
Self-Expandable Metal Stents for Left Sided Colon Obstruction from Diverticulitis. A Single Center Retrospective Series

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Series
2.2. Therapeutic Approach
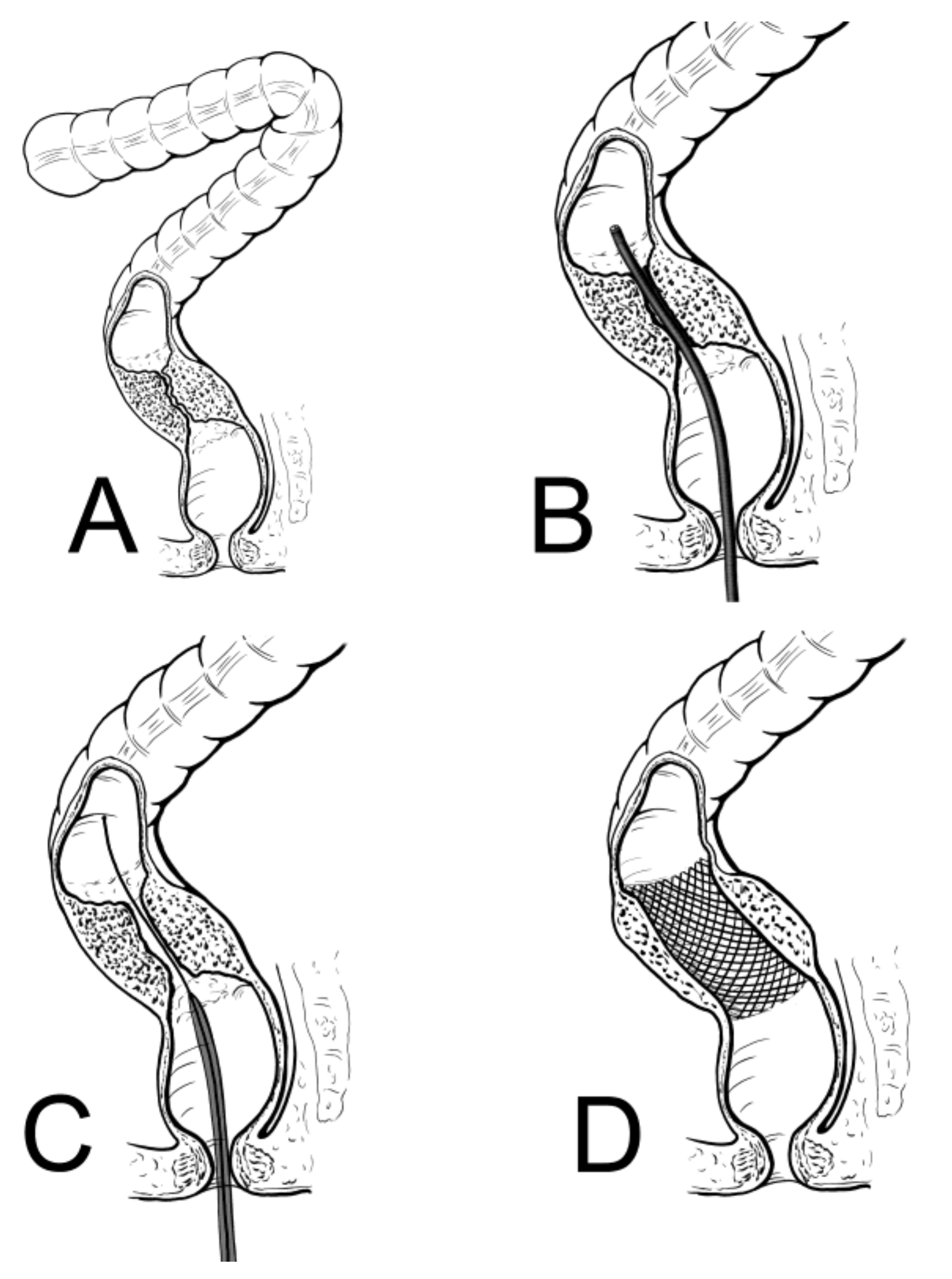
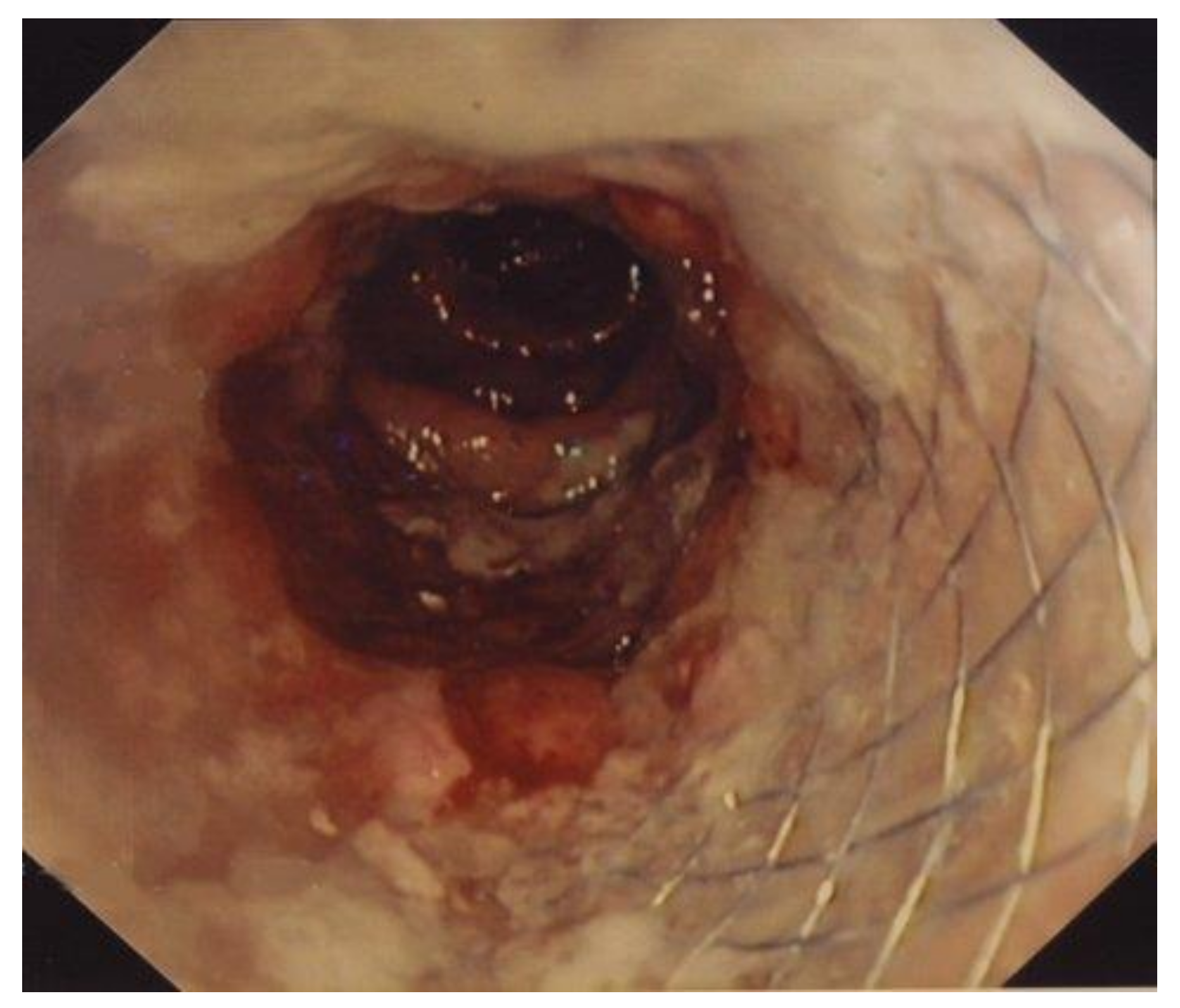
2.3. SEMS Placement
2.4. Follow-Up Evaluation
3. Results
3.1. Early Results (within 7 Days from SEMS Placement)
3.2. Early Results (from 8 Days to 3 Weeks from SEMS Placement)
3.3. Six Months Results
3.3.1. SEMS as Definitive Treatment
3.3.2. SEMS as a Bridge to Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Theodoropoulos, D. Current Options for the Emergency Management of Diverticular Disease and Options to Reduce the Need for Colostomy. Clin. Colon Rectal Surg. 2018, 31, 229–235. [Google Scholar] [CrossRef]
- Shah, S.D.; Cifu, A.S. Management of Acute Diverticulitis. JAMA 2017, 318, 291–292. [Google Scholar] [CrossRef]
- Strate, L.L.; Morris, A.M. Epidemiology, Pathophysiology, and Treatment of Diverticulitis. Gastroenterology 2019, 156, 1282–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young-Fadok, T.M. Diverticulitis. N. Engl. J. Med. 2018, 379, 1635–1642. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Nguyen, L.H.; Song, M.; Jovani, M.; Liu, P.H.; Cao, Y.; Tam, I.; Wu, K.; Giovannucci, E.L.; Strate, L.L.; et al. Intake of Dietary Fiber, Fruits, and Vegetables and Risk of Diverticulitis. Am. J. Gastroenterol. 2019, 114, 1531–1538. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Scarpignato, C.; Strate, L.L.; Lanas, A.; Kruis, W.; Lahat, A.; Danese, S. Colonic diverticular disease. Nat. Rev. Dis. Primers 2020, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Sköldberg, F.; Granlund, J.; Discacciati, A.; Hjern, F.; Schmidt, P.T.; Olén, O. Incidence and lifetime risk of hospitalization and surgery for diverticular disease. Br. J. Surg. 2019, 106, 930–939. [Google Scholar] [CrossRef]
- Hawkins, A.T.; Wise, P.E.; Chan, T.; Lee, J.T.; Glyn, T.; Wood, V.; Eglinton, T.; Frizelle, F.; Khan, A.; Hall, J.; et al. Diverticulitis: An Update from the Age Old Paradigm. Curr. Probl Surg. 2020, 57, 100862. [Google Scholar] [CrossRef]
- Lee, J.M.; Bai, P.; Chang, J.; El Hechi, M.; Kongkaewpaisan, N.; Bonde, A.; Mendoza, A.E.; Saillant, N.N.; Fagenholz, P.J.; Velmahos, G.; et al. Hartmann’s Procedure vs Primary Anastomosis with Diverting Loop Ileostomy for Acute Diverticulitis: Nationwide Analysis of 2,729 Emergency Surgery Patients. J. Am. Coll. Surg. 2019, 229, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Maraj, B.; Wray, C.M. Antibiotic Discretion in the Treatment of Acute Uncomplicated Diverticulitis: A Teachable Moment. JAMA Intern. Med. 2018, 178, 1258–1259. [Google Scholar] [CrossRef]
