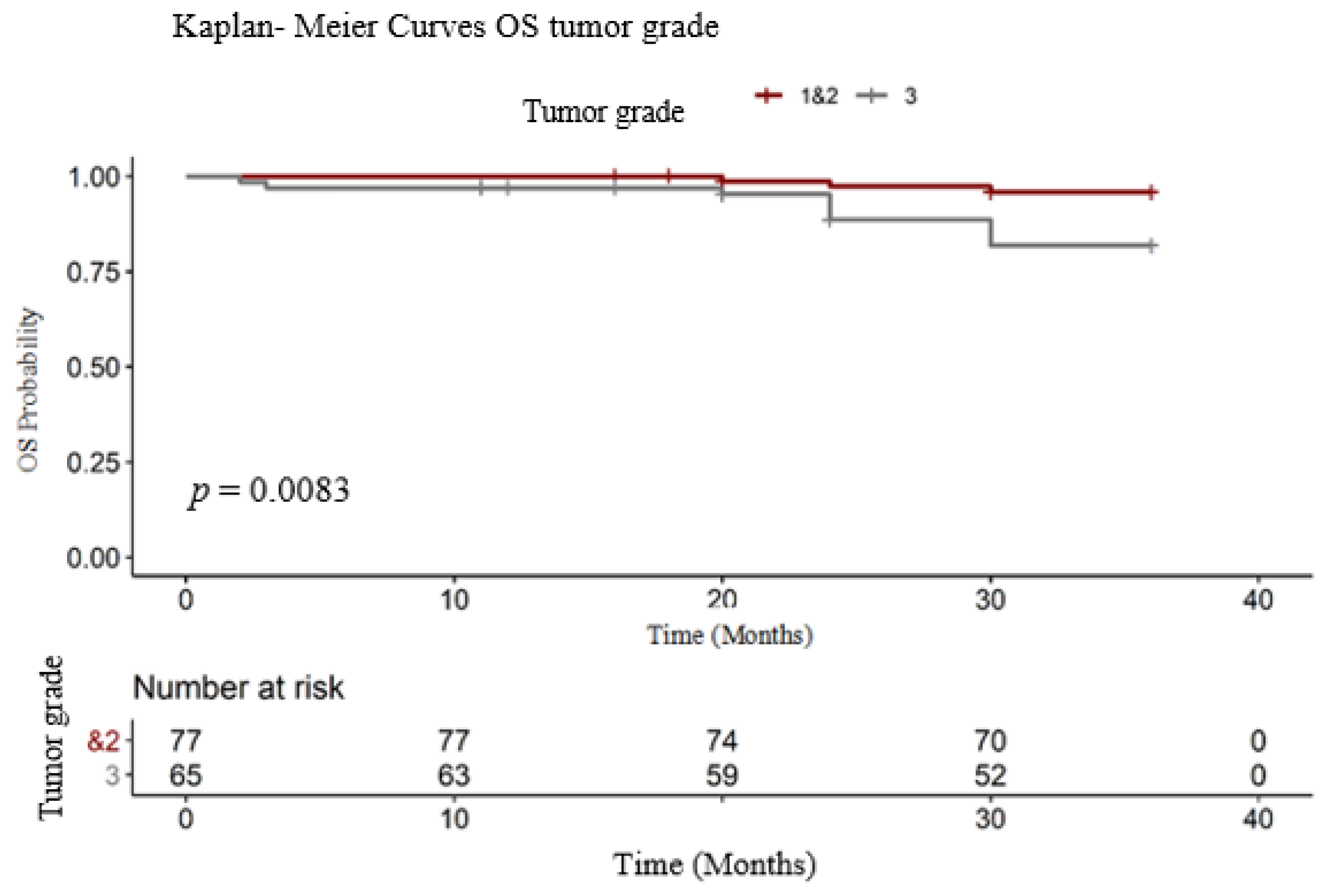
3.1.3. Tumor Grade
3.2. PFS Analysis
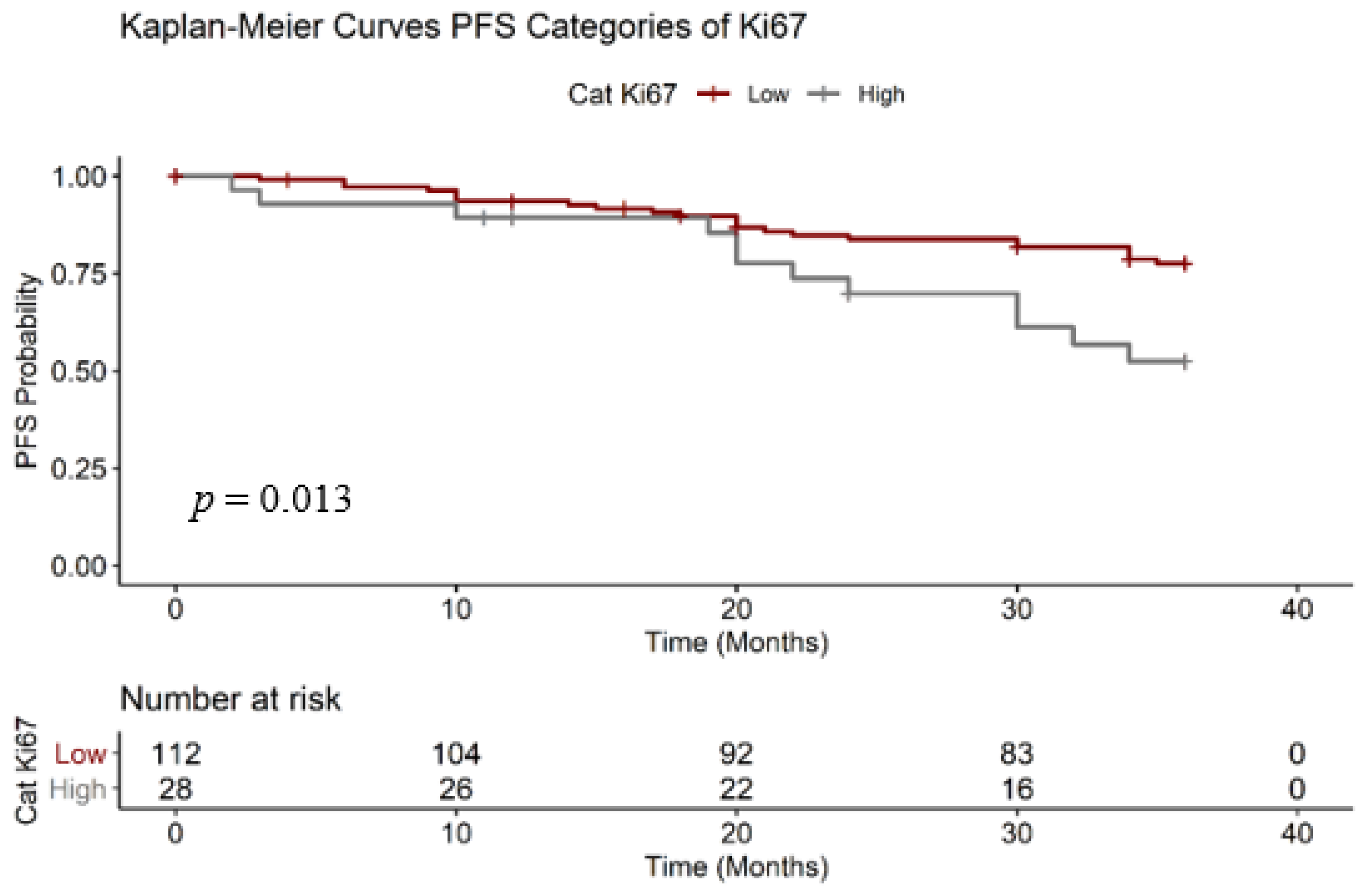
3.2.1. Ki67 Analysis
3.2.2. Histological Type
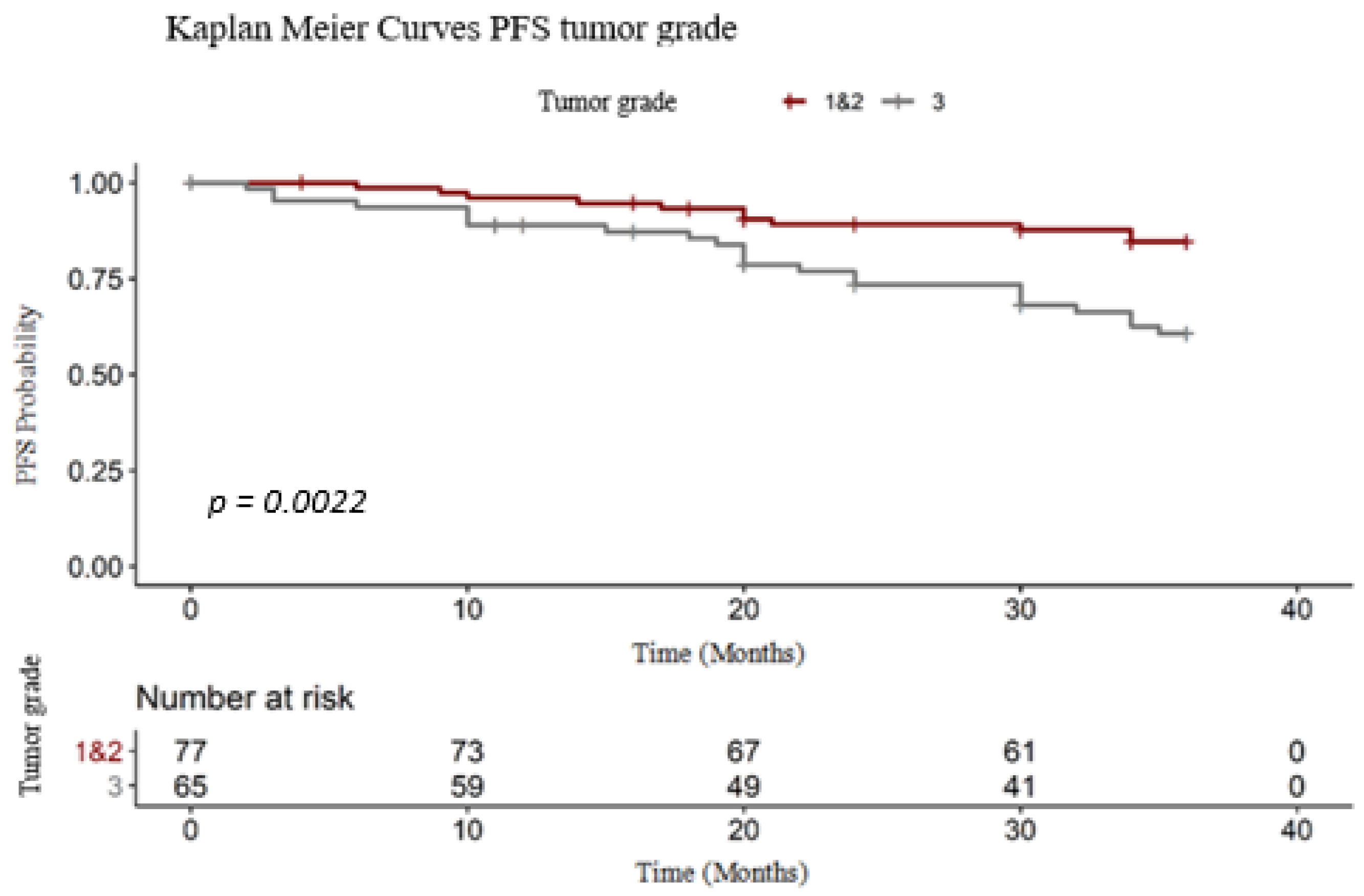
3.2.3. Tumor Grade
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Omata, F.; McNamara, K.M.; Suzuki, K.; Abe, E.; Hirakawa, H.; Ishida, T.; Ohuchi, N.; Sasano, H. Effect of the normal mammary differentiation regulator ELF5 upon clinical outcomes of triple negative breast cancers patients. Breast Cancer 2018, 25, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.J.; Suman, V.J.; Hoog, J.; Goncalves, R.; Sanati, S.; Creighton, C.J.; DeSchryver, K.; Crouch, E.; Brink, A.; Watson, M.; et al. Ki67 Proliferation Index as a Tool for Chemotherapy Decisions During and After Neoadjuvant Aromatase Inhibitor Treatment of Breast Cancer: Results From the American College of Surgeons Oncology Group Z1031 Trial (Alliance). J. Clin. Oncol. 2017, 35, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Penault-Llorca, F.; Radosevic-Robin, N. Ki67 assessment in breast cancer: An update. Pathology 2017, 49, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Jecan, C. Clinical data related to breast reconstruction; looking back on the 21th century and forward to the next steps. J. Mind Med. Sci. 2015, 2, 34–42. [Google Scholar]
- Avino, A.; Răducu, L. Timing between Breast Reconstruction and Oncologic Mastectomy-One Center Experience. Medicina 2020, 56, 86. [Google Scholar] [CrossRef] [Green Version]
- Mandita, A.; Balcangiu-Stroescu, A.-E.; Tanasescu, M.D.; Diaconescu, A.; Dragos, D.; Cosconel, C.I.; Timofte, D.; Balan, D.; Raducu, L.; Stoicescu, S.M.; et al. Hyperuricemia and Cardiovascular Diseases Clinical and paraclinical correlations. Revista de Chimie 2019, 70. [Google Scholar] [CrossRef]
- Tanasescu, M.; Diaconescu, A.; Răducu, L.; Constantin, A.; Daniela Gabriela, B.; Tarmure, V.; Ionescu, D. Cardiovascular Comorbidities, Inflammation and Serum Albumin Levels in a Group of Hemodialysis Patients. Revista de Chimie 2018. [Google Scholar] [CrossRef]
