
The Management between Comorbidities and Pain Level with Physical Activity in Individuals with Hip Osteoarthritis with Surgical Indication: A Cross-Sectional Study


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample
2.3. Instruments
2.3.1. Anthropometric Data
2.3.2. International Physical Activity Questionnaire (IPAQ), Long Form
2.3.3. Visual Analogic Scale (VAS)
2.4. Proceadure—Registration Form
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guilak, F.; Fermor, B.; Keefe, F.J.; Kraus, V.B.; Olson, S.O.; Pisetsky, D.S.; Setton, L.A.; Weinberg, J.B. The role of biomechanics and inflammation in cartilage injury and repair. Clin. Orthop. Relat. Res. 2004, 423, 17–26. [Google Scholar] [CrossRef]
- Murphy, N.J.; Eyles, J.P.; Hunter, D.J. Hip osteoarthritis: Etiopathogenesis and Implications for Management. Adv. Ther. 2016, 33, 1921–1946. [Google Scholar] [CrossRef] [Green Version]
- Stone, R.C.; Baker, J. Painful Choices: A Qualitative Exploration of Facilitators and Barriers to Active Lifestyles among Adults with Osteoarthritis. J. Appl. Gerontol. 2017, 36, 1091–1116. [Google Scholar] [CrossRef]
- Cibulka, M.T.; Bloom, N.J.; Enseki, K.R.; Macdonald, C.W.; Woehrle, J.; McDonough, C.M. Hip Pain and Mobility Deficits—Hip Osteoarthritis: Revision 2017. J. Orthop. Sports Phys Ther. 2017, 47, A1–A37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jotanovic, Z.; Mihelic, R.; Gulan, G.; Sestan, B.; Dembic, Z. Osteoarthritis of the hip: An overview. Period. Biol. UDC 2015, 117, 95–108. [Google Scholar]
- Abhishek, A.; Doherty, M. Diagnosis and clinical presentation of osteoarthritis. Rheum. Dis. Clin. 2013, 39, 45–66. [Google Scholar] [CrossRef] [PubMed]
- Richmond, S.A.; Fukuchi, R.K.; Ezzat, A.; Schneider, K.; Schneider, G.; Emery, C.A. Are joint injury, sport activity, physical activity, obesity, or occupational activities predictors for osteoarthritis? A systematic review. J. Orthop. Sports Phys. Ther. 2013, 43, 515–B19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishidou, Y.; Matsuyama, K.; Sakuma, D.; Setoguchi, T.; Nagano, S.; Kawamura, I.; Maeda, S.; Komiya, S. Osteoarthritis of the hip joint in elderly patients is most commonly atrophic, with low parameters of acetabular dysplasia and possible involvement of osteoporosis. Arch. Osteoporos. 2017, 12, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosvig, K.K.; Jacobsen, S.; Sonne-Holm, S.; Palm, H.; Troelsen, A. Pre-valence of malformations of the hip joint and their relationship to sex, groin pain, and risk of osteoarthritis: A population-based survey. J. Bone Joint. Surg. Am. 2010, 92, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Dai, L.; Jiang, L.; Qiu, S. Difference in Subchondral Cancellous Bone between Postmenopausal Women with Hip Osteoarthritis and Osteoporotic Fracture. Arthritis Rheum. 2012, 64, 3955–3962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Nelson, A.E.; Abbate, L.M.; et al. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2009, 36, 809–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judd, D.L.; Thomas, A.C.; Dayton, M.R.; Stevens-Lasley, J.E. Strength and Functional Deficits in Individuals with Hip Osteoarthritis Compared to Healthy, Older Adults. Disabil. Rehabil. 