- Lamazza, A.; Fiori, E.; Sterpetti, A.V.; Schillaci, A.; De Cesare, A.; Lezoche, E. Endoscopic placement of self-expandable metallic stents for rectovaginal fistula after colorectal resection: A comparison with proximal diverting ileostomy alone. Surg. Endosc. 2016, 30, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Lamazza, A.; Fiori, E.; Carati, M.V.; Guzzo, A.; Pronio, A.; Sterpetti, A.V. Therapeutic options for emergency gastrointestinal malignancy in COVID19 pandemic. The role of operative endoscopy. Br. J. Surg. 2020, 107, e403–e404. [Google Scholar] [CrossRef]
- Lamazza, A.; Fiori, E.; Schillaci, A.; Sterpetti, A.V. A new technique for placement of a self-expanding metallic stent (SEMS) in patients with colon rectal obstruction: A prospective study of 43 patients. Surg. Endosc. 2013, 27, 1045–1048. [Google Scholar] [CrossRef] [PubMed]
- Sterpetti, A.V.; Sapienza, P.; Fiori, E.; Di Marzo, L.; Lamazza, A. Improved results for left-sided malignant colorectal obstruction with a proper selection for self expandable metal stent placement, surgical resection or diverting stoma. Eur. J. Surg. Oncol. 2020, 46, 2064–2067. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, A.T.; Samuels, L.R.; Rothman, R.; Geiger, T.M.; Penson, D.F.; Resnick, M.J. National Variation in Elective Colon Resection for Diverticular Disease. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Angenete, E.; Thornell, A.; Burcharth, J. Laparoscopic lavage is feasible and safe for the treatment of perforated diverticulitis with purulent peritonitis: The first results from the randomized controlled trial DILALA. Ann. Surg. 2016, 263, 117–122. [Google Scholar] [CrossRef]
- Francis, N.K.; Sylla, P.; Abou-Khalil, M.; Arolfo, S.; Berler, D.; Curtis, N.J.; Dolejs, S.C.; Garfinkle, R.; Gorter-Stam, M.; Hashimoto, D.A.; et al. EAES and SAGES 2018 consensus conference on acute diverticulitis management: Evidence-based recommendations for clinical practice. Surg. Endosc. 2019, 33, 2726–2741. [Google Scholar] [CrossRef] [Green Version]
- Stewart, D.B. Review of the American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Treatment of Left-Sided Colonic Diverticulitis. JAMA Surg. 2021, 156, 94–95. [Google Scholar]