- Totan, A.; Andra-Elena, B.-S.; Imre, M.; Miricescu, D.; Balan, D.G.; Stanescu, I.-I.; Ionescu, D.; Timofte, D.; Tanasescu, M.D.; Greabu, M. XOR—Possible Correlations with Oxidative Stress and Inflammation Markers in the Context of Diabetic Kidney Disease. Revista de Chimie 2019, 70, 1396–1398. [Google Scholar] [CrossRef]
- Tanasescu, M.; Diaconescu, A.; Răducu, L.; Balan, D.G.; Mihai, A.; Tanase, M.; Stanescu, I.I.; Ionescu, D. Diabetic Nephropathy: A Concise Assessment of the Causes, Risk Factors and Implications in Diabetic Patients. Revista de Chimie 2018. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 365, 1687–1717. [Google Scholar] [CrossRef]
- Vuong, D.; Simpson, P.T.; Green, B.; Cummings, M.C.; Lakhani, S.R. Molecular classification of breast cancer. Virchows Arch. Int. J. Pathol. 2014, 465, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kennecke, H.; Yerushalmi, R.; Woods, R.; Cheang, M.C.; Voduc, D.; Speers, C.H.; Nielsen, T.O.; Gelmon, K. Metastatic behavior of breast cancer subtypes. J. Clin. Oncol. 2010, 28, 3271–3277. [Google Scholar] [CrossRef] [PubMed]
- Lopez, F.; Belloc, F.; Lacombe, F.; Dumain, P.; Reiffers, J.; Bernard, P.; Boisseau, M.R. Modalities of synthesis of Ki67 antigen during the stimulation of lymphocytes. Cytometry 1991, 12, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Wang, S.; Wang, Y. Expressions of Topo IIα and Ki67 in breast cancer and its clinicopathologic features and prognosis. Pak. J. Med. Sci. 2019, 35, 715–720. [Google Scholar] [CrossRef] [Green Version]
- Guth, A.A.; Chun-Kim, J.; Schwartz, S.; Montes, J.; Snyder, R.A.; Axelrod, D.; Schnabel, F.R. The Relationship of Race, Oncotype DX, and Ki67 in a Population Highly Screened for Breast Cancer. Breast J. 2017, 23, 177–181. [Google Scholar] [CrossRef]