2014, 36, 307–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, L.B.; Helmick, C.G.; Schwartz, T.A.; Renner, J.B.; Tudor, G.; Koch, G.G.; Dragomir, A.D.; Kalsbeek, W.D.; Luta, G.; Jordan, J.M. One in four people may develop symptomatic hip osteoarthritis in his or her lifetime. Osteoarthr. Cartil. 2010, 18, 1372–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Kraus, V.B.; Sprow, K.; Powell, K.E.; Buchner, D.; Bloodgood, B.; Piercy, K.; George, S.M.; Kraus, W.E. Effects of Physical Activity in Knee and Hip Osteoarthritis: A Systematic Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1324–1339. [Google Scholar] [CrossRef]
- Bennell Kl Hinman, R.S. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J. Sci. Med. Sport. 2011, 14, 4–9. [Google Scholar] [CrossRef]
- Lima, D.F.; Levy, R.B.; Luiz, O.C. Recommendations for physical activity and health: Consensus, controversies, and ambiguities. Rev. Panam. Salud Publica 2014, 36, 164–170. [Google Scholar]
- Gonçalves, M.P.; Alchieri, J.C. Motivation to practicing physical activities: A study with non-athletes. Psico-USF 2010, 15, 125–134. [Google Scholar] [CrossRef]
- Byberg, L.; Melhus, H.; Gedeborg, R.; Sundstrom, J.; Ahlbom, A.; Zethelius, B.; Berglund, L.G.; Wolk, A.; Michaelsson, K. Total mortality after changes in leisure time physical activity in 50 year old men: 35 year follow-up of population based cohort. BMJ 2009, 43, 482. [Google Scholar] [CrossRef] [Green Version]
- Hunter, D.J.; Eckstein, F. Exercise and osteoarthritis. J. Anat. 2009, 214, 197–207. [Google Scholar] [CrossRef]
- Arokoski, J.P.; Jurvelin, J.S.; Vaatainen, U.; Helminen, H.J. Normal and pathological adaptations of articular cartilage to joint loading. Scand. J. Med. Sci. Sports 2000, 10, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, M.B.; Helevik, A.I.; Valborg, B.; Furnes Ove Langhammer, A.; Flugsrud, G.; Nordsletten, L.; Storheim, J.A.Z.K. Leisure time physical activity and the risk of hip or knee replacement due to primary osteoarthritis: A population based cohort study (The HUNT Study). BMC Musculoskelet Disord. 2016, 17, 86. [Google Scholar] [CrossRef] [Green Version]
- Griffin, T.M.; Guilak, F. The role of mechanical loading in the onset and progression of osteoarthritis. Exerc. Sport Sci. Rev. 2005, 33, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Matsumoto, S.; Kawashima, T.; Mitani, S.; Miura, Y. Walking speed affects instrumental activities of daily living in patients with hip osteoarthritis. J. Back Musculoskelet Rehabil. 2017, 30, 309–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubbs, B.; Hurley, M.; Smith, T. What are the factors that influence physical activity participation in adults with kneeand hip osteoarthritis? A sistematic review of physical activity correlates. Clin. Rehabil. 2015, 29, 80–94. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.A.; Cook, C.; Abbott, J.H. Variables Associated With the Progression of Hip Osteoarthritis: A Systematic Review. Arthritis Rheum. 2009, 61, 925–936. [Google Scholar] [CrossRef] [PubMed]