- Patel, S.V.; Hendren, S.; Zaborowski, A.; Winter, D.; for Members of the Evidence Based Reviews in Surgery group. Evidence-based Reviews in Surgery Long-term Outcome of Surgery Versus Conservative Management for Recurrent and Ongoing Complaints After an Episode of Diverticulitis: Five-year Follow-up Results of a Multicenter Randomized Controlled Trial (DIRECT-Trial). Ann. Surg. 2020, 272, 284–287. [Google Scholar] [CrossRef]
- Bolkenstein, H.E.; Consten, E.C.J.; van der Palen, J.; van de Wall, B.J.M.; Broeders, I.A.M.J.; Bemelman, W.A.; Lange, J.F.; Boermeester, M.A.; Draaisma, W.A.; Dutch Diverticular Disease (3D) Collaborative Study Group. Long-term Outcome of Surgery Versus Conservative Management for Recurrent and Ongoing Complaints After an Episode of Diverticulitis: 5-year Follow-up Results of a Multicenter Randomized Controlled Trial (DIRECT-Trial). Ann. Surg. 2019, 269, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Biondo, S.; Golda, T.; Kreisler, E.; Espin, E.; Vallribera, F.; Oteiza, F.; Codina-Cazador, A.; Pujadas, M.; Flor, B. Outpatient versus hospitalization management for uncomplicated diverticulitis: A prospective, multicenter randomized clinical trial (DIVER Trial). Ann. Surg. 2014, 259, 38–44. [Google Scholar] [CrossRef]
- Tursi, A.; Picchio, M.; Elisei, W.; Di Mario, F.; Scarpignato, C.; Brandimarte, G. Current Management of Patients with Diverticulosis and Diverticular Disease: A Survey From the 2nd International Symposium on Diverticular Disease. J. Clin. Gastroenterol. 2016, 50 (Suppl. S1), S97–S100. [Google Scholar] [CrossRef] [PubMed]
- Pfützer, R.H.; Kruis, W. Management of diverticular disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 629–638. [Google Scholar] [CrossRef]
- Bocca, A.; Lamazza, A.; Pino, A.; De Masi, E.; Iacomino, M.; Mattei, D.; Rahimi, S.; Fiori, E.; Schillaci, A.; Alimonti, A.; et al. Determination of 30 elements in colorectal biopsies by sector field inductively coupled plasma mass spectrometry: Method development and preliminary baseline levels. Rapid Commun. Mass Spectrom. 2007, 21, 1776–1782. [Google Scholar] [CrossRef] [PubMed]