- Alsadoun, N.; MacGrogan, G.; Truntzer, C.; Lacroix-Triki, M.; Bedgedjian, I.; Koeb, M.H.; El Alam, E.; Medioni, D.; Parent, M.; Wuithier, P.; et al. Solid papillary carcinoma with reverse polarity of the breast harbors specific morphologic, immunohistochemical and molecular profile in comparison with other benign or malignant papillary lesions of the breast: A comparative study of 9 additional cases. Mod. Pathol. Off. J. U. S. Can. Acad. Pathol. 2018, 31, 1367–1380. [Google Scholar] [CrossRef] [Green Version]
- Ross, J.S.; Linette, G.P.; Stec, J.; Clark, E.; Ayers, M.; Leschly, N.; Symmans, W.F.; Hortobagyi, G.N.; Pusztai, L. Breast cancer biomarkers and molecular medicine. Expert Rev. Mol. Diagn. 2003, 3, 573–585. [Google Scholar] [CrossRef]
- Van Diest, P.J.; van der Wall, E.; Baak, J.P. Prognostic value of proliferation in invasive breast cancer: A review. J. Clin. Pathol. 2004, 57, 675–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, C.; Seibt, S.; Al Kuraya, K.; Siraj, A.K.; Mirlacher, M.; Schraml, P.; Maurer, R.; Spichtin, H.; Torhorst, J.; Popovska, S.; et al. Tissue microarrays for comparing molecular features with proliferation activity in breast cancer. Int. J. Cancer 2006, 118, 2190–2194. [Google Scholar] [CrossRef] [PubMed]
- Stalhammar, G.; Robertson, S.; Wedlund, L.; Lippert, M.; Rantalainen, M.; Bergh, J.; Hartman, J. Digital image analysis of Ki67 in hot spots is superior to both manual Ki67 and mitotic counts in breast cancer. Histopathology 2018, 72, 974–989. [Google Scholar] [CrossRef]
- Mook, S.; Schmidt, M.K.; Rutgers, E.J.; van de Velde, A.O.; Visser, O.; Rutgers, S.M.; Armstrong, N.; Veer, L.J.V.; Ravdin, P.M. Calibration and discriminatory accuracy of prognosis calculation for breast cancer with the online Adjuvant program: A hospital-based retrospective cohort study. Lancet Oncol. 2009, 10, 1070–1076. [Google Scholar] [CrossRef]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Weigelt, B.; Geyer, F.C.; Reis-Filho, J.S. Histological types of breast cancer: How special are they? Mol. Oncol. 2010, 4, 192–208. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Senkus, E.; Costa, A.; Papadopoulos, E.; Aapro, M.; André, F.; Harbeck, N.; Aguilar Lopez, B.; Barrios, C.H.; Bergh, J.; et al. 4th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4) †. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 1634–1657. [Google Scholar] [CrossRef]