- Pollard, T.C.B.; Batra, R.N.; Judge, A.; Watkins, B.; McNally, E.G.; Gill, H.S.; Thomas, G.E.R.; Glyn-Jones, S.; Arden, N.K.; Carr, A.J. The hereditary predisposition to hip osteoarthritis and its association with abnormal joint morphology. Osteoarthr. Cartil. 2013, 21, 314–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castano-Betancourt, M.C.; Van Meurs, J.B.J.; Bierna-Zeinstra, S.; Rivadeneira, F.; Hofman, A.; Weinans, H.; Uitterlinden, A.G.; Waarsing, J.H. The contribution of hip geometry to the prediction of hip osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1530–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helgesson, L.; Johannsson Pk Aurell, Y.; Tiderius, C.; Karrholm, J.; Riad, J. Early osteoarthritis after slipped capital femoral epiphysis. Acta Orthop. 2018, 89, 222–228. [Google Scholar] [CrossRef] [Green Version]
- Ganz, R.; Parvizi, J.; Beck, M.; Leunig, M.; Notzli, H.; Siebenrock, K.A. Femoroacetabular Impingement. A cause for Osteoarthritis of the Hip. Clin. Orthop. Relat. Res. 2003, 417, 112–120. [Google Scholar]
- Kemp, J.; Grimaldi, A.; Heerey, J.; Denise, J.; Scholes, M.; Lawrenson, P.; Coburn, S.; King, M. Current trends in sport and exercise hip conditions: Intra-articular and extra-articular hip pain, with detailed focus on femoroacetabular impingement (FAI)syndrome. Best Pracr. Res. Rheumatol. 2019, 33, 66–87. [Google Scholar] [CrossRef]
- LaFrance, R.; Williams, R.; Madsen, W.; Maloney, M.; Drinkwater, C.; Giordano, B. The Prevalence of Radiographic Criteria of Femoral Acetabular Impingement in Patients Undergomig Hip Arthropalsty Surgery. Geriatr. Orthop. Surg. Reabil. 2014, 5, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity:a systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef]
- Teirlinck, C.H.; Dorleijn, D.M.J.; Bos, P.K.; Rijkels-Otters, J.B.M.; Bierma-Zeinstra, S.M.A.; Luijsterburg, P.A.J. Prognostic factors for progression of osteoarthritis of the hip: A systematic review. Arthritis Res. Ther. 2019, 21, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, L.; Rong, J.; Wang, Y.; Hu, F.; Bao, C.; Li, X.; Zhao, Y. The relationship between body mass index and hip osteoarthritis: A systematic review and meta-analysis. Jt. Bone Spine 2011, 78, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Rooji, M.; Van der Leeden, M.; Heymans, M.W.; Holla, J.F.M.; Hakkinen, A.; Lems, W.F.; Roorda, L.D.; Veenhof, C.; Sanchez-Ramirez, D.C.; De vet, H.C.W.; et al. Course and predictors of pain and physical functioning in patients with hip osteoarthritis: Systematic review and meta-analysis. J. Rehabil. Med. 2016, 48, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juhakoski, R.; Malmivaara, A.; Lakka, T.A.; Tenhonen, S.; Hannila, M.L.; Arokoski, J.P. Determinants of pain and functioning in hip osteoarthritis—A two-year prospective study. Clin. Rehabil. 2013, 27, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, J.T.; Wylie, J.D.; Kapron, A.L.; Hanson, J.A.; Maak, T.G.; Aoki, S.K. The Effect of NSAID Prophylaxis and Operative Variables on Heterotopic Ossification After Hip Arthroscopy. Am. J. Sports Med. 2014, 42, 1359–1364. [Google Scholar] [CrossRef] [PubMed]
- Morcos, M.W.; Teeter, M.G.; Somerville, L.E.; Lanting, B. Correlation between hip osteoarthritis and the level of physical activity as measured by wearable technology and patient-reported questionnaires. J. Orthop. 2019, 20, 236–239. [Google Scholar] [CrossRef]
- Rosemann, T.; Kuehlein, T.; Laux, G.; Szecsenyi, J. Osteoarthritis of the knee and hip: A comparison of factors associated with physical activity. Clin. Rheumatol. 2007, 26, 1811–1817. [Google Scholar] [CrossRef]