- Lamazza, A.; Fiori, E.; Demasi, E.; Scoglio, D.; Sterpetti, A.V.; Lezoche, E. Self-expanding metal stents for treatment of anastomotic complications after colorectal resection. Endoscopy 2013, 45, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Venezia, L.; Michielan, A.; Condino, G.; Sinagra, E.; Stasi, E.; Galeazzi, M.; Fabbri, C.; Anderloni, A. Feasibility and safety of self-expandable metal stents in non malignant disease of the lower gastrointestinal tract. World J. Gastrointest Endosc. 2020, 12, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Fiori, E.; Crocetti, D.; Lamazza, A.; DE Felice, F.; Sterpetti, A.V.; Irace, L.; Mingoli, A.; Sapienza, P.; De Toma, G. Is Low Inferior Mesenteric Artery Ligation Worthwhile to Prevent Urinary and Sexual Dysfunction After Total Mesorectal Excision for Rectal Cancer? Anticancer Res. 2020, 40, 4223–4228. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean Age (Range) | 71.5 Years (50–99) |
| Sex (M/F) | 12/9 |
| Acute obstruction (%) | 9/21 (43%) |
| Subacute obstruction (%) | 12/21 (57%) |
| Severe inflammation at admission * | 6/21 |
| Moderate inflammation at admission ** | 9/21 |
| Minimal inflammation at admission *** | 6/21 |
| Abdominal pain | 21/21 |
| Abdominal distension | 21/21 |
| Signs of peritoneal inflammation | 6/21 |
| Characteristic | SEMS as Permanent Solution (4) | SEMS as Bridge to Colectomy (17) |
|---|---|---|
| Distance anal verge (cm) (min-max) | 30 (25–35) | 29 (20–38) |
| Length of stenosis (cm) (min-max) | 6 (4–8) | 6 (4–12) |
| Type of stent (covered/uncovered) | 4/0 | 15/2 |
| Length of stent (cm) | 9–12 | 9–12 |
| Difficult procedure | 0 | 0 |
| Early complications (within 7 days from post-procedure) | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamazza, A.; Carati, M.V.; Guzzo, A.; Pronio, A.M.; Nicolanti, V.; Antoniozzi, A.; Sterpetti, A.V.; Fiori, E. Self-Expandable Metal Stents for Left Sided Colon Obstruction from Diverticulitis. A Single Center Retrospective Series. Medicina 2021, 57, 299. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030299
Lamazza A, Carati MV, Guzzo A, Pronio AM, Nicolanti V, Antoniozzi A, Sterpetti AV, Fiori E. Self-Expandable Metal Stents for Left Sided Colon Obstruction from Diverticulitis. A Single Center Retrospective Series. Medicina. 2021; 57(3):299. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030299
Chicago/Turabian StyleLamazza, Antonietta, Maria Vittoria Carati, Anna Guzzo, Anna Maria Pronio, Virgilio Nicolanti, Angelo Antoniozzi, Antonio V. Sterpetti, and Enrico Fiori. 2021. "Self-Expandable Metal Stents for Left Sided Colon Obstruction from Diverticulitis. A Single Center Retrospective Series" Medicina 57, no. 3: 299. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030299