- Urruticoechea, A.; Smith, I.E.; Dowsett, M. Proliferation marker Ki-67 in early breast cancer. J. Clin. Oncol. 2005, 23, 7212.e20. [Google Scholar] [CrossRef]
- Carbognin, L.; Sperduti, I.; Brunelli, M.; Marcolini, L.; Nortilli, R.; Pilotto, S.; Zampiva, I.; Merler, S.; Fiorio, E.; Filippi, E.; et al. Subpopulation Treatment Effect Pattern Plot (STEPP) analysis of Ki67 assay according to histology: Prognostic relevance for resected early stage ‘pure’ and ‘mixed’ lobular breast cancer. J. Exp. Clin. Cancer Res. 2016, 35, 50. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up †. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [Green Version]
- Gnant, M.; Harbeck, N.; Thomssen, C. St. Gallen/Vienna 2017: A Brief Summary of the Consensus Discussion about Escalation and De-Escalation of Primary Breast Cancer Treatment. Breast Care (Basel, Switzerland) 2017, 12, 102–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.J.; Swain, S.M.; Luminal, A. Breast Cancer and Molecular Assays: A Review. Oncologist 2018, 23, 556–565. [Google Scholar] [CrossRef] [Green Version]
- Christgen, M.; Steinemann, D.; Kühnle, E.; Länger, F.; Gluz, O.; Harbeck, N.; Kreipe, H. Lobular breast cancer: Clinical, molecular and morphological characteristics. Pathol. Res. Pract. 2016, 212, 583–597. [Google Scholar] [CrossRef] [PubMed]
- Tampa, M.; Mitran, C.I.; Mitran, M.I.; Nicolae, I.; Dumitru, A.; Matei, C.; Manolescu, L.; Popa, G.L.; Caruntu, C.; Georgescu, S.R. The Role of Beta HPV Types and HPV-Associated Inflammatory Processes in Cutaneous Squamous Cell Carcinoma. J. Immunol. Res. 2020, 5701639. [Google Scholar] [CrossRef]
- Pak, K.; Uno, H.; Kim, D.H.; Tian, L.; Kane, R.C.; Takeuchi, M.; Fu, H.; Claggett, B.; Wei, L.J. Interpretability of Cancer clinical trials results using restricted mean survival time as an alternative to the Hazard ratio. JAMA Oncol. 2017, 3, 1692–1696. [Google Scholar] [CrossRef]