- Karande, S.P.; Kini, S. Osteoarthritis: Clinical and Radiological Correlation. J. Assoc. Physicians India 2018, 66, 37–39. [Google Scholar]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity ans sedentary behavior. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Matsudo, S.; Araujo, T.; Matsudo, V.; Andrade, D.; Andrade, E.; Oliveira, L.C.; Braggion, G. Questionário Internacional de atividade física (IPAQ): Estudo de Validade e Reprodutibilidade no Brasil. Rer. Bras Ativ. Fís Saúde 2001, 6, 5–18. [Google Scholar]
- Jarrell, J.F.; Vilos, G.A.; Allaire, C.; Burgess, S.; Fortin, C.; Gerwin, R.; Lapensee, L.; Lea, R.H.; Leyland, N.A.; Martyn, P.; et al. No. 164-Consensus Guidelines for the Management of Chronic Pelvic Pain. J. Obstet. Gynaecol. Can. 2018, 40, e747–e787. [Google Scholar] [CrossRef]
- Hallal, P.C.; Gomez, L.F.; Parra, D.C.; Lobelo, F.; Mosquera, J.; Florindo, A.A.; Reis rs Pratt, M.; Sarmiento, O.L. Lessons learned after 10 years of IPAQ use in Brazil and Colombia. J. Phys. Act. Health 2010, 7 (Suppl. 2), S259–S264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistics a power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Kopec, J.A.; Cibere, J.; Li, L.C.; Zhang, C.; Barber, M.; Qian, H.; Wong, H.; Steininger, G.; Prlic, H.; Simatovic, J.; et al. Relationship between physical activity and hip pain in persons with and without cam or pincer morphology: A population-based case-control study. Osteoarthr. Cartil. 2017, 25, 1055–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, M.H.; Van der Pas, S.; Denkinger, M.D.; Parsons, C.; Jamenson, K.A.; Schaap, L.; Zambon, S.; Castel, M.; Herbolsheimer, F.; Nasell, H.; et al. Relationships between physical performance and knee and hip osteoarthritis: Findings from the European Project on osteoarthritis (EPOSA). Age Ageing 2014, 43, 806–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seror, R.; Tubach, F.; Baron, G.; Falissard, B.; Logeart, I.; Dougados, M.; Ravaud, P. Individualizing the WOMAC function subscale: Incorporating patients’ priorities for improvement to measure functional impairment in hip or knee osteoarthritis. Ann. Rheum. Dis. 2008, 67, 494–499. [Google Scholar] [CrossRef] [Green Version]
- Dolin, S.J.; CWilliams, A.C.; Ashford, N.; George, J.; Pereira, L.; Perello, A. Factors affecting medical decision-making in patients with osteoarthritis of the hip: Allocation of surgical priority. Disabil. Rehabil. 2003, 25, 771–777. [Google Scholar] [CrossRef]
- Gademan, M.G.J.; Hofstede, S.N.; Vliet Vlieland, T.P.M.; Nelissen, R.G.H.H.; Marang-van de Mheen, P.J. Indication criteria for total hip or knee arthroplasty in osteoarthritis: A state-of-the-science overview. BMC Musculoskelet Disord. 2016, 17, 463. [Google Scholar] [CrossRef] [Green Version]
- Wyles, C.C.; Heidenreich, M.J.; Jeng, J.; Larson, D.R.; Trousdale, R.T.; Sierra, R.J. The John Charnley Award: Redefining the Natural History of Osteoarthritis in Patients with Hip Dysplasia and Impingement. Clin. Orthop. Relat. Res. 2017, 475, 336–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ku, P.W.; Steptoe, A.; Liao, Y.; Hsueh, M.C.; Chen, L.J. A cut-off daily sedentary time and all-cause mortality in adults: A meta-regression analysis involving more than 1 million participants. BMC Med. 2018, 16, 74. [Google Scholar] [CrossRef]