- Manolescu, L.S.C.; Boeru, C.; Căruntu, C.; Dragomirescu, C.C.; Goldis, M.; Jugulete, G.; Marin, M.; Popa, G.L.; Preda, M.; Radu, M.C.; et al. A Romanian experience of syphilis in pregnancy and childbirth. Midwifery 2019, 78, 58–63. [Google Scholar] [CrossRef]
- Dowsett, M.; Nielsen, T.O.; A’Hern, R.; Bartlett, J.; Coombes, R.C.; Cuzick, J.; Ellis, M.; Henry, N.L.; Hugh, J.C.; Lively, T.; et al. Assessment of Ki67 in breast cancer: Recommendations from the International Ki67 in Breast Cancer working group. J. Natl. Cancer Inst. 2011, 103, 1656–1664. [Google Scholar] [CrossRef] [Green Version]
- Romero, Q.; Bendahl, P.O.; Klintman, M.; Loman, N.; Ingvar, C.; Ryden, L.; Rose, C.; Grabau, D.; Borgquist, S. Ki67 proliferation in core biopsies versus surgical samples—A model for neo-adjuvant breast cancer studies. BMC Cancer 2011, 11, 341. [Google Scholar] [CrossRef] [Green Version]
- Maltoni, R.; Palleschi, M.; Ravaioli, S. Spotlight on Ki67 as a prognostic marker in early breast cancer: All that glitters may not be gold. Diagn. Pathol. 2020, 15, 109. [Google Scholar] [CrossRef] [PubMed]
- Manolescu, L.; Marinescu, P. Sex differences in HIV-1 viral load and absolute CD4 cell count in long term survivors HIV-1 infected patients from Giurgiu, Romania. Rom. Rev. Lab. Med. 2013, 21, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Aileni, R.M.; Pasca, S.; Suciu, G. MIoT applications for wearable technologies used for health monitoring. In Proceedings of the 10th International Conference on Electronics, Computers and Artificial Intelligence (ECAI), Seoul, Korea, 21–24 September 2008; pp. 1–4. [Google Scholar]
- Dillon, D.A.; Guidi, A.J.; Schnitt, S.J. Pathology of invasive breast cancer. In Diseases of the Breast, 4th ed.; Harris, J.R., Lippman, M.E., Morrow, M., Osborne, C.K., Eds.; Lippincott, Williams and Wilkins: Philadelphia, PA, USA, 2009; p. 386. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predictor | Coefficient | p Value | HR [CI95%] |
|---|---|---|---|