- Bennel, K.; Hunter, D.J.; Vicenzino, B. Long-term effects of sports: Preventing and managing OA in the Athlete. Nat. Rev. Rheumatol. 2012, 12, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Veenhof, C.; Huisman, P.A.; Barten, J.A.; Takken, T.; Pisters, M.F. Factors associated with physical activity in patients with osteoarthritis of the hip or knee: A systematic review. Osteoarthr. Cartil. 2012, 20, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| General | Group I | Group II | Group III | |
|---|---|---|---|---|
| Age (Years) | 49.90 ± 14.68 | 49.81 ± 16.22 | 46.89 ± 12.48 | 55.14 ± 16.72 |
| BMI | 26.79 ± 4.97 | 26.99 ± 4.83 | 26.69 ± 5.28 | 27.19 ± 5.33 |
| osteoarthritis etiology | 100% | 51.90% | 35.20% | 13.00% |
| IPAQ | ||||
| Inactive | 22.20% | 32.10% | 10.50% | 14.30% |
| Active | 77.80% | 67.90% | 89.50% | 85.70% |
| Comorbidities | ||||
| Without | 37.00% | 28.60% | 47.40% | 50.00% |
| Present | 63.00% | 71.40% | 52.60% | 42.90% |
| Df (Inter Groups) | Df (Intra Groups) | Z | Sig | |
|---|---|---|---|---|
| GENERAL | 1 | 52 | 10.5 | 0.02 |
| GROUP I | 1 | 26 | 6.08 | 0.02 |
| GROUP II | 1 | 17 | 2.01 | 0.17 |
| GROUP III | 1 | 5 | 0.71 | 0.43 |
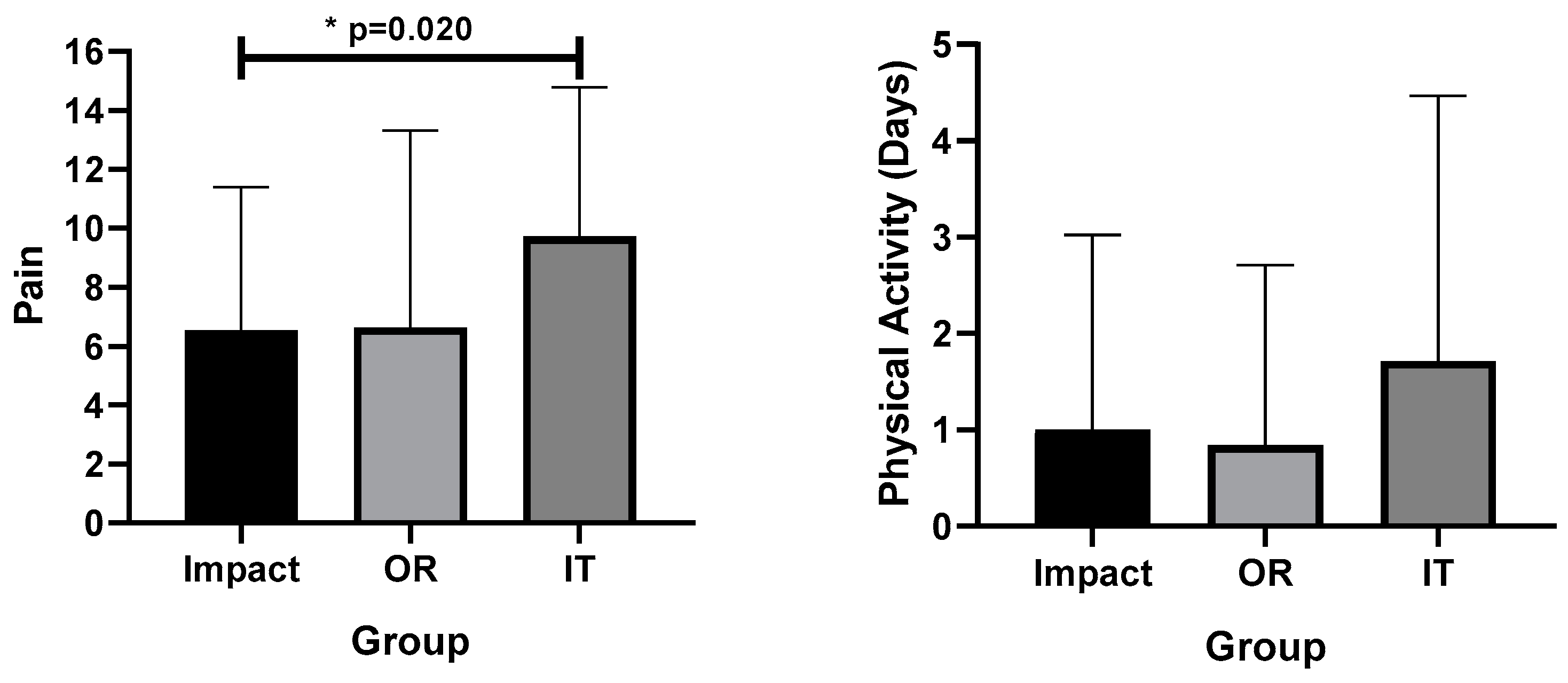
| BMI X ± SD (CI 95%) | TV (Hours) X ± SD (CI 95%) | VAS X ± SD (CI 95%) | |
|---|---|---|---|
| Impact | 28.26 ± 4.96 (23.67–32.85) | 5.43 ± 2.30 (3.30–7.55) | 6.86 ± 1.35 (5.61–8.10) |
| Osteonecrosis + Rheumatics | 25.31 ± 4.52 (21.13–29.49) | 4.29 ± 2.14 (2.31–6.26) | 8.14 ± 1.68 (6.59–9.69) |
| Infectious + Traumatic | 27.19 ± 5.33 (22.26–32.12) | 3.71 ± 1.98 (1.89–5.54) | 6.14 ± 2.19 (4.11–8.17) |
| p | 0.838 | 0.824 | 0.259 |
| η2p | 0.072 # | 0.169 # | 0.277 ## |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santiago, M.S.; Aidar, F.J.; dos Santos Moraes, T.L.; de Farias Neto, J.P.; Vieira Filho, M.C.; de Vasconcelos, D.P.; Leite, V.S.; Doria, F.M.; Sobral Porto, E.; Albuquerque Madruga, R.E.T.T.; et al. The Management between Comorbidities and Pain Level with Physical Activity in Individuals with Hip Osteoarthritis with Surgical Indication: A Cross-Sectional Study. Medicina 2021, 57, 890. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090890
Santiago MS, Aidar FJ, dos Santos Moraes TL, de Farias Neto JP, Vieira Filho MC, de Vasconcelos DP, Leite VS, Doria FM, Sobral Porto E, Albuquerque Madruga RETT, et al. The Management between Comorbidities and Pain Level with Physical Activity in Individuals with Hip Osteoarthritis with Surgical Indication: A Cross-Sectional Study. Medicina. 2021; 57(9):890. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090890
Chicago/Turabian StyleSantiago, Michael Silveira, Felipe J. Aidar, Talita Leite dos Santos Moraes, Jader Pereira de Farias Neto, Mário Costa Vieira Filho, Diego Protásio de Vasconcelos, Victor Siqueira Leite, Felipe Meireles Doria, Erick Sobral Porto, Reuthemann Esequias Teixeira Tenório Albuquerque Madruga, and et al. 2021. "The Management between Comorbidities and Pain Level with Physical Activity in Individuals with Hip Osteoarthritis with Surgical Indication: A Cross-Sectional Study" Medicina 57, no. 9: 890. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090890