| Ki 67 | 0.02 | 0.0268 | 1.02 [1.01–1.04] |
| Strata | Events (%) | RMST OS | Median Survival OS [CI95%] |
|---|---|---|---|
| Ki67 Low | 7.14 | 35.20 | N/A |
| Ki67 High | 25.00 | 31.90 | N/A |
| Strata | Events (%) | RMST OS | Median Survival [CI95%] |
|---|---|---|---|
| NST subtype | 9.70 | 34.70 | N/A |
| Lobular carcinoma | 0.00 | 36.00 | N/A |
| Others | 17.85 | 33.60 | N/A |
| Strata | Events (%) | RMST OS | Median Survival OS [CI95%] |
|---|---|---|---|
| G1 and G2 | 3.89 | 35.50 | N/A |
| G3 | 16.92 | 33.50 | N/A |
| Strata | Events (%) | RMST PFS | Median Survival PFS [CI95%] |
|---|---|---|---|
| Ki67 Low | 20.53 | 32.30 | N/A |
| Ki67 High | 42.85 | 29.00 | N/A [30.00 la N/A] |
| Strata | Events (%) | RMST PFS | Median Survival PFS [CI95%] |
|---|---|---|---|
| G1 and G2 | 14.28 | 33.50 | N/A |
| G3 | 35.38 | 29.80 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niță, I.; Nițipir, C.; Toma, Ș.A.; Limbău, A.M.; Pîrvu, E.; Bădărău, I.A.; Suciu, I.; Suciu, G.; Manolescu, L.S.C. Histological Aspects and Quantitative Assessment of Ki67 as Prognostic Factors in Breast Cancer Patients: Result from a Single-Center, Cross Sectional Study. Medicina 2020, 56, 600. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56110600
Niță I, Nițipir C, Toma ȘA, Limbău AM, Pîrvu E, Bădărău IA, Suciu I, Suciu G, Manolescu LSC. Histological Aspects and Quantitative Assessment of Ki67 as Prognostic Factors in Breast Cancer Patients: Result from a Single-Center, Cross Sectional Study. Medicina. 2020; 56(11):600. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56110600
Chicago/Turabian StyleNiță, Irina, Cornelia Nițipir, Ștefania Andreea Toma, Alexandra Maria Limbău, Edvina Pîrvu, Ioana Anca Bădărău, Ioana Suciu, George Suciu, and Loredana Sabina Cornelia Manolescu. 2020. "Histological Aspects and Quantitative Assessment of Ki67 as Prognostic Factors in Breast Cancer Patients: Result from a Single-Center, Cross Sectional Study" Medicina 56, no. 11: 600. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56110600